Paeds · cardiology
Myocarditis and pericarditis
Also known as Myocarditis · Pericarditis · Myopericarditis · Perimyocarditis · Fulminant myocarditis · Acute pericarditis · Recurrent pericarditis · Post-viral myocarditis
Fellowship guide to acquired inflammatory heart disease in children: myocarditis as inflammation of the cardiac muscle presenting with chest pain, dyspnoea, a raised troponin and arrhythmia, and pericarditis as inflammation of the pericardium presenting with sharp positional chest pain and a friction rub. The page covers the bedside recognition of fulminant myocarditis and tamponade, the diagnostic triad of troponin, electrocardiogram and echocardiogram, the Lake Louise cardiac magnetic resonance criteria, selective immunomodulation (intravenous immunoglobulin and corticosteroids), the newer phenotypes of multisystem inflammatory syndrome in children and mRNA vaccine myocarditis, and the non-steroidal anti-inflammatory plus colchicine regimen for pericarditis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The idea that organises the whole topic is that myocarditis and pericarditis are acquired inflammatory diseases, not structural congenital defects, and their danger lies in how fast a stable child can deteriorate. A school-age child with a viral prodrome and new chest pain can look well and then develop fulminant heart failure or tamponade within hours, so the bedside job is to risk-stratify aggressively rather than to reassure on the basis of a normal examination. [2] [3]
This page covers the recognition and resuscitation of both conditions, the diagnostic pathway of troponin, electrocardiogram and echocardiogram with cardiac magnetic resonance confirmation, the selective use of immunomodulation for myocarditis, the anti-inflammatory regimen for pericarditis, and the newer phenotypes of multisystem inflammatory syndrome in children and mRNA vaccine myocarditis that now dominate the differential in the adolescent. It links to the dilated cardiomyopathy and heart failure leaves for the chronic consequences and to the chest pain leaf for the broader differential. [1] [9]
Overview & Definition
Myocarditis is an inflammatory disease of the myocardium confirmed by clinical, imaging or histological criteria. The heart muscle is infiltrated by inflammatory cells, which injure myocytes through direct viral damage and through the host immune response, producing systolic and diastolic dysfunction and a propensity to arrhythmia. The American Heart Association scientific statement frames it as a clinically suspected syndrome supported by a raised troponin, electrocardiographic changes, imaging abnormalities or biopsy evidence. [1] [3]
Pericarditis is inflammation of the pericardial sac, usually producing a sharp, pleuritic chest pain that eases on sitting forward and worsens on lying back, often with a pericardial friction rub and diffuse electrocardiographic ST elevation. The danger is not the inflammation itself but the pericardial effusion it generates: when fluid accumulates faster than the pericardium can stretch, the heart is compressed and cardiac tamponade follows. The two diseases overlap often, because the visceral pericardium is the epicardium, giving the combined entity myopericarditis. [2] [12]
What makes these conditions hard is that the presentation is nonspecific, especially in infants and young children who cannot describe chest pain. A toddler may simply be tachypnoeic, irritable and off feeds, and the cardiac cause is missed because the clinician attributes the picture to a viral respiratory illness. The discipline that saves these children is to add a troponin and an electrocardiogram to the work-up of any child with unexplained tachypnoea, tachycardia or poor perfusion after a viral illness, and to examine for the friction rub and the signs of tamponade in any child with chest pain. [1] [2]
Classification
Sort inflammatory heart disease by which layer of the heart is inflamed and by the clinical course, because these two axes set the urgency and the treatment. The figure below splits acquired inflammatory cardiac disease into myocarditis, pericarditis and their overlap, and within myocarditis sorts by course (acute, fulminant, chronic) and by cause. [1] [3]
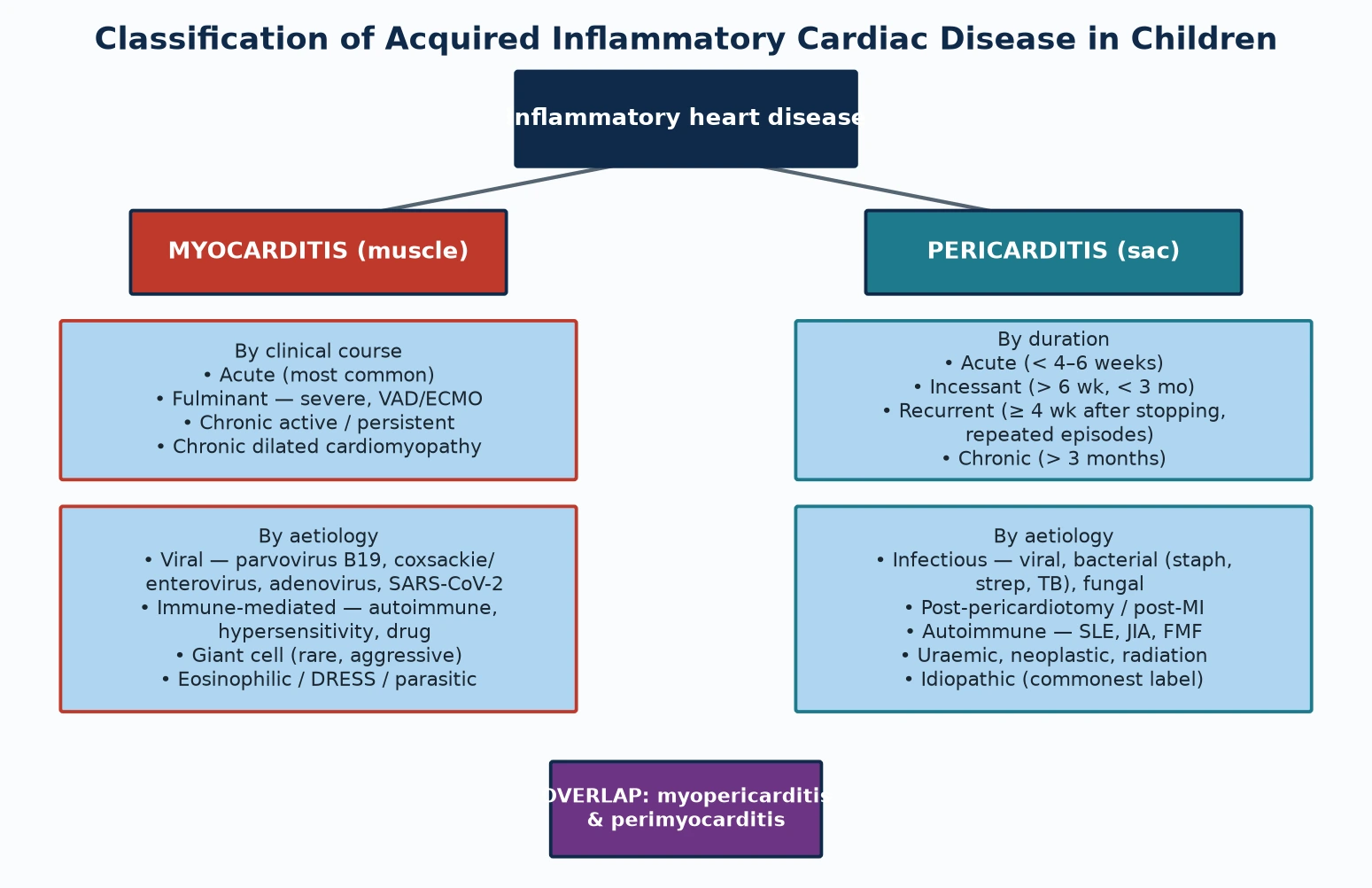
Fulminant myocarditis deserves its own slot because the label changes the prognosis as well as the management. It is defined by severe acute heart failure with cardiogenic shock developing within days of a viral illness, with fever and a marked inflammatory response. The paradox that candidates must hold is that fulminant myocarditis, despite its alarming presentation, often carries a better full-recovery rate than non-fulminant acute myocarditis, provided the child is supported through the acute storm with inotropes and, when needed, mechanical circulatory support. [3] [8]
Pericarditis sorts by duration because duration drives the treatment and the recurrence risk. Acute pericarditis lasts under four to six weeks. Recurrent pericarditis returns after a symptom-free interval off treatment and is the dominant long-term burden for adolescents, where colchicine and, in resistant cases, an interleukin-one blocker transform the outlook. Chronic disease, lasting beyond three months, raises constriction and needs a different work-up. [13] [14]
Myocarditis (muscle)
- Inflammation of the myocardium — raised troponin, dysfunction, arrhythmia
- Course: acute, fulminant (shock), chronic (dilated cardiomyopathy)
- Viral cause dominant: parvovirus B19, coxsackie/enterovirus, SARS-CoV-2
- Treatment is supportive; immunotherapy is selective, not routine
Pericarditis (sac)
- Inflammation of the pericardium — positional pleuritic pain, friction rub
- Duration: acute under 6 weeks, recurrent, chronic over 3 months
- Idiopathic and viral commonest; autoimmune and post-surgery important
- Treatment is NSAID plus colchicine; tamponade needs pericardiocentesis
Overlap & special types
- Myopericarditis: both layers inflamed — troponin raised plus ST elevation
- Giant cell myocarditis: rare, aggressive, needs biopsy and immunosuppression
- MIS-C: post-COVID hyperinflammation with coronary and myocardial involvement
- mRNA vaccine myocarditis: adolescent males, mild, self-limiting course
Epidemiology & Risk Factors
Myocarditis is one of the commoner causes of sudden cardiac death in older children and young athletes, which is why it carries a weight out of proportion to its incidence. True population incidence is hard to pin down because mild cases never reach a cardiologist, but autopsy series place myocarditis behind a meaningful fraction of sudden deaths in the young. The burden falls most on infants, adolescents and young adults, and there is a male predominance. [1] [3]
The dominant trigger worldwide is viral. Historically enteroviruses, especially coxsackie B, headed the list; parvovirus B19, adenovirus, human herpesvirus 6 and Epstein-Barr virus all contribute, and since 2020 SARS-CoV-2 has joined them both directly and through multisystem inflammatory syndrome in children. Bacterial, rickettsial, fungal and parasitic causes (such as Trypanosoma cruzi in endemic regions) are less common but region-dependent. Non-infectious triggers include autoimmune disease, drug hypersensitivity and toxins. [2] [9]
Pericarditis is the most common pericardial disease of childhood and adolescence. Most paediatric cases are labelled idiopathic after infection is excluded, but viral infection, autoimmune disease (systemic lupus erythematosus, juvenile idiopathic arthritis, familial Mediterranean fever), recent cardiac surgery, uraemia and malignancy account for a substantial minority. Recurrence is the rule rather than the exception without colchicine, with up to a third of patients relapsing after a first episode. [12] [13]
The reason the epidemiology matters at the bedside is that it tells the clinician when to suspect the diagnosis. A school-age child or adolescent who presents a week or two after a febrile illness with new chest pain, breathlessness or palpitations sits squarely in the high-risk window, and so does the febrile infant with unexplained tachycardia disproportionate to the fever. Recognising these patterns triggers the troponin and electrocardiogram that catch the disease early. [2] [9]
Pathophysiology
To see why a child with myocarditis deteriorates, picture the injured myocardium as a pump under autoimmune attack. A virus enters the myocyte through receptors such as the coxsackie-adenovirus receptor and replicates, directly damaging the cell and releasing antigen. The host immune response then does most of the lasting harm: cytotoxic T-cells, macrophages and cytokines infiltrate the muscle, autoantibodies form against cardiac proteins, and the inflammation that was meant to clear the virus instead destroys functioning myocardium. [3] [9]
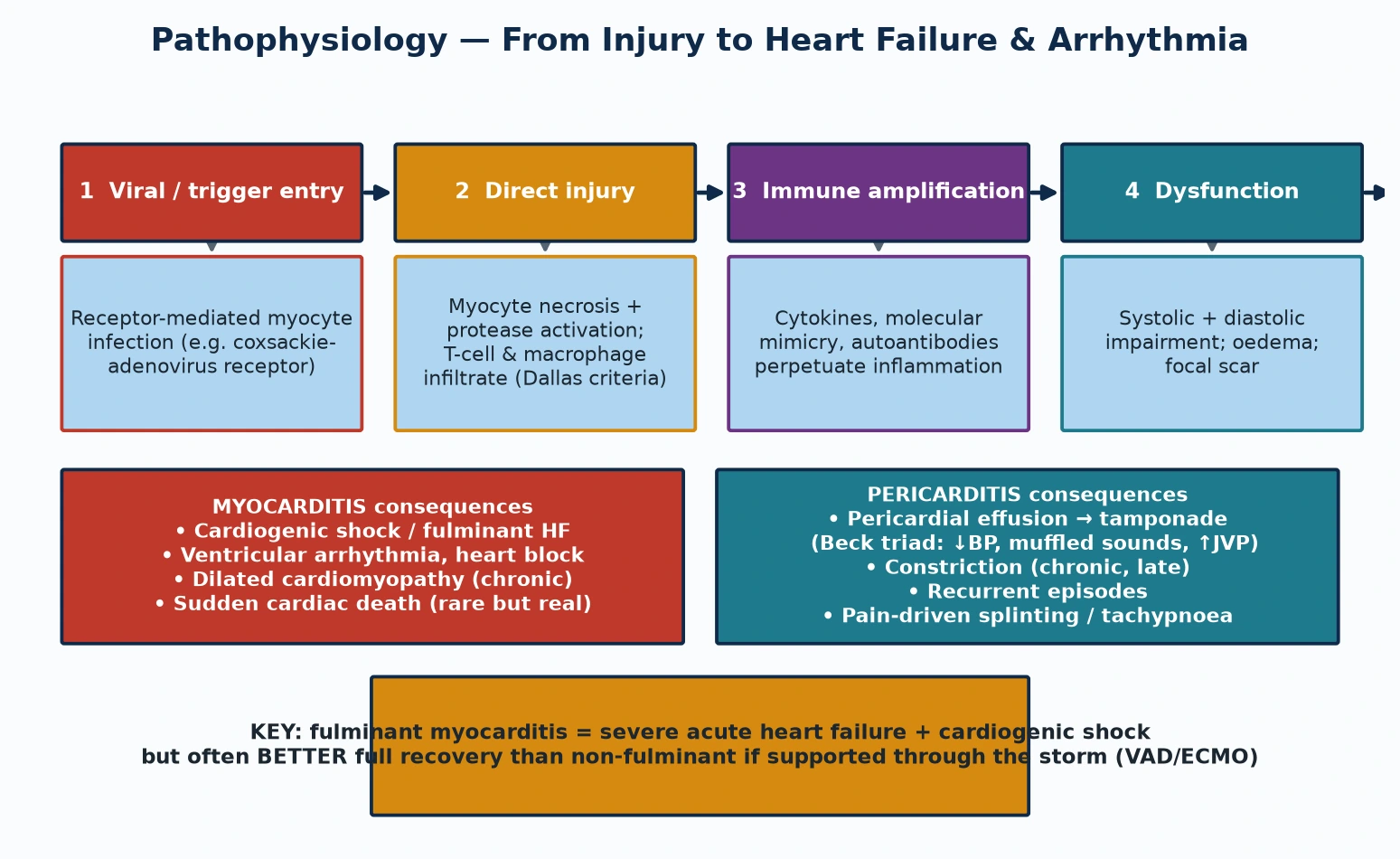
The dysfunction that follows has two parts. Systolic failure — weak pumping — drives the low-output state, gallop rhythm and hepatomegaly of heart failure. Diastolic stiffness from oedema and scar compounds it, and the inflamed myocardium becomes electrically unstable, generating ventricular ectopy, heart block and, rarely, sustained ventricular tachycardia that can arrest the child. The histological counterpart is the Dallas criteria pattern of inflammatory infiltrate with myocyte necrosis, now supplemented by immunohistochemistry and viral genome detection on biopsy. [1] [3]
Pericarditis works by a different but related mechanism. The inflamed pericardium produces fluid, and as the effusion grows the intrapericardial pressure rises. The pericardium is relatively non-compliant in the short term, so a rapidly accumulating effusion — even a modest one — can compress the heart and produce tamponade before the sac has time to stretch. This is why a small but rapidly formed effusion is more dangerous than a large chronic one, and why the bedside sign to watch for is the rise in jugular venous pressure with falling blood pressure and a paradoxical pulse. [15] [12]
The paradoxic recovery of fulminant myocarditis comes from its pathophysiology. Fulminant disease is dominated by a massive but acute inflammatory oedema rather than permanent myocyte loss, so once the child is supported through the hours to days of haemodynamic collapse the oedema resolves and contractile function can return to near-normal. This is the mechanistic reason that a child on ECMO for fulminant myocarditis can walk out of hospital with a normal ejection fraction — a recovery story that does not apply to the smouldering non-fulminant form that more often progresses to dilated cardiomyopathy. [8] [3]
Clinical Presentation
A child with myocarditis presents on a spectrum from a mild influenza-like illness with chest discomfort to fulminant cardiovascular collapse, and the challenge is that the early end of that spectrum looks like every other viral illness. The classic history is a viral prodrome of fever, myalgia and respiratory or gastrointestinal symptoms, followed days later by chest pain, breathlessness, palpitations or exercise intolerance. Infants and toddlers cannot report chest pain, so they present with poor feeding, tachypnoea, lethargy, pallor and mottling, and the cardiac cause is easily missed. [1] [2]
Examination of the myocarditic child shows tachycardia out of proportion to the fever, a gallop rhythm, a soft first heart sound, and signs of heart failure such as hepatomegaly, cool peripheries and a prolonged capillary refill. A murmur of mitral or tricuspid regurgitation may appear as the ventricle dilates. The dangerous examination is the child who looks well but has ventricular ectopy on monitoring, or who tips into cardiogenic shock with hypotension, oliguria and a rising lactate — the fulminant presentation that demands immediate escalation. [3] [8]
Pericarditis declares itself with chest pain that is sharp, pleuritic and positional — worse on lying back or deep inspiration and eased by sitting forward and leaning over. The pathognomonic bedside sign is the pericardial friction rub, a superficial scratching or leather-grating sound with up to three components, heard best at the left sternal edge with the child sitting forward and holding breath in expiration. A large effusion muffles the heart sounds and narrows the pulse pressure, and tamponade adds a raised jugular venous pressure, tachycardia and pulsus paradoxus. [2] [12]
The presentation also now includes the newer syndromes. An adolescent boy presenting within a week of an mRNA coronavirus vaccine with chest pain and a raised troponin has vaccine-associated myocarditis or pericarditis until excluded — typically mild and self-limiting, but it must be distinguished from spontaneous viral disease. And a febrile child two to six weeks after coronavirus disease with conjunctivitis, rash, abdominal pain and cardiovascular instability has multisystem inflammatory syndrome in children until proven otherwise, because its cardiac involvement drives both the acute risk and the long-term coronary surveillance. [11] [10]
Differential Diagnosis
The differential splits into the causes of chest pain with a raised troponin, the causes of acute heart failure, and the causes of pericardial effusion. In the older child with exertional chest pain and a raised troponin, the diagnosis that must not be missed is an anomalous origin of the left coronary artery from the pulmonary artery in the infant, or an anomalous coronary course in the adolescent, because these are surgically correctable and present with ischaemic electrocardiographic changes. Pulmonary embolism, pneumothorax and oesophageal reflux round out the chest-pain differential. [2] [3]
Points to myocarditis
- Viral prodrome then chest pain, dyspnoea, palpitations
- Gallop rhythm, tachycardia disproportionate to fever
- Raised troponin with global electrocardiographic changes
- Reduced ventricular function on echocardiogram
Points to pericarditis
- Sharp positional pleuritic pain eased by sitting forward
- Pericardial friction rub at the left sternal edge
- Diffuse ST elevation and PR depression on ECG
- Pericardial effusion without major dysfunction
Points to a mimic
- Anomalous coronary artery — ischaemic, regional ECG changes
- Pulmonary embolism — hypoxia, right-heart strain
- Sepsis with myocardial depression — uniformly unwell
- Kawasaki disease — fever, coronary aneurysms, rash
For the child presenting in cardiogenic shock, the bedside question is whether this is fulminant myocarditis or a structural cause such as a ductal-dependent lesion in the neonate or a cardiomyopathy. The pulse pattern helps: myocarditis gives a narrow pulse pressure with cool peripheries and a gallop, whereas ductal-dependent disease gives differential saturations or weak femoral pulses. Echocardiography resolves most of this at the bedside and should be obtained early, before the child is moved. [3] [8]
In the child with a pericardial effusion, separate the benign viral or idiopathic effusion from purulent bacterial pericarditis, which is a surgical and antibiotic emergency, and from the effusion of autoimmune disease or uraemia. Fever with toxicity, a marked inflammatory response and a loculated effusion point to purulent disease and warrant pericardiocentesis for both diagnosis and drainage. Missing a purulent pericarditis by labelling it idiopathic is a classic and dangerous error. [12] [15]
Clinical & Bedside Assessment
The focused assessment rests on three bedside manoeuvres and the discipline to add cardiac blood tests to any unwell child after a viral illness. Look hard for the friction rub in any child with chest pain, by examining the child sitting forward and leaning over, holding the breath in expiration, listening at the left lower sternal edge. The rub is evanescent — it comes and goes — so its absence on one examination does not exclude pericarditis; listen again. [2] [12]
In suspected myocarditis, assess perfusion and the haemodynamic state in detail, because the severity of shock sets the urgency. Look for the gallop rhythm, hepatomegaly, cool peripheries, weak pulses and a prolonged capillary refill that mark low cardiac output, and measure the blood pressure, the respiratory rate and the oxygen saturation in all limbs. Tachycardia that does not settle with fever control or fluid, or that is disproportionate to the clinical picture, is a red flag for a myocarditic pump. [1] [3]
For the child with a pericardial effusion, examine specifically for tamponade. The Beck triad of hypotension, raised jugular venous pressure and muffled heart sounds is the classical cluster, and pulsus paradoxus — a fall in systolic blood pressure of more than ten millimetres of mercury on inspiration — is the confirmatory bedside sign. A child with clinical tamponade needs emergency pericardiocentesis rather than further imaging, because the diagnosis is made at the bedside and the treatment relieves the compression before it arrests the circulation. [15] [12]
Examine for the stigmata of the systemic diseases that cause pericarditis and myocarditis. A malar rash, arthritis and oral ulcers suggest systemic lupus erythematosus. Recurrent fevers with serositis and a family history point to familial Mediterranean fever, where colchicine is both diagnostic and therapeutic. Persistent fever, conjunctivitis, strawberry tongue and a polymorphous rash suggest Kawasaki disease, which brings coronary aneurysms into the differential. These findings change both the cardiac and the systemic management. [13] [9]
Investigations
The diagnostic backbone is the triad of troponin, electrocardiogram and echocardiogram, with cardiac magnetic resonance as the non-invasive gold standard when the child is stable enough. Troponin, ideally a high-sensitivity assay, is the most sensitive single marker of myocardial injury and should be sent in any child with suspected myocarditis; a normal troponin makes clinically significant myocarditis unlikely, while a markedly raised troponin with compatible features makes the diagnosis likely even before imaging. [1] [3]
The electrocardiogram is abnormal in most children with myocarditis but the changes are nonspecific — ST-segment changes, T-wave inversion, low voltages, conduction delay and arrhythmia. In pericarditis the pattern is more characteristic: diffuse concave ST elevation and PR-segment depression across multiple leads, evolving through stages. The electrocardiogram also catches the dangerous rhythm consequences of myocarditis — complete heart block, ventricular ectopy and sustained ventricular tachycardia — which is why continuous cardiac monitoring is mandatory from the moment myocarditis is suspected. [2] [13]
Echocardiogram
- Bedside, repeatable, defines ventricular function and effusion
- Shows regional or global dysfunction, valve regurgitation, thrombus
- Quantifies any pericardial effusion and tamponade physiology
- Normal echo does not exclude myocarditis — tissue may be inflamed but function preserved
Cardiac MRI (Lake Louise)
- Non-invasive gold standard for tissue characterisation
- Lake Louise criteria: oedema, late gadolinium enhancement, hyperaemia
- Confirms myocarditis when echo and troponin are equivocal
- Patchy mid-wall or subepicardial enhancement favours myocarditis over ischaemia
Endomyocardial biopsy
- Historical gold standard — Dallas criteria of inflammatory infiltrate and necrosis
- Now reserved for fulminant disease, suspected giant cell or eosinophilic myocarditis
- Adds immunohistochemistry and viral polymerase-chain-reaction for the cause
- Not routine because of sampling error and procedural risk
Echocardiography is the first imaging test and is obtained at the bedside. It defines the left and right ventricular function (global or regional hypokinesis supports myocarditis), excludes structural lesions, detects valve regurgitation and intracardiac thrombus, and quantifies any pericardial effusion with its haemodynamic effect. A normal echocardiogram does not exclude myocarditis, because early inflammation may coexist with preserved systolic function; this is the gap that cardiac magnetic resonance fills. [15] [2]
Cardiac magnetic resonance is the non-invasive reference standard for myocarditis in the stable child. The updated Lake Louise criteria combine tissue oedema, late gadolinium enhancement and hyperaemia to confirm inflammation, and the pattern of patchy mid-wall or subepicardial enhancement — often in the lateral or inferolateral wall — distinguishes myocarditis from ischaemic injury. Endomyocardial biopsy retains a narrow but vital role, reserved for fulminant disease, suspected giant cell or eosinophilic myocarditis, and failure to respond to therapy, where immunohistochemistry and viral genome detection change the immunosuppressive plan. [4] [5]
Management — Resuscitation
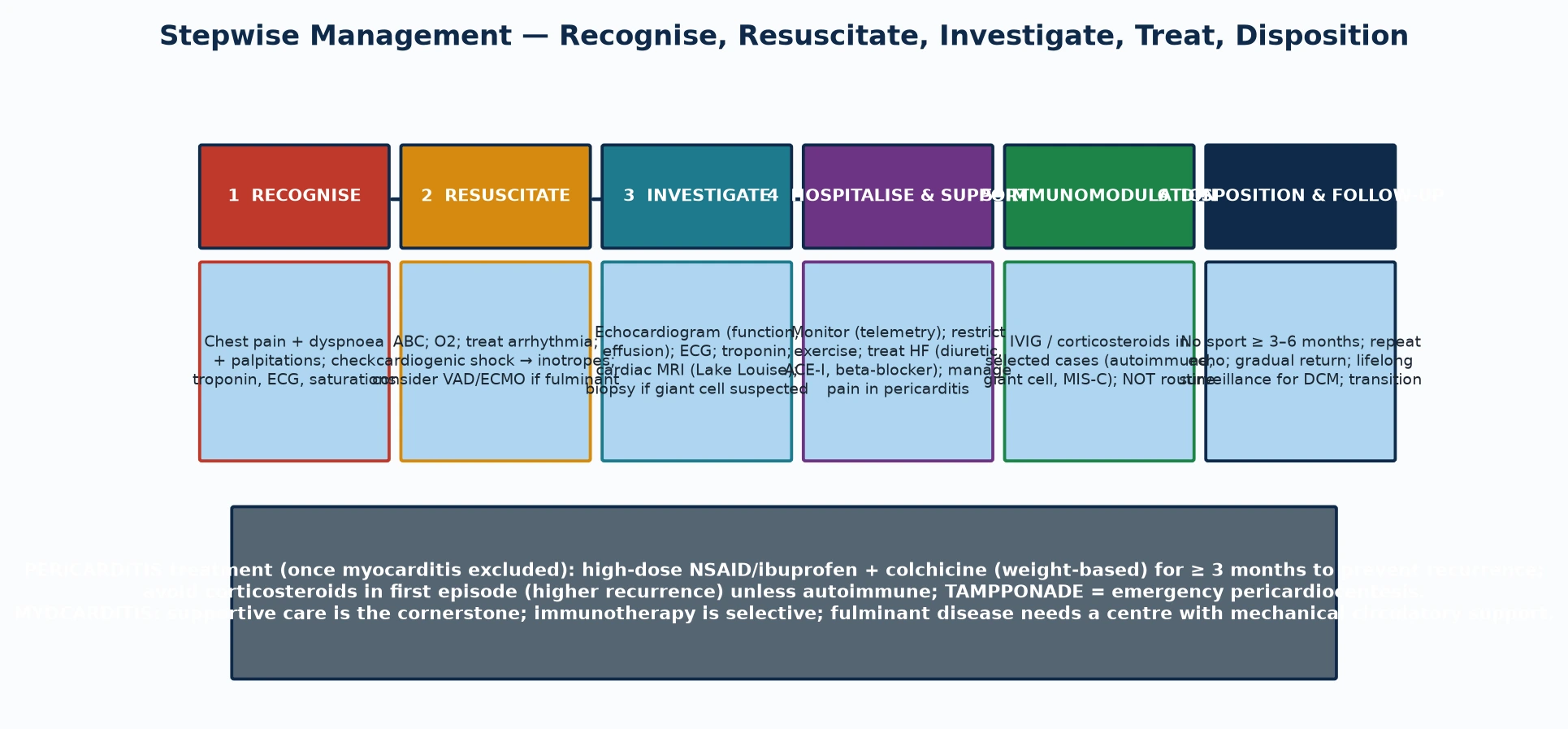
Resuscitation of the child with suspected myocarditis starts with the airway, breathing and circulation and an honest assessment of how sick the child is. Any child with cardiogenic shock, a ventricular arrhythmia or high-degree heart block belongs in a paediatric intensive care unit with continuous monitoring and immediate access to inotropes and mechanical circulatory support, because the transition from compensated to decompensated shock can be rapid and unpredictable. Early discussion with a retrieval and cardiac centre is mandatory. [8] [1]
Treat arrhythmia promptly. Ventricular tachycardia is treated with synchronised cardioversion and antiarrhythmic therapy, and complete heart block may need temporary pacing. Correct electrolytes, especially potassium and magnesium, because the inflamed myocardium is electrically irritable. Give oxygen and ventilatory support for respiratory distress or shock, and use cautious fluid resuscitation only — a volume-loaded, inflamed ventricle tolerates boluses poorly, and small aliquots guided by perfusion and lactate are safer than a standard bolus. [3] [8]
Inotropic support drives the resuscitation of the low-output myocarditic heart. Agents such as milrinone, dobutamine or low-dose adrenaline improve contractility and perfusion while the inflammation resolves, titrated to the clinical state and the lactate trend. When medical support fails to restore perfusion — the definition of refractory cardiogenic shock in fulminant myocarditis — early mechanical circulatory support with venoarterial extracorporeal membrane oxygenation or a ventricular assist device is the bridge to recovery or transplant, and the evidence shows that early deployment saves lives. [8] [3]
Management — Definitive & Stepwise
Definitive management of myocarditis is predominantly supportive, and the candidate must hold this clearly: rest the heart, support the circulation, treat the arrhythmia, and reserve specific immunotherapy for selected indications. Activity restriction — no competitive sport or strenuous exercise for three to six months — is non-negotiable, because exercise during the inflammatory phase increases the risk of sudden death. Heart failure therapy with diuretics, an angiotensin-converting-enzyme inhibitor and a beta-blocker is introduced once the child is stable, guided by ventricular function. [1] [3]
The role of immunomodulation is selective, and this is where most candidates over-treat in the exam. Intravenous immunoglobulin and corticosteroids are not routinely indicated for uncomplicated viral myocarditis — the Cochrane review finds no firm evidence of benefit for intravenous immunoglobulin, and the meta-analysis of corticosteroids and immunoglobulin in children shows possible benefit without conclusive proof. They earn their place in autoimmune myocarditis, giant cell myocarditis, eosinophilic disease and multisystem inflammatory syndrome in children, where the immune mechanism justifies immunosuppression. Matching the immunotherapy to the mechanism is the skill. [6] [7]
Pericarditis is treated once myocarditis is excluded, and the regimen is highly effective: a high dose of a non-steroidal anti-inflammatory drug such as ibuprofen for the inflammation, combined with weight-based colchicine to prevent recurrence, continued for at least three months. Corticosteroids are avoided in a first idiopathic episode because they increase the recurrence rate, and are reserved for autoimmune disease or colchicine-resistant recurrence where an interleukin-one antagonist such as anakinra is now an evidence-backed option. Tamponade and purulent disease are managed with pericardiocentesis and, for purulent pericarditis, surgical drainage and targeted antibiotics. [13] [14]
Specific Subtypes & Scenarios
Fulminant myocarditis is the scenario that tests acute decision-making. A previously well child develops severe heart failure and cardiogenic shock within days of a viral illness, with fever, a marked inflammatory response and ventricular dysfunction on imaging. The management is early escalation to a centre with mechanical circulatory support, because venoarterial extracorporeal membrane oxygenation or a ventricular assist device bridges the child to recovery, and the recovery is often complete. The pitfall is delaying support while waiting for biopsy confirmation. [8] [3]
Multisystem inflammatory syndrome in children is the post-coronavirus phenotype that now dominates the paediatric cardiology differential. A child presents two to six weeks after coronavirus disease with persistent fever, multisystem involvement — gastrointestinal, mucocutaneous, neurological — and cardiac dysfunction driven by a hyperinflammatory, vasculitic process. Troponin and pro-brain natriuretic peptide are raised, the echocardiogram shows dysfunction and sometimes coronary changes, and the management is multidisciplinary with immunomodulation (immunoglobulin, corticosteroids, sometimes biologics) and low-dose aspirin. Coronary surveillance at follow-up is mandatory. [9] [10]
mRNA vaccine-associated myocarditis and pericarditis is the adolescent scenario that tests balanced counselling. Adolescent and young-adult males, most often within a week of a second dose of an mRNA coronavirus vaccine, present with chest pain and a raised troponin. The course is typically mild and self-limiting with supportive care, and the benefit of vaccination outweighs the small risk, but the diagnosis must be confirmed and the child excluded from sport during recovery. The candidate must present the risk honestly without either dismissing it or over-stating it. [11] [3]
Recurrent pericarditis in the adolescent is the chronic scenario that tests long-term management. After a first episode, up to a third of patients relapse, often repeatedly, with each attack responding to non-steroidal anti-inflammatory drugs but the recurrences becoming the dominant burden. Colchicine for at least three months reduces recurrence substantially, and an interleukin-one blocker such as anakinra is now an evidence-backed option for colchicine-resistant disease. Avoiding corticosteroids in the first episode is part of prevention, because steroids raise the recurrence rate. [13] [14]
Complications & Pitfalls
The untreated or unrecognised myocarditis carries the heaviest burden: progression to dilated cardiomyopathy, sustained ventricular arrhythmia and sudden cardiac death. Many of these are preventable with early recognition, activity restriction and escalation, which is why the single biggest modifiable factor is the speed of diagnosis and the discipline of taking a troponin in the unwell child after a viral illness. [1] [3]
After the acute illness, the dominant complications are persistent ventricular dysfunction, the evolution to dilated cardiomyopathy, exercise-related arrhythmia and the psychological burden of an exercise restriction on a child or adolescent. Recurrent pericarditis is the dominant complication of pericardial disease, and constrictive pericarditis — late scarring that impedes filling — is the rarer but serious long-term consequence that needs pericardiectomy. [13] [12]
The treatment carries its own pitfalls. Missing fulminant myocarditis by reassurance of a borderline examination delays the mechanical support that reverses the course. Treating uncomplicated viral myocarditis with immunoglobulin or steroids routinely exposes children to therapy without proven benefit and obscures the selective indications. Labelling a purulent pericardial effusion as idiopathic denies the child the antibiotics and drainage that the infection demands. Returning a child to competitive sport too early courts exercise-related sudden death during the vulnerable inflammatory window. Each is an avoidable harm rooted in forgetting the disease's behaviour. [8] [6]
Prognosis & Disposition
The prognosis of paediatric myocarditis is bimodal, and candidates must hold both ends. Most children with mild acute myocarditis recover fully with supportive care, and fulminant myocarditis — despite its alarming presentation — often recovers near-normal function when supported through the acute storm with mechanical circulatory support. The minority progress to chronic dilated cardiomyopathy, with its attendant heart-failure trajectory and, in some, the need for transplant. Early and complete recovery is the common story, but the dilated-cardiomyopathy trajectory is the reason for lifelong surveillance. [1] [3]
Pericarditis has an excellent prognosis for the acute episode but a substantial recurrence burden. With a non-steroidal anti-inflammatory drug plus colchicine, most acute episodes settle within days to weeks, and colchicine markedly lowers the recurrence rate. The outlook for recurrent disease has improved further with interleukin-one blockade. The rarer long-term concerns are constrictive pericarditis and, for purulent disease, the consequences of delayed drainage. [13] [14]
Disposition depends on severity. Any child with cardiogenic shock, a significant arrhythmia, or moderate to severe ventricular dysfunction is managed in a paediatric intensive care unit with cardiac support, and fulminant disease is managed in a centre with mechanical circulatory support and transplant capability. Mild myocarditis and uncomplicated pericarditis are managed on the ward or as an outpatient with close follow-up. The general paediatrician's role is to recognise the disease early, escalate appropriately, and then champion the activity restriction and surveillance that protect the recovering heart. [2] [12]
Special Populations
Infants and toddlers present the greatest diagnostic challenge, because they cannot describe chest pain and present with nonspecific feeding difficulty, tachypnoea and lethargy that mimic a respiratory virus. The discipline here is to add a troponin and an electrocardiogram to the work-up of any infant with unexplained tachycardia disproportionate to fever, and to escalate the infant with poor perfusion to a cardiac assessment without delay. Enteroviral neonatal myocarditis is particularly severe and may present with sepsis-like collapse and multiorgan failure. [2] [1]
Adolescents and young athletes carry the sudden-death risk that makes activity restriction non-negotiable. The drive to return to competitive sport is strong, so the clinician must be explicit that no competitive sport or strenuous training is permitted for three to six months and until the troponin, electrocardiogram and imaging have normalised. The mRNA vaccine myocarditis phenotype sits in this group, and honest, balanced counselling about the small risk versus the larger benefit of vaccination is part of the encounter. [11] [3]
Children with multisystem inflammatory syndrome need integrated cardiac and rheumatological or infectious-disease care, because the hyperinflammation drives both the acute cardiac dysfunction and the coronary surveillance. Immunocompromised children and those from remote or Indigenous communities face the dual burden of more severe infectious triggers and the logistics of access to tertiary cardiac and intensive-care services, so a clear retrieval pathway, telehealth follow-up and cultural support are essential parts of the disposition, alongside the low-dose aspirin and immunomodulation that the syndrome demands. [9] [10]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric myocarditis is anchored in the American Heart Association scientific statement of Law and colleagues (2021), which sets out the diagnostic criteria and the supportive-first management philosophy. The review of Ammirati and colleagues in the Journal of the American Medical Association (2023) and the paediatric review of Tunuguntla and colleagues (2019) cover the practical bedside approach. The Lake Louise magnetic resonance criteria — the original white paper of Friedrich and colleagues (2009) and the updated expert recommendations of Ferreira and colleagues (2018) — define the non-invasive tissue diagnosis. [1] [4]
The pericarditis evidence rests on the systematic review of Imazio and colleagues in the Journal of the American Medical Association (2015), which established the non-steroidal-anti-inflammatory-plus-colchicine regimen and the corticosteroid-avoidance principle, and the paediatric pericarditis update of Shahid and colleagues (2023) and the colchicine systematic review of Alsabri and colleagues (2025). The Kwon review (2021) frames the mechanical circulatory support decision in fulminant paediatric myocarditis. The MIS-C literature — McMurray (2020) and Wu (2021) — and the vaccine myocarditis review of Bozkurt (2021) cover the newer phenotypes. [13] [8]
Regional practice aligns internationally on the supportive-first principle, but the newer phenotypes have introduced regional variation. Australia and New Zealand integrated multisystem-inflammatory-syndrome and mRNA vaccine myocarditis surveillance into their existing paediatric cardiology and public-health pathways, with low-dose aspirin and echocardiographic follow-up embedded in the protocol. Access to paediatric intensive care, retrieval services and mechanical circulatory support varies across remote and regional areas, so early referral and retrieval are emphasised. The main controversies are the routine use of immunoglobulin, the duration of activity restriction, and the intensity of coronary follow-up after multisystem inflammatory syndrome. [11] [10]
Exam Pearls
Hold one sentence for the viva: a child with acute chest pain, breathlessness and a raised troponin after a viral illness has myocarditis until proven otherwise, and the management is supportive with early escalation of any shock or arrhythmia, reserving immunomodulation for autoimmune, giant cell and multisystem-inflammatory-syndrome disease. [1] [3]
State the frequently tested facts correctly. The diagnostic backbone is troponin, electrocardiogram and echocardiogram, with cardiac magnetic resonance (Lake Louise criteria) as the non-invasive gold standard. Endomyocardial biopsy is reserved for fulminant disease and suspected giant cell myocarditis. Fulminant myocarditis paradoxically recovers well when supported mechanically. Pericarditis is treated with a non-steroidal anti-inflammatory drug plus colchicine, avoiding corticosteroids in the first episode. Tamponade is a pericardiocentesis emergency. Multisystem inflammatory syndrome in children follows coronavirus disease by two to six weeks. mRNA vaccine myocarditis affects adolescent males and is usually mild. [2] [12]
The high-yield pairings: a child with chest pain and a friction rub has pericarditis; an unwell child after a virus with a raised troponin has myocarditis; a shocked child with a pericardial effusion and pulsus paradoxus has tamponade; a febrile child two to six weeks after coronavirus disease with multiorgan involvement has multisystem inflammatory syndrome in children; an adolescent boy within a week of an mRNA vaccine with chest pain has vaccine-associated myocarditis. These pairings do most of the diagnostic work in the written and clinical examinations. [13] [9]
References
- [1]Law YM; Lal AK; Chen S; et al Diagnosis and Management of Myocarditis in Children: A Scientific Statement From the American Heart Association. Circulation, 2021.PMID 34229446
- [2]Tunuguntla H; Jeewa A; Denfield SW Acute Myocarditis and Pericarditis in Children. Pediatr Rev, 2019.PMID 30600275
- [3]Ammirati E; Moslehi JJ; et al Diagnosis and Treatment of Acute Myocarditis: A Review. JAMA, 2023.PMID 37014337
- [4]Ferreira VM; Schulz-Menger J; Holmvang G; et al Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J Am Coll Cardiol, 2018.PMID 30545455
- [5]Friedrich MG; Sechtem U; Schulz-Menger J; et al Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol, 2009.PMID 19389557
- [6]Robinson J; Hartling L; Crumley E; et al Intravenous immunoglobulin for presumed viral myocarditis in children and adults. Cochrane Database Syst Rev, 2020.PMID 32835416
- [7]Li Y; Yu Y; Dong R; et al Corticosteroids and Intravenous Immunoglobulin in Pediatric Myocarditis: A Meta-Analysis. Front Pediatr, 2019.PMID 31475124
- [8]Kwon HW When should mechanical circulatory support be considered in pediatric patients with acute fulminant myocarditis? Clin Exp Pediatr, 2021.PMID 32972050
- [9]McMurray JC; May JW; Cunningham A; et al Multisystem Inflammatory Syndrome in Children (MIS-C), a Post-viral Myocarditis and Systemic Vasculitis-A Critical Review of Its Pathogenesis and Treatment. Front Pediatr, 2020.PMID 33425823
- [10]Wu EY; Campbell MJ; et al Cardiac Manifestations of Multisystem Inflammatory Syndrome in Children (MIS-C) Following COVID-19. Curr Cardiol Rep, 2021.PMID 34599465
- [11]Bozkurt B; Kamat I; Hotez PJ Myocarditis With COVID-19 mRNA Vaccines. Circulation, 2021.PMID 34281357
- [12]Shahid R; Jin J; Cooper JN; et al Pediatric Pericarditis: Update. Curr Cardiol Rep, 2023.PMID 36749541
- [13]Imazio M; Gaita F; LeWinter M Evaluation and Treatment of Pericarditis: A Systematic Review. JAMA, 2015.PMID 26461998
- [14]Alsabri M; Elsayed SM; Alsahlly A; et al Efficacy and Safety of Colchicine in Pediatric Pericarditis: A Systematic Review and Future Directions. Pediatr Cardiol, 2025.PMID 39080042
- [15]Perez-Casares A; Cesar S; Brunet-Garcia L; et al Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade. Front Pediatr, 2017.PMID 28484689