Paeds · cardiology
Supraventricular tachycardia
Also known as SVT · Paroxysmal supraventricular tachycardia · AV re-entry tachycardia · AV nodal re-entry tachycardia · Wolff-Parkinson-White syndrome
Fellowship guide to supraventricular tachycardia in children: the mechanisms (AVRT in infants, AVNRT in adolescents), the clinical presentations from irritable pale infant to palpitating teenager, the ECG hallmarks of a fast regular narrow complex, the stepwise acute termination with vagal manoeuvres and adenosine, long-term pharmacological control, catheter ablation, the special case of Wolff-Parkinson-White syndrome and sudden death risk, and the AHA/ACC/HRS, ESC and PACES/EHRA guideline positions.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the four-month-old brought to the emergency department pale and floppy after a feed, whose nurse says the heart rate monitor reads 250 and will not come down. The mother says he has been fussier at feeds for a day. You attach leads and see a regular narrow-complex tachycardia at 260 per minute with no visible P waves. That child carries the whole story of paediatric SVT — the commonest significant arrhythmia of childhood, and one where prompt recognition and a single drug can reverse heart failure within seconds. [3]
Supraventricular tachycardia is a rapid, regular tachycardia originating from a circuit or focus above the His bundle. The heart rate is typically 220 to 280 per minute in infants and 180 to 240 per minute in older children, which distinguishes SVT from sinus tachycardia where the rate rarely exceeds 220 in an infant and varies with stimulation. The mechanism is usually a reentrant circuit — a self-sustaining electrical loop — though a minority are driven by an automatic ectopic focus. [1] [2]
The clinical importance of SVT rests on three facts. It is eminently treatable — most episodes terminate with vagal manoeuvres or adenosine, and catheter ablation is curative. Infants often present non-specifically with poor feeding, irritability and pallor, so the diagnosis is missed unless a heart rate is measured and an ECG obtained. And Wolff-Parkinson-White syndrome, the most important substrate for SVT in children, carries a small but real risk of sudden cardiac death that demands assessment and sometimes ablation. [4] [9]
Classification
The most useful way to classify paediatric SVT is by the underlying mechanism, because the mechanism determines the ECG appearance, the response to adenosine, the long-term prognosis and the ablation target. Two reentrant mechanisms dominate: AVRT using an accessory pathway, and AVNRT using dual atrioventricular nodal pathways. A third category — focal atrial tachycardia — is driven by an automatic or triggered focus and behaves differently. [1] [3]
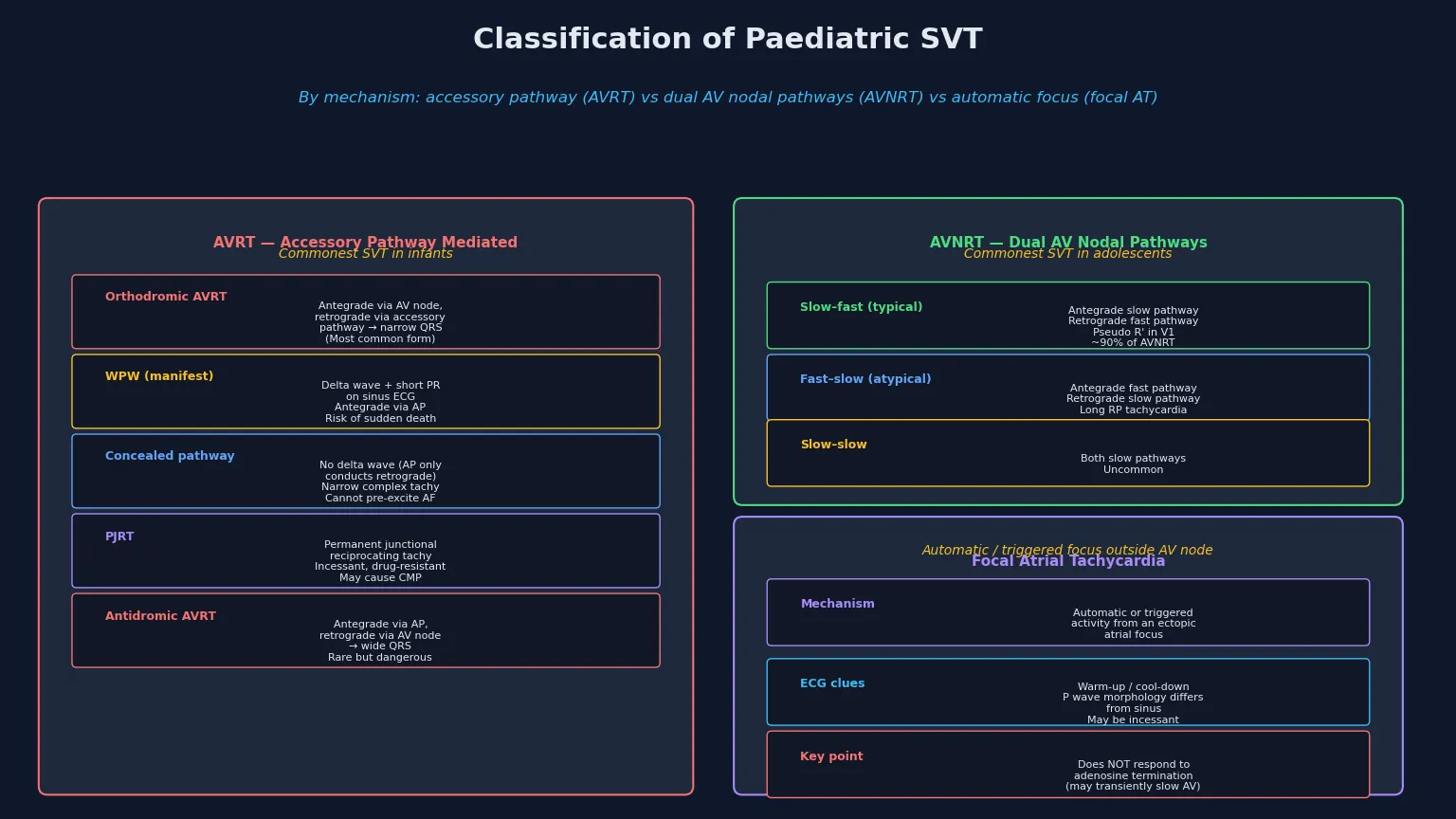
AVRT (accessory pathway)
commonest in infants
- Orthodromic: antegrade AV node, retrograde AP — narrow QRS
- WPW: delta wave + short PR on resting ECG
- Concealed: AP conducts only retrograde, no delta wave
- PJRT: incessant, long RP, negative P in inferior leads
- Risk of sudden death if manifest WPW (AF conduction)
AVNRT (dual nodal)
commonest in adolescents
- Slow–fast (typical, 90%): pseudo R' in V1
- Fast–slow (atypical): long RP, visible P waves
- Circuit confined to AV node tissue
- No accessory pathway, no pre-excitation
- Adenosine-responsive, excellent ablation success
Focal atrial tachycardia
automatic / triggered
- Ectopic atrial focus, warm-up / cool-down
- P wave morphology differs from sinus
- May be incessant — risk of tachycardiomyopathy
- Adenosine may slow AV conduction but rarely terminates
- Ablation target is the atrial focus, not the AV node
The distinction between manifest and concealed accessory pathways matters for prognosis. A manifest pathway — producing the Wolff-Parkinson-White pattern with a delta wave and short PR interval on the resting ECG — can conduct antegradely from atrium to ventricle during atrial fibrillation, producing very rapid ventricular rates that can degenerate to ventricular fibrillation. A concealed pathway conducts only retrogradely and cannot pre-excite the ventricle, so it carries no sudden death risk from atrial fibrillation. [4] [9]
Permanent junctional reciprocating tachycardia (PJRT) deserves special recognition because its incessant nature can cause a reversible cardiomyopathy. It is an orthodromic AVRT using a slowly conducting concealed accessory pathway near the coronary sinus, producing a long RP tachycardia with deeply inverted P waves in the inferior leads. The key teaching point is that PJRT is often misdiagnosed as sinus tachycardia because the rate is lower than typical SVT and the P waves can look almost normal. [10]
Epidemiology & Risk Factors
SVT is uncommon in absolute terms but central in the paediatric cardiology curriculum because it is the commonest arrhythmia requiring intervention in childhood. The incidence is estimated at around one per 250 to one per 1000 children, and it accounts for over half of all paediatric arrhythmia referrals. Presentation peaks twice — in infancy (when accessory pathway-mediated AVRT dominates) and in adolescence (when AVNRT dominates). [3] [5]
The most important risk factor for SVT in infancy is the presence of an accessory pathway. Up to 90 per cent of infants presenting with SVT have an accessory pathway, and a substantial proportion show the Wolff-Parkinson-White pattern on the post-termination ECG. Prematurity, congenital heart disease (especially Ebstein anomaly and congenitally corrected transposition), and a family history of arrhythmia or sudden death raise the background risk. [3] [9]
The numbers that anchor your viva
Infant-onset SVT has a reassuring natural history: approximately 60 to 80 per cent of infants will have spontaneous resolution of their SVT by one year of age, likely due to maturation of the accessory pathway. However, up to 30 per cent may experience recurrence later in childhood, typically around school age, so families should be counselled about this possibility even after successful medication withdrawal. [6] [3]
Pathophysiology
The teaching model rests on the concept of re-entry, which accounts for the great majority of paediatric SVT. A reentrant circuit requires two electrically distinct pathways that connect the same two structures, with a unidirectional block that allows an impulse to travel down one pathway and return via the other, creating a self-sustaining loop. Adenosine terminates reentrant SVT by transiently blocking the AV node, which is a limb of the circuit in both AVRT and AVNRT. [1] [2]
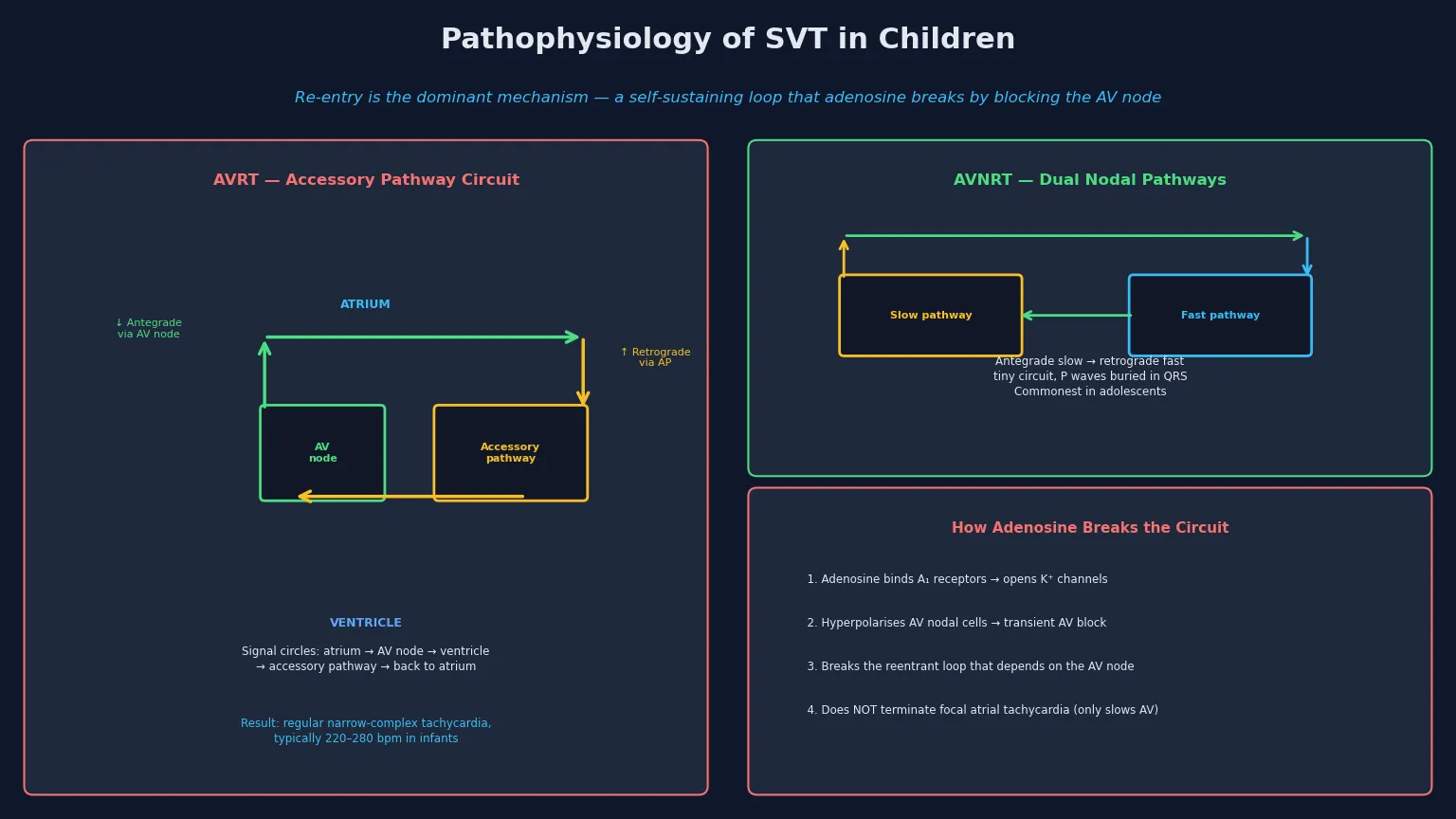
In AVRT, the circuit runs from atrium through the AV node to the ventricle and back to the atrium via an accessory pathway (orthodromic), producing a narrow QRS tachycardia. The accessory pathway is a remnant of the embryonic atrioventricular connections that failed to regress. When the pathway conducts antegradely during sinus rhythm, the ventricle is pre-excited and the resting ECG shows a delta wave and short PR interval — the Wolff-Parkinson-White pattern. [4] [2]
In AVNRT, the circuit is confined to the compact AV node and its surrounding tissue, which functionally behaves as two pathways — a slow pathway with short refractory period and a fast pathway with longer refractory period. A premature atrial beat blocks in the fast pathway, travels down the slow pathway, and returns retrogradely up the fast pathway, completing the loop. The circuit is tiny, so the P waves are buried within or immediately after the QRS. [1] [2]
[1] [12]Clinical Presentation
The presentation differs sharply by age because infants cannot describe palpitations. An infant in SVT is typically pale, irritable, feeding poorly, and breathing fast — a picture easily mistaken for sepsis or bronchiolitis unless a heart rate is measured. The rate is usually above 220 per minute and is fixed, meaning it does not vary with crying or stimulation, which is the key distinction from sinus tachycardia. [3] [6]
If SVT persists for hours to days, the infant develops signs of congestive heart failure: hepatomegaly, gallop rhythm, poor perfusion, and respiratory distress. This progression is the reason that any infant with unexplained tachycardia above 220 per minute needs an ECG urgently. The heart failure is reversible once the SVT is terminated, but prolonged tachycardia can lead to a tachycardiomyopathy. [6]
Older children describe the classic symptoms of SVT: sudden-onset rapid, regular palpitations, often with chest discomfort, dizziness, or breathlessness, and an equally sudden termination. Some children learn to break the episode themselves with vagal manoeuvres such as breath-holding, Valsalva, or cold water to the face. A careful history of the onset and offset pattern — abrupt start and abrupt stop — distinguishes SVT from anxiety-related awareness of sinus rhythm. [1] [8]
| Clinical picture | What it implies | Act |
|---|
A few children present with syncope during palpitations, which is a red flag suggesting a rapid accessory pathway or pre-excited atrial fibrillation. Any history of syncope with palpitations mandates urgent electrophysiological assessment, because this may be the only warning before sudden cardiac death in a Wolff-Parkinson-White patient. [4] [11]
Differential Diagnosis
Build the differential around the ECG and the heart rate. The first distinction is between SVT and sinus tachycardia: sinus tachycardia has a normal P wave axis, a rate that varies with stimulation, and a rate generally below 220 in infants and below 180 in older children. SVT is faster, fixed, and has abnormal or absent P waves. The hyperoxia test and fever do not distinguish them — the ECG does. [1] [2]
The second distinction is between narrow-complex and wide-complex tachycardia. Most paediatric SVT is narrow-complex (QRS less than 120 milliseconds), but antidromic AVRT, pre-excited atrial fibrillation, and ventricular tachycardia all produce a wide-complex tachycardia. A wide-complex tachycardia should be treated as ventricular tachycardia until proven otherwise, and adenosine should be used cautiously and only with a defibrillator at the bedside. [1] [3]
Sinus tachycardia
- Normal P wave axis, visible P waves
- Rate varies with crying, fever, pain
- Infant rate usually below 220; child below 180
- Causes: fever, dehydration, sepsis, anxiety, anaemia
- Treat the cause, not the rhythm
SVT
- Rate fixed, fast (infant above 220, child above 180)
- P waves absent, retrograde, or pseudo R' in V1
- Abrupt onset and offset
- No response to fever control or fluids alone
- Vagal manoeuvres and adenosine terminate it
Wide-complex tachy
- QRS over 120 ms
- Treat as ventricular tachycardia until proven otherwise
- May be antidromic AVRT or pre-excited AF
- Adenosine only with defibrillator ready
- Consider VT, electrolyte disturbance, cardiomyopathy
Atrial flutter and atrial fibrillation are rare in structurally normal children but occur after atrial surgery (for example, the Fontan circulation, atrial septal defect repair) and in children with dilated cardiomyopathy or sepsis. These produce an irregularly irregular or sawtooth pattern rather than the regular tachycardia of typical SVT, and they require a different management pathway involving rate control and anticoagulation. [1] [3]
Clinical & Bedside Assessment
Assessment runs in parallel with termination, because a child in SVT with cardiovascular compromise needs the rhythm broken without delay. Secure the airway, breathing and circulation, attach a cardiac monitor and a 12-lead ECG, obtain intravenous access, and assess the haemodynamic status. If the child is unstable — hypotensive, profoundly pale, in heart failure, or with altered consciousness — proceed directly to synchronised DC cardioversion. [1] [3]
The history targets the onset pattern (sudden versus gradual), the triggers (exercise, emotion, caffeine), the frequency and duration of episodes, and any self-termination manoeuvres. Ask specifically about syncope or near-syncope with palpitations, which raises the suspicion of a high-risk accessory pathway. Take a family history of arrhythmia, sudden cardiac death, or Wolff-Parkinson-White syndrome, and a perinatal history of prematurity or congenital heart disease. [4] [9]
[1] [4]Examination looks for the haemodynamic consequences of SVT: pallor, poor perfusion, weak pulses, prolonged capillary refill, hepatomegaly, and signs of heart failure. Listen for a gallop rhythm. Examine for features of congenital heart disease, especially Ebstein anomaly, which is strongly associated with right-sided accessory pathways. A careful baseline examination also identifies signs of structural heart disease that would change the management pathway. [3] [1]
Investigations
The 12-lead ECG is the single most important investigation and should be obtained during tachycardia whenever possible. The key features are a regular, narrow-complex tachycardia with no visible P waves, retrograde P waves, or a pseudo R-prime in V1 (the "rSsr'" pattern of typical AVNRT). If the tachycardia is already terminated, obtain a resting ECG and look specifically for the Wolff-Parkinson-White pattern: a delta wave, short PR interval, and widened QRS. [1] [2]
After termination, the resting ECG guides the long-term plan. A normal resting ECG suggests a concealed accessory pathway or AVNRT, both of which carry an excellent prognosis. A Wolff-Parkinson-White pattern identifies a subgroup requiring risk stratification. The ECG also rules out long QT syndrome, hypertrophic cardiomyopathy, and other inherited arrhythmia syndromes that may coexist. [4] [9]
The standard diagnostic workup
12-lead ECG during tachycardia — rate, QRS width, P wave morphology, RP interval
Post-termination resting 12-lead ECG — look for delta wave, short PR (WPW pattern)
Echocardiogram — rule out structural heart disease (Ebstein, cardiomyopathy, cardiac tumour)
Baseline bloods — electrolytes, magnesium, calcium, thyroid function
Ambulatory ECG (Holter) or event monitor for recurrent or infrequent episodes
Exercise testing for exercise-induced SVT or to assess WPW risk
Electrophysiological study for risk stratification of asymptomatic WPW or pre-ablation mapping
An echocardiogram is recommended at first presentation to exclude structural heart disease, assess cardiac function (especially if heart failure is present), and look for the atrial tumours that can cause atrial tachycardias. Blood tests check for electrolyte disturbances, thyroid dysfunction, and infection that may have precipitated the SVT. Ambulatory monitoring captures intermittent episodes and helps assess burden and response to therapy. [3] [1]
Management — Resuscitation
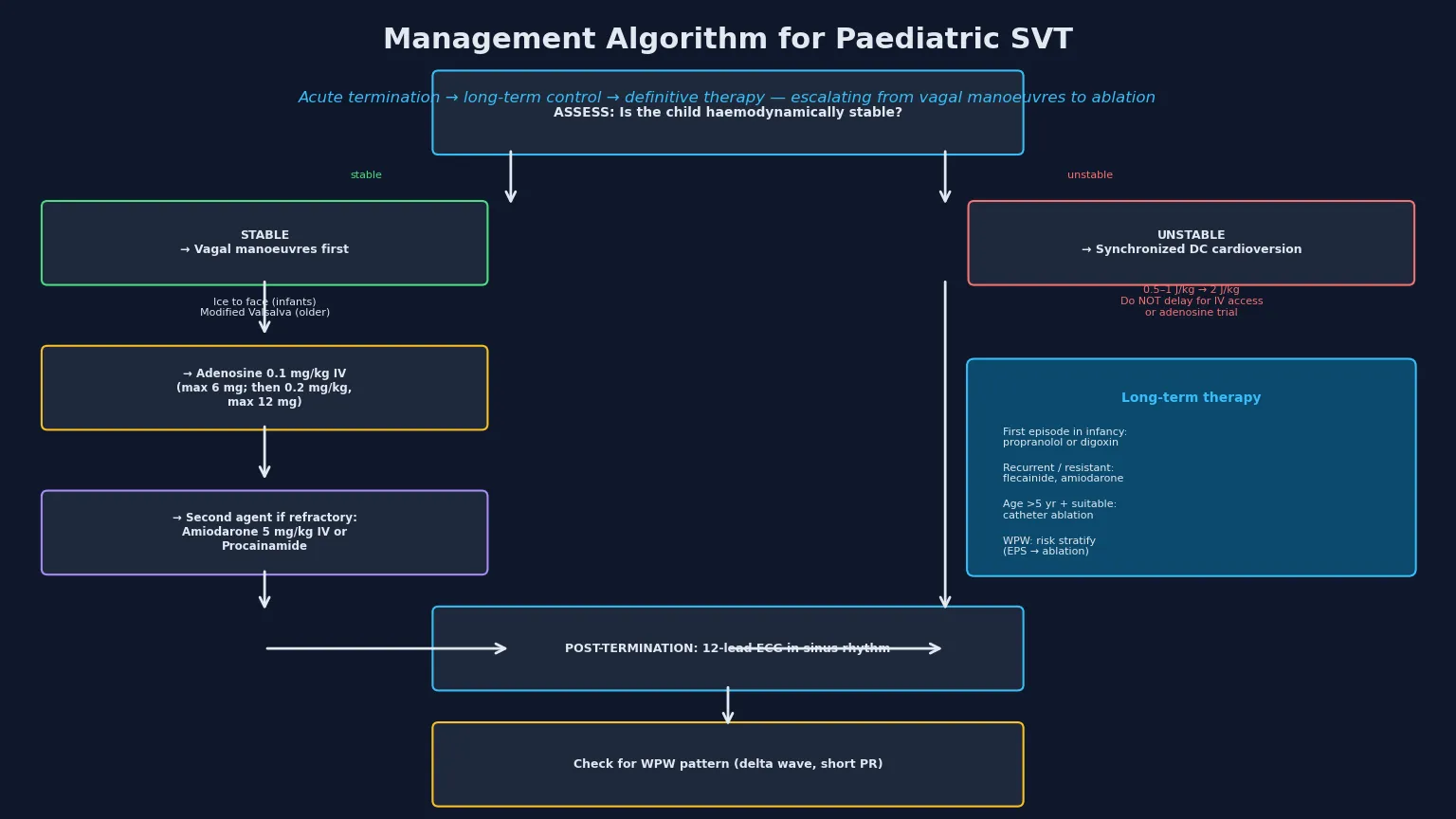
Acute management begins with a decision about haemodynamic stability. The stable child with normal perfusion and blood pressure can be treated stepwise with vagal manoeuvres then adenosine. The unstable child with hypotension, severe pallor, altered consciousness, or heart failure needs immediate synchronised DC cardioversion without delay for intravenous access or a trial of adenosine. [1] [3]
For the stable child, vagal manoeuvres are the first step and should be attempted before any drug. In infants, the most reliable technique is the diving reflex: breakable ice in a sealed bag or a cold gel pack applied to the face for 15 to 30 seconds. In older, cooperative children, a modified Valsalva manoeuvre — semi-recumbent forced expiration against a closed glottis for 15 seconds, then repositioning to supine with leg elevation — is effective, with the REVERT trial showing superior termination rates over the standard Valsalva in adults. [8] [2]
SVT-BREAK
Adenosine is the first-line pharmacological agent for SVT termination. The dose is 0.1 milligramme per kilogramme as a rapid intravenous bolus, with a maximum first dose of 6 milligrammes, followed immediately by a saline flush through the largest-bore cannula closest to the heart. If the first dose fails, the second dose is 0.2 milligramme per kilogramme with a maximum of 12 milligrammes. The rapid bolus technique is essential because adenosine is metabolised within seconds by endothelial adenosine deaminase. [12] [1]
Adenosine
Dose
0.1 mg/kg rapid IV bolus (max 6 mg); if ineffective, 0.2 mg/kg (max 12 mg)
For the unstable child, synchronised DC cardioversion at 0.5 to 1 joule per kilogramme is the treatment of choice, escalating to 2 joules per kilogramme if the first shock fails. Sedation is ideal but must not delay cardioversion in the compromised child. If the child is in refractory SVT despite vagal manoeuvres, adenosine, and cardioversion, intravenous amiodarone at 5 milligrammes per kilogramme over one hour, or procainamide, are the next agents. [3] [1]
Management — Definitive & Stepwise
After the acute episode is terminated, the long-term strategy depends on the age of the child, the frequency and severity of episodes, the underlying mechanism, and the presence of the Wolff-Parkinson-White pattern. The goals are to prevent recurrence, protect the child from haemodynamic deterioration, and either cure the arrhythmia with ablation or outgrow it naturally. [3] [5]
For infants with a first episode of SVT, prophylactic antiarrhythmic therapy is standard because recurrence is common. The first-line agents are propranolol (2 to 4 milligrammes per kilogramme per day in three divided doses) or digoxin (10 microgrammes per kilogramme per day). Flecainide is added or substituted for resistant or recurrent cases, and amiodarone is reserved for refractory SVT. Most infants can be weaned from therapy at 12 months given the high spontaneous resolution rate. [6] [3]
The life arc of paediatric SVT
For older children and adolescents with recurrent SVT, the management pathway depends on the mechanism and the burden. AVNRT in an adolescent can be managed with a "pill in the pocket" strategy (a single dose of a beta-blocker or calcium-channel blocker taken at the onset of an episode) for infrequent, well-tolerated episodes, or with daily prophylaxis for frequent episodes. Catheter ablation is curative and is recommended for recurrent or poorly tolerated SVT in children over approximately five years of age. [5] [13]
Catheter ablation uses radiofrequency energy or cryotherapy to eliminate the arrhythmia substrate — the accessory pathway in AVRT, the slow pathway in AVNRT, or the ectopic focus in focal atrial tachycardia. The multicenter paediatric ablation registry reports acute success rates exceeding 95 per cent for AVNRT and AVRT, with recurrence rates of 5 to 10 per cent. Cryoablation is preferred for AVNRT in young children because of the lower risk of AV nodal injury. Ablation is generally deferred until after five years of age because of the small risk of coronary artery injury from radiofrequency lesions near the coronary sinus, unless the SVT is medically refractory or life-threatening. [13] [15]
Specific Subtypes & Scenarios
Wolff-Parkinson-White syndrome is the most important specific scenario because of the small but real risk of sudden cardiac death. The WPW pattern on the resting ECG — a delta wave, short PR interval, and widened QRS — indicates an accessory pathway capable of antegrade conduction. During atrial fibrillation, the pathway can conduct very rapidly to the ventricles, producing ventricular rates above 300 per minute that may degenerate to ventricular fibrillation. Risk stratification involves assessing the shortest pre-excited RR interval during atrial fibrillation, either non-invasively with exercise testing and ambulatory monitoring or invasively with an electrophysiological study. A pathway that loses pre-excitation during exercise is low-risk; a shortest pre-excited RR interval below 250 milliseconds is high-risk and warrants ablation. [4] [9]
Permanent junctional reciprocating tachycardia (PJRT) is an incessant orthodromic AVRT using a concealed, slowly conducting accessory pathway near the coronary sinus or septum. The ECG shows a long RP tachycardia with inverted P waves in the inferior leads (II, III, aVF), and the rate is typically slower than typical SVT — often 130 to 200 per minute — which is why it is frequently mistaken for sinus tachycardia. The incessant nature can cause a tachycardiomyopathy, and catheter ablation of the pathway is the definitive treatment, often with dramatic recovery of ventricular function. [10]
Focal atrial tachycardia accounts for approximately 5 to 10 per cent of paediatric SVT. It is driven by an automatic or triggered focus outside the reentrant circuit, typically in the right atrium near the crista terminalis or in the pulmonary vein ostia. The ECG shows a warm-up and cool-down phenomenon, and the P wave morphology differs from sinus. Adenosine may slow AV conduction and reveal the atrial rhythm but rarely terminates the tachycardia, which is a diagnostic clue. Incessant focal atrial tachycardia can cause tachycardiomyopathy, and catheter ablation of the focus is the definitive treatment. [7]
SVT in the setting of congenital heart disease is a distinct scenario. After atrial surgery — particularly the Fontan procedure, atrial septal defect repair, or Mustard or Senning operations for transposition — intra-atrial re-entry tachycardia (IART) is common and challenging. The management involves rate control, antiarrhythmics, catheter ablation using three-dimensional mapping, and sometimes surgical revision. Ebstein anomaly is strongly associated with right-sided accessory pathways and WPW, and ablation should be considered before or at the time of tricuspid valve surgery. [3] [5]
Complications & Pitfalls
The complications of SVT range from the nuisance of recurrent episodes to life-threatening events. The most serious acute complication is cardiovascular collapse from sustained tachycardia, particularly in infants who cannot compensate and develop progressive heart failure over hours to days. This is why any infant with a heart rate above 220 per minute needs urgent assessment and termination. [6] [3]
Tachycardiomyopathy is a reversible form of ventricular dysfunction caused by chronic or incessant tachycardia. It occurs with PJRT, incessant focal atrial tachycardia, and persistent junctional ectopic tachycardia. The key teaching point is that the ventricular dysfunction can be severe enough to mimic dilated cardiomyopathy, but it recovers completely after the arrhythmia is controlled — so any new diagnosis of cardiomyopathy must prompt a search for an occult tachyarrhythmia. [10] [7]
The risks that drive management
The common pitfalls are clinical and avoidable. The first is failing to measure a heart rate in a pale, irritable infant and attributing the symptoms to feeding problems or colic. The second is giving adenosine too slowly — a common error that leads to apparent non-response because the drug is metabolised before reaching the AV node. The third is misclassifying sinus tachycardia as SVT and giving adenosine unnecessarily — the distinction is the variability of the rate and the P wave morphology. The fourth is failing to obtain a post-termination ECG and missing the Wolff-Parkinson-White pattern. [12] [1]
[2] [3]Prognosis & Disposition
The prognosis of paediatric SVT is excellent. Most episodes terminate with vagal manoeuvres or adenosine, catheter ablation is curative in over 95 per cent of suitable children, and infant-onset SVT resolves spontaneously in 60 to 80 per cent by one year of age. Children with AVNRT and concealed accessory pathways have an excellent prognosis with low sudden death risk. [5] [13]
The main exception is the Wolff-Parkinson-White subgroup, where the small but real risk of sudden cardiac death from pre-excited atrial fibrillation means that risk stratification is essential. After successful ablation of a high-risk pathway, the sudden death risk is eliminated, and the child can return to full activity including competitive sport. [4] [11]
Disposition after a first episode of SVT depends on the child's age and the mechanism. An infant presenting with SVT and heart failure is admitted for observation, initiation of prophylactic medication, and parental education on recognising and responding to recurrence. An older child with a well-tolerated episode that terminated easily can be discharged with outpatient cardiology follow-up and a prescription for a "pill in the pocket" strategy if appropriate. Every child needs a post-termination ECG and cardiology referral for long-term planning. [3] [1]
Children who undergo catheter ablation typically return for a follow-up Holter and exercise test at three to six months, and are then discharged to routine follow-up if asymptomatic. Sports participation is unrestricted after successful ablation, and after a period of observation for those managed medically. Structured transition to adult congenital or electrophysiology care applies to those with Wolff-Parkinson-White syndrome, congenital heart disease, or complex arrhythmia substrates. [5] [2]
Special Populations
Infants presenting with SVT deserve special attention because their non-specific presentation often delays diagnosis. The key to early recognition is measuring the heart rate of any pale, irritable, or unwell infant and obtaining an ECG if the rate is above 220 per minute. Once terminated, infants are started on prophylactic therapy (typically propranolol or digoxin) and monitored for recurrence, with the expectation that most will resolve by one year. [6] [3]
Children with Wolff-Parkinson-White syndrome require lifelong awareness of the sudden death risk, even after successful ablation. Although ablation eliminates the pathway, the genetic substrate for accessory pathways may produce new pathways in a small proportion of patients. Families should be counselled about the importance of reporting syncope, near-syncope, or a return of palpitations, and of informing healthcare providers of the WPW history during any future presentation. [4] [9]
Children with congenital heart disease and SVT are a complex population managed jointly by the congenital cardiologist and electrophysiologist. Post-operative atrial tachycardias, accessory pathways in Ebstein anomaly, and conduction defects after surgery all influence the management pathway. Culturally safe, equitable access to paediatric electrophysiology is essential for Indigenous, rural, refugee, and socioeconomically disadvantaged families, who may face barriers to specialist referral and follow-up. [3] [5]
The transitioning adolescent and young adult with SVT needs structured handover from paediatric to adult electrophysiology services. The risks of non-adherence with medication, recreational stimulant use, and unplanned pregnancy converge in this group, so education about triggers, self-management with vagal manoeuvres, and awareness of the WPW risk are part of standard transition care. [2] [5]
Evidence, Guidelines & Regional Differences
| Region | Key guideline | Acute termination | Long-term strategy |
|---|
The two main controversies a candidate should be able to discuss are the approach to the asymptomatic child with a Wolff-Parkinson-White pattern, and the age at which catheter ablation should be offered. The PACES/HRS consensus recommends risk stratification for all asymptomatic WPW patients, with invasive electrophysiological study for those who do not lose pre-excitation on exercise testing. The ablation age debate centres on the small risk of coronary artery injury from radiofrequency lesions in very young children, which has driven the general practice of deferring ablation until after approximately five years of age unless the SVT is refractory or life-threatening. [4] [14]
Exam Pearls
References
- [1]Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia. J Am Coll Cardiol, 2016.PMID 26409259
- [2]Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. Eur Heart J, 2020.PMID 31504425
- [3]Brugada J, Blom N, Sarquella-Brugada G, et al. Pharmacological and non-pharmacological therapy for arrhythmias in the pediatric population: EHRA and AEPC-Arrhythmia Working Group joint consensus statement. Europace, 2013.PMID 23851511
- [4]Cohen MI, Triedman JK, Cannon BC, et al. PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern. Heart Rhythm, 2012.PMID 22579340
- [5]Paul T, Hofferberth SC, Cohen MI, et al. Advancing the science of management of arrhythmic disease in children and adult congenital heart disease patients within the last 25 years. Europace, 2023.PMID 37622573
- [6]Wei N, Pflaumer A, Chubb H, et al. Medical Management of Infants With Supraventricular Tachycardia: Results From a Registry and Review of the Literature. CJC Pediatr Congenit Heart Dis, 2022.PMID 37969556
- [7]Kang KT, Potts JE, Radbill AE, et al. Current management of focal atrial tachycardia in children: a multicenter experience. Circ Arrhythm Electrophysiol, 2014.PMID 25015944
- [8]Appelboam A, Reuben A, Mann C, et al. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet, 2015.PMID 26314489
- [9]Al-Khatib SM, Arshad A, Balk EM, et al. Risk Stratification for Arrhythmic Events in Patients With Asymptomatic Pre-Excitation: A Systematic Review for the 2015 ACC/AHA/HRS SVT Guideline. J Am Coll Cardiol, 2016.PMID 26409260
- [10]Kang KT, Potts JE, Radbill AE, et al. Permanent junctional reciprocating tachycardia in children: a multicenter experience. Heart Rhythm, 2014.PMID 24769425
- [11]Obeyesekere MN, Leong-Sit P, Massel D, et al. Preventing Sudden Death in Asymptomatic Wolf-Parkinson-White Patients. JACC Clin Electrophysiol, 2018.PMID 30067482
- [12]Losek JD, Endom E, Dietrich A, Stewart G, Zempsky W, Smith K Adenosine and pediatric supraventricular tachycardia in the emergency department: multicenter study and review. Ann Emerg Med, 1999.PMID 9922414
- [13]Van Hare GF, Javitz H, Carmelli D, et al. Prospective assessment after pediatric cardiac ablation: demographics, medical profiles, and initial outcomes. J Cardiovasc Electrophysiol, 2004.PMID 15250858
- [14]Campbell RM, Strieper MJ, Frias PA, Collins KK, Van Hare GF, Dubin AM Survey of current practice of pediatric electrophysiologists for asymptomatic Wolff-Parkinson-White syndrome. Pediatrics, 2003.PMID 12612279
- [15]Van Hare GF, Carmelli D, Smith WM, et al. Prospective assessment after pediatric cardiac ablation: design and implementation of the multicenter study. Pacing Clin Electrophysiol, 2002.PMID 11990663