Paeds · cardiology
Innocent murmurs and normal paediatric cardiovascular variants
Also known as Innocent cardiac murmur · Functional murmur · Physiological murmur · Still's murmur · Normal cardiovascular variants in children
Fellowship guide to recognising innocent murmurs and normal paediatric cardiovascular variants, distinguishing them from pathology, and avoiding unnecessary referral and investigation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Quote the source before you argue a cut-off, and never call a murmur innocent until you have excluded the red flags. [1] [2]
The 7 innocent murmurs
Overview & Definition
An innocent murmur is an audible sound generated by normal turbulent blood flow in a structurally normal heart, with no haemodynamic abnormality and no cardiac symptoms. It is the single most common reason a child is referred for a "heart check", and the skill of confidently recognising it saves families from anxiety, unnecessary investigations and sport restriction. [1] [2]
The same label should never be used loosely. Before you call a murmur innocent you must confirm a normal history (growth, feeding, exertion, colour, syncopal symptoms), normal heart sounds, normal pulses and a normal oxygen saturation, and you must be dealing with one of the recognised innocent patterns. [3] [6]
Classification
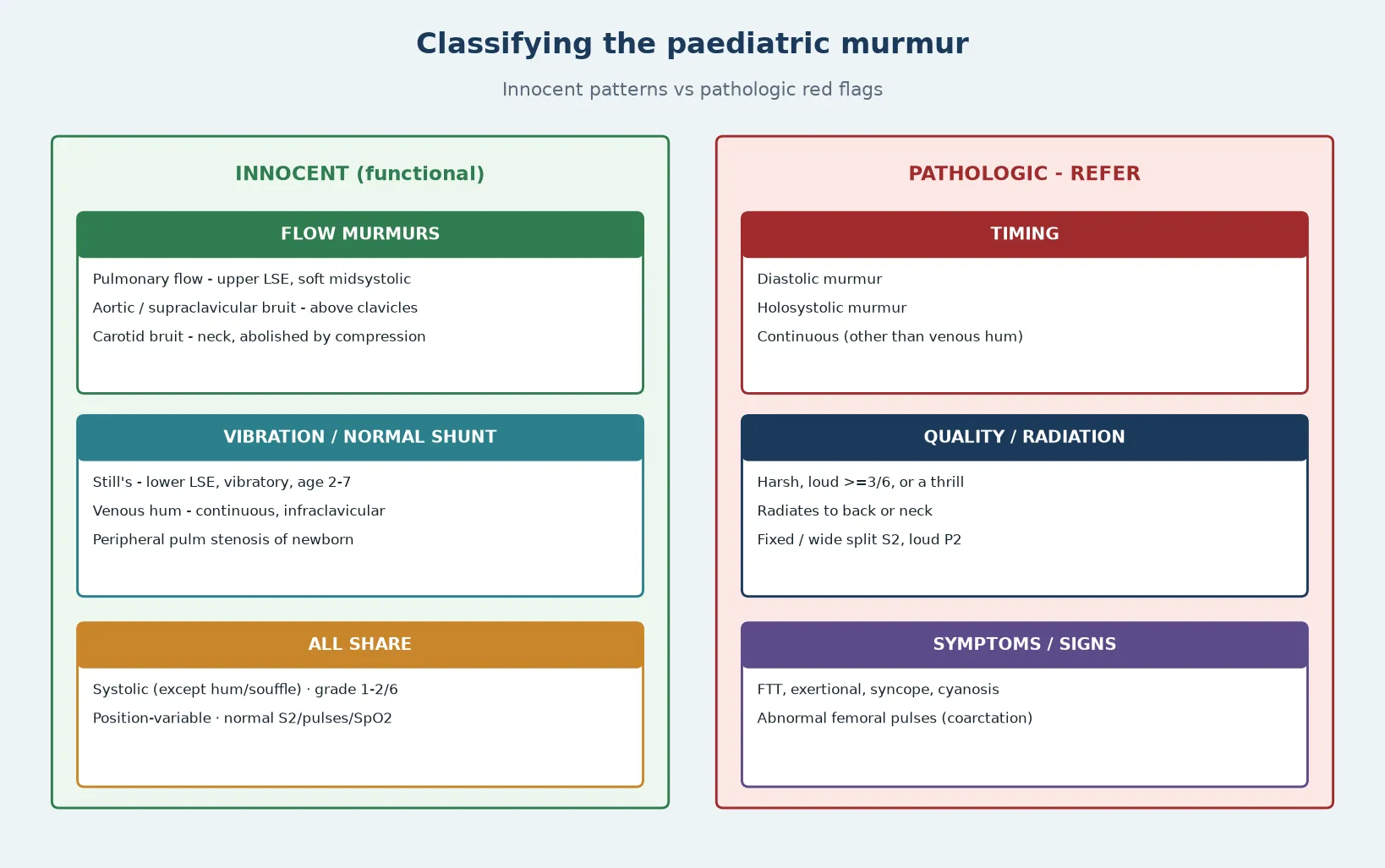
Think first about the child at the bedside, not the category. The innocent murmur you will hear most often is a soft, short, position-variable systolic sound in a thriving child — Still's vibratory at the lower left sternal edge, a pulmonary flow murmur at the upper left sternal edge, or a venous hum at the infraclavicular area. Behind these patterns lie two mechanisms: benign high-flow turbulence (pulmonary, aortic/supraclavicular, carotid) and normal vibration or shunt (Still's, venous hum, peripheral pulmonary stenosis of the newborn, mammary souffle). All are systolic except the venous hum and mammary souffle, which can be continuous. [3] [5]
Pathologic features are defined by what they are not: not soft, not short, not position-variable, and not confined to a recognised innocent location. Any diastolic murmur, any holosystolic murmur and any continuous murmur other than a classical venous hum is pathologic until proven otherwise. [1] [2]
Epidemiology & Risk Factors
Innocent murmurs are extremely common. Up to 80% of children have a heart murmur at some point in childhood, yet fewer than 1% of these are due to congenital heart disease. [1] [2] The prevalence peaks during periods of rapid somatic growth and high cardiac output — infancy, preschool and adolescence — and rises further with fever, anaemia, dehydration, anxiety and exercise. [5]
The patient who is mislabelled is usually well. The trap is the reverse: assuming a well-looking child cannot have pathology. Neonates are the exception. A murmur in a newborn carries a much higher probability of structural disease than the same murmur in a five-year-old, and the characteristics are harder to interpret during the transitional circulation. [1] [2]
Pathophysiology
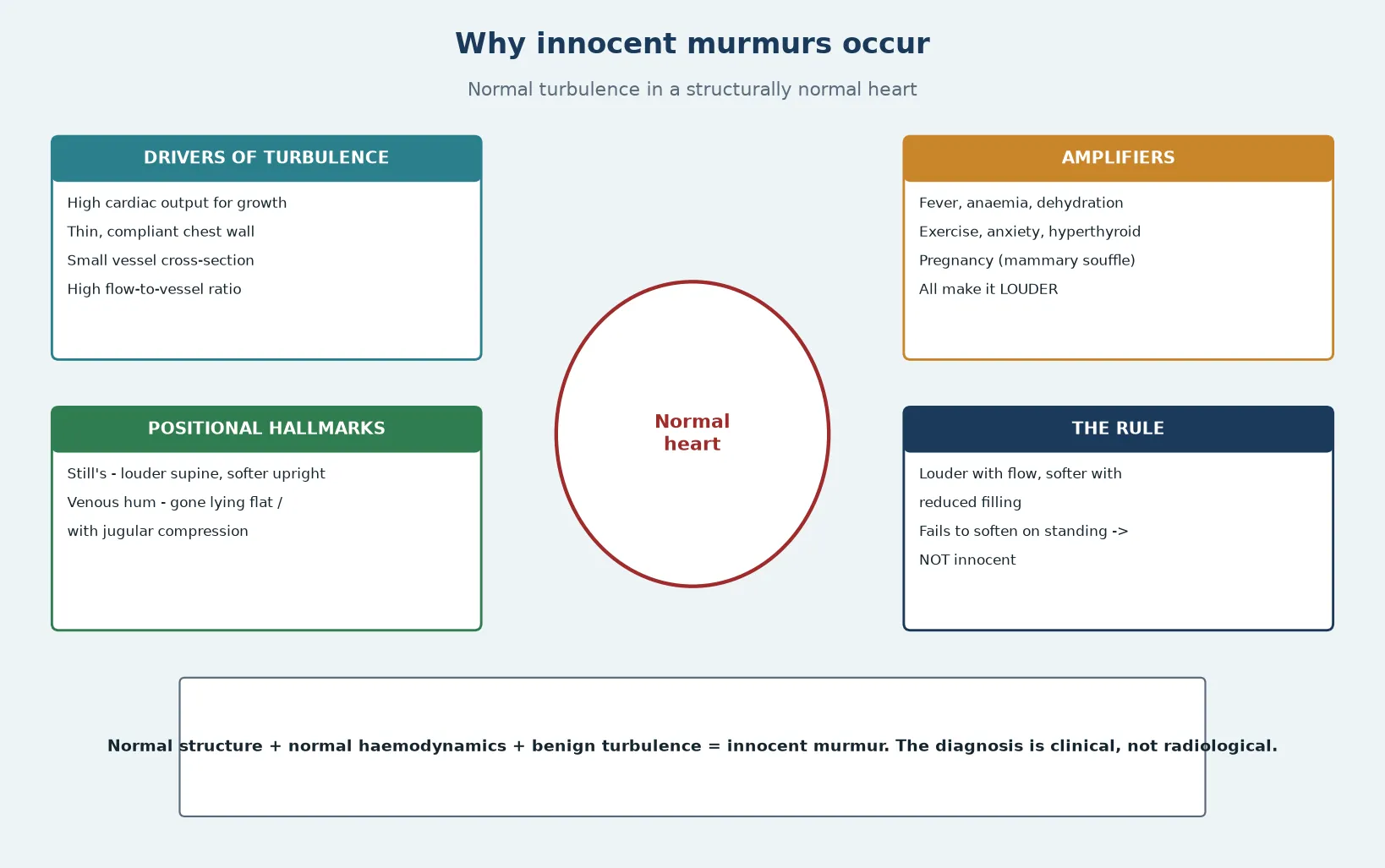
Cardiac output rises steeply through childhood to drive growth, so aortic and pulmonary flow velocities are high relative to vessel size. Thin chest walls, a sternum that has not yet hardened, and a small thoracic cross-section transmit that turbulence to the stethoscope. Still's murmur is thought to arise from vibration of pulmonary valve leaflets, chordal structures or the left ventricular outflow; the venous hum from turbulent flow in the jugular and subclavian veins. [5] [8]
The practical corollary is that anything increasing flow (fever, anaemia, exercise, hyperthyroidism) makes an innocent murmur louder, and anything reducing flow or filling (lying flat, compressing the jugular veins) makes it softer or disappears it. A murmur that gets louder on standing or fails to soften with positional change should not be labelled innocent. [5] [3]
Clinical Presentation
The child is thriving and asymptomatic. Parents may report that the murmur was "found at a routine check", after a febrile illness, or during a school or sporting assessment. There are no episodes of colour change, no breathlessness on feeding or exertion, no syncope or pre-syncope, and no squatting. Growth is normal for age. [1] [2]
On examination the child looks well, is well-grown, is pink, and is not distressed. The murmur is grade 1–2/6, soft, short and systolic, varies with respiration and posture, and sits in a recognised innocent location. The first and second heart sounds are normal; S2 moves physiologically with respiration and is not widely or fixed split. Femoral pulses are normal and symmetrical, with no radio-femoral delay, and oxygen saturation is normal in room air. [3] [6]
Differential Diagnosis
The job is not to list every congenital lesion but to separate innocent flow turbulence from the pathology that mimics it. A soft pulmonary-area murmur may be a pulmonary flow murmur or valvar pulmonary stenosis; a left-sternal-edge murmur may be Still's or a ventricular septal defect; a continuous infraclavicular hum may be a venous hum or a patent ductus arteriosus. [2] [10]
The discriminator is always the combination of murmur quality, heart sounds, pulses, symptoms and saturation — never the murmur alone. Atrial septal defect is the classic trap: the murmur is soft and pulmonary, but S2 is fixed and widely split, and the lesion is missed if you listen only to systole. Coarctation is the other trap: a systolic murmur with weak or absent femoral pulses. [1] [2]
Clinical & Bedside Assessment
Examine the child when calm, warm and ideally settled on a parent's lap, then repeat when cooperative supine, sitting and standing. Listen across the four classical areas and the back, using both the diaphragm and the bell. Palpate the apex for a heave and thrills, and feel the brachial and femoral pulses together, checking for radio-femoral delay. [5] [6]
Bedside manoeuvres confirm innocence. Still's murmur is louder supine and softer upright; a venous hum disappears when the child lies flat or when the jugular veins are compressed; a pulmonary flow murmur softens on sitting forward. Measure an oxygen saturation in room air — a normal value excludes most cyanotic disease but does not exclude an acyanotic shunt. [1] [11]
Investigations
In a child who meets all the innocent criteria, no investigations are required. Echocardiography, electrocardiography and chest radiography should not be ordered reflexively: they misclassify murmurs, they add cost, and a borderline result creates anxiety without changing management. [1] [10]
Investigate only when a red flag is present or the diagnosis is genuinely uncertain. Echocardiography is then the definitive test and confirms or excludes structural disease. Pulse oximetry is a useful adjunct in any neonate or infant with a murmur, because a low or differential saturation flags critical congenital heart disease that auscultation can miss. [1] [2]
Management — Resuscitation
There is no resuscitation in the classic innocent murmur, but the decision point is recognition of the sick child who has been mislabelled. Any child with a murmur and shock, respiratory distress, profound cyanosis or hepatomegaly has pathology and needs emergency assessment, not a clinic letter. [2]
The red-flag list is your safety net. If a murmur is diastolic, holosystolic, continuous (other than venous hum), harsh, loud with a thrill, associated with abnormal pulses, a fixed split S2, symptoms or poor growth, abandon the innocent label and arrange paediatric cardiology review. [1] [2]
Management — Definitive & Stepwise
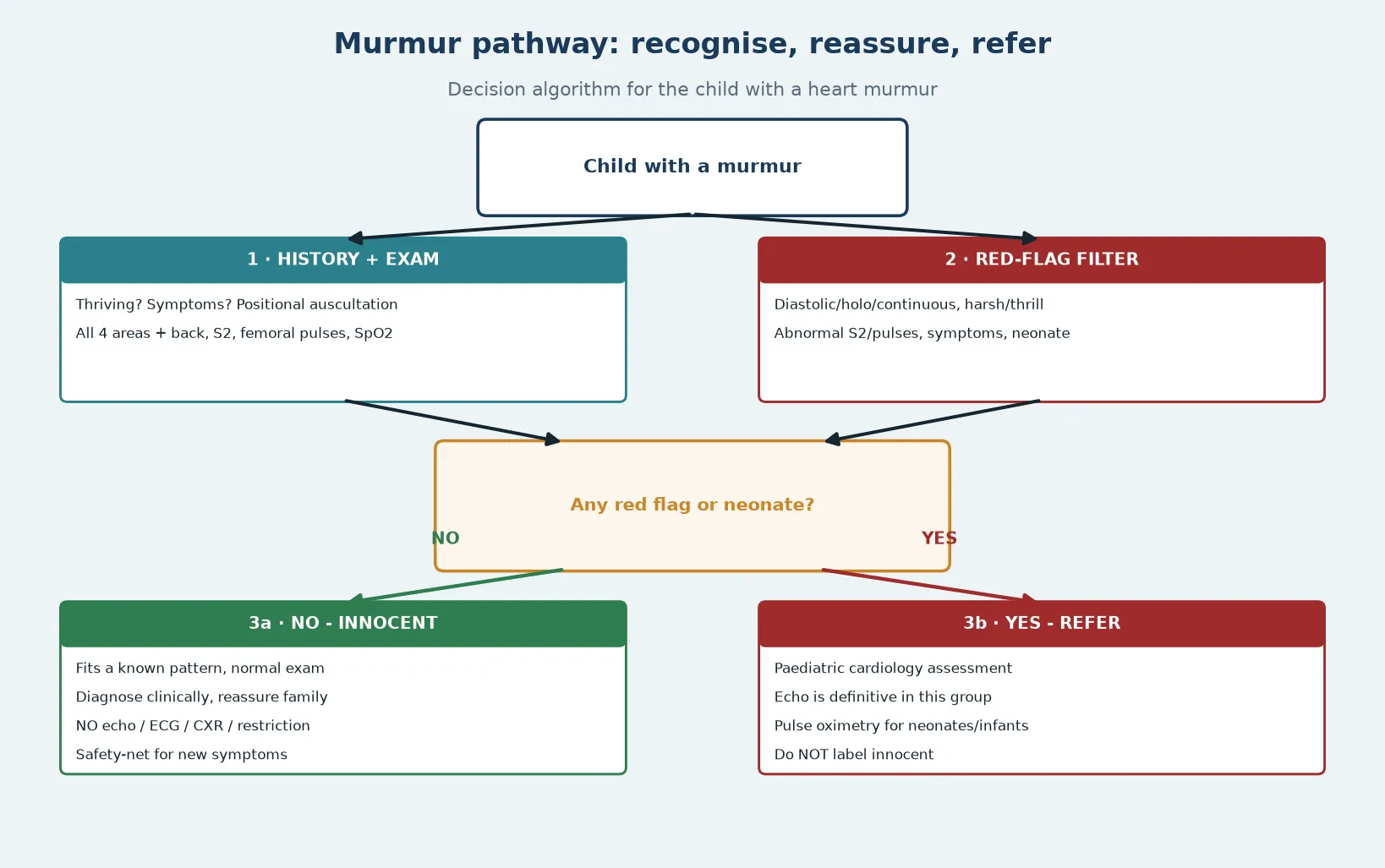
- Confirm the child is thriving and asymptomatic on focused history.
- Examine positionally with all four areas, the back, heart sounds and both pulses.
- Apply the red-flag filter; if any flag is present, refer to paediatric cardiology.
- If all criteria fit a recognised innocent pattern, make the diagnosis clinically.
- Reassure the family, document the specific innocent murmur and why, and safety-net for any new symptoms.
- No echocardiogram, no restriction, no endocarditis prophylaxis, and no follow-up unless symptoms change. [1] [3] [6]
Specific Subtypes & Scenarios
Still's vibratory murmur is the commonest innocent murmur, heard in children aged 2–7 years. It is a low-pitched, vibratory or musical, grade 2/6 systolic murmur at the lower left sternal edge, loudest supine and softer when upright; heart sounds and pulses are normal. [3] [7]
Pulmonary flow murmur is a soft, short, midsystolic murmur at the upper left sternal edge, normal S2, common in children and adolescents and louder with high-output states. Distinguish from an atrial septal defect by checking S2 splits normally. [2] [5]
Venous hum is a continuous, humming murmur in the infraclavicular area, louder on the right, loudest sitting and disappearing when supine or with jugular compression. It is the one innocent murmur that is continuous — so confirm the positional hallmark before you reassure. [3] [6]
Peripheral pulmonary stenosis of the newborn is a soft systolic murmur at the axillae and back in the first weeks of life from branch pulmonary artery angles; it resolves by 6 months but must be distinguished from true pulmonary stenosis. Supraclavicular and carotid bruits are systolic, heard above the clavicles, and abolished by shoulder extension or carotid compression. [5] [2]
Neonate with a murmur. Never label a newborn murmur innocent on first hearing. Refer newborns for paediatric cardiology assessment, because neonatal murmurs carry higher pathology rates and the transitional circulation changes the picture; perform pulse oximetry screening to catch critical congenital heart disease. [1] [2]
Complications & Pitfalls
The harm in this topic is iatrogenic: unnecessary echocardiograms, parental anxiety, sport restriction, and endocarditis prophylaxis given where none is needed. A borderline echocardiogram that over-reads a normal variant converts a well child into a "cardiac patient". [1] [10]
The opposite error is more dangerous. Mislabelling a pathologic murmur as innocent delays diagnosis of coarctation, atrial septal defect, valvar stenosis or a small ventricular septal defect. The commonest mechanisms are listening only to systole (missing fixed split S2), not feeling the femoral pulses, and assuming a thriving child cannot have pathology. [2] [11]
Prognosis & Disposition
Innocent murmurs resolve with growth as the chest wall thickens and flow velocities normalise, usually within months to a few years. Once correctly diagnosed, the child needs no follow-up, no activity restriction, no endocarditis prophylaxis, and routine dental care. Families can be counselled that the heart is structurally normal. [1] [3]
Disposition is therefore reassurance and discharge from the general paediatric clinic, with a safety-net to return if new symptoms appear (exertional intolerance, syncope, breathlessness, colour change, poor growth). The exception is the neonate, who is referred onward. [2]
Special Populations
Neonates and infants. Apply a lower threshold. Refer newborns rather than label, and use pulse oximetry to detect critical congenital heart disease. [1]
Adolescents. Still's murmur is less common but pulmonary flow murmurs, supraclavicular bruits and a pregnancy-related mammary souffle appear; the athletic adolescent also presents for pre-participation screening. [4]
Fever, anaemia, dehydration. High-output states amplify innocent murmurs; reassess when the child is well, and do not label a murmur during acute illness unless it is clearly an old known finding. [5]
Children with disability or limited cooperation. Examine in a calm position, use a reliable saturation, and accept a lower threshold for echocardiography when the history or examination is uncertain. [11]
Evidence, Guidelines & Regional Differences
Ford and colleagues (2022) give the contemporary primary-care algorithm: most older-child murmurs are innocent and can be followed serially if no red flags; refer newborns; do not reflexively image. [1] Huq and Rahman (2024) give the ANZ general-practice perspective, stressing that around half of children have a murmur at some point and under 1% reflect congenital heart disease. [2] Menashe (2007) remains the paediatric-in-review teaching anchor. [3] Pelech's two reviews define the physiology and the when-to-refer reasoning. [5] [6]
Emerging evidence supports computer-assisted and artificial-intelligence auscultation: convolutional neural networks distinguish Still's murmur from pathology with high sensitivity, and computer-assisted auscultation has reduced referrals of asymptomatic children. [9] [12] These tools may help non-specialist settings but do not yet replace the clinical red-flag assessment. [9]
Exam Pearls
- An innocent murmur is systolic, soft, short, position-variable, with normal S2, normal pulses and a thriving asymptomatic child. [1]
- Any diastolic, holosystolic or continuous (non-venous-hum) murmur is pathologic. [2]
- Still's murmur: lower left sternal edge, vibratory, ages 2–7, softer upright. [3]
- Venous hum: continuous, infraclavicular, gone when supine or with jugular compression. [6]
- Atrial septal defect masquerades as an innocent murmur — check for a fixed widely split S2. [2]
- Never label a neonatal murmur innocent; refer and screen with pulse oximetry. [1]
- No routine echocardiography, ECG or CXR for the clearly innocent murmur. [1]
References
- [1]Ford B Heart Murmurs in Children: Evaluation and Management. American family physician, 2022.PMID 35289571
- [2]Huq A Cardiac murmurs in children. Australian journal of general practice, 2024.PMID 38957059
- [3]Menashe V Heart murmurs. Pediatrics in review, 2007.PMID 17400822
- [4]Naik RJ Teenage heart murmurs. Pediatric clinics of North America, 2014.PMID 24267454
- [5]Pelech AN The physiology of cardiac auscultation. Pediatric clinics of North America, 2004.PMID 15561171
- [6]Pelech AN The cardiac murmur. When to refer? Pediatric clinics of North America, 1998.PMID 9491089
- [7]Dursun H Blood pressure and heart rate monitoring in children and adolescent with Still's vibratory murmur. Blood pressure monitoring, 2022.PMID 34992203
- [8]Advani N The diagnosis of innocent murmurs in childhood. Cardiology in the young, 2000.PMID 10950330
- [9]Shekhar R Automated identification of innocent Still's murmur using a convolutional neural network. Frontiers in pediatrics, 2022.PMID 36210944
- [10]Begic Z Evaluation of Diagnostic Methods in the Differentiation of Heart Murmurs in Children. Acta informatica medica, 2016.PMID 27147798
- [11]Hueckel RM Pediatric Murmurs. The Nursing clinics of North America, 2023.PMID 37536793
- [12]Watrous RL The impact of computer-assisted auscultation on physician referrals of asymptomatic patients with heart murmurs. Clinical cardiology, 2008.PMID 18257026