Paeds · cardiology
Truncus arteriosus and single-ventricle physiology
Also known as Truncus arteriosus · Common arterial trunk · Persistent truncus arteriosus · Single-ventricle physiology · Functional single ventricle · Fontan circulation · Univentricular heart
Fellowship guide to two cyanotic congenital lesions that share the single idea of mixing red and blue blood. Truncus arteriosus is one great artery and one truncal valve carrying fully mixed blood to the body and lungs, with an obligatory ventricular septal defect, presenting first as neonatal cyanosis and then as high-output heart failure as pulmonary vascular resistance falls. Single-ventricle physiology is any heart with one functional pumping chamber, palliated through the staged Fontan pathway — Norwood, Glenn, Fontan — that routes venous blood passively to the lungs in series. Covers the Collett–Edwards and Van Praagh classifications, the near-obligatory 22q11.2 deletion, complete neonatal repair versus staged palliation, interstage mortality and home monitoring, and the lifelong Fontan burden of arrhythmia, protein-losing enteropathy and Fontan liver disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The thread running through this topic is mixing, and what you do about it. [2] [8] When red and blue blood cannot be kept apart, the body gets blue blood and the lungs get more blood than they can handle. Truncus arteriosus solves this with one operation that separates the circulations. Single-ventricle physiology solves it with three operations that route venous blood to the lungs without a second pump. This page covers recognition, the bedside and echocardiographic anatomy, the Collett–Edwards and Van Praagh classifications, the prostaglandin-E1-first rule, the complete neonatal repair of truncus, the staged Fontan palliation, the interstage mortality that home monitoring targets, and the lifelong burden both groups carry. It links to the ductal-dependent congenital heart disease leaf for the broader differential and to the hypoplastic left heart syndrome leaf for the detailed Norwood content.
Overview & Definition
Picture a normal heart first: two ventricles sit side by side, the right pumps blue blood to the lungs and the left pumps red blood to the body, and two separate great vessels leave through two separate valves. Truncus arteriosus collapses that design. One great artery — the truncus — leaves the heart through a single truncal valve and then branches to give off the coronaries, the aorta and the pulmonary arteries. Because a ventricular septal defect sits directly under the truncal valve, blood from both ventricles pours into the same trunk and mixes completely. The body and the lungs therefore receive the same mixed, partially blue blood. [1] [2]
Two consequences follow directly from that anatomy, and they explain everything you will see at the bedside. First, the baby is cyanosed, because the body is being fed mixed blood. Second — and this is the part candidates miss — the lungs are being fed by the same trunk with no resistance between the aorta and the pulmonary bed. After birth the pulmonary vascular resistance falls, so more and more of the mixed blood takes the easy path into the lungs. The lungs flood, the heart works harder and harder, and the baby slides into high-output heart failure over the first weeks of life. Cyanosis comes first; heart failure follows. [3]
Single-ventricle physiology is the other half of this topic, and it is a strategy rather than a single defect. It describes any heart in which only one ventricle is usable, because the other is hypoplastic, atretic or has no inlet or outlet. Hypoplastic left heart syndrome, tricuspid atresia, pulmonary atresia with intact septum, double-inlet left ventricle and unbalanced atrioventricular septal defect all produce it. Because there is no second pump to push blood to the lungs, you cannot simply close a hole. Instead, surgeons keep the one good ventricle as the systemic pump and route the venous return passively and directly to the lungs, in stages, until the circulations run in series. That staged pathway is called the Fontan strategy. [8] [10]
The reason these two lesions sit on one page is that both force you to think about the balance between lung blood flow and body blood flow. In truncus the balance is dangerously tipped toward the lungs. In single-ventricle physiology the entire surgical plan is about restoring a workable balance. Master that idea and the rest follows. [2] [10]
Classification
Candidates sort truncus arteriosus along one axis — where the pulmonary arteries come from — and single-ventricle lesions along another — which stage of palliation the child has reached. The figure below splits truncus by the Collett and Edwards pattern and single-ventricle physiology by the staged Fontan pathway. [2] [10]
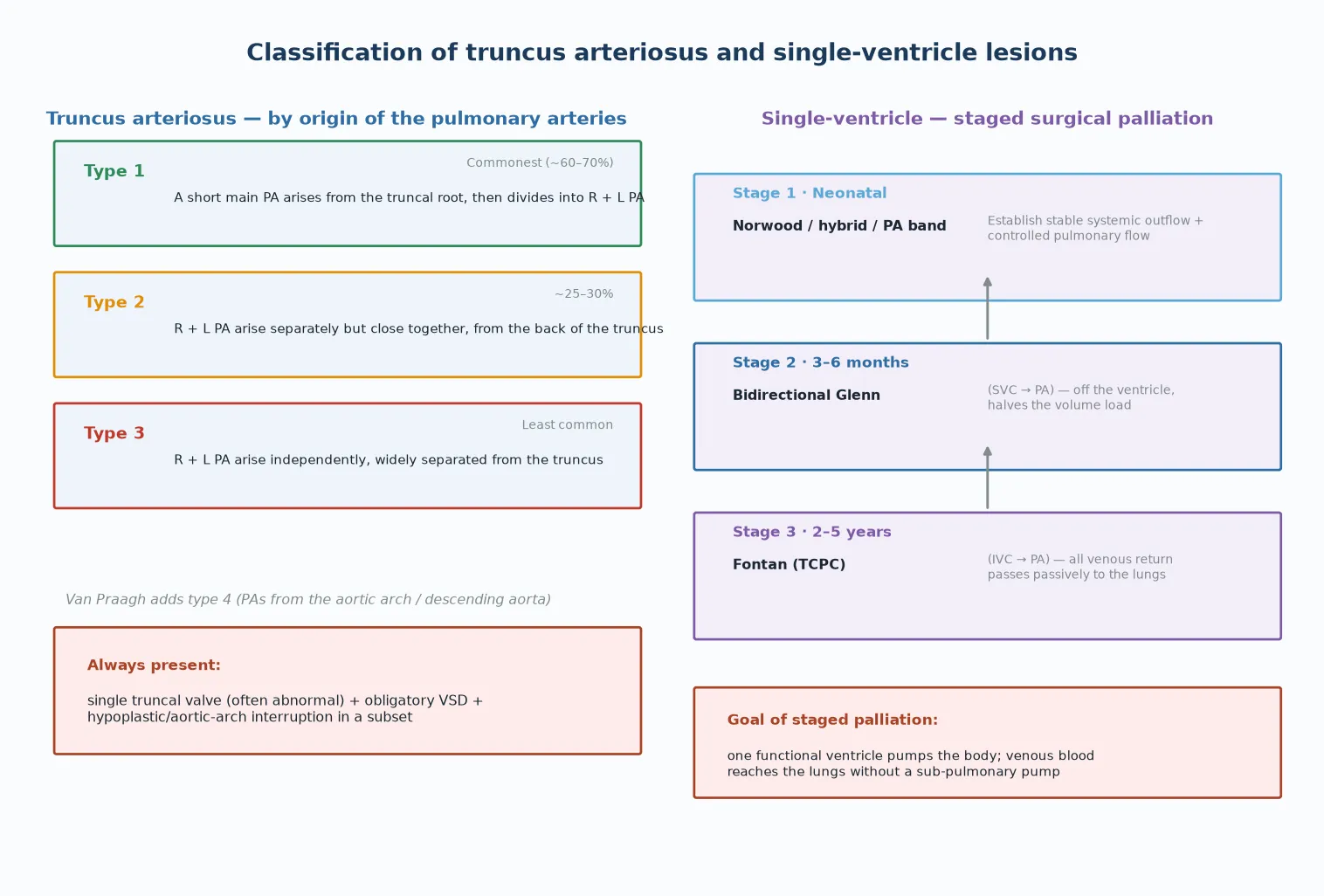
Truncus type I
- A short main PA arises from the truncal root, then divides into R + L PA
- Commonest pattern (~60–70%)
- Easiest surgical separation of the PAs from the trunk
Truncus type II
- R + L PA arise separately but close together, off the back of the trunk
- ~25–30% of cases
- PA origins still separable at repair
Truncus type III
- R + L PA arise independently and widely separated
- Least common; harder surgical anatomy
- Branch PA stenosis a later problem
Van Praagh extended the scheme with a type IV, in which the pulmonary arteries arise from the aortic arch or the descending aorta, and the simplified modern categorisation used in surgical databases folds these into a practical description of the pulmonary artery origin and the aortic arch. [2] Two features are constant across every type and you must name them in any viva: a single truncal valve that is often abnormal (quadricuspid or with regurgitation), and a ventricular septal defect directly beneath the truncal root. A right aortic arch is present in a sizeable minority and is a useful clue when you see the chest radiograph.
For single-ventricle physiology the classification that matters clinically is the surgical stage, because it tells you the child's current circulation, their risks, and what deterioration means. Stage one is the neonatal operation (Norwood, hybrid, or a pulmonary artery band) that buys a stable systemic outflow. Stage two is the bidirectional Glenn, performed around four to six months, which connects the superior vena cava to the pulmonary arteries and halves the volume load on the single ventricle. Stage three is the Fontan, performed between two and five years, which completes the passive venous-to-pulmonary circuit. A child "post-Glenn, pre-Fontan" behaves very differently from a child "post-Fontan", and the stage drives every management decision. [10]
Epidemiology & Risk Factors
Truncus arteriosus is uncommon but not rare: it accounts for roughly one to two percent of all congenital heart defects and occurs in about five to ten infants per hundred thousand live births. It is one of the conotruncal lesions, sitting alongside tetralogy of Fallot, transposition and interrupted aortic arch. [1] [3]
The single genetic association you must name is 22q11.2 deletion syndrome (DiGeorge syndrome). A large minority of infants with truncus arteriosus carry a 22q11.2 deletion, and truncus is one of the classic cardiac lesions of the syndrome, alongside interrupted aortic arch and tetralogy of Fallot. The implication is operational: every infant with truncus arteriosus (or interrupted aortic arch) should have chromosomal microarray or 22q11.2 testing, because the result changes calcium management, immunology, airway and palate assessment, feeding and long-term developmental care. [5] [6]
Other associations that change the surgical plan and the counselling include interrupted aortic arch, a right aortic arch, an aberrant subclavian artery and additional ventricular septal defects. A family history of a left-sided obstructive or conotruncal lesion earns recurrence-risk counselling and dedicated fetal echocardiography in later pregnancies. [2] Single-ventricle physiology is spread across several anatomies, so its epidemiology is the sum of those conditions; what matters for the general paediatrician is that staged palliation now carries most of these children into adulthood, and their numbers are growing in transition clinics.
Pathophysiology
To understand truncus arteriosus, follow the blood. Both ventricles eject into a single trunk, so the red blood from the lungs and the blue blood returning from the body meet and mix completely before any of it leaves the heart. From that mixed pool, one portion goes to the body and one portion to the lungs. The body therefore receives blood that is only partially oxygenated — hence the cyanosis. [2] [3]
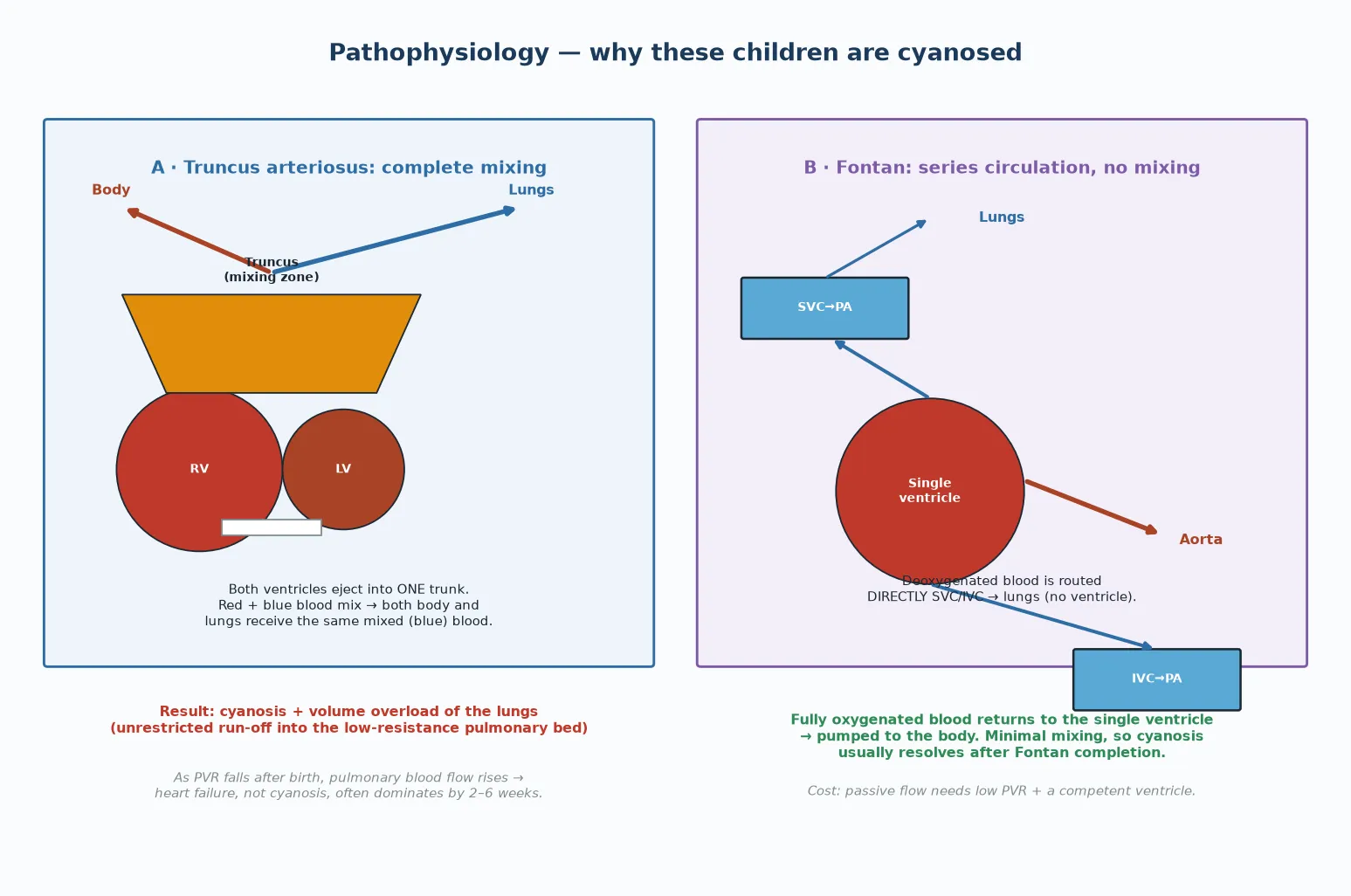
The reason truncus deteriorates after the neonatal period is a falling number, not a random event. Pulmonary vascular resistance is high at birth, so the lungs and the body share the mixed blood roughly equally. Over the first weeks of life the resistance in the pulmonary bed drops, exactly as it should in a normal baby. But in truncus there is no valve or narrowing protecting the pulmonary circuit from the systemic pressure, so blood increasingly takes the path of least resistance into the lungs. The lungs flood, the left heart fills with returning blood, and the heart pumps ever harder just to maintain systemic output. This is the pulmonary run-off that turns a stable cyanotic baby into a failing one. [3]
The same run-off explains the bounding pulses and the wide pulse pressure you feel at the bedside. In diastole, blood runs off from the trunk into the low-resistance pulmonary bed, so the diastolic pressure drops low and the pulse pressure widens. A cyanotic neonate with bounding pulses should make you think of truncus, or of a large patent ductus arteriosus, before you think of pure lung disease. [3]
Single-ventricle physiology is governed by a different problem: there is no second pump. In a normal heart the right ventricle pushes blue blood to the lungs and the left pushes red blood to the body, and the two never mix after birth. When only one ventricle works, both blue and red blood return to it and mix, so the body is fed partly-blue blood and the child is cyanosed. You cannot fix this by closing a hole, because the underdeveloped ventricle can never become a competent pump. [8] [10]
The Fontan strategy works around the missing pump by changing the plumbing. Instead of pushing venous blood to the lungs with a ventricle, surgeons connect the great veins — first the superior vena cava in the Glenn, then the inferior vena cava in the Fontan — directly to the pulmonary arteries. Venous blood now flows passively to the lungs, is oxygenated, and returns to the single ventricle, which pumps it to the body. The two circulations are in series, there is no mixing, and the cyanosis usually resolves. The catch is that passive flow has no pump behind it: it works only while the pulmonary vascular resistance is low, the pulmonary arteries are unobstructed, and the single ventricle is compliant and competent. If any of those fail, the Fontan fails. [10]
Clinical Presentation
A truncus baby usually presents in one of two ways, and both are classic exam material. The dramatic presentation is a neonate noticed to be dusky in the first days of life. The cyanosis is often mild, because mixing is shared between body and lungs, so the oxygen saturation may sit in the high eighties rather than being profoundly low. The baby then becomes increasingly tachypnoeic, sweaty and distressed on feeds over the next two to six weeks, and starts to fail to thrive. [3]
The other presentation is the antenatally detected lesion, picked up on fetal echocardiography at the anomaly scan and managed from birth in a cardiac centre. These babies avoid the late-presenting heart-failure scenario but still need the same neonatal repair. The increasing pick-up rate on antenatal screening is one reason late presentation is becoming less common. [1]
On examination of a truncus neonate, look for four things and you will narrow the diagnosis at the bedside. The pulses are bounding with a wide pulse pressure. There is a loud systolic ejection murmur at the left sternal edge from flow across the truncal valve and the ventricular septal defect. The second heart sound is single, because there is only one semilunar valve. And there may be a systolic click and a diastolic murmur if the truncal valve is regurgitant. A right aortic arch may be suggested on the chest radiograph. [3] [4]
Single-ventricle physiology presents according to the underlying anatomy, and the stage of palliation dominates the picture. A neonate with tricuspid atresia or pulmonary atresia is cyanosed from birth because blood cannot reach the lungs without the duct. A neonate with hypoplastic left heart or an interrupted arch is shocked at ductal closure, with weak pulses and acidosis. After stage one palliation, the child enters the interstage period, and any deterioration there — fever, poor feeding, tachypnoea, a colour change, or a home saturation that has dropped from the eighties into the seventies — is circulatory failure until proven otherwise. After the Fontan, the child is usually pink but carries the burden of a passive circulation, presenting years later with exercise intolerance, palpitations, leg swelling or chronic diarrhoea. [10] [12]
Differential Diagnosis
When a neonate is cyanotic, your first job is to separate cardiac from respiratory and other causes, and within the cardiac causes to separate those with increased pulmonary markings from those with reduced. Truncus arteriosus belongs in the group with increased pulmonary markings: the lungs are over-circulated. The main companions there are transposition of the great arteries, total anomalous pulmonary venous connection, hypoplastic left heart, and large left-to-right shunts that decompensate. The chest radiograph and the hyperoxia test start the sorting. [1]
The wide pulse pressure of truncus has its own short differential. Patent ductus arteriosus, a large arteriovenous malformation and aortic regurgitation can all produce bounding pulses and a run-off physiology. The distinguishing feature of truncus is the single second heart sound and the cyanosis with increased markings. [3]
Two look-alike lesions deserve a named distinction because the surgery differs. An aortopulmonary window is a hole between the aorta and the pulmonary artery, but there are still two separate semilunar valves and two separate outflow tracts — the mixing is at great-vessel level, not ventricular. Hemitruncus (one pulmonary artery arising from the ascending aorta) is a related anomaly in which only one lung is over-circulated. Both need cardiology, but neither is a true truncus, and the viva rewards the candidate who states the difference precisely. [2]
For single-ventricle physiology, the differential is the cause of cyanosis or shock in the neonate, and it resolves into the ductal-dependent congenital heart disease family. The unifying rule: a neonate who collapses after a period of wellbeing, with shock, acidosis and weak or uneven pulses, has a ductal-dependent lesion until proven otherwise and gets prostaglandin E1 before the echo. [10]
Clinical & Bedside Assessment
Examine the cyanotic neonate systematically and you will generate the cardiac shortlist before the echo. Look first at colour and perfusion: a grey, mottled child is in low output. Feel the brachial and femoral pulses together and in all four limbs: uniformly weak pulses point to a ductal-dependent systemic obstruction such as hypoplastic left heart, while bounding pulses with a wide pulse pressure point to truncus or a run-off lesion. Measure blood pressure in all four limbs: a gradient between the arms and the legs suggests coarctation or interrupted arch. [3] [10]
Listen carefully. A single second heart sound means there is only one semilunar valve — think truncus or pulmonary atresia. A systolic ejection murmur at the left sternal edge with a systolic click points to truncal valve flow. A diastolic murmur raises truncal valve regurgitation. Record the oxygen saturation in the right hand (pre-ductal) and a foot (post-ductal): a large gap suggests differential cyanosis. Then perform the hyperoxia test, giving one hundred percent oxygen and rechecking: if the saturation cannot be raised and the partial pressure of oxygen stays low, the cause is cyanotic congenital heart disease rather than lung disease. [1]
The synthesis you are aiming for is a one-line problem representation: "a three-week-old with mild cyanosis, bounding pulses, a single second sound and increasing tachypnoea on feeds — likely truncus arteriosus with pulmonary over-circulation." That sentence drives the next steps: prostaglandin E1 only if a duct-dependent component is plausible, an urgent echocardiogram, four-limb blood pressures, a chest radiograph and transfer to a cardiac centre. [3]
For the interstage single-ventricle infant, the assessment is faster and the threshold lower. Any deviation from the child's usual baseline — a feed they would not take, a colour the parents find wrong, a saturation below their agreed threshold — is treated as circulatory compromise. The parents' report is the most sensitive sign, because they know the child's baseline. [12]
Investigations
Echocardiography is the definitive investigation for both truncus and single-ventricle lesions, and it should be requested and performed by paediatric cardiology. In truncus it shows the single great vessel overriding the ventricular septal defect, the origin and branching pattern of the pulmonary arteries (which fixes the Collett–Edwards type), the morphology and regurgitation of the truncal valve, the side of the aortic arch, any interruption of the arch, and the patency of the ductus. [1] [2]
Before the echo arrives, order the bedside tests that direct the resuscitation and that you may need for the viva. Four-limb blood pressure, pre- and post-ductal saturations and a hyperoxia test define the physiology. A chest radiograph shows pulmonary plethora, cardiomegaly and sometimes a right aortic arch. An electrocardiogram is usually non-specific but rules in rhythm disturbances. Blood gas and lactate track the perfusion. [3]
Two investigations are easy to forget and change the long-term plan. The first is chromosomal microarray or 22q11.2 testing, which is indicated for every infant with truncus arteriosus or interrupted aortic arch. A positive result prompts calcium monitoring, immunology assessment, airway and palate evaluation, feeding support and developmental surveillance. The second, for single-ventricle patients, is cardiac catheterisation before the Glenn and Fontan, which measures the pulmonary vascular resistance and maps the pulmonary artery anatomy that the next operation depends on. [5] [6]
The principle for investigation timing is that the echo and the transfer to a cardiac centre happen together, not in sequence. If a duct-dependent lesion is plausible, prostaglandin E1 is running before, during and after the echo, because the diagnosis does not change the need for an open duct in a collapsing neonate. [10]
Management — Resuscitation
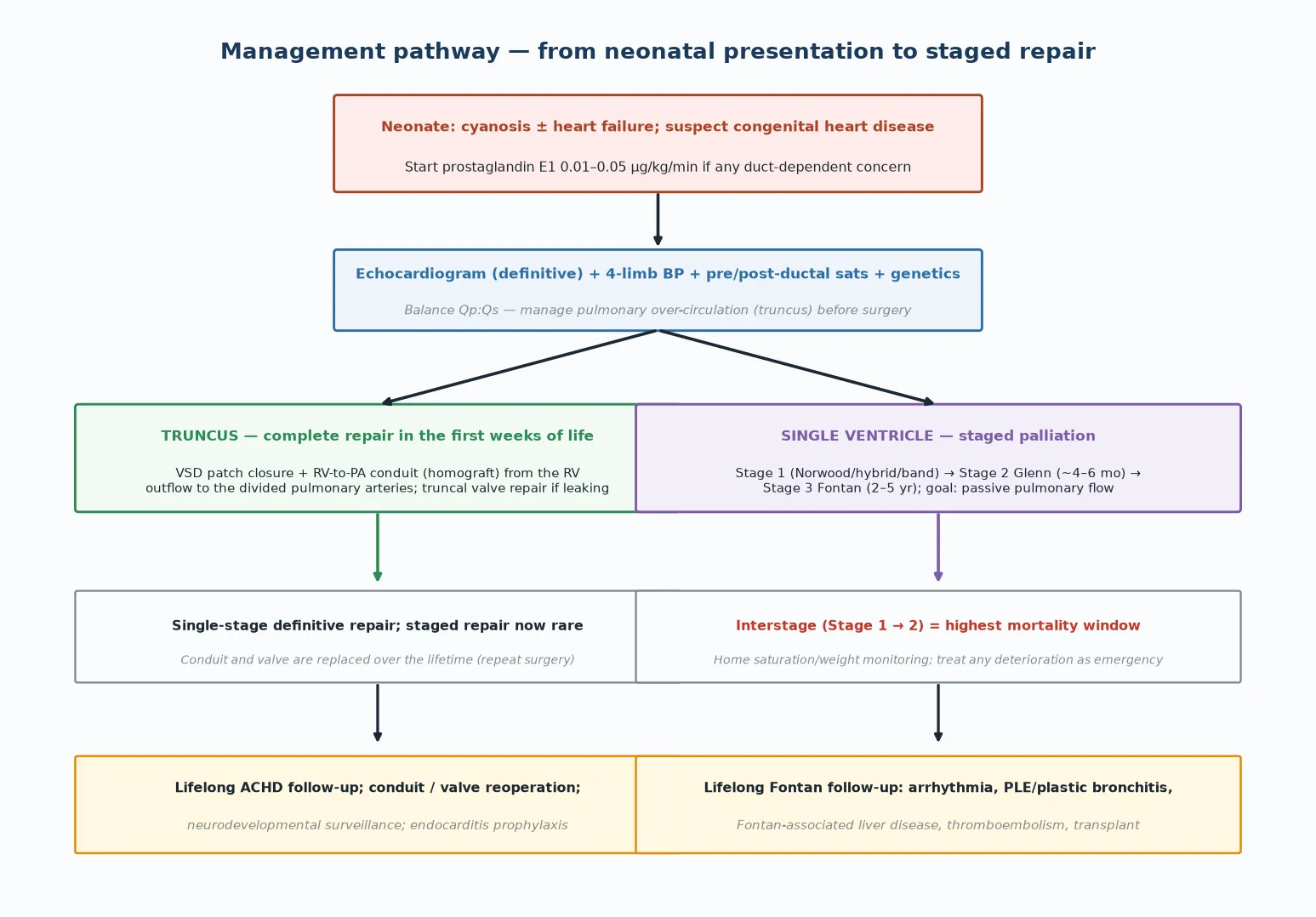
The non-negotiable resuscitation rule for the neonate is the prostaglandin-E1-first principle. If a ductal-dependent lesion is on the differential — any cyanotic or collapsing neonate with weak or uneven pulses, metabolic acidosis or a single second sound — start prostaglandin E1 at 0.01 to 0.05 micrograms per kilogram per minute before the echocardiogram. The reasoning is simple: the cost of an unnecessary dose is apnoea and hypotension, both manageable, while the cost of delay in a true ductal lesion is death. [1] [10]
The caveats are the side effects. Prostaglandin E1 causes apnoea, so an infant being retrieved on it should travel intubated, or with airway expertise, because an unplanned apnoea in transit is a preventable death. It causes hypotension and fever, which need fluid and antipyretic support but rarely force you to stop. If the duct is genuinely needed, you manage the side effects rather than abandoning the drug. [10]
For the truncus baby who is not collapsing but is over-circulating, the resuscitation problem is balancing the pulmonary and systemic flows. Because the run-off into the lungs rises as pulmonary vascular resistance falls, you may deliberately manipulate the resistance to buy time before surgery. Lowering the inspired oxygen, adding nitrogen or a little carbon dioxide, and using vasoactive drugs to support systemic pressure can shift the balance toward the body. The surgery is the definitive fix, so these are holding measures. [3]
The general paediatrician's role in resuscitation is to recognise, start prostaglandin E1 if indicated, secure the airway for retrieval, establish intravenous access, take the baseline bloods and arrange urgent transfer to a paediatric cardiac centre. Do not delay transfer for imaging that can be done there. [10]
Management — Definitive & Stepwise
Definitive management divides cleanly along the two halves of this topic. Truncus arteriosus is repaired in one operation in early infancy. Single-ventricle physiology is palliated in three stages over the first years of life. [1] [10]
For truncus, the operation is complete repair and it is now done in the neonatal period or early infancy. [1] [3] The surgeon closes the ventricular septal defect so the left ventricle ejects into the truncal root, which now becomes the aorta. The pulmonary arteries are separated from the trunk, and right-ventricle-to-pulmonary-artery continuity is restored with a valved homograft conduit. If the truncal valve is regurgitant it is repaired or replaced at the same operation, because an incompetent truncal valve is a major risk factor for early and late mortality. [4] [7]
Staged repair of truncus (banding the pulmonary arteries first, then completing the repair later) is now rare, used only for unstable neonates or unusual anatomy, because delaying repair risks irreversible pulmonary vascular disease. The landmark outcomes series document the steady improvement in neonatal repair mortality to below ten percent in contemporary centres. [3] [7]
For single-ventricle physiology, the staged Fontan pathway is the definitive plan, and you should be able to name each stage and what it achieves. Stage one, in the neonatal period, establishes a stable systemic outflow and a controlled source of pulmonary blood flow. In the Norwood operation the surgeon reconstructs the hypoplastic arch, connects the pulmonary trunk to the reconstructed aorta so the single ventricle pumps the body, and provides lung flow through either a modified Blalock–Taussig shunt or a right-ventricle-to-pulmonary-artery conduit (the Sano modification). The hybrid procedure — a ductal stent plus pulmonary artery bands — is an alternative for high-risk infants or a bridge. [10]
Stage two is the bidirectional Glenn, performed around four to six months, which connects the superior vena cava directly to the pulmonary arteries. This halves the volume load on the single ventricle and removes the fragile shunt, so the child is more stable. Stage three is the Fontan, performed between two and five years, which completes the total cavopulmonary connection by routing the inferior vena caval blood to the pulmonary arteries. After the Fontan, all venous return flows passively to the lungs and the circulations are in series. [8] [9] [10]
Two further definitive-care decisions deserve a mention. A Fontan fenestration — a small surgical communication between the Fontan circuit and the atrium — is used in higher-risk patients to decompress the circuit and maintain cardiac output at the cost of a little right-to-left shunting and mild cyanosis. And cardiac transplantation is the rescue therapy for a failing Fontan or for the small group in whom staged palliation cannot proceed. [10]
Specific Subtypes & Scenarios
Truncus arteriosus with an interrupted aortic arch is a particularly demanding subtype and a strong pointer to 22q11.2 deletion. The arch must be reconstructed at the same operation as the truncus repair, which raises the surgical complexity and the perioperative risk. Recognising the interruption on the echo and screening for 22q11.2 changes the whole perioperative plan, including calcium and immunology management. [5] [6]
Truncal valve regurgitation is the subtype that most affects operative risk and long-term outcome. A regurgitant truncal valve at presentation predicts higher early mortality and drives later reoperation. Surgeons will repair or replace it at the index operation, and the fate of the truncal valve is a long-term issue for the survivor. [4]
The 22q11.2 deletion (DiGeorge) infant with truncus is a whole-child scenario. Beyond the cardiac repair, these children may have hypocalcaemia needing monitoring and supplementation, immune deficiency affecting blood-product choice, palatal and airway anomalies affecting feeding and intubation, and a heavier neurodevelopmental burden. Coordinated care across cardiology, immunology, endocrinology, speech and language and developmental paediatrics is the standard. [5]
Heterotaxy with single-ventricle physiology is the subtype where outcomes are hardest. Systemic and pulmonary venous anomalies, atrial isomerism, atrioventricular valve regurgitation and a high arrhythmia burden complicate every stage, and the interstage and Fontan outcomes are worse than in non-heterotaxy single-ventricle patients. [10]
The hybrid stage-one procedure is a scenario in its own right. By stenting the duct and banding the pulmonary arteries, the hybrid avoids cardiopulmonary bypass in a fragile neonate and is used in some centres as the primary stage or as a bridge for high-risk infants. The candidate should know that it exists and that it changes the anatomy for the subsequent comprehensive stage-two operation. [10]
The failing Fontan is the long-term scenario the general paediatrician and the transition physician must recognise. New exercise intolerance, palpitations, leg swelling, ascites, chronic diarrhoea or a cough productive of bronchial casts signals protein-losing enteropathy, plastic bronchitis, atrial arrhythmia or Fontan-associated liver disease. These can decompensate quickly and need urgent adult congenital heart disease review, because the rescue options (catheter fenestration, lymphatic intervention, medical therapy, transplant) are time-sensitive. [10]
Complications & Pitfalls
Untreated truncus arteriosus is lethal, and the mechanism is twofold. In the short term the baby dies of intractable heart failure from pulmonary over-circulation. In the longer term, if repair is delayed, the unprotected pulmonary bed develops irreversible high-resistance pulmonary vascular disease — Eisenmenger physiology — after which the child is inoperable. This is the reason complete repair is done early, in the neonatal period, rather than waiting. [3]
After truncus repair, the long-term complications are mechanical and reoperation-driven. The right-ventricle-to-pulmonary-artery conduit does not grow with the child and degenerates, so it must be replaced, often several times across childhood and adolescence. The truncal or neoaortic valve may develop stenosis or regurgitation and need reoperation. Branch pulmonary artery stenosis, arrhythmia and endocarditis round out the burden. The truncus survivor is a lifelong cardiac patient. [4] [7]
The single-ventricle and Fontan patient carries the heaviest long-term burden in congenital cardiology. The four pillars of Fontan morbidity are atrial arrhythmia and sinus node dysfunction, protein-losing enteropathy, plastic bronchitis and Fontan-associated liver disease, with thromboembolism and progressive cyanosis from fenestration or venous anomalies adding to the load. Each can appear years after an apparently successful Fontan and each can precipitate Fontan failure and the need for transplant assessment. [10]
The highest-mortality window in the whole pathway is the interstage period between stage one and stage two — between the Norwood and the Glenn. The circulation is fragile, the shunt is the only source of lung flow, and any insult (a febrile illness, a feed refusal, a pulmonary hypertensive spike) can collapse it. Interstage home-monitoring programmes — daily weight and saturation checks with a low threshold to contact the team — reduce this mortality and are the standard of care. [12]
The common pitfall at first presentation is attributing truncus cyanosis to lung disease and delaying cardiology referral. The bounding pulses and the single second sound should redirect you within seconds of laying hands on the child. The complementary pitfall is over-oxygenating a single-ventricle neonate: high inspired oxygen drops pulmonary vascular resistance and steals systemic output into the lungs, so use oxygen deliberately, not reflexively. [3] [10]
Prognosis & Disposition
The prognosis of truncus arteriosus has transformed over a generation. Neonatal complete repair now carries operative survival above ninety percent in contemporary series, and most survivors reach adulthood. The price of that success is a lifetime of follow-up: conduit and valve reoperations, arrhythmia surveillance, endocarditis prophylaxis, exercise guidance and transition to adult congenital heart disease services. The child is cured of the neonatal lesion but never leaves cardiac care. [1] [7]
For single-ventricle physiology, survival to and beyond the Fontan has also improved markedly, but the attrition continues across the decades. The contemporary Fontan cohort reaches adulthood in good numbers, yet a meaningful fraction develops late Fontan failure, arrhythmia, liver disease or the protein-losing complications described above. The general paediatrician should expect these patients in transition clinics and should know that a previously well Fontan patient who develops new symptoms is a cardiac emergency. [9] [10]
The neurodevelopmental outcome of both groups is a fellowship-level topic in its own right. Children with single-ventricle physiology score lower than peers on measures of cognition, executive function, attention and social skills, and a substantial minority need educational support. Syndromic children — particularly those with 22q11.2 deletion or heterotaxy — carry a heavier burden. Routine neurodevelopmental surveillance, early intervention and school support are part of standard care, not optional extras. [11]
Disposition is the same for both groups: urgent transfer to a paediatric cardiac centre at presentation, lifelong follow-up in a congenital cardiac service, endocarditis prophylaxis before procedures, and a planned transition to adult congenital heart disease services in adolescence. The general paediatrician coordinates with the cardiac team, the school, the family and the transition clinic, and holds the long view. [10] [11]
Special Populations
The 22q11.2 deletion (DiGeorge) infant is the special population most tightly bound to this topic. Across truncus, interrupted arch and other conotruncal lesions, the deletion changes the perioperative and lifelong plan. Coordinate calcium and vitamin D, choose irradiated cytomegalovirus-safe blood products, assess the palate and airway, support feeding, and plan developmental surveillance. The deletion also brings behavioural and psychiatric risks in adolescence that the transition team must own. [5] [6]
The Indigenous, remote and rural child faces a particular burden in these lesions. Antenatal detection may be delayed, the distance to a cardiac centre is long, and retrieval can take hours at the exact moment the duct is closing. Families are separated from their community for weeks of neonatal surgery. Coordinated retrieval, culturally safe care, accommodation near the cardiac centre and clear follow-up pathways that reach back to the community are part of good practice across Australia and Aotearoa New Zealand. [10]
The child with disability or neurodevelopmental impairment is over-represented in both truncus and single-ventricle cohorts. The impairment shapes the goals-of-care discussion before high-risk surgery, the school plan, and the support the family needs through a long and repeated operative pathway. A trauma-informed, neurodiversity-aware approach to repeated procedures and admissions reduces harm. [11]
The adolescent and young adult in transition needs explicit planning. Pregnancy in a Fontan patient carries significant risk and needs pre-conception cardiac counselling and contraceptive advice. Exercise, occupation and driving are constrained by the circulation. Structured transition to adult congenital heart disease services — with a written summary, a named adult cardiologist, and education about red flags — reduces the loss-to-follow-up that kills young adults with congenital heart disease. [10]
The socioeconomically disadvantaged family carrying an interstage infant needs tangible support to make home monitoring work: the equipment, the education, the contact number, and the practical help with transport and time off work. An interstage programme only reduces mortality if the family can actually use it. [12]
Evidence, Guidelines & Regional Differences
The evidence base for truncus repair is built on large surgical series and registry studies. Thompson and colleagues documented the steady improvement in neonatal repair outcomes over the 1990s, establishing early complete repair as the standard. Russell and colleagues proposed the simplified modern categorisation of the common arterial trunk and reported the Society of Thoracic Surgeons outcomes, including the strong effect of truncal valve surgery on mortality. Derridj and colleagues confirmed the impact of surgical technique on contemporary outcomes. [2] [3] [4] [7] The 22q11.2 deletion and congenital heart disease association is anchored by Goldmuntz's review and by O'Byrne's perioperative analysis. [5] [6]
The Fontan literature is anchored by Fontan and Baudet's original 1971 report, by the Pediatric Heart Network contemporary Fontan outcomes study, and by the American Heart Association scientific statement on the evaluation and management of the child and adult with a Fontan circulation, which is the practical reference for lifelong care. The Sananes neurodevelopmental follow-up quantifies the long-term cognitive burden of single-ventricle physiology. [8] [9] [10] [11]
Regional differences are mainly operational. The timing of complete truncus repair is now early everywhere, but the choice of Fontan technique (extracardiac conduit versus lateral tunnel, fenestration versus no fenestration), the organisation of interstage home monitoring, and the structure of transition to adult services vary across centres and countries. The candidate should present the shared principle — staged palliation, passive pulmonary flow, lifelong follow-up — and acknowledge local variation in technique. [10] [12]
Exam Pearls
In a written question, truncus is the cyanotic neonate with increased pulmonary markings, a wide pulse pressure, bounding pulses and a single second heart sound, moving into heart failure by two to six weeks. The mechanism question is always the falling pulmonary vascular resistance and uncontrolled run-off. The genetic question is 22q11.2 deletion. The surgical answer is neonatal complete repair: ventricular septal defect closure plus a right-ventricle-to-pulmonary-artery conduit, with truncal valve repair if it leaks. [3] [5]
In the single-ventricle question, the answer is the staged Fontan pathway and its complications. Name the three stages and what each achieves. Know that the interstage period is the highest-mortality window and that home monitoring is the intervention. Know the four pillars of Fontan morbidity — arrhythmia, protein-losing enteropathy, plastic bronchitis, Fontan liver disease — and that a failing Fontan needs urgent adult congenital review. [10] [12]
In a short case, examine the hands (bounding pulses, wide pulse pressure), the precordium and the heart sounds (single second sound, truncal murmur). In a long case on a Fontan survivor, lead with the complications and the transition plan. In a counselling or communication station, the family of a truncus baby needs to hear the genetic testing, the single-operation plan, the reoperation burden and the lifelong follow-up; the family of a single-ventricle baby needs to hear the three stages, the interstage monitoring, and the neurodevelopmental surveillance. [1] [10]
The two sentences that earn marks in any format: truncus is one trunk, one valve and a ventricular septal defect, repaired neonatally; and single-ventricle physiology is one ventricle palliated through Norwood, Glenn and Fontan, with passive pulmonary flow and a lifelong burden. Everything else is detail on those two skeletons. [2] [10]
References
- [1]Naimo PS; Konstantinov IE Surgery for Truncus Arteriosus: Contemporary Practice. Ann Thorac Surg, 2021.PMID 32828754
- [2]Russell HM; Jacobs ML; Anderson RH; et al A simplified categorization for common arterial trunk. J Thorac Cardiovasc Surg, 2011.PMID 20965518
- [3]Thompson LD; McElhinney DB; Reddy M; et al Neonatal repair of truncus arteriosus: continuing improvement in outcomes. Ann Thorac Surg, 2001.PMID 11515872
- [4]Russell HM; Pasquali SK; Jacobs JP; et al Outcomes of repair of common arterial trunk with truncal valve surgery: a review of the society of thoracic surgeons congenital heart surgery database. Ann Thorac Surg, 2012.PMID 22088417
- [5]Goldmuntz E 22q11.2 deletion syndrome and congenital heart disease. Am J Med Genet C Semin Med Genet, 2020.PMID 32049433
- [6]O'Byrne ML; Yang W; Mercer-Rosa L; et al 22q11.2 Deletion syndrome is associated with increased perioperative events and more complicated postoperative course in infants undergoing infant operative correction of truncus arteriosus communis or interrupted aortic arch. J Thorac Cardiovasc Surg, 2014.PMID 24629220
- [7]Derridj N; Villemain O; Khoshnood B; et al Outcomes after common arterial trunk repair: Impact of the surgical technique. J Thorac Cardiovasc Surg, 2021.PMID 33342576
- [8]Fontan F; Baudet E Surgical repair of tricuspid atresia. Thorax, 1971.PMID 5089489
- [9]Anderson PA; Sleeper LA; Mahony L; et al Contemporary outcomes after the Fontan procedure: a Pediatric Heart Network multicenter study. J Am Coll Cardiol, 2008.PMID 18598886
- [10]Rychik J; Atz AM; Celermajer DS; et al Evaluation and Management of the Child and Adult With Fontan Circulation: A Scientific Statement From the American Heart Association. Circulation, 2019.PMID 31256636
- [11]Sananes R; Goldberg CS; Newburger JW; et al Six-Year Neurodevelopmental Outcomes for Children With Single-Ventricle Physiology. Pediatrics, 2021.PMID 33441486
- [12]Rudd NA; Ghanayem NS; Hill GD; et al Interstage Home Monitoring for Infants With Single Ventricle Heart Disease: Education and Management: A Scientific Statement From the American Heart Association. J Am Heart Assoc, 2020.PMID 32777961