Paeds · cardiology
Total anomalous pulmonary venous connection
Also known as total anomalous pulmonary venous connection · TAPVC · total anomalous pulmonary venous return · TAPVR · anomalous pulmonary venous drainage · TAPVD
A fellowship approach to total anomalous pulmonary venous connection: the cyanosed neonate with pulmonary oedema as a surgical emergency, the Darling classification of where the pulmonary veins drain, the echocardiographic diagnosis, the obligatory atrial septal communication, the surgical repair that re-routes blood to the left atrium, and the lifelong surveillance for recurrent pulmonary venous obstruction.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A two-day-old term baby is brought in blue and grunting, with a chest radiograph that shows a normal-sized heart and fluffy, waterlogged lungs; or a six-week-old infant presents with mild duskiness, poor feeding, and failure to thrive over several weeks; or a prenatal scan at twenty weeks flags an abnormal pulmonary venous connection and the family is counselled before delivery. The fellowship task in each is the same: think of total anomalous pulmonary venous connection, confirm it with echocardiography, and decide whether this child needs the operating theatre today or a planned repair in infancy. [7] [4]
The five moves — Suspect, Scan, Stabilise, Re-route, Survey
Overview & Definition
Total anomalous pulmonary venous connection means that all four pulmonary veins, instead of returning oxygenated blood to the left atrium, drain into the systemic venous circulation. The blood therefore arrives back at the right atrium, mixes with the deoxygenated systemic venous return, and can only reach the left side of the heart by crossing an atrial communication. This is what makes the lesion cyanotic, and it is why an atrial septal defect or patent foramen ovale is obligatory for survival. [7] [1]
The lesion is distinguished from partial anomalous pulmonary venous return, in which only some of the pulmonary veins are anomalous and the rest drain normally to the left atrium. A partial lesion behaves as a left-to-right shunt and is often asymptomatic for years, whereas the total lesion produces obligatory mixing and cyanosis from birth. The distinction matters because the total form is a neonatal emergency or an early-infancy surgical problem, while the partial form is usually an elective closure decision. [1]
The clinical importance of the condition comes from what happens when the anomalous pathway is narrowed. An obstructed connection floods the lungs with fluid, drives up the pulmonary pressures, and produces severe cyanosis and respiratory failure within the first day or two of life. This is the obstructed neonate, and recognising them is the must-not-miss skill of the topic. The unobstructed form, by contrast, behaves more like a large shunt with cyanosis, and it declares itself over weeks to months. [1] [2]
Classification
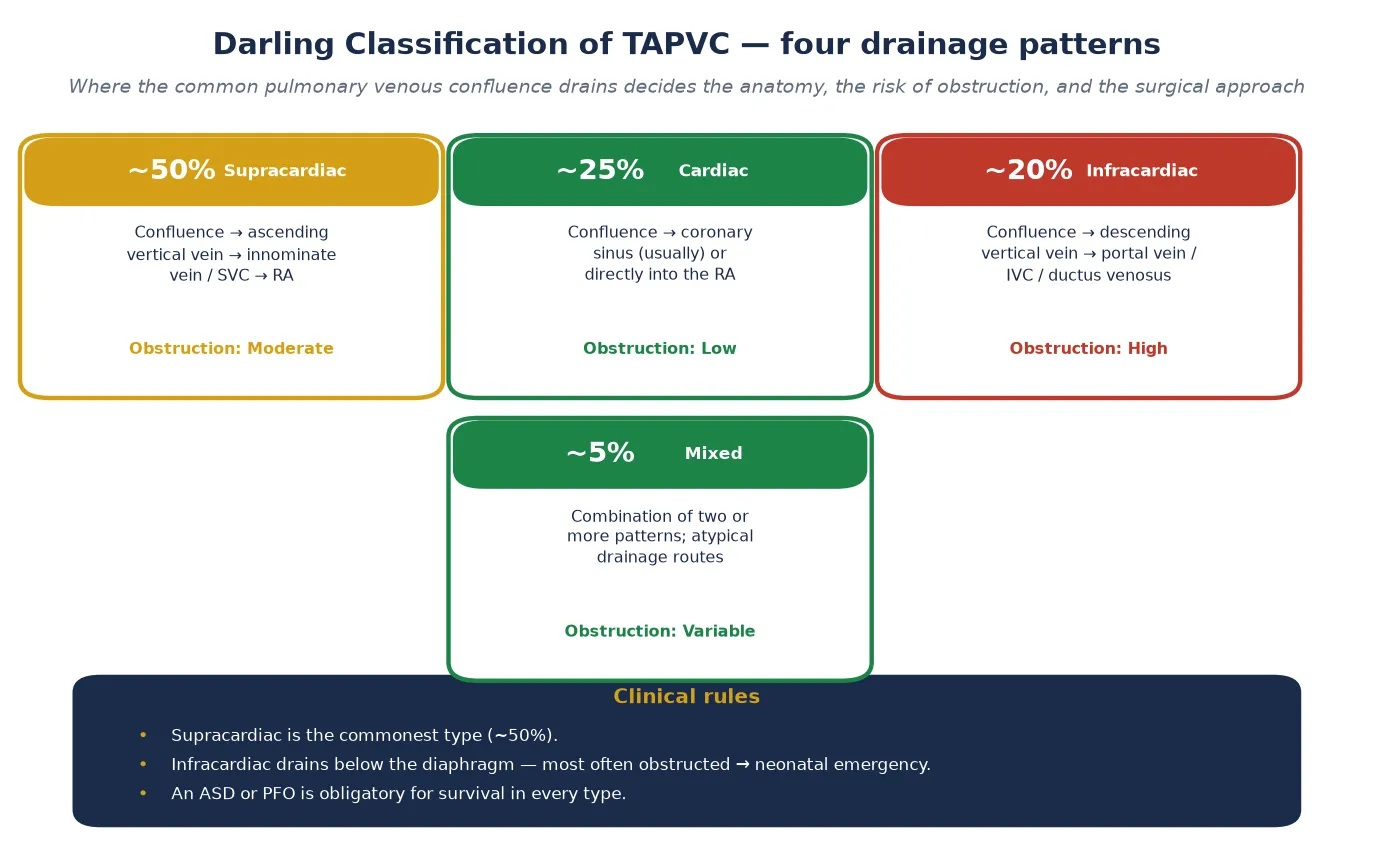
Classification rests on where the common pulmonary venous confluence drains, because that location predicts the risk of obstruction and shapes the surgical approach. The Darling system, which every fellowship candidate carries, names four patterns by the drainage route. [1] [7]
The supracardiac type is the commonest, accounting for about half of all cases. The four pulmonary veins collect into a confluence behind the heart, then an ascending vertical vein carries the blood up to the innominate vein or directly to the superior vena cava, and from there it reaches the right atrium. This pathway is relatively wide and short, so it is only moderately likely to obstruct. [1]
The cardiac type accounts for about a quarter of cases. Here the confluence drains into the coronary sinus, the venous channel that runs in the groove between the left atrium and the left ventricle, or sometimes directly into the right atrium. Because the coronary sinus is short and wide, this type is the least likely to obstruct, and it tends to present later with heart failure rather than as a neonatal emergency. [1] [7]
The infracardiac type accounts for about a fifth of cases and is the dangerous one. The confluence drains through a descending vertical vein that passes through the diaphragm to connect below to the portal vein, the inferior vena cava, or the ductus venosus. This long, narrow pathway, exposed to hepatic and portal pressures, is the one most likely to obstruct, which is why the infracardiac type is the classic neonatal surgical emergency. The mixed type, about five per cent, combines two or more drainage patterns and demands individualised imaging before any surgical plan. [5] [1]
Epidemiology & Risk Factors
Total anomalous pulmonary venous connection accounts for about one to one and a half per cent of congenital heart lesions, and it presents in roughly one to two of every ten thousand live births. It is not among the commonest defects, but it carries a disproportionate share of neonatal cardiac morbidity because the obstructed forms declare themselves in the first days of life. [11] [1]
A slightly higher rate is found when stillbirths and terminations are counted, because the lesion often coexists with other complex cardiac and extracardiac anomalies that carry their own mortality. The isolated form, by contrast, tends to be the one that presents as a single, treatable problem, and its outcome has improved markedly with modern neonatal surgery. [1]
The risk factor that matters for the fellowship answer is the association with heterotaxy syndromes, particularly asplenia (right atrial isomerism) and polysplenia (left atrial isomerism). In these syndromes the pulmonary venous drainage is frequently anomalous and obstructed, and the work-up must include an assessment of the situs, the splenic function, and the associated cardiac and abdominal anatomy. The asplenic child also needs antibiotic prophylaxis against overwhelming sepsis. [7] [1]
Prenatal diagnosis by fetal echocardiography identifies the confluence and its drainage route during the second-trimester scan, and antenatal detection improves the neonatal outcome by allowing planned delivery at or near a cardiac surgical centre. The impact-of-prenatal-diagnosis studies show that detected babies arrive in better condition, are stabilised and transferred immediately, and avoid the dangerous preoperative delay of the undiagnosed obstructed neonate. [4] [10]
Pathophysiology
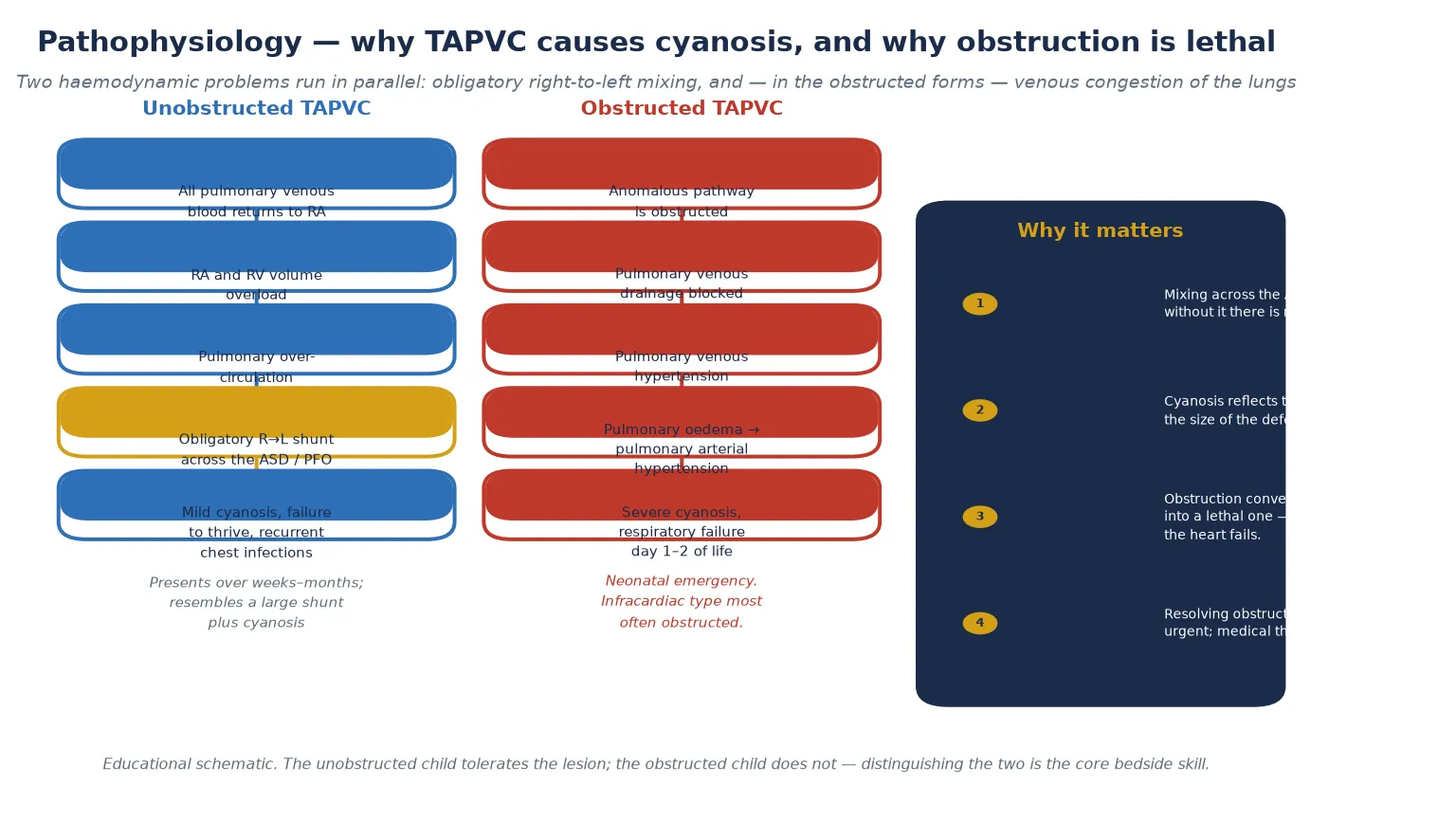
The pathophysiology turns on a single plumbing fact. All the oxygenated blood returning from the lungs is delivered to the right atrium instead of the left, so it mixes completely with the deoxygenated systemic venous return. The only way that mixed blood can reach the left atrium and the systemic circulation is by crossing an atrial communication, which is why an atrial septal defect or patent foramen ovale is obligatory for survival. [7] [1]
This obligatory right-to-left shunt is the source of the cyanosis, and it explains a point examiners probe: the degree of cyanosis reflects the amount of mixing and the pulmonary blood flow, not the size of the atrial defect. A larger atrial communication allows more mixing and a higher systemic output but also more desaturation, because the blood reaching the body is a blend of oxygenated and deoxygenated return. A restrictive septum, by contrast, limits the shunt and causes profound cyanosis with poor systemic output, which is why a balloon septostomy can be a life-saving bridge. [7]
In the unobstructed form, the right heart receives the entire pulmonary venous return plus the systemic venous return, so the right atrium and right ventricle are volume-loaded and the pulmonary bed is over-circulated. This behaves like a very large left-to-right shunt layered on top of the obligatory cyanosis, and it produces right heart dilation, pulmonary over-circulation, and heart failure over weeks to months rather than the collapse of the obstructed neonate. [1]
The danger, and the reason the obstructed form is lethal, is venous congestion of the lungs. When the anomalous pathway is narrowed, the pulmonary veins cannot empty, the pulmonary venous pressure rises, fluid leaks into the alveoli, and the lungs become oedematous. The rising pulmonary venous pressure also drives reflex pulmonary arterial vasoconstriction and secondary pulmonary hypertension. The result is severe cyanosis, respiratory failure, and shock within hours of birth. [7] [2]
The important clinical point is that the pulmonary arterial hypertension of the obstructed form is largely reversible if the obstruction is relieved promptly. The lungs flood before the heart fails, so a neonate who looks moribund can recover dramatically once the surgeon re-routes the blood. This is why prompt surgery is curative and delay is fatal, and why the resuscitation and the transfer run in parallel rather than in sequence. [2] [7]
Clinical Presentation
The presentation depends entirely on whether the anomalous pathway is obstructed, and the fellowship skill is to frame it as two distinct diseases that share an anatomy. The obstructed neonate is a surgical emergency; the unobstructed infant is an elective surgical problem. Recognising which one is in front of you is the first decision. [1] [7]
The obstructed neonate presents on day one or two of life with severe cyanosis, grunting respirations, and increasing work of breathing. The chest radiograph is the early clue: a normal-sized or even small heart with a diffuse, reticulogranular pattern of pulmonary oedema, sometimes a near white-out of the lung fields. The heart is quiet because it is not volume-loaded; the problem is upstream, in the obstructed veins. There is often no murmur, which makes the lesion easy to miss as lung disease. [7] [2]
The unobstructed infant presents over weeks to months with mild, persistent cyanosis, tachypnoea, poor feeding, sweating with feeds, failure to thrive, and recurrent chest infections. The right heart is volume-loaded, so there may be a right ventricular impulse, a soft systolic murmur of increased flow across the pulmonary valve, and occasionally a mid-diastolic flow rumble. The chest radiograph shows cardiomegaly with increased pulmonary vascular markings, the picture of a large shunt. [1]
The snowman or figure-of-eight cardiac silhouette is a classic radiograph sign of the older, unobstructed supracardiac patient, produced by the dilated vertical vein and the dilated superior vena cava forming the rounded upper border. It is rarely seen in the sick neonate, and a fellowship candidate should know that its absence does not exclude the diagnosis. The neonatal chest radiograph shows pulmonary oedema, not a snowman. [1] [7]
A restrictive atrial septum produces its own presentation, with severe cyanosis and poor systemic output that may improve transiently after a balloon septostomy enlarges the communication. This is the scenario that tests whether a candidate understands why the atrial septum is obligatory and what to do when it is too small. [7]
Differential Diagnosis
The differential splits into two bedside questions. In the obstructed neonate, what else causes cyanosis and pulmonary oedema on day one or two? In the unobstructed infant, what else causes cyanosis, a large shunt, and failure to thrive? The discriminating move in both is the echocardiogram. [7]
For the obstructed neonate, the dangerous mimics are neonatal respiratory distress syndrome, persistent pulmonary hypertension of the newborn, congenital pneumonia, and the other cyanotic congenital heart lesions. The time course helps: respiratory distress syndrome worsens from birth in a premature infant, whereas obstructed connection often presents in a term infant who was well for the first hours. The chest radiograph helps: a normal-sized heart with pulmonary oedema points to a venous obstruction, while a large heart with oligaemic or plethoric fields points elsewhere. [7] [1]
Persistent pulmonary hypertension of the newborn mimics the cyanosis and the right-to-left shunting, and it can be hard to distinguish clinically. The distinguishing feature is the pulmonary venous doppler on echocardiography: in persistent pulmonary hypertension the pulmonary veins drain normally to the left atrium, whereas in total anomalous connection they drain to an anomalous site. This is why the echo, not the hyperoxia test, closes the differential. [7]
The other cyanotic lesions to distinguish are transposition of the great arteries, which presents with cyanosis and a duct-dependent circulation, and hypoplastic left heart syndrome, which presents with shock as the duct closes. Both show their anatomy on echocardiography. The unobstructed total connection resembles a large left-to-right shunt such as a ventricular septal defect or atrioventricular septal defect, but the cyanosis is the tell, because a simple shunt lesion does not desaturate until it develops Eisenmenger physiology. [1]
| Feature | Obstructed TAPVC | Neonatal RDS | PPHN | Transposition |
|---|---|---|---|---|
| Onset | Day 1–2, term infant | From birth, often preterm | Term, first hours | From birth |
| Chest XR heart | Normal or small | Small, granular lungs | Normal, oligoaemic | Variable, egg-on-string |
| Lung fields | Pulmonary oedema | Ground-glass, low volume | Oligoaemic | Plethoric |
| Hyperoxia test | No rise, often falls | May rise with oxygen | Variable | No rise |
| Key echo | Anomalous confluence + obstruction | Normal heart | Normal pulmonary veins | Parallel great vessels |
Clinical & Bedside Assessment
The recognition move begins with the time course and the oxygen response. A term infant who was well at birth and turns blue on day one or two, with pulmonary oedema and little improvement on oxygen, is the obstructed neonate until the echocardiogram says otherwise. The general paediatrician's job is to hold that suspicion, start the stabilisation, and arrange the echo and the transfer without delay. [7] [1]
The history gathers the discriminators. Confirm the gestation and the birth history, because prematurity shifts the differential toward lung disease. Ask when the cyanosis began and whether it has progressed, because a sudden deterioration on day one or two fits an obstructed connection. Ask about feeding, weight gain, and respiratory symptoms over the preceding weeks for the unobstructed form, because failure to thrive and recurrent infections point to a large shunt. Ask about a prenatal cardiac scan, because a detected lesion changes the whole plan. [4] [7]
Examination is focused and rapid. Assess the work of breathing, the colour, and the perfusion, because these gauge the severity and the urgency. Feel the precordium: the obstructed neonate has a quiet heart, while the unobstructed infant has a right ventricular impulse. Auscultate for a murmur, but remember its absence does not exclude the lesion. Palpate the liver, because hepatomegaly signals right heart failure. Measure the pre- and post-ductal saturations and the four-limb blood pressures to map the shunt and the duct. [7] [1]
Inspect for the syndromic features that shape the work-up. Look for the features of heterotaxy, such as ambiguous situs, a midline liver, and asplenia, because these carry a high rate of anomalous pulmonary venous drainage and change the perioperative risk. The general paediatrician synthesises the findings into a one-line problem representation — for example, "a term two-day-old with sudden cyanosis, pulmonary oedema, and a quiet heart" — and that representation drives the urgent echocardiogram. [1] [7]
Investigations
Echocardiography is the single diagnostic investigation, and it answers every question the fellowship examiner will ask. Two-dimensional imaging shows the pulmonary venous confluence, the anomalous drainage route, and the atrial septum. Colour and pulse-wave doppler confirm the direction of flow and demonstrate any obstruction, shown as high-velocity or continuous turbulent flow along the anomalous pathway. The right ventricular size and the estimated pulmonary artery pressure complete the picture. [7] [1]
The key doppler skill is to interrogate the entire pulmonary venous pathway. Obstruction may sit at the origin of the vertical vein, where it crosses the diaphragm, or at its insertion into the portal or systemic vein, and a candidate who finds the confluence but misses the obstruction has not completed the study. The echocardiogram also confirms the obligatory atrial communication and assesses whether it is restrictive, which decides whether a balloon septostomy is needed. [1] [5]
The chest radiograph is the first bedside clue but is never diagnostic. In the obstructed neonate it shows a normal-sized heart with pulmonary oedema; in the unobstructed infant it shows cardiomegaly with increased pulmonary vascular markings. The snowman sign of the older supracardiac patient is a recognised but late feature. The electrocardiogram shows right ventricular hypertrophy and right axis deviation, supportive but not diagnostic. [1] [7]
Cardiac computed tomography or magnetic resonance imaging is indicated when the echocardiogram cannot fully define the drainage, which is most often the case with the mixed type or with complex associated anatomy. The cross-sectional imaging maps every pulmonary vein and its drainage site, and it is essential before surgery when the echo leaves doubt. Cardiac catheterisation is reserved for measuring pulmonary vascular resistance in the late-presenting or postoperative patient rather than for diagnosis, because echo and CT now define the anatomy. [1] [7]
The blood gas, the lactate, and the mixed venous saturation quantify the severity of the cyanosis and the shock before transfer. A metabolic acidosis with a rising lactate signals a failing circulation and raises the urgency. These bedside measures are part of the resuscitation, and they are repeated to track the response. [7]
Management — Resuscitation
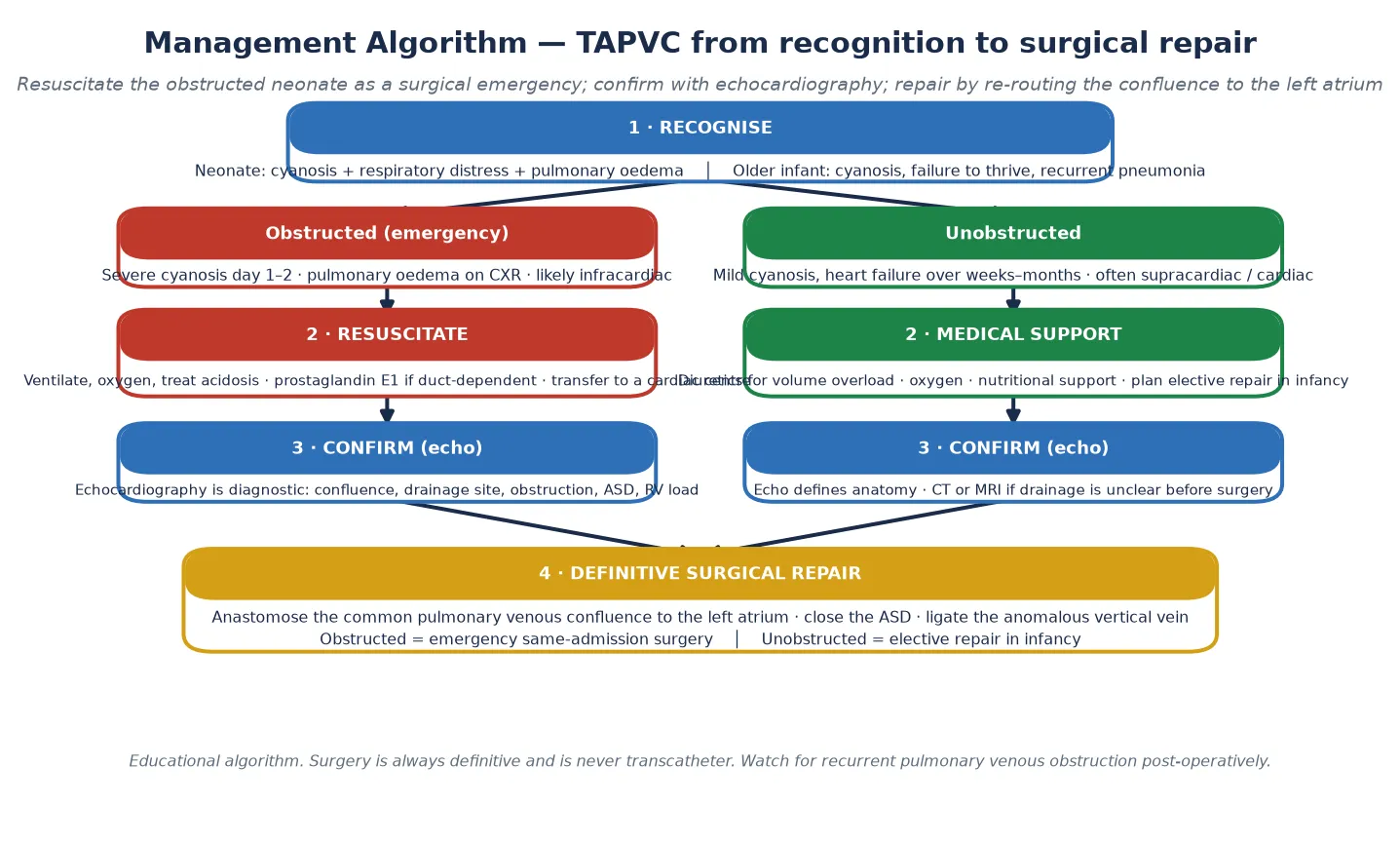
Resuscitation in total anomalous pulmonary venous connection applies almost entirely to the obstructed neonate, who is a surgical emergency. The priorities are to support the airway, breathing, and circulation while arranging urgent transfer to a congenital cardiac surgical centre. The resuscitation and the transfer run in parallel, not in sequence, because waiting for the oxygenation to improve before moving the child is a fatal error. [7] [2]
The infant is intubated and ventilated, with oxygen to lower the pulmonary vascular resistance and improve oxygenation. Metabolic acidosis is corrected with fluid and bicarbonate, and inotropic support is started for poor perfusion. The goal is to deliver a stable, oxygenated, perfused child to the operating theatre, and every minute of delay lets the pulmonary oedema and the pulmonary hypertension worsen. [7]
The role of prostaglandin E1 in isolated obstructed connection is debated, and a fellowship candidate should be able to discuss this honestly. Prostaglandin maintains ductal patency, but in isolated obstructed connection the ductus is not the primary problem, so its use is reserved for the genuinely duct-dependent or the unstable circulation where maintaining the duct offers a temporary right-to-left pop-off. Inhaled nitric oxide is used cautiously, because lowering the pulmonary arterial pressure without relieving the venous obstruction can worsen the pulmonary oedema. [7] [2]
A restrictive atrial septum is a specific problem that needs a specific bridge. When the atrial communication is too small to allow adequate systemic output, a balloon atrial septostomy enlarges it and can dramatically improve the oxygenation as a temporary measure while the definitive surgery is arranged. In the sickest neonates who cannot be stabilised, extracorporeal membrane oxygenation may be used as a bridge to the operating theatre. [7]
Management — Definitive & Stepwise
The definitive treatment is surgical repair, and it is always surgical because the problem is a drainage error that needs anatomical re-routing. No transcatheter device can re-connect the pulmonary veins to the left atrium, which is the clearest contrast with a secundum atrial septal defect that a device can plug. The operation is performed by a congenital cardiac surgeon with cardiopulmonary bypass. [7] [8]
On cardiopulmonary bypass, the surgeon creates a wide anastomosis between the common pulmonary venous confluence and the left atrium, so that oxygenated blood flows directly to the left heart. The atrial septal defect is then closed, restoring the normal separation of the circulations, and the anomalous vertical vein is ligated and divided, abolishing the abnormal drainage pathway. The exact technique adapts to the anatomy: the cardiac-to-coronary-sinus type is repaired by unroofing the coronary sinus into the left atrium, while the infracardiac type requires a confluence-to-left-atrium anastomosis above the diaphragm. [1] [7]
The timing is set by the obstruction. The obstructed neonate is repaired as an emergency in the same admission, because the pulmonary oedema and the pulmonary hypertension will not resolve until the obstruction is relieved. The unobstructed infant is repaired electively in early infancy, allowing growth and stabilisation before a planned operation. The Karamlou analysis of the Society of Thoracic Surgeons database showed that preoperative obstruction, lower weight, and younger age were independently associated with higher mortality and reoperation, which frames the risk counselling. [2]
The immediate postoperative period is managed in the cardiac intensive care unit. The priorities are to support the myocardium, manage the pulmonary vascular resistance, and detect early complications such as bleeding, low cardiac output, phrenic nerve injury, and arrhythmia. Serial echocardiography confirms the repair, the absence of a residual shunt, and the patency of the pulmonary venous anastomosis, because early obstruction can declare itself within days. [7] [3]
The surgical repair in four steps
Wide anastomosis between the common pulmonary venous confluence and the left atrium, restoring normal inflow.
Closure of the atrial septal defect, separating the systemic and pulmonary circulations.
Ligation and division of the anomalous vertical vein, abolishing the abnormal drainage pathway.
Intraoperative and early postoperative echocardiography to confirm a patent anastomosis and no residual shunt.
Specific Subtypes & Scenarios
The supracardiac type, the commonest at about half of cases, drains via an ascending vertical vein to the innominate vein or superior vena cava. It is only moderately likely to obstruct, so it often presents as the unobstructed infant with a large shunt and cyanosis. The repair redirects the confluence to the left atrium and ligates the vertical vein. The snowman sign on the chest radiograph of the older unobstructed patient is the classic image of this type. [1] [7]
The cardiac type, about a quarter, drains to the coronary sinus or directly to the right atrium. It is the least likely to obstruct and tends to present later with heart failure. The repair for the coronary sinus variant unroofs the sinus into the left atrium and closes the atrial septal defect, which reroutes the coronary venous return and the pulmonary venous return into the left atrium. [1]
The infracardiac type, about a fifth, is the dangerous one. It drains via a descending vertical vein below the diaphragm to the portal vein, the inferior vena cava, or the ductus venosus, and it is the type most likely to obstruct. It presents as the neonatal surgical emergency with pulmonary oedema and severe cyanosis, and the repair is urgent. The long, narrow pathway below the diaphragm is the anatomical reason for the obstruction. [5] [2]
The mixed type, about five per cent, combines two or more drainage patterns and demands individualised cross-sectional imaging before any surgical plan, because a standard approach may miss an anomalous vein. Each pulmonary vein must be traced to its drainage site, and the operation is tailored to the anatomy. [1] [7]
The restrictive atrial septum is a scenario that tests whether a candidate understands the obligatory mixing. A small atrial communication limits the systemic output and causes profound cyanosis, and a balloon atrial septostomy enlarges it as a bridge to surgery. The late-presenting adult with an unobstructed lesion may present with pulmonary vascular disease or atrial arrhythmia, and the closure decision depends on whether the pulmonary vascular resistance is still reversible. [7] [8]
Complications & Pitfalls
Recurrent pulmonary venous obstruction is the most feared late complication, and it drives the entire postoperative surveillance strategy. It presents weeks to months after repair with pulmonary oedema, rising pulmonary pressures on echocardiography, and high-velocity flow at the anastomosis. The child may have tachypnoea, poor feeding, and recurrent respiratory symptoms, and the diagnosis is confirmed on echo and catheterisation. [3] [6]
The two forms of recurrence carry different prognoses. Anastomotic obstruction is a discrete narrowing at the surgical join, and it may be amenable to surgical revision or transcatheter balloon dilation with stenting. Diffuse intrinsic pulmonary vein stenosis extends into the pulmonary veins themselves, is driven by intimal proliferation, carries a poor prognosis, and is the form most associated with the lethal late course. The sutureless marsupialisation technique, which leaves the obstructed vein alone and enlarges the atrial communication around it, is favoured for recurrent diffuse disease. [6] [3]
The early postoperative complications are those of any neonatal cardiac surgery: bleeding, low cardiac output, phrenic nerve injury, and arrhythmia. Residual pulmonary hypertension may persist or progress in the patient repaired late or with established vascular disease, and it needs surveillance. These complications are managed in the cardiac intensive care unit with the standard supports. [7]
The diagnostic pitfalls share a common root: mistaking the obstructed neonate for lung disease. The cyanosis, the pulmonary oedema, and the lack of a murmur all point toward respiratory distress syndrome or pneumonia, and the trap is to escalate the respiratory support rather than to image the heart. A second pitfall is delaying surgery while awaiting improved oxygenation, which is a fatal error because the obstruction will not resolve. A third is underestimating the obstruction by not interrogating the whole venous pathway on echo. The safeguard is a low threshold for echocardiography in any cyanosed neonate and an early transfer to a cardiac centre. [7] [1]
Prognosis & Disposition
The overall surgical mortality in the modern era is roughly five to ten per cent for an uncomplicated repair, and it has fallen steadily with improvements in neonatal surgery and intensive care. The mortality rises steeply with obstruction, low birth weight, young age, and associated lesions, as the Society of Thoracic Surgeons database analysis showed, and these factors frame the risk counselling for the obstructed neonate. [2] [7]
The timing of repair is the single biggest determinant of outcome. Prompt surgery in the obstructed neonate relieves the obstruction before the pulmonary hypertension becomes fixed, and the right heart and the pulmonary bed recover. A patient repaired late, or one who develops recurrent pulmonary venous obstruction, faces a measurable reduction in survival and quality of life. The lesson is that the disease is curable when treated in time, and the natural history of a serious illness when it is not. [1] [3]
For the patient without recurrent obstruction, the prognosis is excellent. Growth and function are near-normal, exercise tolerance returns, and the child lives a full life. The residual risk is small but real, and it is the reason the follow-up never fully ends. Pulmonary hypertension may persist in those repaired late, and atrial arrhythmia remains more common than in the general population. These residual risks are the substance of the adult congenital follow-up. [8] [9]
The general paediatrician owns the recognition and the referral, and the disposition is shared, structured care. Paediatric cardiology drives the repair and the early follow-up. The adult congenital cardiology service takes over at transition and provides the lifelong surveillance for recurrent obstruction, pulmonary hypertension, and arrhythmia. A named coordinator prevents the fragmentation that is the enemy of a lifelong plan, and the transition to adult care is structured and documented. [8] [9]
Special Populations
Total anomalous pulmonary venous connection interacts with the child's social, geographic, and developmental context, and the same surgical plan behaves differently across populations. Access to a congenital cardiac surgical centre, to timely retrieval, and to lifelong follow-up are the determinants of outcome, and a plan that is clinically correct but unattainable for a family is no plan at all. [7] [8]
Indigenous children in Australia and Aotearoa New Zealand may face later presentation through reduced access to prenatal diagnosis, echocardiography, and specialist referral, particularly in remote communities. An obstructed neonate in a remote setting depends on a retrieval service that can deliver stabilisation and transport within hours, and a low threshold to image the heart and to transfer is the safeguard. Telehealth and outreach extend the diagnostic and follow-up net into communities that a clinic-based model would miss. [8] [7]
Migrant, refugee, and asylum-seeking families may arrive with no prenatal diagnosis and an uncertain cardiac history, and the lesion may not have been detected in the country of origin. A careful history, a cardiovascular examination at the arrival health check, and an echocardiogram for any cyanosed or failing infant are the foundations. The heterotaxy association is particularly relevant here, because these syndromes may be undiagnosed and carry the asplenia risk that needs antibiotic prophylaxis. [7]
Socioeconomic disadvantage shapes access to surgery, to transport, and to follow-up. The limiting step is often logistics — travel to the cardiac centre, accommodation near the hospital, time off work — rather than the procedure itself. Structuring the repair and the follow-up around a coordinated visit, linking the family to transport and accommodation support, and using telehealth to reduce travel all improve engagement. The transition to adult congenital care is the point at which young people are most often lost to follow-up, and targeted support at that transition protects the long-term outcome. [8] [9]
Evidence, Guidelines & Regional Differences
The evidence base rests on the Seale international population-based morphology and outcome study, which defined the Darling distribution and the obstruction rates across a large cohort, and the Karamlou analysis of 377 children in the Society of Thoracic Surgeons database, which identified the factors associated with mortality and reoperation. These two studies frame the risk and the natural history that every fellowship candidate carries. [1] [2]
The Seale postoperative pulmonary venous obstruction outcome study and the UK, Ireland and Sweden pulmonary vein stenosis collaborative study define the most feared late complication, its two forms, and its prognosis. Together they justify the intensive postoperative surveillance and the sutureless repair strategy for recurrent disease. The Voleti Chivukula 2025 Clinics in Perinatology review is a current single-source reference for the neonatal presentation and the management. [3] [6]
The 2018 American Heart Association and American College of Cardiology guideline for the management of adults with congenital heart disease, and the 2020 European Society of Cardiology guideline for adult congenital heart disease, frame the lifelong follow-up after repair, including the surveillance for recurrent obstruction, pulmonary hypertension, and arrhythmia, and the structured transition to adult care. These guidelines are the operational standard for the adult congenital service. [8] [9]
Where the evidence is weak, a fellowship answer says so honestly. The role of prostaglandin E1 in isolated obstructed connection is debated, and the rationale turns on whether the ductus offers a useful pop-off. The optimal timing of elective repair in the unobstructed infant is not fully settled, and the role of prenatal balloon atrial septostomy for the restrictive septum is still being defined. The long-term outcome of the sutureless repair relative to conventional re-anastomosis for diffuse stenosis is accumulating. Naming these uncertainties is a mark of intellectual honesty that examiners reward. [7] [6]
In Australia and Aotearoa New Zealand, total anomalous pulmonary venous connection is managed according to the international guidelines, with paediatric cardiology and congenital cardiac surgery concentrated in the major centres. The obstructed neonate in a rural or remote setting depends on a retrieval service for stabilisation and transport, and telehealth extends the diagnostic and follow-up net. Repair is performed in the congenital cardiac centres, and the transition to adult congenital cardiology happens in the late teens. The Cardiac Society of Australia and New Zealand provides the operational standard. [8] [9]
Exam Pearls
A fellowship candidate answering on total anomalous pulmonary venous connection should land five anchor points and avoid three classic traps. The anchors are the framework examiners listen for, and the traps are where easy marks are lost. [1] [7]
Anchor one: recognise the obstructed neonate. A cyanosed neonate with pulmonary oedema on day one or two has obstructed total anomalous connection until the echo proves otherwise. The hyperoxia test does not discriminate here; the echo does. [7]
Anchor two: classify by the Darling system. Supracardiac is the commonest at about half, cardiac about a quarter, infracardiac about a fifth, and mixed about five per cent. The infracardiac type is the one most likely to obstruct. [1]
Anchor three: understand the obligatory atrial septum. An atrial septal defect or patent foramen ovale is obligatory for survival, because it is the only route for oxygenated blood to reach the systemic circulation. A restrictive septum may need a balloon septostomy. [7]
Anchor four: repair is always surgical. The operation anastomoses the confluence to the left atrium, closes the atrial defect, and ligates the anomalous vein. There is no transcatheter option, and the obstructed neonate is repaired as an emergency. [2]
Anchor five: survey for recurrent obstruction. Recurrent pulmonary venous obstruction is the most feared late complication, and it drives the lifelong follow-up. Anastomotic obstruction may be dilated, but diffuse stenosis carries a poor prognosis. [3]
The three traps to avoid are mistaking the obstructed neonate for lung disease, delaying surgery while awaiting improved oxygenation, and forgetting that there is no transcatheter option. Supracardiac accounts for about half, the infracardiac type most often obstructs, an atrial septal defect is obligatory for survival, and the repair is always surgical — the high-yield facts a candidate holds. [1] [7]
References
- [1]Seale AN, Uemura H, Webber SA, Partridge J, Roughton M, Ho SY, McCarthy KP, Jones S, Shaughnessy L, Sunnegardh J, Hanseus K, Berggren H, Johansson S, Rigby ML, Keeton BR, Daubeney PE, British Congenital Cardiac Association. Total anomalous pulmonary venous connection: morphology and outcome from an international population-based study. Circulation, 2010.PMID 21135364
- [2]Karamlou T, Gurofsky R, Al Sukhni E, Coles JG, Williams WG, Caldarone CA, Van Arsdell GS, McCrindle BW. Factors associated with mortality and reoperation in 377 children with total anomalous pulmonary venous connection. Circulation, 2007.PMID 17353446
- [3]Seale AN, Uemura H, Webber SA, Partridge J, Roughton M, Ho SY, McCarthy KP, Jones S, Shaughnessy L, Sunnegardh J, Hanseus K, Berggren H, Johansson S, Rigby ML, Keeton BR, Daubeney PE, British Congenital Cardiac Association. Total anomalous pulmonary venous connection: outcome of postoperative pulmonary venous obstruction. J Thorac Cardiovasc Surg, 2013.PMID 22892140
- [4]Seale AN, Carvalho JS, Gardiner HM, Mellander M, Roughton M, Simpson J, Tometzki A, Uzun O, Webber SA, Daubeney PE, British Congenital Cardiac Association. Total anomalous pulmonary venous connection: impact of prenatal diagnosis. Ultrasound Obstet Gynecol, 2012.PMID 22262371
- [5]Seale AN, Uemura H, Sethia B, Magee AG, Ho SY, Daubeney PE. Total anomalous pulmonary venous connection to the supradiaphragmatic inferior vena cava. Ann Thorac Surg, 2008.PMID 18291209
- [6]Seale AN, Webber SA, Uemura H, Partridge J, Roughton M, Ho SY, McCarthy KP, Jones S, Shaughnessy L, Sunnegardh J, Hanseus K, Rigby ML, Keeton BR, Daubeney PE, British Congenital Cardiac Association. Pulmonary vein stenosis: the UK, Ireland and Sweden collaborative study. Heart, 2009.PMID 19737738
- [7]Voleti Chivukula S. Total Anomalous Pulmonary Venous Connections. Clin Perinatol, 2025.PMID 41233009
- [8]Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, Crumb SR, Dearani JA, Fuller S, Gurvitz M, Khairy P, Landzberg MJ, Saidi A, Valente AM, Van Hare GF. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol, 2019.PMID 30121239
- [9]Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Lung B, Kluin J, Lang IM, Meijboom F, Moons P, Mulder BJM, Oechslin E, Roos-Hesselink JW, Schwerzmann M, Sondergaard L, Zeppenfeld K, ESC Scientific Document Group. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J, 2021.PMID 32860028
- [10]van Velzen CL, Clur SA, Rijlaarsdam ME, Bax CJ, Pajkrt E, Heymans MW, Bekker MN, Hruda J, de Groot CJ, Blom NA, Haak MC. Prenatal detection of congenital heart disease - results of a national screening programme. BJOG, 2016.PMID 25625301
- [11]Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol, 2002.PMID 12084585