Paeds · cardiology
Postural orthostatic tachycardia syndrome
Also known as Postural orthostatic tachycardia syndrome · POTS · Postural tachycardia syndrome · Chronic orthostatic intolerance · Orthostatic intolerance · Dysautonomia
Fellowship guide to postural orthostatic tachycardia syndrome (POTS) in young people: chronic daily orthostatic symptoms with an excessive heart-rate rise on standing (≥40 bpm in adolescents, or ≥120 bpm) WITHOUT orthostatic hypotension, the neuropathic/hyperadrenergic/hypovolaemic phenotypes, the 10-minute active stand test, exclusion of cardiac syncope with an ECG on every child, and the stepwise management from fluid and salt to recumbent exercise and then phenotype-guided pharmacotherapy.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
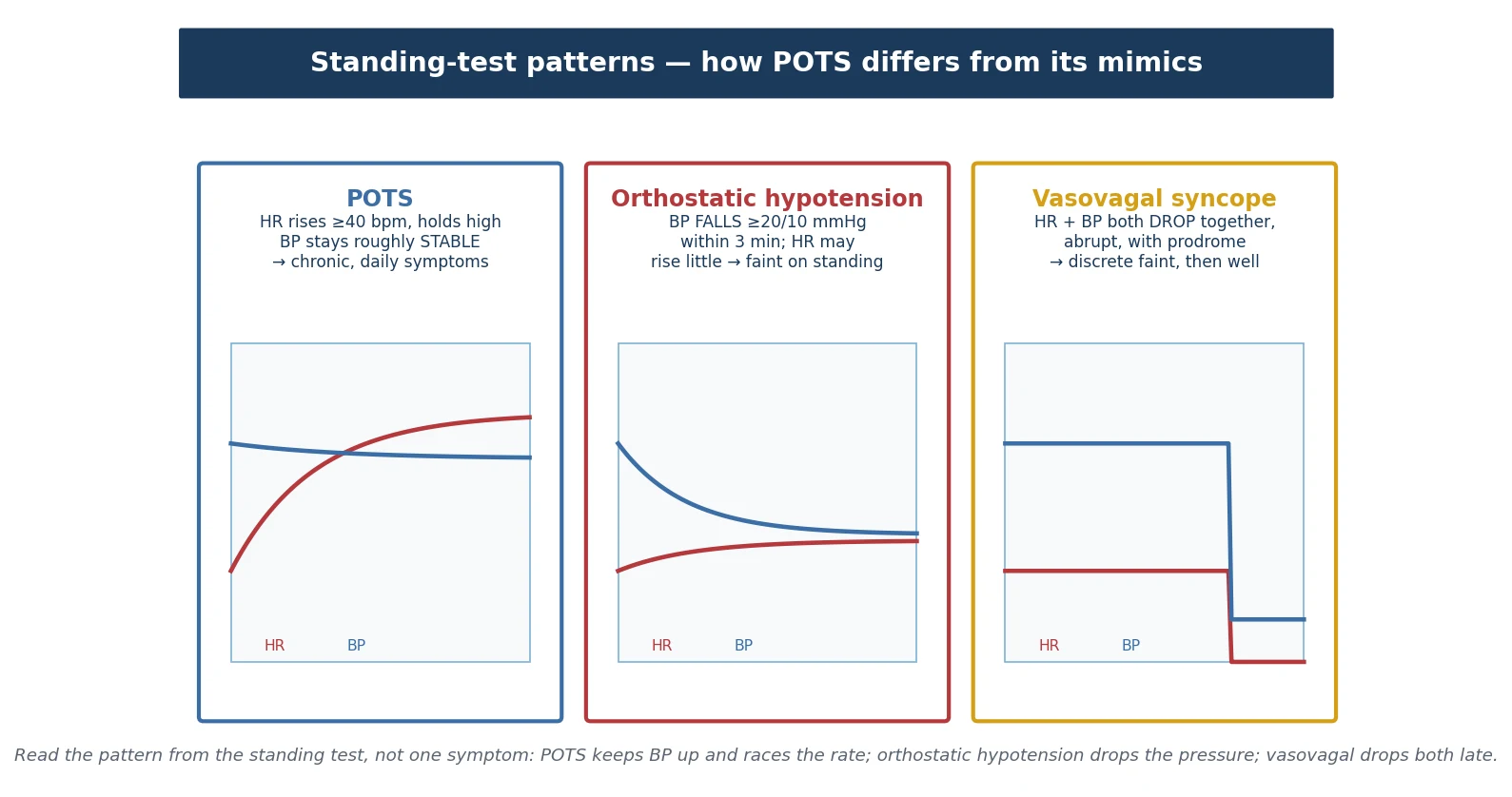
The idea that holds the whole topic together is the standing-test pattern. POTS keeps the blood pressure up and races the heart rate; orthostatic hypotension drops the blood pressure; vasovagal syncope drops both together late. Once you can picture those three patterns, you can place almost any fainting or dizzy adolescent in the right box. [3] [9]
This page covers the definition and the heart-rate threshold, the three overlapping phenotypes, the pathophysiology of an inadequate venous return, the differential that includes cardiac syncope and deconditioning, the ten-minute stand test and when to tilt, the stepwise non-pharmacological then pharmacological management, the deconditioning and school-impact spiral, and the post-viral and post-COVID trigger. It links to the syncope and channelopathy leaves for the cardiac work-up rather than duplicating those pathways. [1] [6]
Overview & Definition
Start with what the family will tell you. Their teenager, often a girl who has always been well, begins to feel dizzy, shaky and exhausted whenever she stands for more than a few minutes. The symptoms ease the moment she lies down. Over weeks they creep into school, sport and social life, and she may have a viral illness or a growth spurt just before it all starts. That daily, posture-driven picture — not a single dramatic faint — is the face of POTS. [5] [9]
The formal definition turns that picture into numbers. POTS is a chronic orthostatic intolerance of at least six months, present most days, in which assuming an upright posture produces a sustained heart-rate rise of at least forty beats per minute in children and adolescents (the adult threshold is thirty), or an upright heart rate of at least one hundred and twenty beats per minute, within ten minutes of standing or head-up tilt, without an orthostatic fall in blood pressure of twenty millimetres of mercury systolic or ten diastolic. [1] [6]
Three parts of that definition carry the whole diagnosis, so they are worth separating. Orthostatic intolerance is the basket of symptoms provoked by standing and eased by lying down — lightheadedness, palpitations, tremor, fatigue, brain fog, nausea, headache, presyncope. Tachycardia is the heart-rate response that defines the syndrome; it is excessive because the blood pressure does not fall, so the heart does not need to race to save it — and yet it does. Chronicity sets the three-month floor, which excludes the transient tachycardia of fever, dehydration, anxiety or a single viral illness. [2] [3]
Why the chronicity matters at the bedside: a frightened, dehydrated or recently febrile child can easily push a standing heart rate above one hundred and twenty, but that is not POTS. Labelling a child prematurely traps them in a chronic diagnosis and starts them on a treatment ladder they do not need. The three-month rule and the requirement for daily symptoms are there to protect against exactly that error. [3] [9]
POTS sits within the wider family of orthostatic intolerance syndromes but is distinguished from its cousins by the heart-rate pattern. It is not vasovagal syncope (an episodic reflex faint with a prodrome), and it is not orthostatic hypotension (a blood-pressure fall). It is its own entity, and the standing test is what tells them apart. [1] [7]
Classification
The most useful way to sort POTS is by the mechanism that is loudest in a given young person, because the loudest mechanism points to the most useful treatment. The figure below lays out the three overlapping phenotypes alongside the diagnostic pathway. [2] [4]
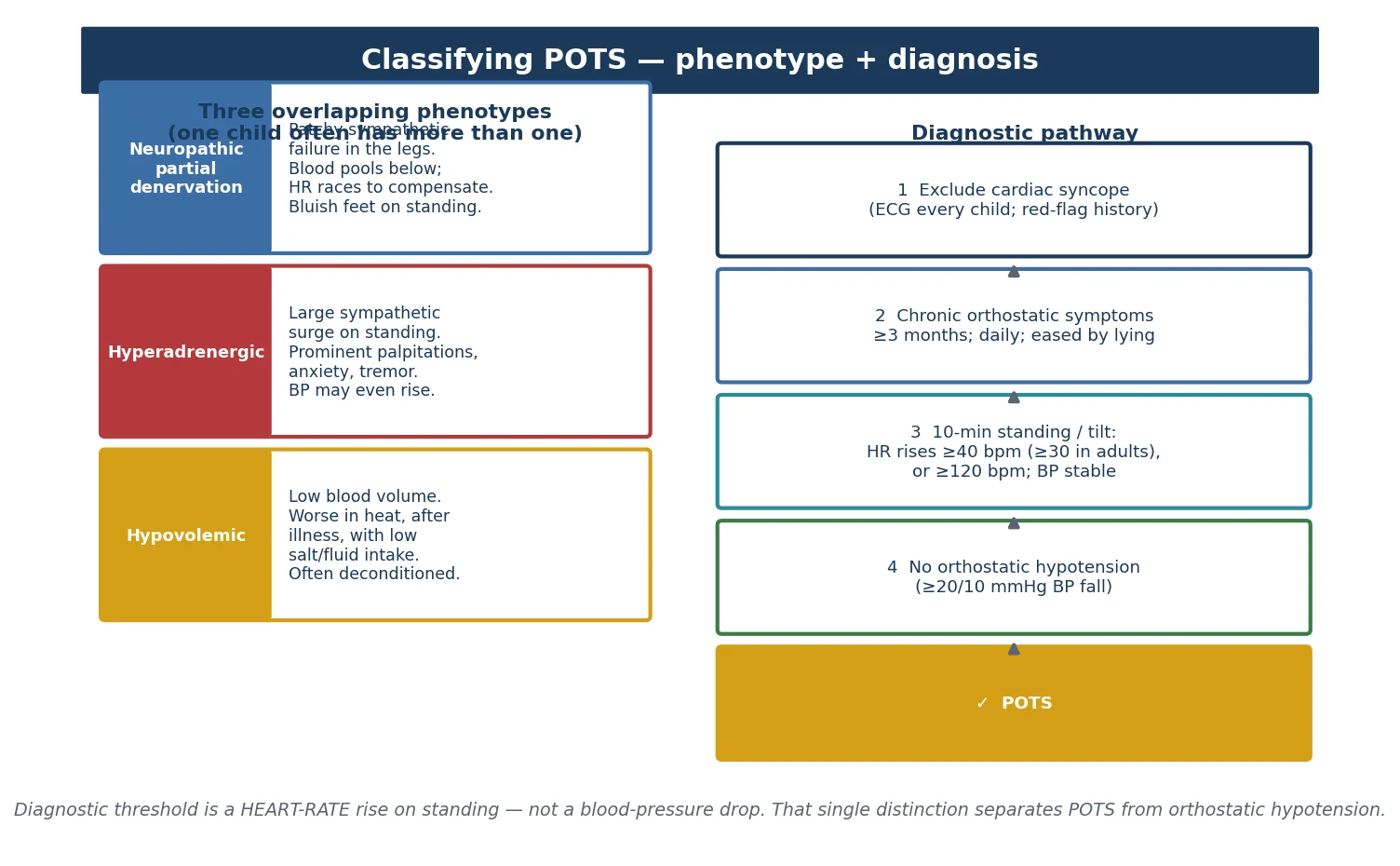
Neuropathic POTS — venous pooling
- Partial sympathetic denervation, especially of the legs; veins will not constrict
- Blood pools below, the heart races to compensate, blood pressure holds
- Acrocyanosis (purple-blue discolouration) of the lower legs on standing is supportive
- Responds to compression garments, counter-pressure and adequate volume
Hyperadrenergic POTS — sympathetic surge
- Large sympathetic discharge on standing; palpitations, tremor, anxiety, migraine
- Blood pressure may rise rather than stay flat; upright noradrenaline is high
- Often overlaps with migraine and with mast-cell-type symptoms
- May respond better to a beta-blocker or ivabradine
Hypovolaemic POTS — low volume
- Low plasma volume; worse in heat, after illness, with low salt and fluid intake
- Often combined with deconditioning and a low-renin state
- Exacerbated by menstruation and by skipped meals
- Responds to aggressive fluid, salt and sometimes fludrocortisone
One young person often carries more than one of these patterns at the same time, so the phenotypes are a guide to the dominant mechanism rather than rigid boxes. Naming the loudest mechanism is still useful, because it tells you which rung of the treatment ladder to emphasise first. [2] [8]
A second, practical classification sorts the young person by trigger and trajectory: a post-viral onset (including post-COVID), a growth-spurt or menarche onset, a post-surgical or post-concussion onset, and a deconditioning-dominant course with prolonged school absence. The trigger predicts the trajectory and the rehabilitation need, even when the physiology overlaps. [9] [14]
Epidemiology & Risk Factors
POTS is predominantly a disorder of adolescent females, with onset typically around menarche and the pubertal growth spurt, and a female-to-male ratio of roughly four to five to one in adolescent series. [5] [9] Precise population figures are hard to pin down, but POTS is one of the more common chronic conditions seen in adolescent autonomic and cardiology clinics, and the apparent rise in recognition reflects both better awareness and a genuine post-pandemic increase in post-viral orthostatic intolerance. [3] [14]
Recognised triggers come before the symptoms in a clear majority. A viral illness in the weeks beforehand is the classic one — Epstein-Barr virus, influenza and now SARS-CoV-2 are all described. A rapid growth spurt, an operation or an injury, a period of prolonged bed rest, and a concussion can all unmask the syndrome in a susceptible young person. [5] [6]
The conditions that travel with POTS matter, because they change the phenotype and the management. Joint hypermobility and hypermobile Ehlers-Danlos syndrome are common co-travellers and bring chronic pain, joint instability and gastrointestinal symptoms with them. [13] Mast-cell activation symptoms (flushing, hives, gastrointestinal upset) overlap in a subset. Chronic fatigue, headache, abdominal pain, anxiety and depression are frequent comorbidities and are not either-or diagnoses — they coexist and each needs its own plan. [9] [2]
Deconditioning is both a risk factor and a consequence, and it is the single most modifiable one. The less the young person moves, the lower their blood volume and the smaller their cardiac stroke volume, which worsens the orthostatic tachycardia, which makes them move even less. That spiral is what turns a manageable syndrome into a disabling one, and it is also what treatment is designed to break. [3] [10]
Pathophysiology
The shared endpoint of every POTS mechanism is the same: an inadequate venous return to the heart on standing. When blood fails to come back from the legs and the splanchnic bed, the stroke volume falls, and a baroreflex-driven compensatory tachycardia keeps the blood pressure roughly stable. The figure below traces that chain. [2] [10]
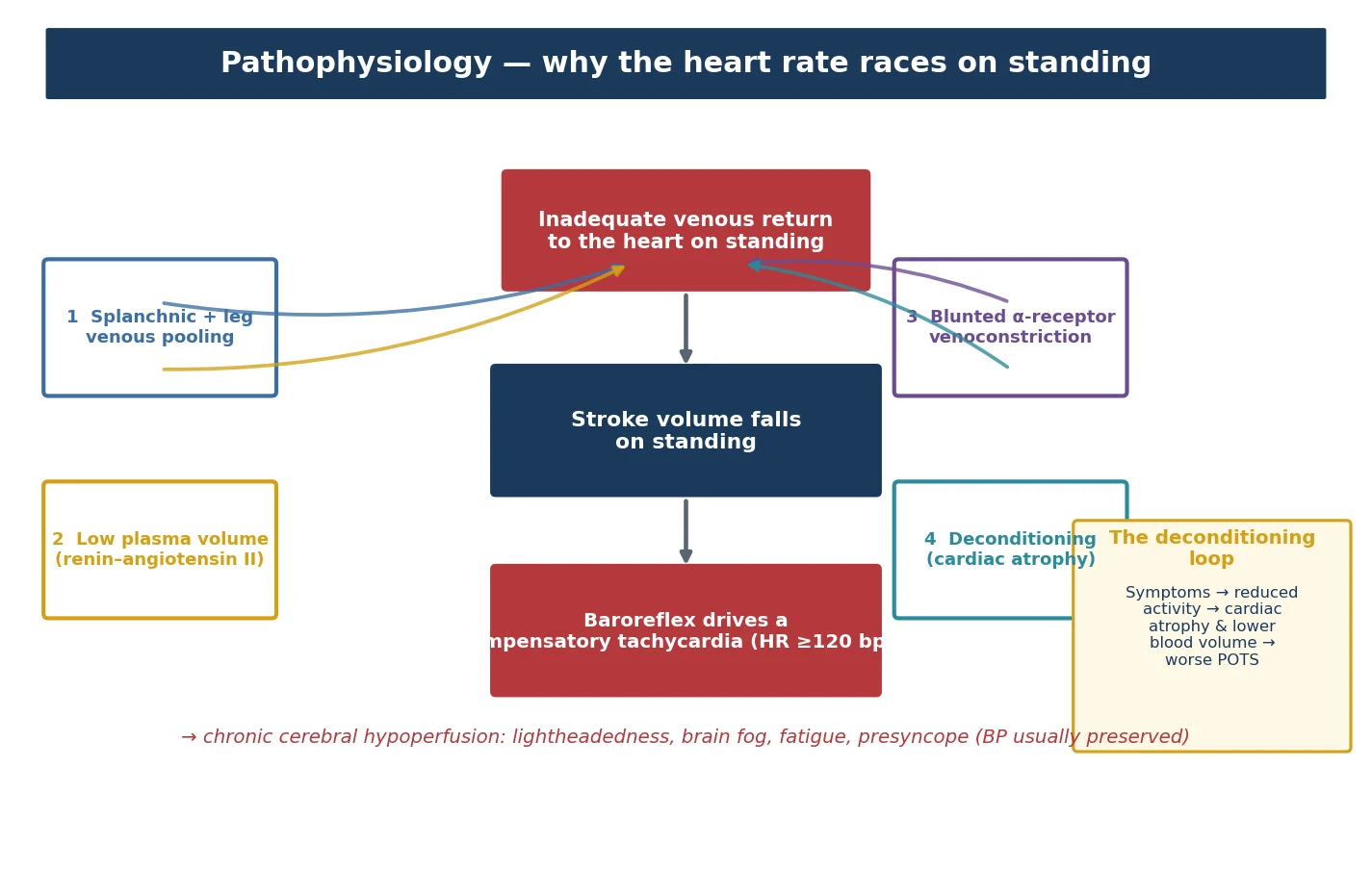
Walk through the four mechanisms, because they map directly onto the phenotypes and the treatment. Venous pooling from partial sympathetic (small-fibre) denervation of the legs lets blood sit in the capacitance vessels below the heart. Low plasma volume from an abnormal renin-angiotensin-aldosterone response means there is simply less blood to return. Blunted alpha-receptor-mediated venoconstriction fails to squeeze the veins as the young person stands. Cardiac deconditioning from inactivity leaves a smaller, less compliant heart with a lower stroke volume for any given filling. [2] [4]
Add a sympathetic overshoot in the hyperadrenergic form and you get the palpitations, tremor and anxiety that dominate that phenotype — and sometimes an upright blood pressure that actually rises rather than stays flat. [10] In every form, the baroreflex senses the threatened stroke volume and fires the sinus node hard, producing the tachycardia that defines the syndrome. [1]
The symptoms make sense once you hold that chain in mind. The brain is being perfused at the margin, so any further fall — heat, a meal, a hot shower, a menstrual cycle, prolonged standing — tips the young person into lightheadedness, brain fog and presyncope. The blood pressure is preserved, which is why a true faint is uncommon; it is the chronic, marginal cerebral perfusion, not acute hypotension, that drives the daily misery. [6] [9]
The deconditioning spiral deserves its own sentence because it is where the clinician can do the most good or the most harm. Symptoms reduce activity; reduced activity shrinks blood volume and cardiac mass; a smaller heart and lower volume worsen the orthostatic tachycardia; the worse tachycardia further limits activity. Left alone, this loop deepens disability and school absence. Actively reversed with recumbent exercise, the loop runs in reverse and is the most evidence-based component of treatment. [3] [10]
Clinical Presentation
The history is the diagnosis waiting to be heard, so take it slowly and let the pattern emerge. The cardinal features are posture, chronicity and trigger. [5] [7]
The postural pattern is the most discriminating single feature. Symptoms come on within minutes of standing — sitting up in bed, getting out of a chair, standing in a school assembly or a hot shower — and ease within minutes of lying down. The young person describes lightheadedness or dizziness, a racing or pounding heart, tremulousness, exercise intolerance, a heaviness in the legs, fatigue, difficulty concentrating (the much-used phrase "brain fog"), nausea, headache and presyncope. [9] [6]
The chronicity is the second key. These symptoms are present on most days and have been there for at least six months. They are not the brief episodes of a reflex faint but a daily lived experience that has begun to shrink the young person's world — fewer outings, less sport, missed school. [3]
The trigger often sits at the onset: a viral illness in the preceding weeks, a growth spurt or menarche, an operation or injury, a concussion, or a period of bed rest. Asking "what was happening in your life just before this started?" frequently surfaces the trigger and supports the diagnosis. [5] [14]
Exacerbating and relieving factors sharpen the picture. Heat, prolonged standing, large carbohydrate meals, alcohol, menstruation and dehydration all worsen symptoms; cold, recumbency, fluid and rest relieve them. A family history of fainting or of joint hypermobility is common; a family history of sudden death is a red flag that points away from POTS. [13] [2]
Examination in POTS is typically normal when the young person is supine, which is itself reassuring. On standing, watch for acrocyanosis — a purple or dusky-red discolouration of the lower legs and feet that appears within minutes of being upright and fades on lying down. It reflects venous pooling and supports a neuropathic component. Look also for signs of joint hypermobility, chronic pain and any cardiac abnormality that would redirect the diagnosis. [5] [13]
Now the red flags that must change your plan. POTS does not cause exertional collapse, syncope while supine or swimming, syncope from a loud noise or fright, palpitations at the exact moment of collapse, or chest pain. Any of these — and any family history of sudden death before about fifty — points to a cardiac cause and demands an ECG and cardiology review before POTS is concluded. [3] [1]
Differential Diagnosis
The differential has three layers, and working through them in order keeps the diagnosis safe. First, separate POTS from its closest autonomic cousins. Second, exclude the conditions that raise the standing heart rate for other reasons. Third, never lose sight of cardiac syncope, which is uncommon but dangerous. [3] [7]
The autonomic cousins are separated by the standing test, which is why the test matters so much. Orthostatic hypotension shows a blood-pressure fall of twenty over ten or more within three minutes, with a modest heart-rate rise. Vasovagal syncope shows an abrupt late drop in both heart rate and blood pressure with a prodrome. POTS shows a sustained heart-rate rise with a stable blood pressure. The figure below puts the three patterns side by side. [1] [9]
The tachycardia mimics are the conditions that raise the standing heart rate without being POTS, and they are mostly removable. Anaemia, hyperthyroidism, fever, dehydration, and medications or substances (stimulants including ADHD medicines, decongestants, excess caffeine, caffeine or nicotine withdrawal) all drive a fast standing rate. Check a full blood count, ferritin and thyroid function, and take a careful substance and medication history, before settling on POTS. [3] [8]
The functional and psychiatric mimics deserve a careful, non-dismissive approach. Deconditioning from any cause, chronic fatigue syndrome, generalised anxiety, panic disorder and somatisation can all produce a fast heart rate and dizziness on standing, and they can coexist with genuine POTS. The diagnosis is not made by excluding these but by demonstrating the objective standing-test pattern and treating whatever comorbidity is present. [2] [9]
The cardiac causes of collapse — long-QT syndrome, hypertrophic cardiomyopathy, arrhythmogenic cardiomyopathy, catecholaminergic polymorphic ventricular tachycardia, Wolff-Parkinson-White and congenital complete heart block — are individually rare but are the reason the screen exists. They are clinically silent between events, so the ECG and the red-flag history are the only things standing between a safe diagnosis and a fatal one. [1] [3]
Clinical & Bedside Assessment
The assessment has four parts: the orthostatic history, the red-flag screen, the standing test, and the cardiac examination with an ECG. Do them in that order and the diagnosis usually resolves without any further testing. [6] [7]
The orthostatic history establishes the posture-driven, chronic, daily pattern and the trigger. Ask exactly when the symptoms come (on standing), how long they last, what eases them (lying down), how long this has been going on (at least six months), and what was happening just before it began. Map the impact on school, sport, sleep and mood, because the functional cost is part of the diagnosis and the treatment plan. [9]
The red-flag screen is the same one used for syncope, applied with the same rigour. Exertional collapse, supine or swimming syncope, syncope from noise or fright, no prodrome, palpitations at the moment of collapse, chest pain, and a family history of sudden death under about fifty each mandate cardiac investigation before POTS is concluded. [3] [1]
The ten-minute active stand test is the diagnostic core, and doing it well matters. Lay the young person supine for five to ten minutes in a quiet room, then record the resting heart rate and blood pressure. Ask them to stand, and re-measure heart rate and blood pressure at two, five and ten minutes while asking about symptoms at each point. A heart-rate rise of at least forty beats per minute (or an upright rate of at least one hundred and twenty), sustained and symptomatic, with no blood-pressure fall of twenty over ten, is the positive test. [1] [14]
The cardiac examination and ECG close the assessment. Feel all four limb pulses and measure four-limb blood pressures, auscultate for a murmur of obstruction, and look for the stigmata of Marfan and hypermobility. Then read the 12-lead ECG yourself, looking for a long QTc, pre-excitation, Brugada pattern, heart block or the voltage and T-wave changes of cardiomyopathy. An ECG is obtained on every child, without exception. [3] [1]
A common technique error is to record only the heart rate during the stand test and to forget the blood pressure. Without the blood pressure you cannot distinguish POTS from orthostatic hypotension, so the test is wasted. Another error is to stop the stand at two minutes; the rise can take up to ten minutes to declare itself, and cutting it short misses the diagnosis. [6] [7]
Investigations
POTS is a clinical diagnosis confirmed by the standing test; there is no blood test, scan or tilt result that makes it on its own. Investigations exist to exclude the mimics and the dangerous causes, not to prove POTS. [3] [6]
First-line tests are few and purposeful. A 12-lead ECG is done on every child to exclude the arrhythmia substrate. A full blood count, ferritin and iron studies, urea and electrolytes, and thyroid function exclude anaemia, dehydration and hyperthyroidism. These are cheap, fast and resolve most of the tachycardia mimics in one round. [8] [3]
The 10-minute active stand test is itself the investigation that confirms POTS, performed as described above. It is reproducible, needs no special equipment beyond a manual or automated pressure cuff and a watch, and can be done in any clinic or even at home with supervision. [6] [14]
First-line work-up for suspected POTS
Head-up tilt-table testing is reserved for the atypical or equivocal case — when the active stand is inconclusive, when the history and the stand disagree, or when another autonomic diagnosis is genuinely in play. It is not a first-line test in straightforward adolescent POTS, and overusing it adds cost and false positives without changing management. [1] [2]
Ambulatory ECG (Holter) and echocardiography have defined roles. A Holter is useful when the history suggests an intermittent arrhythmia rather than a postural tachycardia — for example, truly random palpitations at rest. An echocardiogram is indicated when the examination or ECG suggests structural disease, when there is a murmur, or when exertional symptoms keep cardiac disease on the table. Neither is routine for a clean POTS presentation. [3] [7]
Plasma volume, standing catecholamines, supine and upright noradrenaline, and small-fibre nerve testing are research and specialist-autonomic-laboratory tools. They are rarely needed in routine paediatric practice and should not delay treatment of a clear case. [2] [10]
Management — Resuscitation
POTS is rarely a resuscitation diagnosis, but the acute-risk step is the one that matters most. Before concluding POTS, exclude cardiac syncope: any exertional, supine, warning-free or family-history-positive collapse gets an ECG, sport restriction and urgent cardiology referral. [3] [1]
An acute presyncopal episode in clinic is managed simply: lie the young person flat and elevate the legs. Most settle within minutes as venous return is restored. Reassure the family that this is the expected physiology and that lying down is the treatment. [6]
An intercurrent illness or dehydration can sharply worsen symptoms during a flare, because fever and reduced intake drop an already-low blood volume further. Oral rehydration settles most flares; intravenous fluid is reserved for the young person who cannot keep oral fluids down or who is profoundly symptomatic. [8] [5]
Genuine haemodynamic instability — shock, a persistent arrhythmia, chest pain — is not expected in POTS and should prompt immediate reassessment for an alternative diagnosis, starting with a repeat ECG and a cardiac-focused examination. [3]
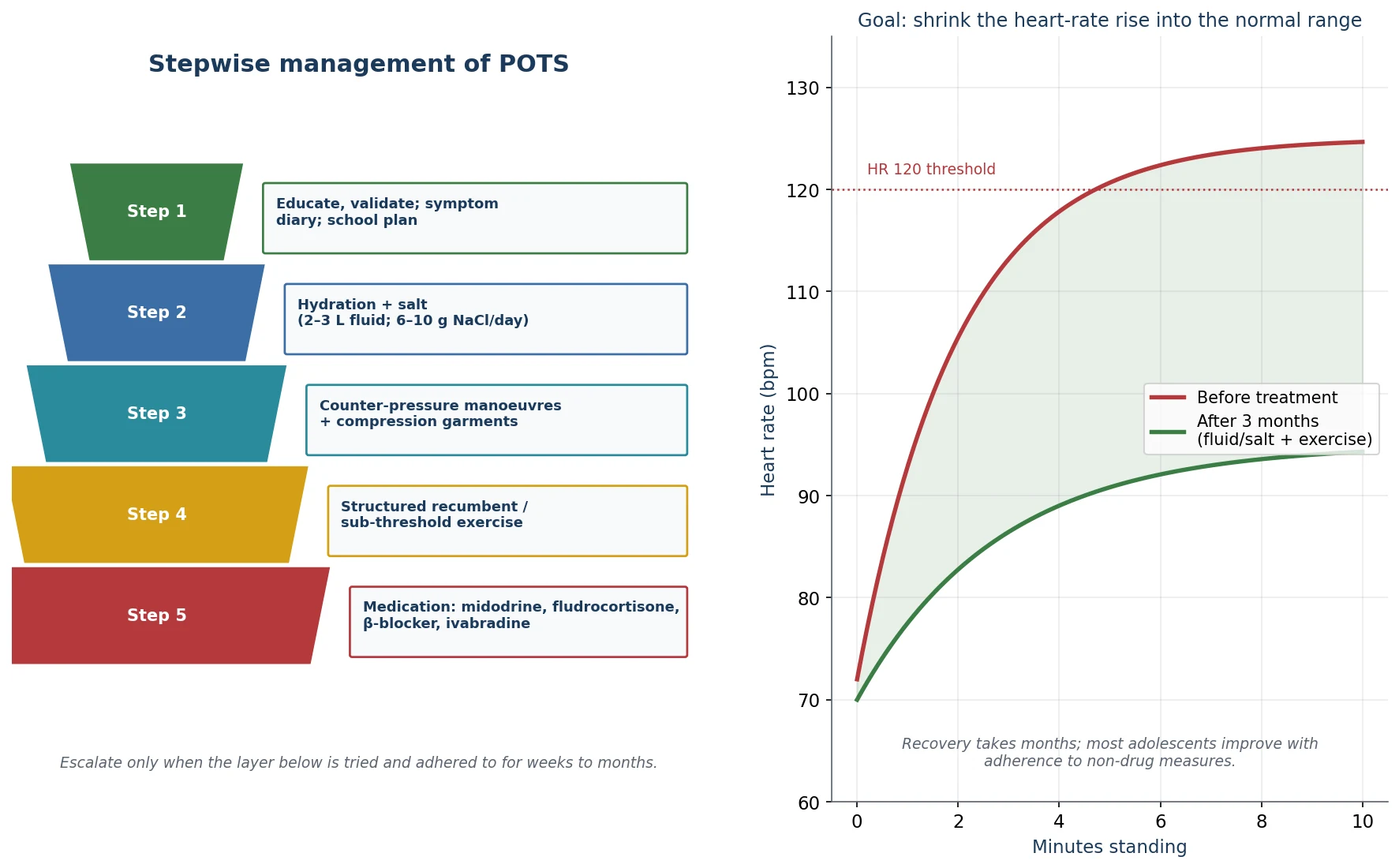
Management — Definitive & Stepwise
Management is a ladder, and the bottom rungs do most of the work. The figure below sets out the five steps and the goal of treatment — to shrink the standing heart-rate rise back into the normal range. [5] [10]
Step one — education, validation and a school plan. The most therapeutic single intervention is the explanation that this is a real, recognised and treatable condition, not anxiety, not "all in the head", and not a heart defect. Validate the family's experience, because most have been through several clinics before the diagnosis landed. Keep a symptom and standing diary to track the pattern and the response to treatment, and put a school plan in place early — allowances for late starts, movement breaks, water and salt at school, and a graded return after absence. [5] [9]
Step two — hydration and salt. Aim for around two to three litres of fluid and six to ten grams of sodium chloride per day in an adolescent, titrated to symptoms and tolerance, with the higher end of salt reserved for the hypovolaemic phenotype. This expands plasma volume and blunts the standing tachycardia. Avoid pushing salt in hypertension, renal disease or fluid-retaining states. [4] [8]
Step three — counter-pressure and compression. Teach physical counter-pressure manoeuvres (leg-crossing, hand-grip, arm-tensing, squatting) that the young person can use at the first hint of symptoms to push blood back up from the legs. Waist-high or abdominal compression garments (twenty to thirty millimetres of mercury) reduce venous pooling and are especially useful for the neuropathic phenotype. [2] [10]
Step four — structured recumbent or sub-threshold exercise. This is the most evidence-based component of treatment and the one that reverses the deconditioning spiral. Begin with recumbent exercise — a rowing machine, a recumbent bike, swimming — at a heart rate below the symptomatic threshold, and progress over weeks to months toward upright activity. The programme is slow, structured and progressive; jumping into upright aerobic exercise too early flares the symptoms and breaks adherence. [3] [10]
Step five — pharmacotherapy. Medication is reserved for young people who remain symptomatic despite adherence to the measures above, and the choice is phenotype-guided rather than protocol-driven. [11] [8]
Phenotype-guided drug choices in POTS (second-line)
The evidence base for drug therapy in paediatric POTS is modest — mostly observational and small-trial — so pharmacotherapy is an adjunct to, not a replacement for, the non-pharmacological programme. The Hasan systematic review of medication and the Zhang individualised-treatment update both frame the drugs as phenotype-guided add-ons. [11] [8] Midodrine in children has paediatric data going back to the copeptin-guided study of Zhao, and ivabradine is supported by a randomised trial in hyperadrenergic adults (Taub) that has shifted practice toward sinus-node slowing in that phenotype. [12]
Whatever the drug, review it against the goal: a young person moving more, attending school and feeling better, not just a slower standing heart rate on paper. Sleep, mental health and a graded return to school and activity are treated in parallel, because they are part of the syndrome, not separate problems. [9] [2]
Specific Subtypes & Scenarios
Hyperadrenergic POTS announces itself with palpitations, tremor, anxiety and sometimes a rising blood pressure on standing. A beta-blocker or ivabradine is often the most useful pharmacological add-on, alongside the core programme. Watch for coexistent migraine and mast-cell-type symptoms, which may need their own management. [10] [12]
Hypovolaemic POTS is driven by low plasma volume and is the phenotype most responsive to aggressive fluid and salt. Fludrocortisone is a reasonable add-on when fluid and salt alone are insufficient, with attention to potassium and to blood pressure. [4] [8]
Neuropathic POTS, with venous pooling and acrocyanosis, responds best to compression garments and counter-pressure manoeuvres, with midodrine as the pharmacological option when non-drug measures fall short. [2] [5]
Post-viral POTS, including post-COVID orthostatic intolerance, follows the same pathway but the trajectory may be more protracted. The ten-minute passive standing test has been specifically used to identify orthostatic intolerance in children with long COVID, and the management principles are identical: validate, expand volume, recondition, and add medication only when needed. [14] [9]
Post-concussion orthostatic intolerance is managed jointly: gradual cognitive and physical return alongside the POTS programme, with close coordination between the autonomic and concussion clinicians. Hypermobility and hypermobile Ehlers-Danlos-associated POTS needs physiotherapy that protects joints while building cardiovascular capacity. [13] [2]
The severely deconditioned young person with prolonged school absence is the scenario that tests the system. They need a staged, multidisciplinary rehabilitation and return-to-school plan, and a small minority benefit from a structured inpatient rehabilitation programme. Early diagnosis and the reconditioning ladder are the best way to avoid reaching that point. [3] [9]
Complications & Pitfalls
The most dangerous pitfall is missing a cardiac cause by settling on POTS in a young person whose collapse is exertional, supine, warning-free or family-history-positive. POTS is a diagnosis of a chronic orthostatic pattern, made only after the cardiac red flags and the ECG are clean. [3] [1]
The most common pitfall is diagnosing POTS on a single standing heart rate without a structured ten-minute stand test and without measuring blood pressure throughout. A fast standing rate alone, especially in an anxious, febrile or dehydrated child, is not POTS. The blood pressure must be measured, and the chronicity and daily pattern must be present. [6] [3]
A third pitfall is over-investigating a clear case with tilt-table testing, catecholamines and repeated imaging, which adds cost and anxiety without changing management. A clean history, a clean ECG and a positive stand test are enough to begin treatment. [2] [7]
A fourth pitfall is relying on medication while neglecting fluid, salt and reconditioning. The drugs blunt the numbers but do not reverse the deconditioning that perpetuates the syndrome; without the exercise programme, improvement stalls. [10] [3]
The fifth pitfall is missing the deconditioning and school-absence spiral. Untreated or under-treated POTS deepens as activity falls, and the school absence itself becomes a secondary disability. Early, assertive rehabilitation and a concrete school plan are how you prevent that outcome. [9]
Failing to screen for and treat the mental-health comorbidity — anxiety, depression, chronic pain, sleep disruption — leaves the young person partly treated. These are not either-or diagnoses; they coexist with POTS and each needs its own plan. [2] [9]
Prognosis & Disposition
POTS in young people carries a favourable long-term prognosis. Most improve substantially over months to a few years, particularly when deconditioning is reversed and the young person returns to school and activity. A relapsing-remitting course is common, with flares triggered by illness, heat, stress or menstruation, and a minority remain significantly symptomatic into early adulthood. [5] [9]
Outcome is best when three things line up: an early, accurate diagnosis that excludes cardiac disease; an assertive reconditioning programme; and coordinated support for school return and mental health. Young people who recondition do better than those who rest, which is why advice to "just take it easy" is counterproductive. [3] [10]
The disposition is outpatient in the great majority. Emergency or inpatient care is reserved for three situations: an acute collapse that needs exclusion of cardiac syncope; a severe flare with dehydration needing intravenous fluid; and the most deconditioned young person needing a structured inpatient rehabilitation programme. [7] [9]
Transition to adult autonomic services is planned in later adolescence for the minority who are still symptomatic, with a clear handover of the diagnosis, the standing-test results, the treatments tried and the response. Most young people will not need it. [2]
Special Populations
Adolescent females at and after menarche are the largest group. Address the modifiable contributors — menstrual blood loss, dieting, skipped meals, dehydration, rapid growth — as part of the plan, not as an afterthought. [5] [9]
The young person with joint hypermobility or hypermobile Ehlers-Danlos syndrome often has a more complex phenotype with chronic pain, gastrointestinal symptoms and mast-cell-type features. Care is integrated across autonomic, musculoskeletal and gastrointestinal services, and physiotherapy is joint-protective. [13]
Neurodivergent young people and those with a disability may report and experience symptoms differently and need an accessible, flexible assessment and a management plan built around their communication and sensory needs. [2]
Post-concussion and post-viral cohorts (including post-COVID) need coordinated rehabilitation that respects both the autonomic and the cognitive load, with a graded return to learning and activity. [14] [9]
Indigenous, rural-remote, migrant-refugee and socioeconomically disadvantaged young people face real access barriers to the multidisciplinary, school-flexibility and physiotherapy support that POTS needs. Care is planned explicitly with the family, the school and primary care to bridge those barriers, using telehealth to maintain continuity where distance is a factor. [7]
Gender-diverse young people may be affected and need confidentiality, an affirming approach and attention to the interaction of any gender-affirming hormones with the cardiovascular and autonomic picture. [2]
Evidence, Guidelines & Regional Differences
The evidence base draws on a chain of consensus statements and paediatric reviews. The 2015 Heart Rhythm Society expert consensus (Sheldon and colleagues) sets the diagnostic criteria and the stepwise approach that still anchors practice. [1] The 2019 National Institutes of Health expert consensus meeting, reported by Vernino and colleagues in 2021, updates the science and the clinical care. [2] The 2020 Canadian Cardiovascular Society position statement (Raj and colleagues) sets out a national framework for POTS and related chronic orthostatic intolerance. [3] The critical appraisal of Olshansky (2020) keeps the deconditioning and overlap debate in view. [3]
The paediatric-specific evidence rests on the reviews of Boris (2018), Chen (2020), Zhang (2020), Jarjour (2013) and Heyer (2017), which set out the pathophysiology and the individualised, phenotype-guided management. [4] [5] [6] [7] [8] The mechanisms and new therapies review of Mar and Raj (2020) is the bridge between the physiology and the pharmacotherapy. [10]
The pharmacotherapy evidence is modest and worth being honest about. The Hasan (2020) systematic review of medication and the Zhang (2020) individualised-treatment update frame the drugs as phenotype-guided add-ons with limited randomised data in children. [11] [8] Ivabradine is supported by the Taub (2021) randomised trial in hyperadrenergic adults, which has shifted practice toward sinus-node slowing in that phenotype, and midodrine by the copeptin-guided paediatric study of Zhao. [12] The hEDS–POTS–mast-cell link is set out by Kucharik (2020), and post-COVID orthostatic intolerance in children by Morrow (2025), who used a ten-minute passive standing test to identify it. [13] [14]
The main controversies are the exact heart-rate threshold in adolescents (the adult thirty-beat figure versus the paediatric forty); the role and timing of head-up tilt testing; the relative contribution of deconditioning versus primary dysautonomia; the validity of mast-cell activation as a co-condition; and the strength of evidence for pharmacotherapy, which remains mostly observational. [2] [3] [11]
Exam Pearls
Hold the one-sentence viva: POTS is chronic daily orthostatic intolerance — at least six months — in which standing drives an excessive heart-rate rise (≥40 bpm in adolescents, or ≥120 bpm) without an orthostatic fall in blood pressure; confirm it with a 10-minute active stand, exclude cardiac syncope with an ECG on every child, and treat with fluid, salt and recumbent exercise before reaching for medication. [1] [3]
The thresholds to know to the number: heart-rate rise ≥40 bpm (adolescent) or ≥30 bpm (adult) within 10 minutes of standing or tilt, or an upright rate ≥120 bpm; no blood-pressure fall of 20 mmHg systolic or 10 diastolic; symptoms for ≥6 months on most days. [1] [6]
The three standing-test patterns to quote: POTS races the rate and holds the pressure; orthostatic hypotension drops the pressure by 20/10; vasovagal drops both together late with a prodrome. [3] [9]
The management ladder to recite: educate and validate; hydrate and salt; counter-pressure and compression; recumbent exercise; phenotype-guided medication (midodrine, fludrocortisone, beta-blocker, ivabradine). [5] [10]
The traps to avoid: diagnosing POTS on a single standing heart rate; forgetting to measure the blood pressure during the stand; settling on POTS in an exertional or family-history-positive collapse; relying on medication without reconditioning; and missing the deconditioning and school-absence spiral. [3] [9]
The comorbidity picture to name: hypermobility and hypermobile Ehlers-Danlos, mast-cell activation, chronic fatigue, migraine, anxiety and depression, and post-viral (including post-COVID) orthostatic intolerance — co-travellers, not exclusions. [13] [14]
References
- [1]Sheldon RS; Grubb BP; Olshansky B; et al 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm, 2015.PMID 25980576
- [2]Vernino S; Stiles LE; Low P; et al Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1. Auton Neurosci, 2021.PMID 34144933
- [3]Olshansky B; Cannom D; Fedorowski A; et al Postural Orthostatic Tachycardia Syndrome (POTS): A critical assessment. Prog Cardiovasc Dis, 2020.PMID 32222376
- [4]Chen G; Wu L; Yu T; et al Postural Tachycardia Syndrome in Children and Adolescents: Pathophysiology and Clinical Management. Front Pediatr, 2020.PMID 32974246
- [5]Boris JR Postural orthostatic tachycardia syndrome in children and adolescents. Auton Neurosci, 2018.PMID 29778304
- [6]Jarjour IT Postural tachycardia syndrome in children and adolescents. Semin Pediatr Neurol, 2013.PMID 23465770
- [7]Heyer GL Postural Tachycardia Syndrome: Diagnosis and Management in Adolescents and Young Adults. Pediatr Ann, 2017.PMID 28414396
- [8]Zhang Q; Chen G; Wu L; et al Update of Individualized Treatment Strategies for Postural Orthostatic Tachycardia Syndrome in Children. Front Neurol, 2020.PMID 32655482
- [9]Soroken C; Lesavre N; Tard C; et al Postural tachycardia syndrome among adolescents. Arch Pediatr, 2022.PMID 35523634
- [10]Mar PL; Raj SR Postural Orthostatic Tachycardia Syndrome: Mechanisms and New Therapies. Annu Rev Med, 2020.PMID 31412221
- [11]Hasan B; Aslim M; Bushnag T; et al Treatment of Postural Orthostatic Tachycardia Syndrome With Medication: A Systematic Review. J Child Neurol, 2020.PMID 32838632
- [12]Taub PR; Bhatti T; Taggedoe D; et al Randomized Trial of Ivabradine in Patients With Hyperadrenergic Postural Orthostatic Tachycardia Syndrome. J Am Coll Cardiol, 2021.PMID 33602468
- [13]Kucharik AH; Maurer K The Relationship Between Hypermobile Ehlers-Danlos Syndrome (hEDS), Postural Orthostatic Tachycardia Syndrome (POTS), and Mast Cell Activation Syndrome (MCAS). Clin Rev Allergy Immunol, 2020.PMID 31267471
- [14]Morrow AK; Halai M; Johnson J; et al Orthostatic Intolerance in Children With Long COVID Utilizing a 10-Minute Passive Standing Test. Clin Pediatr (Phila), 2025.PMID 39123312