Paeds · cardiology
Transposition of the great arteries
Also known as Transposition of the great arteries · d-TGA · Complete transposition · Ventriculoarterial discordance · Jatene arterial switch · Simple transposition · TGA with ventricular septal defect · TGA with left ventricular outflow tract obstruction
Fellowship guide to transposition of the great arteries (d-TGA): the parallel-circulation problem that presents as deepening neonatal cyanosis with little respiratory distress, the anatomy that splits it into simple, VSD and LVOTO subtypes, the recognition sequence from failed hyperoxia test to diagnostic echocardiogram, the resuscitation trio of prostaglandin E1, balloon atrial septostomy and definitive arterial switch (Jatene), and the long-term legacy of the atrial-switch era.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The organising principle is the parallel circulation. In a normal heart the right ventricle pumps to the lungs, the left ventricle pumps to the body, and the two loops sit in series so that every drop of blood passes through both. In d-TGA the right ventricle pumps deoxygenated blood back into the aorta and around the body, while the left ventricle pumps oxygenated blood straight back to the lungs, so the two loops never connect in the intended way. The body can only receive oxygen if some blood spills between the loops at the duct, the atrial septum or a ventricular septal defect. When that mixing fails — typically as the duct closes in the first day or two of life — cyanosis deepens, lactate rises, and the infant heads towards cardiovascular collapse. [2] [3]
This page covers the full breadth of d-TGA for a fellowship candidate: the anatomy and its three subtypes, the parallel-circulation physiology, the recognition sequence from a failed hyperoxia test to a diagnostic echocardiogram, the resuscitation trio of prostaglandin E1, balloon atrial septostomy and arterial switch, the surgical legacy of the atrial-switch (Mustard and Senning) era, and the long-term neuropsychological and exercise outcomes that shape follow-up. It cross-links to the cyanotic newborn and duct-dependent congenital heart disease leaves rather than repeating the general stabilisation pathway. [1] [4]
Overview & Definition
d-Transposition of the great arteries is defined by atrioventricular concordance with ventriculoarterial discordance. The right atrium connects normally to the right ventricle, and the left atrium to the left ventricle, but the aorta arises from the morphologic right ventricle and the pulmonary artery from the morphologic left ventricle. The great vessels lie side by side rather than wrapped around each other, giving the aorta an anterior position and the pulmonary artery a posterior position — the origin of the "dextro" (d-) label, although in modern usage d- refers to the rightward position of the aortic valve relative to the pulmonary valve rather than to dextrocardia. [2] [1]
It is the most common cyanotic congenital heart lesion to present in the neonatal period, and it is the lesion most likely to cause critical illness from a closing ductus in an otherwise well term infant. Untreated, the natural history documented before the surgical era was grim: the Liebman cohort from 1969 showed that around ninety per cent of infants with complete transposition died within the first year of life, almost all from progressive hypoxaemia as mixing sites closed. [3] Modern repair has transformed this prognosis — survival into adulthood is now the expectation rather than the exception — but the lesion has lost none of its urgency at first presentation. [4] [12]
Classification
The clinically useful classification of d-TGA rests on the ventricular septum and the left ventricular outflow tract, because these two features decide both how well the infant mixes and which operation will be possible. The figure below splits d-TGA into its three subtypes and sets out the diagnostic work-up that every neonate with the lesion needs. [1] [2]
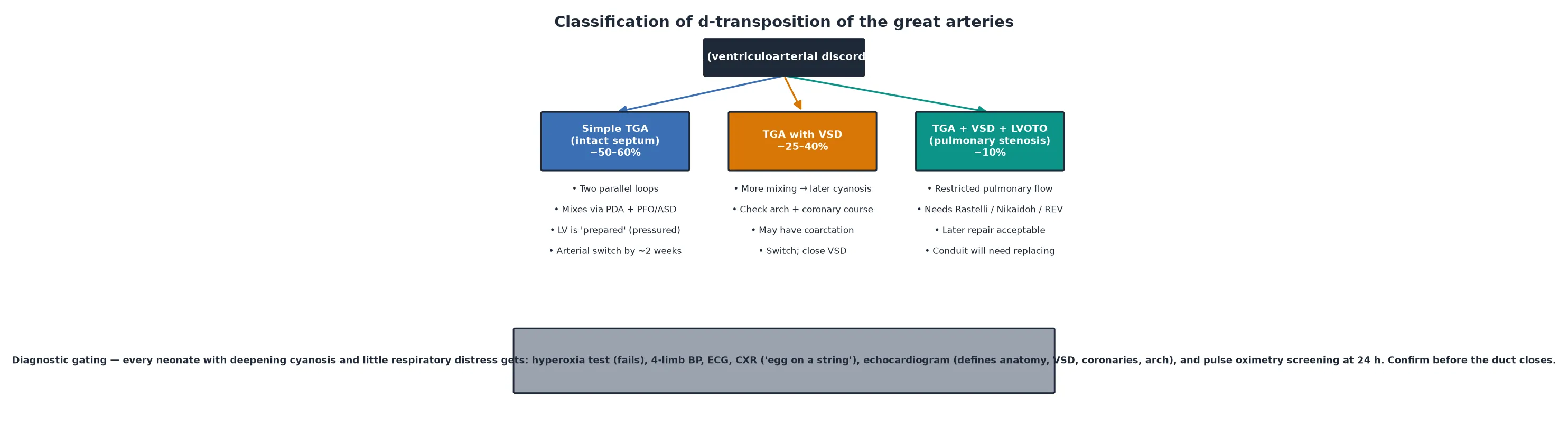
Simple TGA (intact septum)
- ~50–60% of cases: two parallel loops, no VSD
- Mixing relies on the ductus and the atrial septum (PFO/ASD)
- Left ventricle is 'prepared' — still at systemic pressure before pulmonary vascular resistance falls
- Arterial switch (Jatene) within ~2 weeks of life
TGA with VSD
- ~25–40% of cases: more mixing, so cyanosis may appear later
- Define arch (exclude coarctation/interruption) and coronary course
- Pulmonary over-circulation can dominate once PVR falls
- Arterial switch with VSD closure, usually in the first weeks
TGA + VSD + LVOTO
- ~10%: pulmonary stenosis restricts pulmonary blood flow
- Switch often not feasible — left ventricle cannot support systemic output past obstruction
- Rastelli, Nikaidoh or Révol (REV) procedures reroute flow
- Later repair acceptable; RV-to-PA conduit will need replacing
Taussig-Bing anomaly
- d-TGA with a subpulmonary (malalignment) VSD
- Great arteries are side-by-side; presents with heart failure and cyanosis
- Repaired with an arterial switch plus VSD redirection to the neoaortic valve
- Higher early surgical risk than simple TGA
Epidemiology & Risk Factors
d-TGA occurs in roughly two to three per ten thousand live births and accounts for around five to seven per cent of all congenital heart disease. Unlike many cyanotic lesions it is usually an isolated cardiac defect — extracardiac anomalies and chromosomal syndromes are uncommon, which is a useful discriminator from, for example, tetralogy of Fallot associated with 22q11.2 deletion. There is a consistent male predominance of around two to three to one. [2]
The strongest recognised maternal risk factor is pregestational diabetes, which raises the risk of conotruncal and outflow-tract lesions including d-TGA. Assisted reproductive technology, advanced maternal age, maternal smoking, and exposure to certain medications in early pregnancy have all been associated with a modestly increased risk. The sibling recurrence risk for congenital heart disease in general sits around two to three per cent, and d-TGA in a first-degree relative roughly doubles background risk — relevant to counselling but not usually to a syndromic work-up, which is seldom required. [2] [1]
Why d-TGA is a neonatal emergency — the 'comfortably blue' infant
Pathophysiology
The single concept that explains everything in d-TGA is the parallel circulation, shown against the normal in-series circuit in the figure below. In a normal heart the right ventricle sends deoxygenated blood to the lungs, oxygenated blood returns to the left atrium and left ventricle, and the left ventricle pumps it to the body, so each red cell passes through both circuits in turn. In d-TGA the right ventricle pumps deoxygenated blood into the aorta and the left ventricle pumps oxygenated blood into the pulmonary artery, so the systemic loop recirculates deoxygenated blood and the pulmonary loop recirculates oxygenated blood. [2] [1]
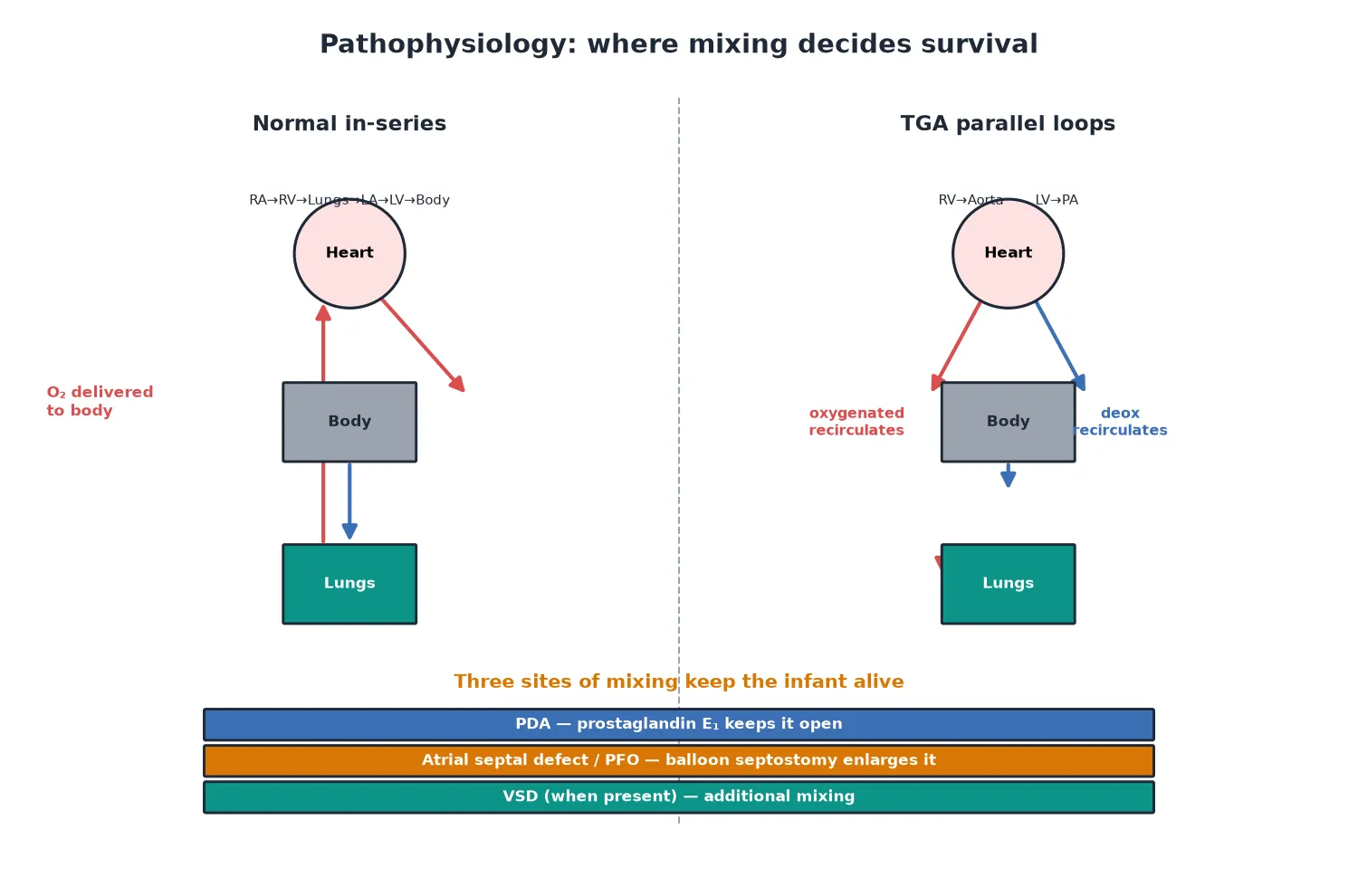
Because the two loops are separate, total systemic oxygen delivery depends almost entirely on the volume of bidirectional shunt at the mixing sites. A large patent ductus, a generous atrial septal defect or a ventricular septal defect allows enough exchange to keep the saturation acceptable; as the ductus closes over the first day or two, mixing falls, the arterial oxygen content drops, and the body extracts more oxygen per litre of blood, producing a rising lactate and a metabolic acidosis. Pulmonary blood flow is usually increased, which is why the infant often shows little respiratory distress despite deep cyanosis — the gas exchange surface is well perfused, it is simply being fed blood that has nowhere useful to go. [2]
The left ventricle is a critical player in surgical planning. In simple d-TGA with an intact septum the left ventricle pumps only to the low-resistance pulmonary bed, so once pulmonary vascular resistance falls over the first weeks of life the left ventricle deconditions and its wall mass falls. A left ventricle that has deconditioned cannot immediately take over systemic pressures at an arterial switch, which is why simple d-TGA is switched early — within the first two weeks, and at some centres even earlier — while the left ventricle is still prepared. A ventricular septal defect keeps the left ventricle at higher pressure for longer, which buys more time, but it also raises the risk of pulmonary over-circulation and early pulmonary vascular disease. [1] [4]
What the parallel circulation produces
- Deep cyanosis with little work of breathing (lungs well perfused)
- Rising lactate and metabolic acidosis as the duct closes and mixing falls
- Differential cyanosis when a PDA carries oxygenated blood to the lower body
- Pulmonary over-circulation once PVR falls, especially with a VSD
What determines the surgical plan
- Intact septum → early switch before the LV deconditions
- VSD → switch plus closure, more time available
- Left ventricular outflow tract obstruction → switch often not feasible
- Coronary anatomy → must be mapped, it dictates switch safety
Clinical Presentation
The classic presentation is a term infant who becomes progressively cyanosed over the first hours to days of life and who, tellingly, does not look like a sick respiratory baby. The infant is often described as 'comfortably blue' — centrally cyanosed but breathing comfortably, feeding, and showing little distress — because the pulmonary circulation is generous and the gas exchange apparatus is intact. A murmur is frequently absent, which can falsely reassure the examiner. As the ductus arteriosus closes, the saturation falls further, the infant becomes irritable and then lethargic, and a metabolic acidosis develops from tissue hypoxia. [2] [1]
Differential cyanosis is a pathognomonic clue when present: the lower limbs (perfused across a ductus from the pulmonary artery, carrying oxygenated blood) appear pinker than the upper body (perfused by the aorta carrying deoxygenated blood). Reverse differential cyanosis — hands pinker than feet — suggests d-TGA with a ductus and persistent pulmonary hypertension of the newborn shunting deoxygenated blood across the duct. Either pattern should prompt urgent echocardiography. The general paediatrician must remember that antenatal detection is improving but remains incomplete, and that a normal antenatal scan does not exclude critical congenital heart disease. [9] [2]
Differential Diagnosis
The neonate with deepening cyanosis generates a focused differential that pivots on the hyperoxia test and the chest X-ray. A failure to raise the partial pressure of oxygen above around one hundred millimetres of mercury on one hundred per cent oxygen points to a fixed intracardiac right-to-left shunt rather than a diffusely under-ventilated lung, and d-TGA sits at the top of that list alongside the other cyanotic congenital heart lesions. [2] [1]
Cyanotic congenital heart disease
- d-TGA: deep cyanosis, little distress, fails hyperoxia, egg-on-a-string CXR
- Tetralogy of Fallot: varies with right ventricular outflow obstruction, murmur, normal-to-oligaemic lung fields
- Total anomalous pulmonary venous connection: cyanosis, 'snowman' sign, pulmonary oedema
- Tricuspid atresia / pulmonary atresia: cyanosis depends on the source of pulmonary blood flow
Non-cardiac neonatal cyanosis
- Respiratory distress syndrome, transient tachypnoea, meconium aspiration: usually distress and abnormal CXR
- Persistent pulmonary hypertension of the newborn: right-to-left shunting, often differential cyanosis
- Sepsis / pneumonia: systemic signs, inflammatory markers
- Methaemoglobinaemia: saturation unresponsive to oxygen with a chocolate-brown blood sample
The practical point for the ward and emergency department is that a cyanosed neonate with little respiratory distress should be assumed to have a duct-dependent cyanotic heart lesion until an echocardiogram proves otherwise, and prostaglandin E1 should be started on clinical suspicion while the definitive test is arranged. Waiting for complete certainty before starting prostaglandin E1 is the most dangerous single error in this presentation, because the cost of the infusion (apnoea, fever) is reversible while the cost of delay (cardiovascular collapse) may not be. [10] [2]
Clinical & Bedside Assessment
The bedside assessment of the suspected d-TGA is brief and decisive because the definitive test is the echocardiogram. Four-limb blood pressures look for a coarctation or interrupted arch (a differential between upper and lower limb pressures). Pre- and post-ductal saturations map the shunt: a lower post-ductal saturation supports right-to-left ductal flow, while a higher post-ductal saturation is the differential cyanosis of d-TGA. Peripheral pulses, precordial activity, and the presence and character of any murmur are documented, but their absence does not exclude the lesion. [2] [1]
Pulse oximetry screening, performed at twenty-four hours of life, was added to newborn examination precisely to catch lesions like d-TGA that can be missed before ductal closure. The American Heart Association and American Academy of Pediatrics scientific statement defines a positive screen as a saturation below ninety per cent, or between ninety and ninety-five per cent on three consecutive measurements, or a differential of three percentage points or more between the right hand and a foot. The Swedish screening study of nearly forty thousand newborns showed that adding pulse oximetry detected the majority of duct-dependent lesions that were otherwise missed, and the PulseOx test-accuracy study confirmed a sensitivity adequate for population screening. [7] [8] [9]
Investigations
The investigation pathway confirms the lesion, defines the anatomy for the surgeon, and excludes the mimics. Echocardiography is the diagnostic test and is performed as soon as the diagnosis is suspected; the other tests support the assessment and the resuscitation. [1] [2]
Investigation sequence for suspected d-TGA
Hyperoxia test: fails (PaO₂ stays low on 100% oxygen) → fixed intracardiac shunt
Arterial blood gas: hypoxaemia with a metabolic acidosis as the duct closes
Four-limb blood pressures and pre/post-ductal saturations: map the shunt and the arch
Chest X-ray: 'egg on a string' — narrow mediastinum, egg-shaped cardiac silhouette, increased pulmonary markings
ECG: usually normal for age (right ventricular dominance is normal in the neonate)
Echocardiogram (diagnostic): defines the great-vessel origins, VSD, coronary pattern, arch, duct and atrial septum
The echocardiogram does the decisive work. It confirms that the aorta arises from the right ventricle and the pulmonary artery from the left ventricle, measures the atrial and ventricular septal defects, defines the ductus, excludes a coarctation or interrupted arch, and — critically for surgical planning — maps the coronary artery anatomy. Coronary patterns vary in d-TGA, and an unusual course (for example a single coronary or an intramural segment) raises the technical risk of the arterial switch, because the coronaries must be excised and reimplanted onto the neoaorta. The echo also assesses left ventricle readiness by estimating left ventricular pressure, often from the ventricular septal geometry or a tricuspid regurgitation jet. [1] [4]
Pulse oximetry screening for CCHD — Swedish cohort (de-Wahl Granelli 2009)
Prospective screening study of 39,821 newborns comparing pulse oximetry plus clinical examination to clinical examination alone
Practice change
Pulse oximetry at 24 h is now a standard part of newborn CCHD screening and catches d-TGA before ductal collapse
Management — Resuscitation
The resuscitation of d-TGA is a sequence built around securing mixing until a definitive repair can be performed, shown in the algorithm below. The first action on suspicion of a duct-dependent cyanotic lesion is to start prostaglandin E1 to keep the ductus open, and the first decision after stabilisation is whether mixing is adequate or whether an urgent balloon atrial septostomy is needed. [10] [1]
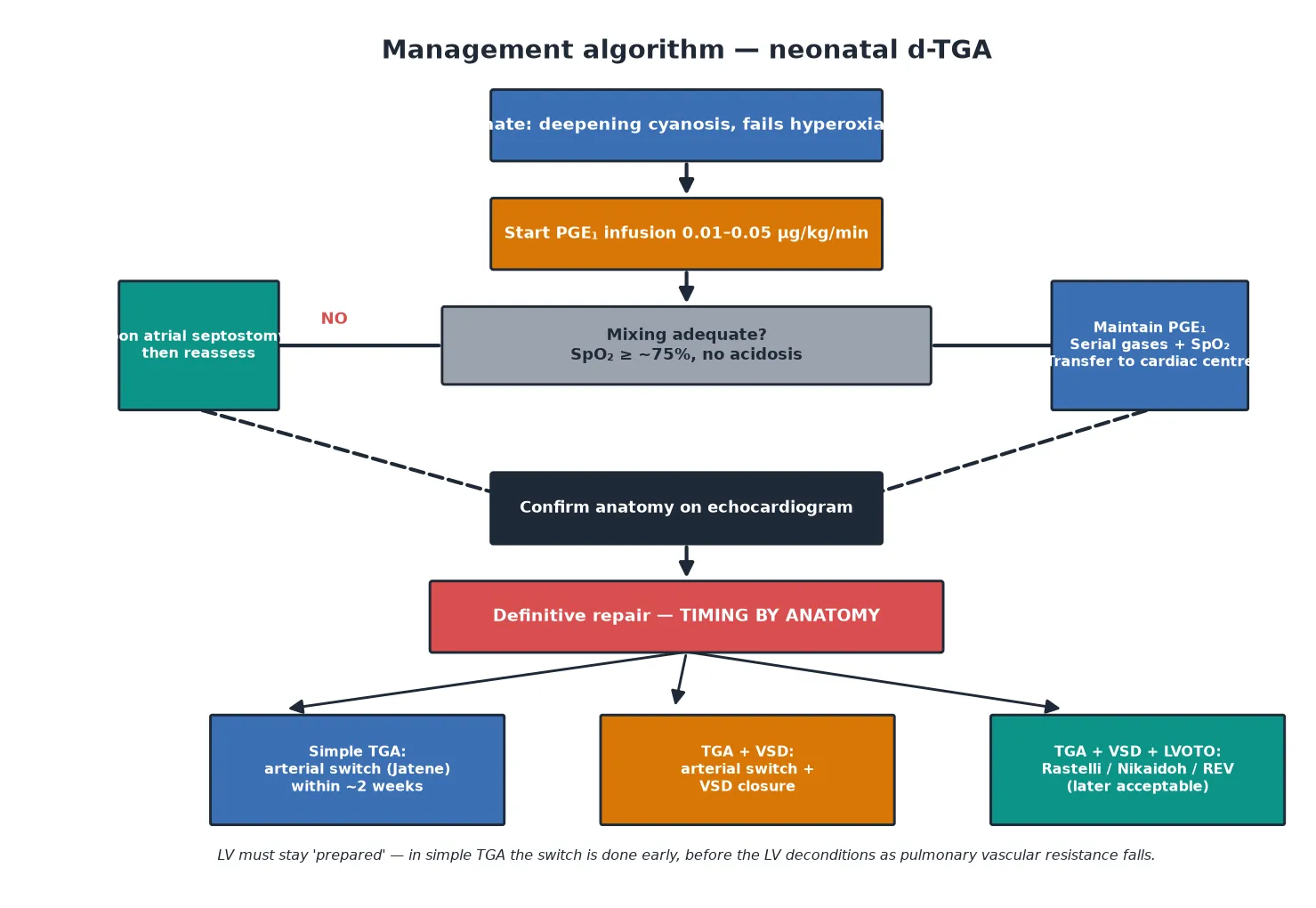
Prostaglandin E1 (alprostadil) is started at a low dose — around 0.01 to 0.05 microgram per kilogram per minute — and titrated to the saturation and acid-base status. It keeps the ductus arteriosus patent and improves mixing. The predictable adverse effects are apnoea, fever, hypotension, and flush, so the clinician should plan for the airway (have intubation equipment ready), treat the fever, and monitor the blood pressure. In an unstable infant a higher dose may be needed but raises the apnoea and hypotension risk, which often necessitates elective intubation and ventilation for transfer. [10]
Prostaglandin E1 (alprostadil)
Dose
0.01–0.05 microgram/kg/min IV continuous infusion; titrate to saturation and acid-base; in extremis may use up to 0.1 microgram/kg/min
When prostaglandin E1 alone does not secure adequate oxygenation, the next step is a balloon atrial septostomy (the Rashkind procedure). A catheter is passed across the foramen ovale or atrial septal defect — usually via the umbilical vein in the neonate — and a balloon is inflated and pulled back to tear the atrial septum, creating a larger atrial communication that improves mixing. It can be performed at the bedside under echocardiographic guidance in the neonatal unit and is a temporising measure, not a repair. A restrictive atrial septum detected antenatally or at presentation is the classic indication. [1] [2]
Management — Definitive & Stepwise
Definitive surgical management of d-TGA is the arterial switch operation, with Rastelli-type procedures reserved for the subgroup with left ventricular outflow tract obstruction. The choice and timing of operation depend entirely on the ventricular septum and the outflow tract, which is why the preoperative echocardiogram and, where needed, cardiac catheterisation matter so much. [4] [5]
Definitive surgical pathway by anatomy
Simple TGA (intact septum): arterial switch (Jatene) within ~2 weeks, before the LV deconditions
TGA with VSD: arterial switch with VSD closure, usually in the first weeks; more time available as LV is prepared
TGA + VSD + LVOTO: Rastelli (LV-to-aorta baffle via VSD, RV-to-PA conduit) or Nikaidoh or REV; later repair acceptable
Taussig-Bing: arterial switch with VSD redirection to the neoaortic valve
Adult after atrial switch (Mustard/Senning): surveillance for arrhythmia, baffle obstruction and systemic RV failure
The arterial switch operation (Jatene), first performed successfully in the 1970s and refined through the 1980s, transects the aorta and pulmonary artery above the valves, swaps them to their correct ventricles, and reimplants the coronary arteries onto the neoaorta. It restores a normal in-series circulation, leaves the left ventricle as the systemic pump, and avoids the long-term atrial-arrhythmia and right-ventricular-failure burden of the atrial-switch repairs it replaced. Long-term follow-up from large cohorts shows excellent survival and functional status into the second and third decades and beyond, with reoperations most often for branch pulmonary artery stenosis, supravalvar stenosis, neo-aortic root dilation or regurgitation, and coronary stenosis. [4] [5] [6]
The Melbourne group's long-term arterial-switch cohort reported low late mortality and a reoperation-free survival that supports the switch as the standard of care, while the Congenital Heart Surgeons' Society d-TGA cohort confirmed durable late survival and acceptable patient-perceived health status across the repaired population. The key technical hazards at surgery are the coronaries — an abnormal course raises the risk of ischaemia and mortality — and the branch pulmonary arteries, which can be stretched by the Lecompte manoeuvre (repositioning the pulmonary artery anterior to the aorta) and later require angioplasty or stenting. [5] [12]
Long-term arterial switch outcomes — Melbourne cohort (Fricke 2022)
Single-centre long-term follow-up of a large arterial-switch cohort over more than two decades
Practice change
The arterial switch delivers durable survival; surveillance focuses on the pulmonary arteries, the neoaortic root and the coronaries
Specific Subtypes & Scenarios
Three scenarios deserve separate attention because they change the surgical calculus and the counselling. The first is d-TGA with a ventricular septal defect, which mixes better and so presents later and with less drama, but which raises the risk of pulmonary over-circulation and early pulmonary vascular disease once the pulmonary vascular resistance falls. The surgeon must also interrogate the arch for a coarctation or interruption and map the coronary course, because both alter the operation. The arterial switch is combined with closure of the VSD, and the timing is a little more flexible because the left ventricle stays prepared. [1] [2]
The second is d-TGA with a ventricular septal defect and left ventricular outflow tract obstruction. Here the pulmonary stenosis restricts pulmonary blood flow, and a simple arterial switch is usually not feasible because the left ventricle cannot deliver adequate output past the obstruction into the neoaortic position. The surgical answer is an anatomic repair that reroutes flow: the Rastelli procedure baffles the left ventricle to the aorta through the VSD and places a right-ventricle-to-pulmonary-artery conduit, the Nikaidoh procedure mobilises the aortic root, and the Révol (REV) procedure repositions the great arteries without a conduit. Each leaves the child with a conduit that will need replacing over time, so lifelong surveillance is built in. [1] [4]
The third, and increasingly common in transition clinics, is the adult who had an atrial-switch (Mustard or Senning) repair in the era before the arterial switch became standard. In these patients the circulation was rerouted at the atrial level — systemic venous return is baffled to the mitral valve and pulmonary venous return to the tricuspid valve — so the morphologic right ventricle remains the systemic pump. These patients carry a heavy late burden of atrial arrhythmia (especially atrial flutter), baffle leaks and obstruction, sinus node dysfunction, and systemic right-ventricular failure, and a new arrhythmia in this group is a cardiology emergency rather than a benign palpitation. Many are candidates for late conversion to an arterial switch or transplantation when the systemic right ventricle fails. [4] [6]
Complications & Pitfalls
The complications of d-TGA fall into the acute, the perioperative, and the long-term. Acute complications belong to the resuscitation: prostaglandin E1 apnoea and hypotension, acidosis and cardiovascular collapse if the duct closes before surgery, and the procedural risks of balloon atrial septostomy (air embolism, vessel injury, arrhythmia, failure to enlarge the septum). The pitfall to avoid at this stage is withholding prostaglandin E1 while waiting for diagnostic certainty, because the reversible side effects of the drug are trivial beside the irreversible cost of a ductal closure. [10] [2]
Perioperative complications centre on the coronary arteries. An abnormal coronary course raises the risk of myocardial ischaemia and early mortality at the arterial switch, and coronary stenosis can present late as exertional chest pain, ventricular arrhythmia, or sudden death in a repaired patient. Branch pulmonary artery stenosis from the Lecompte manoeuvre, supravalvar pulmonary stenosis, neo-aortic root dilation and neo-aortic regurgitation are the common late structural problems that bring patients back to the catheter laboratory or operating theatre. [4] [5]
Acute / resuscitation
- Prostaglandin E1 apnoea — plan the airway
- Ductal closure with collapse if mixing is not secured
- Balloon septostomy: air embolism, vessel injury, arrhythmia
Perioperative / late structural
- Coronary ischaemia from abnormal course or late stenosis
- Branch pulmonary artery stenosis (Lecompte), supravalvar stenosis
- Neo-aortic root dilation and regurgitation
- Atrial-switch legacy: atrial flutter, baffle obstruction, systemic RV failure
Neurodevelopmental
- Higher rates of attention and executive-function difficulty than peers
- Cognitive outcomes mostly in the average range but with a shifted distribution
- Psychiatric morbidity elevated across the lifespan
- warrants structured neurodevelopmental follow-up
The neurodevelopmental and psychiatric outcomes deserve their own recognition. The state-of-the-art review of d-TGA across the lifespan found that, although most operated patients live independently and achieve average cognitive scores, the distribution is shifted toward attention and executive-function difficulties, and psychiatric morbidity — including anxiety, depression and, in the atrial-switch group, psychosis-spectrum symptoms — is elevated. These outcomes are attributable to the combination of preoperative hypoxaemia, the operative period of circulatory arrest or low-flow bypass used in earlier eras, and the lived experience of chronic disease. They justify structured neurodevelopmental surveillance alongside the cardiac follow-up. [11]
Prognosis & Disposition
The prognosis of d-TGA after a successful arterial switch is excellent, and this is one of the great success stories of congenital heart surgery. Survival into adulthood is now the expectation, with large cohorts reporting over ninety per cent late survival and most patients in functional class one. The Congenital Heart Surgeons' Society cohort confirmed durable late survival and acceptable patient-perceived health status, and the Melbourne long-term data showed low late mortality with a predictable reoperation burden concentrated in the pulmonary arteries and the neoaortic root. [5] [12] [6]
Disposition is shaped by the need for lifelong follow-up. Even the well, asymptomatic, repaired patient is followed in a congenital cardiac service, because the late complications — coronary stenosis, branch pulmonary artery stenosis, neo-aortic root problems, and arrhythmia — are silent until they are dangerous. The patient who had an atrial-switch repair needs closer surveillance for atrial arrhythmia and systemic right-ventricular failure, and the patient with a conduit (after a Rastelli or REV) needs the conduit watched for degeneration. Transition to adult congenital heart disease services is planned in adolescence so that no patient is lost to follow-up at the handover. [4] [6]
Special Populations
d-TGA in the developing world is a different disease. Where antenatal detection, prostaglandin E1 availability, neonatal transfer and surgical capacity are limited, presentation is later, resuscitation is harder, and operative outcomes are worse than in high-resource settings. The developing-world cohort study of d-TGA surgery documented higher operative mortality and later presentation, reflecting the infrastructure rather than the biology. The general paediatrician in a resource-limited setting must advocate for early detection, reliable prostaglandin supply, and robust transfer pathways, and must recognise that a neonate with deepening cyanosis is a time-critical referral. [1]
Adolescents and young adults with repaired d-TGA face the twin tasks of transition and ongoing surveillance. The transition is not only a handover of cardiac care but a transfer of knowledge — the patient must understand their anatomy, their operations, their residual risks, and the symptoms that demand urgent review (chest pain, syncope, palpitations). Pregnancy is generally well tolerated in the well-repaired arterial-switch patient but needs a pre-conception cardiac assessment, and the atrial-switch patient with a failing systemic right ventricle is a higher-risk pregnancy that requires specialist input. Exercise is encouraged in the asymptomatic repaired patient, with the caveat that competitive sport and isometric loading may be restricted for those with significant residual lesions. [4] [11]
Evidence, Guidelines & Regional Differences
In Australia and New Zealand, pulse oximetry screening is embedded in newborn examination, and all neonates with suspected duct-dependent congenital heart disease are transferred to one of the paediatric cardiac centres for definitive imaging and surgery. Prostaglandin E1 is commenced at the referring hospital on suspicion, and retrieval services are experienced in the ventilated, prostaglandin-infused neonate. The arterial switch is the standard repair for simple d-TGA, performed in the first two weeks of life. [9] [5]
The guideline base for d-TGA is shared across regions. The AHA/AAP pulse oximetry scientific statement defines screening thresholds; the PulseOx and Swedish screening studies provide the test-accuracy and population-level evidence; the long-term arterial-switch cohorts (Melbourne, Congenital Heart Surgeons' Society) define outcomes; and the lifespan neuropsychiatric review frames the non-cardiac follow-up. There is little genuine regional controversy — the arterial switch is standard everywhere it can be performed — and the differences are those of access and infrastructure rather than of biology or surgical philosophy. [7] [5] [11]
Exam Pearls
One-sentence answer: the approach to the neonate with d-TGA
A neonate with deepening cyanosis, little respiratory distress and a failed hyperoxia test has d-TGA until proven otherwise — start prostaglandin E1 immediately to keep the duct open, confirm the anatomy and coronary pattern on echocardiogram, perform a balloon atrial septostomy if mixing is inadequate, and proceed to an arterial switch within the first two weeks of life for simple disease, with Rastelli-type procedures reserved for d-TGA with ventricular septal defect and left ventricular outflow tract obstruction.
Definition and the parallel circulation
- d-TGA = AV concordance with ventriculoarterial discordance: aorta from RV, PA from LV
- Two parallel loops — survival depends on mixing at the duct, atrial septum or VSD
- Most common cyanotic CHD presenting in the neonate
- Usually isolated; extracardiac anomalies and syndromes uncommon
Presentation and recognition
- 'Comfortably blue' neonate: cyanosis with little respiratory distress
- Fails the hyperoxia test (PaO₂ stays low on 100% oxygen)
- CXR: 'egg on a string' — narrow mediastinum, increased pulmonary markings
- ECG usually normal for age; murmur often absent
- Differential cyanosis when a PDA carries oxygenated blood to the lower body
Resuscitation
- Prostaglandin E1 (alprostadil) 0.01–0.05 µg/kg/min — keep the duct open
- Plan for prostaglandin apnoea: airway and intubation ready
- Balloon atrial septostomy (Rashkind) if mixing inadequate
- Start prostaglandin on suspicion — do not wait for diagnostic certainty
Definitive repair
- Simple TGA: arterial switch (Jatene) within ~2 weeks, before the LV deconditions
- TGA + VSD: arterial switch with VSD closure
- TGA + VSD + LVOTO: Rastelli / Nikaidoh / REV (switch often not feasible)
- Atrial-switch (Mustard/Senning) legacy: atrial arrhythmia, baffle obstruction, systemic RV failure
Long-term
- Excellent survival after arterial switch (over 90% late survival)
- Surveillance: branch PA stenosis, supravalvar stenosis, neo-aortic root, coronaries
- Neurodevelopmental and psychiatric follow-up is part of the plan
- Lifelong congenital cardiac follow-up; structured transition to adult services
Frequently misremembered facts, stated correctly: d-TGA is usually an isolated lesion and is not strongly associated with 22q11.2 deletion (that distinction belongs to tetralogy of Fallot and interrupted arch). The "d" refers to the rightward position of the aortic valve relative to the pulmonary valve, not to dextrocardia. The left ventricle in simple d-TGA is normal at birth but deconditions over weeks as pulmonary vascular resistance falls, which is the reason the switch is done early rather than late. And the atrial-switch repairs (Mustard and Senning), although superseded, were genuine advances in their time — the patients who had them are adults now and their systemic right ventricles are failing, which is the contemporary problem the arterial switch was designed to prevent. [4] [6]
The one diagram that answers every d-TGA question is the parallel circulation: the right ventricle pumps to the aorta, the left ventricle to the pulmonary artery, and the two loops survive only on what mixes between them. Every clinical question maps onto it. Why is the infant 'comfortably blue'? Because the lungs are well perfused by the parallel loop. Why does the saturation crash on day two? Because the duct closes and mixing falls. Why does the left ventricle have to be 'prepared'? Because it has been pumping to the low-resistance pulmonary bed and must take over systemic pressures. Why an arterial switch and not an atrial switch? Because the switch restores the left ventricle as the systemic pump and removes the long-term burden on the systemic right ventricle. Know the parallel circulation, and the whole lesion follows. [2] [1]
References
- [1]Carter E; Rogers LS Transposition of the great arteries: anatomy, physiology and surgical outcomes today. Curr Opin Pediatr, 2025.PMID 40820908
- [2]Martins P; Castela E Transposition of the great arteries. Orphanet J Rare Dis, 2008.PMID 18851735
- [3]Liebman J; Cullum L; Belloc NB Natural history of transposition of the great arteries. Anatomy and birth and death characteristics. Circulation, 1969.PMID 4240356
- [4]Moe TG; Bardo DME Long-term Outcomes of the Arterial Switch Operation for d-Transposition of the Great Arteries. Prog Cardiovasc Dis, 2018.PMID 30227186
- [5]Fricke TA; Buratto E; Weintraub RG; et al Long-term outcomes of the arterial switch operation. J Thorac Cardiovasc Surg, 2022.PMID 33715839
- [6]Williams WG; McCrindle BW; Ashburn DA; et al Outcomes of 829 neonates with complete transposition of the great arteries 12-17 years after repair. Eur J Cardiothorac Surg, 2003.PMID 12853039
- [7]Mahle WT; Newburger JW; Matherne GP; et al Role of pulse oximetry in examining newborns for congenital heart disease: a scientific statement from the AHA and AAP. Circulation, 2009.PMID 19581492
- [8]Ewer AK; Middleton LJ; Furmston AT; et al Pulse oximetry screening for congenital heart defects in newborn infants (PulseOx): a test accuracy study. Lancet, 2011.PMID 21820732
- [9]de-Wahl Granelli A; Wennergren M; Sandberg K; et al Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns. BMJ, 2009.PMID 19131383
- [10]Singh Y; Mikrou P Use of prostaglandins in duct-dependent congenital heart conditions. Arch Dis Child Educ Pract Ed, 2018.PMID 29162633
- [11]Kasmi L; Bonnet D; Montreuil M; et al Neuropsychological and Psychiatric Outcomes in Dextro-Transposition of the Great Arteries across the Lifespan: A State-of-the-Art Review. Front Pediatr, 2017.PMID 28393063
- [12]Devlin PJ; Jegatheeswaran A; Williams WG; et al Late Survival and Patient-Perceived Health Status of the Congenital Heart Surgeons' Society dextro-Transposition of the Great Arteries Cohort. Ann Thorac Surg, 2019.PMID 31348901