Paeds · cardiology
Kawasaki disease and coronary complications
Also known as Kawasaki disease · Kawasaki syndrome · Mucocutaneous lymph node syndrome · KD
Fellowship guide to Kawasaki disease and its coronary complications: the febrile infant with conjunctivitis, rash and red cracked lips, the diagnostic criteria for complete and incomplete disease, the 10-day IVIG and aspirin window that prevents aneurysms, the IVIG-resistant child and escalation to infliximab or steroids, coronary artery z-score grading and anti-thrombotic management, the long-term risk of stenosis and myocardial infarction, and the AHA, European SHARE and ANZ consensus positions.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eighteen-month-old who has been hot and miserable for six days, with red sticky-free eyes, a cracked bleeding mouth, an angry widespread rash, and swollen peeling hands that make her scream when you examine them. No single feature is unique to one illness, but together they are Kawasaki disease — and the clock is already running on a ten-day window to protect her coronary arteries. [1]
Kawasaki disease is an acute, febrile, self-limited vasculitis of childhood that preferentially involves medium-sized muscular arteries, with a striking and characteristic tropism for the coronary arteries. It is the leading cause of acquired heart disease in children in high-income countries. First described by Tomisaku Kawasaki in Japan in 1967, it replaces the older term mucocutaneous lymph node syndrome and is now defined by a clinical cluster of features rather than by any single laboratory test. [4]
Three ideas anchor the whole topic for a fellowship candidate. Kawasaki disease is common enough that every general paediatrician will meet it, and its coronary complications are preventable if treated within ten days. It is a clinical diagnosis, so the skill is in pattern recognition and a low threshold to treat incomplete disease. And it is never truly "over" for a child who develops aneurysms — the lesions can regress, but they can also progress to stenosis, thrombosis and myocardial infarction decades later, which is why surveillance is lifelong. [1]
Classification
The most useful way to think about Kawasaki disease is along three axes that each change what you do: the clinical phenotype, the response to IVIG, and the severity of coronary involvement on echocardiography. [1]
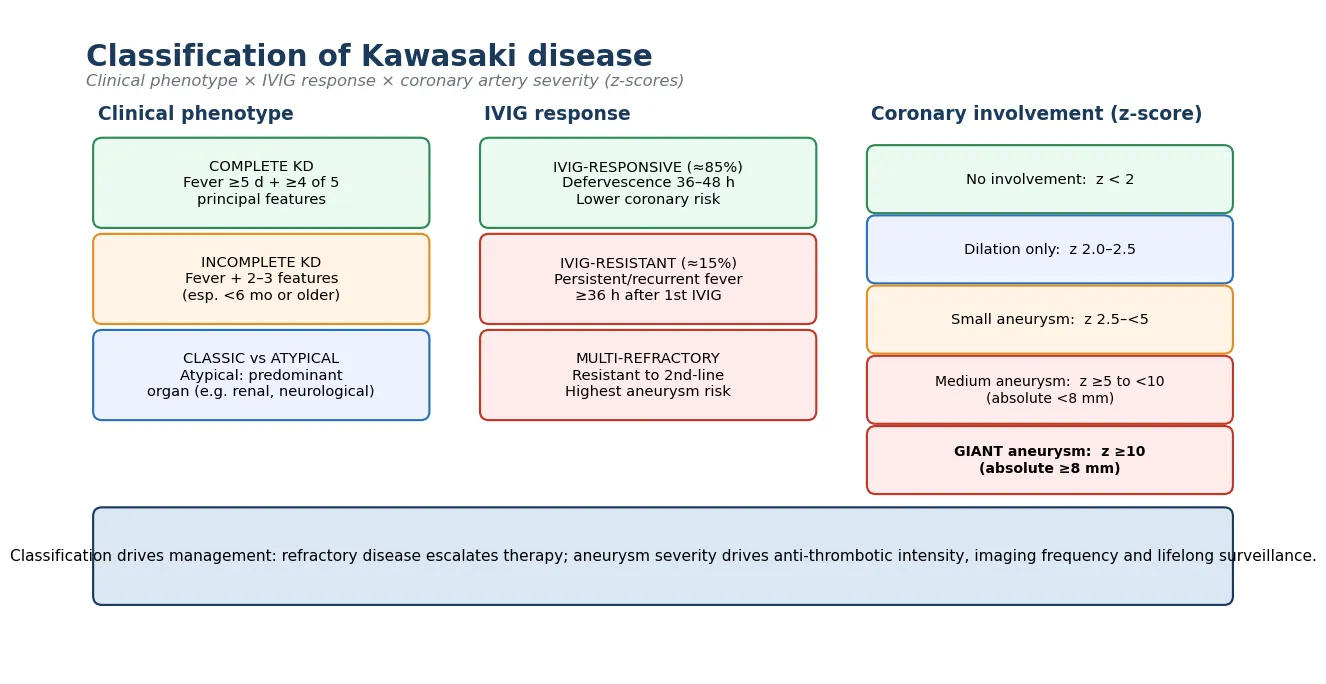
On the phenotype axis, complete Kawasaki disease is fever for five days or more plus at least four of the five principal clinical features. Incomplete disease is fever with only two or three features, and it carries its own danger because the coronary risk is at least as high and the diagnosis is delayed. Atypical disease presents with an unusual predominant feature — say, renal or neurological involvement — that can mislead the clinician away from the diagnosis. [1] [4]
The IVIG-response axis matters because it separates the children whose inflammation settles cleanly from the fifteen per cent or so whose fever persists or returns. IVIG-responsive disease resolves within 36 to 48 hours and carries a lower coronary risk. IVIG-resistant disease — persistent or recrudescent fever 36 to 48 hours after the first infusion — marks the children at highest risk of aneurysms and drives escalation to a second IVIG, infliximab or other adjuncts. Multi-refractory disease resists second-line therapy and carries the worst coronary outlook. [6] [8]
Complete KD
full criteria
- Fever ≥5 d + ≥4 of 5 features
- Straightforward diagnosis
- Standard IVIG + aspirin
- Lower diagnostic delay
Incomplete KD
fever + 2–3 features
- Commonest in <6 mo and older children
- Coronary risk at least as high
- Treat on suspicion + labs + echo
- Do not wait for full criteria
IVIG-resistant
≈15%
- Fever ≥36 h after first IVIG
- Highest aneurysm risk
- Second IVIG or infliximab
- Repeat echo, trend inflammation
Giant aneurysm
z ≥10 or ≥8 mm
- Highest thrombosis and MI risk
- Add anticoagulation
- Lifelong specialist surveillance
- Risk of late stenosis
The coronary-severity axis, graded by z-score, decides the intensity of anti-thrombotic treatment and the frequency of follow-up. Dilation alone is a z-score from 2.0 to 2.5, a small aneurysm is 2.5 to under 5, a medium aneurysm is z-score ≥5 to under 10 with absolute diameter under 8 mm, and a giant aneurysm is a z-score of ten or more or an absolute diameter of at least eight millimetres. Giant aneurysms rarely regress fully and carry the highest risk of thrombosis and myocardial infarction. [1] [5]
Epidemiology & Risk Factors
Kawasaki disease is most common in children under five years, who account for around eighty per cent of cases, and the peak age is between six months and two years. It is rare under three months and over five years, but those atypical ages carry a higher rate of incomplete presentation and coronary complications. Boys are affected slightly more often than girls, and the disease shows a clear ethnic gradient — children of East Asian descent have the highest incidence, roughly ten to twenty times that of children of European ancestry. [4] [9]
The incidence tells the regional story. In Japan the annual rate approaches three hundred per one hundred thousand children under five, the highest in the world. In Australia and New Zealand the rate is much lower but higher than in Europe, with the Australian surveillance study confirming substantial rates in children of East Asian and Pacific heritage, and a recognised burden in Aboriginal and Torres Strait Islander children. There is seasonal clustering and a well-described three-year epidemic cycle. [9]
The numbers that anchor your viva
The strongest risk factor for coronary aneurysm is not an inherited trait but a modifiable one: delay in treatment beyond ten days. The other recognised predictors of aneurysms are age under six months, age over five years, male sex, a high C-reactive protein and low albumin at baseline, IVIG resistance, and evidence of coronary involvement on the baseline echocardiogram. These are the variables that should lower your threshold to escalate therapy and intensify surveillance. [1] [6]
Pathophysiology
The central mechanism is an uncontrolled inflammatory response in the walls of medium-sized muscular arteries, driven by an exaggerated innate immune reaction in a genetically susceptible host after an infectious trigger. The coronaries are preferentially affected because of their anatomy and the response of their vasa vasorum. [1] [4]
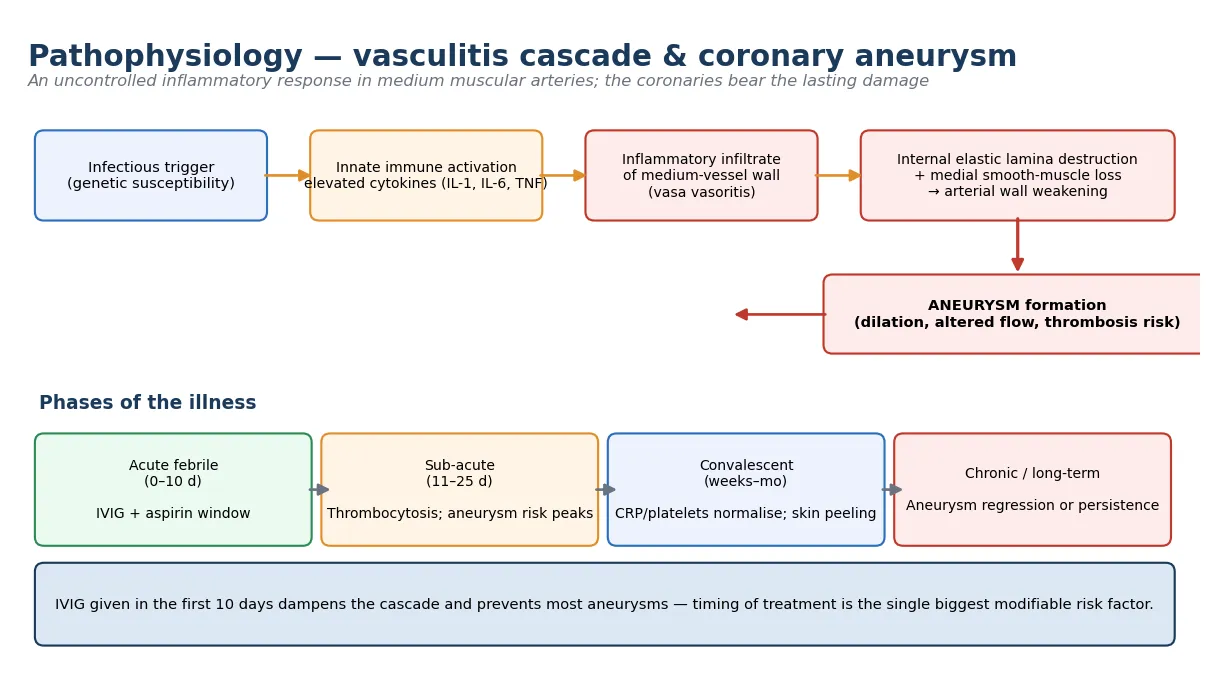
In the acute phase, inflammatory cells — macrophages, neutrophils and cytotoxic T lymphocytes — infiltrate the vascular wall, beginning in the vasa vasorum. The inflammation destroys the internal elastic lamina and depletes the medial smooth-muscle layer, so the arterial wall weakens and balloons outward into an aneurysm under systemic arterial pressure. The altered flow within the dilated segment, combined with endothelial dysfunction and a hypercoagulable state from the intense inflammation and rising platelet count, sets up the risk of thrombosis. [1]
The illness runs in recognisable phases that explain both the clinical course and the timing of complications. The acute febrile phase, lasting one to eleven days, is the window for IVIG and aspirin and the period in which aneurysms begin to form. The sub-acute phase, from around day eleven to day twenty-five, brings falling fever, thrombocytosis, peeling of the fingers and toes, and the peak risk of aneurysm development and coronary thrombosis. The convalescent phase, over weeks to months, is when inflammatory markers normalise. The chronic phase is the lifelong period in which aneurysms may regress or, especially if large, progress to stenotic lesions. [4] [13]
[1] [2]Clinical Presentation
The clinical picture is a cluster, and the skill is in seeing the pattern rather than fixing on any single feature. Fever is the constant and the anchor: it is high, remittent, and unresponsive to antibiotics, and it lasts five days or more unless treated. The other features are not all present at once and may appear sequentially, which is why a child seen on day three can look non-specific and the same child on day six can look unmistakable. [1] [9]
The five principal features, alongside the fever, are well worth memorising because the criteria are examinable. Bilateral, painless, non-purulent conjunctivitis spares the limbs and is often the first feature noticed by parents. Oral changes include red cracked lips, a strawberry tongue with prominent papillae, and oropharyngeal erythema without ulceration. The rash is polymorphous — morbilliform, maculopapular or even scarlatiniform — and is often concentrated in the perineum, where it peels early. Extremity changes are acute erythema and oedema of the palms and soles, followed in the second week by membranous peeling of the fingertips. Cervical lymphadenopathy, usually unilateral and at least 1.5 centimetres, is the least common of the five features. [1] [4]
| Clinical picture | What it implies | Act |
|---|
Children may also be irritable, and this irritability out of proportion to the clinical state is a frequently under-recognised clue. Other associated features include anterior uveitis, sterile pyuria, arthritis, abdominal pain, diarrhoea, vomiting, hepatic dysfunction, gallbladder hydrops, aseptic meningitis, and a reactive arthritis of the small joints. None of these is a principal criterion, but their presence in a febrile child should raise Kawasaki disease on the differential. [4] [1]
Differential Diagnosis
Build the differential in layers, because Kawasaki disease is a diagnosis of exclusion when features are incomplete, and several mimics are common and treatable. The first layer is the febrile exanthem of childhood: measles (Koplik spots, prodrome, rash progression), scarlet fever (pastorial lines, sandpaper rash, positive streptococcal test), and other viral exanthems such as adenovirus, enterovirus and Epstein–Barr virus. [4] [11]
The second layer is the drug reaction. Stevens–Johnson syndrome and toxic epidermal necrolysis share mucosal involvement but show blistering, target lesions and skin detachment, and staphylococcal scalded skin syndrome shows widespread superficial peeling. The most feared mimic is staphylococcal toxic shock syndrome, which shares fever, rash, conjunctivitis and later peeling, but adds hypotension and multi-organ failure and is driven by toxin-producing staphylococci. [1]
Viral exanthems
- Measles (Koplik spots, prodrome)
- Adenovirus, enterovirus
- Epstein–Barr virus
- Roseola (human herpesvirus 6)
Drug & toxin
- Stevens–Johnson syndrome (target lesions, blistering)
- Toxic epidermal necrolysis
- Staphylococcal toxic shock (hypotension)
- Scalded skin syndrome
Bacterial & other
- Scarlet fever (sandpaper rash)
- Juvenile idiopathic arthritis (systemic)
- Rickettsial disease
- Multisystem inflammatory syndrome in children
The third and newest layer is multisystem inflammatory syndrome in children, the post-infectious inflammatory condition linked to SARS-CoV-2. It overlaps strikingly with Kawasaki disease — fever, conjunctivitis, rash and coronary involvement — but tends to affect older children, has prominent gastrointestinal and cardiac dysfunction, and often shows left-ventricular dysfunction rather than isolated coronary aneurysms. The COVID-19 pandemic also drove delayed and missed diagnoses of classic Kawasaki disease, which is a warning to keep the diagnosis actively in mind. [11] [15]
The decisive step when the diagnosis is uncertain is not a single test but a synthesis of the clinical pattern, the inflammatory markers, and the echocardiogram. If Kawasaki disease is plausible and inflammatory markers are high, treat within the window rather than waiting for certainty, because the cost of a missed early window is a preventable aneurysm. [1]
Clinical & Bedside Assessment
Assessment runs in parallel with the decision to treat, because the ten-day window is short and a febrile, irritable child can deteriorate. Take a focused history of the fever duration and pattern, the sequence of features, recent infections and immunisations, and any sick contacts, while you examine for the principal features and the associated clues. Document the day of illness at presentation, because that single number drives the urgency of treatment. [1]
The examination looks systematically for the five principal features and the supporting signs. Check the conjunctivae for bilateral sparing injection, the mouth for cracked lips and strawberry tongue, the skin for the polymorphous rash and early perineal peeling, the hands and feet for erythema and oedema, and the neck for cervical lymphadenopathy. Look for irritability, anterior uveitis on slit lamp, arthritis, and abdominal signs. [4]
[1] [11]A careful baseline cardiovascular examination is essential, though it is often normal in uncomplicated disease. Listen for a gallop, a tachycardia out of proportion to fever, a pericardial rub, or a murmur of mitral regurgitation from papillary muscle ischaemia, any of which suggests cardiac involvement and raises the urgency of echocardiography. Document the blood pressure, perfusion and pulses, and weigh the child, because weight determines the IVIG dose. [1]
Investigations
There is no diagnostic blood test for Kawasaki disease, so investigations serve three purposes: to support the diagnosis in incomplete cases, to stage the inflammatory burden, and to detect coronary involvement. The supporting laboratory profile is one of acute systemic inflammation: a raised C-reactive protein and erythrocyte sedimentation rate, a neutrophil-predominant leucocytosis, thrombocytosis in the second week, anaemia of chronic disease, hypoalbuminaemia, and often mild hepatic dysfunction and sterile pyuria. [1]
Echocardiography is the cornerstone and the investigation that defines the coronary complications. A baseline study should be obtained at diagnosis to look for coronary dilation, aneurysms, pericardial effusion, valvular regurgitation and ventricular dysfunction, and it should be repeated at one to two weeks and again at four to six weeks after treatment, or sooner if clinical changes occur. Coronary dimensions are reported as z-scores — standard-deviation scores adjusted for body surface area — because a single millimetre value means different things in an infant and a teenager. [5] [1]
When the clinical picture is incomplete, the AHA supplementary laboratory criteria help tip the balance toward treatment. These include anaemia for age, a platelet count over 450 000 per microlitre after day seven, an albumin ≤30 g/L (≤3.0 g/dL), a raised alanine aminotransferase, a white cell count over 15 000, and a urine with ten or more white cells per high-power field. Fever plus two or three clinical features plus an abnormal echocardiogram or a raised CRP or ESR with three or more supplementary lab criteria supports treatment. [1]
The standard diagnostic workup
Document fever duration and the five principal features; examine for associated clues.
Full blood count, CRP, ESR, albumin, liver function, urine microscopy and culture.
Baseline echocardiogram with coronary z-scores at diagnosis.
Repeat echocardiogram at 1–2 weeks and 4–6 weeks (or sooner if clinical change).
Screen for mimics (measles, streptococcal, viral serology, SARS-CoV-2) where relevant.
For incomplete disease, apply AHA supplementary laboratory criteria and treat on suspicion.
After the acute illness, the imaging strategy follows the coronary severity. Children with normal coronaries return to routine care. Those with aneurysms enter serial echocardiographic surveillance, and larger or giant aneurysms often require additional cardiac magnetic resonance or coronary angiography to define stenosis, thrombus and collateral flow, particularly when symptoms of ischaemia appear. [13] [12]
Management — Resuscitation
Resuscitation in Kawasaki disease is rarely about airway or circulation in the immediate sense, because most children are haemodynamically stable. The emergency is the inflammatory cascade and the closing ten-day window to prevent aneurysms, so the resuscitation mindset is to diagnose early, treat aggressively, and support the child through the febrile illness with fluids, antipyretics and comfort. [1]
Children who are genuinely unwell — those with myocarditis, pericardial effusion with tamponade, shock, or a toxic overlap with multisystem inflammatory syndrome — need the full paediatric resuscitation approach: airway and breathing support, intravenous fluids cautiously titrated because of myocardial involvement, inotropes for shock, and a low threshold for paediatric intensive care. These presentations blur the line between Kawasaki disease and multisystem inflammatory syndrome and demand early cardiology and intensive-care involvement. [15] [1]
KAWASAKI
A practical point for the retrieving clinician: a child in a rural or remote setting with a compatible illness should receive IVIG and aspirin before transfer if the diagnosis is likely, rather than waiting for the cardiac centre to confirm it, because the journey can consume the remaining treatment window. Telehealth consultation with a paediatric cardiologist supports the decision to treat locally. [9]
Management — Definitive & Stepwise
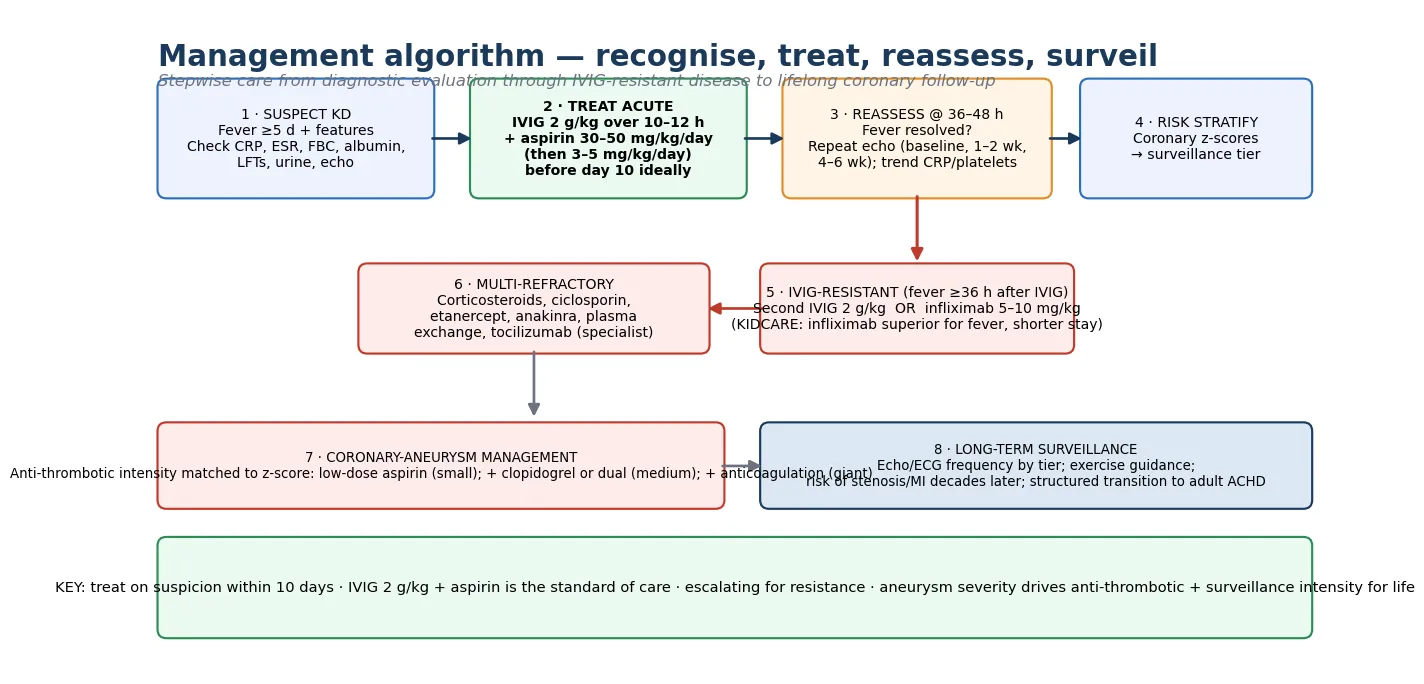
Definitive management is the combination of intravenous immunoglobulin and aspirin, given as early as possible and ideally within ten days of fever onset. The standard regimen is a single infusion of IVIG at 2 g/kg over ten to twelve hours, together with high-dose aspirin at 30 to 50 mg/kg per day in divided doses. Once the child is afebrile, aspirin steps down to an anti-thrombotic dose of 3 to 5 mg/kg per day and continues until the coronary arteries are shown to be normal six to eight weeks after onset. [1] [2]
The evidence base for this regimen is one of the strongest in paediatric cardiology. The landmark 1986 trial showed that IVIG plus aspirin reduced coronary aneurysms from about a fifth to a few per cent, and the 1991 trial established that a single 2 g/kg infusion was superior to four smaller infusions, which is why the single-dose regimen is now standard. These trials transformed Kawasaki disease from a leading cause of childhood heart disease into a largely preventable one. [2] [3]
The treatment arc of Kawasaki disease
For IVIG-resistant disease — persistent or recurrent fever 36 to 48 hours after the first infusion — the stepwise escalation begins with a second dose of IVIG at 2 g/kg or infliximab at 5 to 10 mg/kg. The KIDCARE randomised trial directly compared infliximab with a second IVIG infusion and found that infliximab shortened fever duration and length of stay with a similar coronary outcome, which has shifted practice toward infliximab as a first second-line agent in many centres. The original infliximab case series in refractory disease established its tolerability and effect. [8] [7]
Children who are resistant to second-line therapy, or who present with an aneurysm at diagnosis, may need more intensive regimens. Corticosteroids — as pulses of methylprednisolone or longer courses — have a role, especially combined with IVIG in high-risk patients or as escalation in refractory disease. Other adjuncts used in multi-refractory disease include ciclosporin, the interleukin-1 receptor antagonist anakinra, the tumour necrosis factor blocker etanercept (tested as a primary adjunct in a randomised trial), the interleukin-6 blocker tocilizumab, and plasma exchange. These are specialist decisions, usually made in a tertiary paediatric cardiology or rheumatology service. [14] [6]
For children with established coronary aneurysms, anti-thrombotic therapy is matched to severity. Small aneurysms are managed with low-dose aspirin alone. Medium aneurysms often warrant aspirin plus an anti-platelet agent such as clopidogrel, and giant aneurysms require anticoagulation with warfarin or a direct oral anticoagulant in addition to anti-platelet therapy, because the thrombotic risk is high. The aim is to prevent the catastrophic complication of coronary thrombosis and myocardial infarction. [1] [12]
Specific Subtypes & Scenarios
Incomplete Kawasaki disease is the subtype that catches out the unwary, because the child does not meet full criteria yet carries at least as much coronary risk. It is most common in infants under six months and in older children, and the AHA guidance is explicit: in a child with fever and two or three features, treat on the basis of supportive laboratory criteria and echocardiographic findings rather than waiting for the full clinical picture to emerge. [1] [11]
IVIG-resistant disease is the scenario that demands prompt escalation. Persistent or recurrent fever 36 to 48 hours after IVIG identifies the fifteen per cent or so of children who do not respond, and these children have the highest rate of coronary aneurysms. The pathway is a second IVIG or infliximab, with repeat echocardiography and close monitoring of inflammatory markers, and onward escalation for multi-refractory disease. [6] [8]
Giant coronary aneurysm is the most dangerous subtype of coronary involvement. Defined by a z-score of ten or more or an absolute diameter of at least eight millimetres, it carries a high risk of thrombosis, myocardial infarction and sudden death, often regresses poorly, and may progress to stenotic lesions over years. Management combines anticoagulation with anti-platelet therapy, frequent imaging, and a low threshold for investigation of any cardiac symptom. [13] [12]
The adolescent or young adult with a remote history of Kawasaki disease and coronary aneurysms is a growing population in adult congenital and cardiology clinics. They may present with exertional chest pain, syncope or arrhythmia as the first sign of coronary stenosis, and they need urgent evaluation with electrocardiography, troponin, echocardiography and often coronary angiography or computed tomography. Structured transition from paediatric to adult cardiac care prevents the dangerous "lost to follow-up" gap in early adulthood. [12] [13]
Complications & Pitfalls
The complications divide into the cardiovascular, which dominate, and the non-cardiovascular, which are usually self-limited. The non-cardiovascular complications include hydrops of the gallbladder, sterile pyuria, anterior uveitis, arthritis, aseptic meningitis and transient hepatic dysfunction, most of which resolve with the acute illness. The cardiovascular complications are where the long-term stakes lie. [1]
Coronary artery aneurysms are the defining complication. They develop in about a quarter of untreated children and in under five per cent of those treated with IVIG within ten days, and they range from small dilations that regress fully to giant aneurysms that persist and threaten thrombosis. Myocarditis and pericarditis with effusion are common in the acute illness and usually mild, but they can progress to heart failure or shock in the most severe cases, especially where Kawasaki disease overlaps with multisystem inflammatory syndrome. [1] [15]
The risks that drive surveillance
The long-term complications of aneurysms are the source of the lifelong surveillance. Small and medium aneurysms often regress as the vessel wall remodels, but giant aneurysms may narrow into stenotic lesions or develop thrombus, producing myocardial ischaemia or infarction years to decades later. Kawasaki disease is a leading cause of myocardial infarction in young adults with a childhood cardiac history, and any such patient with chest pain or syncope has ischaemia until proven otherwise. Valvular regurgitation, arrhythmia and heart failure round out the late burden. [12] [13]
The common pitfalls are clinical and avoidable. Waiting for the full criteria in incomplete disease delays treatment past the window. Failing to reassess at 36 to 48 hours and missing IVIG-resistant disease lets the inflammation run and the aneurysms form. Discharging a child with aneurysms from follow-up because the acute illness has resolved ignores the long-term risk. And confusing Kawasaki disease with multisystem inflammatory syndrome or a viral exanthem in the pandemic era has driven well-documented delays and missed diagnoses. [11] [1]
[10]Prognosis & Disposition
The prognosis of Kawasaki disease treated promptly is excellent, and it is one of the great success stories of modern paediatric cardiology. Children who receive IVIG within ten days and have normal coronary arteries on serial echocardiography recover fully, stop aspirin at six to eight weeks, and return to routine care with a prognosis essentially the same as the general population. The acute illness is self-limited, and recurrence is uncommon, affecting about three per cent. [1] [9]
The prognosis changes markedly once coronary aneurysms develop. Small aneurysms usually regress and carry a benign outlook, but medium and especially giant aneurysms carry an ongoing risk of thrombosis, stenosis and myocardial infarction that persists for life. The diameter trajectory is predictable in broad terms — aneurysms enlarge in the sub-acute phase, then many regress over one to two years — but giant aneurysms tend to persist and progress, which is why their presence moves a child into high-intensity surveillance and anti-thrombotic therapy indefinitely. [13] [12]
Disposition after the acute illness depends on the coronary status. Children with normal coronaries go home with their family and the local paediatrician, with a final echocardiogram at four to six weeks and a return to normal activities. Children with aneurysms enter a structured surveillance programme that matches imaging frequency and anti-thrombotic intensity to the z-score, and they need a planned transition to adult cardiac care in adolescence. Counselling about fever recurrence, exercise, and the warning signs of ischaemia is part of that disposition. [1]
Special Populations
Infants under six months deserve special attention because they most often present with incomplete disease, are most vulnerable to aneurysms, and are most likely to be missed. A febrile, irritable infant in this age group with raised inflammatory markers and no alternative diagnosis warrants Kawasaki disease on the differential, a full laboratory and echocardiographic workup, and treatment on suspicion. The threshold to treat is lower and the vigilance higher in this group. [1] [11]
Children of East Asian, Pacific and Indigenous heritage carry a higher incidence and may present through communities with more limited access to timely care. Culturally safe assessment, attention to language and health literacy, and a low threshold to treat and refer are part of standard care, and the Australian surveillance data underline the disproportionate burden in these populations. The same principles apply to migrant, refugee and socioeconomically disadvantaged families, for whom the cost and availability of IVIG and echocardiography can be barriers. [9]
The child with multisystem inflammatory syndrome sits at the boundary of Kawasaki disease and demands a coordinated cardiology, rheumatology and intensive-care approach. The overlap is substantial — fever, conjunctivitis, rash, and coronary involvement — but the phenotype skews older, with prominent gastrointestinal and cardiac dysfunction, and management shares the IVIG and aspirin backbone while addressing the multisystem failure. Recognising where the two conditions lie on a spectrum prevents both over- and under-treatment. [15] [11]
The transitioning adolescent and young adult with a history of Kawasaki disease and aneurysms is a defined and growing population. The risks of lost follow-up, unrecognised ischaemia, unplanned pregnancy and non-adherence with anti-thrombotic therapy converge in this group, so structured transition programmes — education, self-management, and a warm handover to adult cardiac care — are now standard and are emphasised in the AHA and CSANZ guidance. [1] [12]
Evidence, Guidelines & Regional Differences
| Region | Key guideline | Second-line agent | Surveillance |
|---|
The two controversies a candidate should be able to discuss are the optimal second-line agent for IVIG-resistant disease and the role of primary adjuncts in high-risk patients. The KIDCARE trial shifted practice toward infliximab as a first second-line agent by showing shorter fever and stay with comparable coronary outcomes, while the choice in multi-refractory disease among corticosteroids, ciclosporin, anakinra, etanercept and plasma exchange remains individualised. Primary adjuncts such as corticosteroids and etanercept are considered for children at the highest baseline risk of aneurysms, and the evidence continues to evolve. [8] [14]
Exam Pearls
References
- [1]McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation, 2017.PMID 28356445
- [2]Newburger JW, Takahashi M, Burns JC, Beiser AS, Chung KJ, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med, 1986.PMID 2426590
- [3]Newburger JW, Takahashi M, Beiser AS, Burns JC, Bastian J, et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med, 1991.PMID 1709446
- [4]Burns JC, Glodé MP Kawasaki syndrome. Lancet, 2004.PMID 15302199
- [5]Dallaire F, Dahdah N New equations and a critical appraisal of coronary artery Z scores in healthy children. J Am Soc Echocardiogr, 2011.PMID 21074965
- [6]Dionne A, Burns JC, Dahdah N Treatment Intensification in Patients With Kawasaki Disease and Coronary Aneurysm at Diagnosis. Pediatrics, 2019.PMID 31048414
- [7]Burns JC, Mason WH, Hauger SB, Janai H, Chen AL, et al. Infliximab treatment for refractory Kawasaki syndrome. J Pediatr, 2005.PMID 15870671
- [8]Burns JC, Roberts SC, Tremoulet AH, Mahle WT, Cuellar TL, et al. Infliximab versus second intravenous immunoglobulin for treatment of resistant Kawasaki disease in the USA (KIDCARE): a randomised, multicentre comparative effectiveness trial. Lancet Child Adolesc Health, 2021.PMID 34715057
- [9]Saundankar J, Yim D, Itotoh B, Payne R, Maslin K, et al. The epidemiology and clinical features of Kawasaki disease in Australia. Pediatrics, 2014.PMID 24685950
- [10]de Graeff N, Groot N, Ozen S, Honold J, Kone-Paut I, et al. European consensus-based recommendations for the diagnosis and treatment of Kawasaki disease - the SHARE initiative. Rheumatology (Oxford), 2019.PMID 30535127
- [11]Harahsheh AS, Dahdah N, Newburger JW, Portman MA, Slee A, et al. Missed or delayed diagnosis of Kawasaki disease during the 2019 novel coronavirus disease (COVID-19) pandemic. J Pediatr, 2020.PMID 32370951
- [12]Ghelani SJ, Baker AL, Friedman K, Tremoulet AH, Shimizu C, et al. Myocardial Infarction in Kawasaki Disease. J Pediatr, 2025.PMID 40368243
- [13]Tsuda E, Hashimoto S Changes in Coronary Aneurysm Diameters After Acute Kawasaki Disease from Infancy to Adolescence. Pediatr Cardiol, 2021.PMID 34132855
- [14]Portman MA, Dahdah NS, Slee A, Berezin S, Walker E, et al. Etanercept With IVIg for Acute Kawasaki Disease: A Randomized Controlled Trial. Pediatrics, 2019.PMID 31048415
- [15]Lee S, Harahsheh AS, Raghuveer G, Hor KN, Altaye M, et al. Spectrum of Coronary Artery Involvement With Multisystem Inflammatory Syndrome in Children Versus Kawasaki Disease. J Am Heart Assoc, 2025.PMID 40265601