Paeds · cardiology
Ventricular septal defect
Also known as Ventricular septal defect · VSD · Interventricular communication · Perimembranous VSD · Maladie de Roger (small VSD)
Fellowship guide to the commonest congenital heart defect: the anatomic and haemodynamic classification of a ventricular septal defect, the left-to-right shunt physiology, the natural history from spontaneous closure to Eisenmenger syndrome, the murmur and heart-failure presentations, echocardiographic sizing, and the surgical, device and medical management across infancy and adolescence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A ventricular septal defect (VSD) is a congenital communication between the two ventricles through the interventricular septum. Because the left ventricle generates higher pressures than the right, blood shunts from left to right across the defect. The result is extra blood flowing into the pulmonary circulation, and the child's whole clinical course is set by how much blood crosses that gap. [1]
The VSD is the commonest congenital heart lesion present at birth, accounting for roughly thirty to forty percent of all structural heart disease. It sits at one end of a spectrum so wide that it runs from a tiny muscular defect that closes itself within weeks to a large non-restrictive defect that floods the lungs, causes infant heart failure, and over years can cause irreversible pulmonary vascular disease. [1] [2]
Classification
A VSD is classified on two independent axes: where it sits on the septum (anatomy) and how much it restricts the shunt (haemodynamics). Both must be stated, because a small perimembranous VSD and a large inlet VSD are entirely different clinical problems that share only the name. [1] [9]
The anatomic types are defined by their position viewed from the right ventricle. A perimembranous defect sits in the membranous septum next to the atrioventricular and aortic valves and is by far the commonest type, making up about eighty percent of defects. A muscular defect lies within the muscular septum, often has multiple fenestrations, and is the type most likely to close spontaneously. An inlet defect lies posteriorly behind the tricuspid valve and is the ventricular component of an atrioventricular septal defect, classically seen in Down syndrome. An outlet (subarterial, supracristal, doubly-committed) defect lies beneath the semilunar valves and is uncommon in European populations but more common in Asian populations; it carries a particular risk of aortic cusp prolapse and aortic regurgitation. [1] [9]
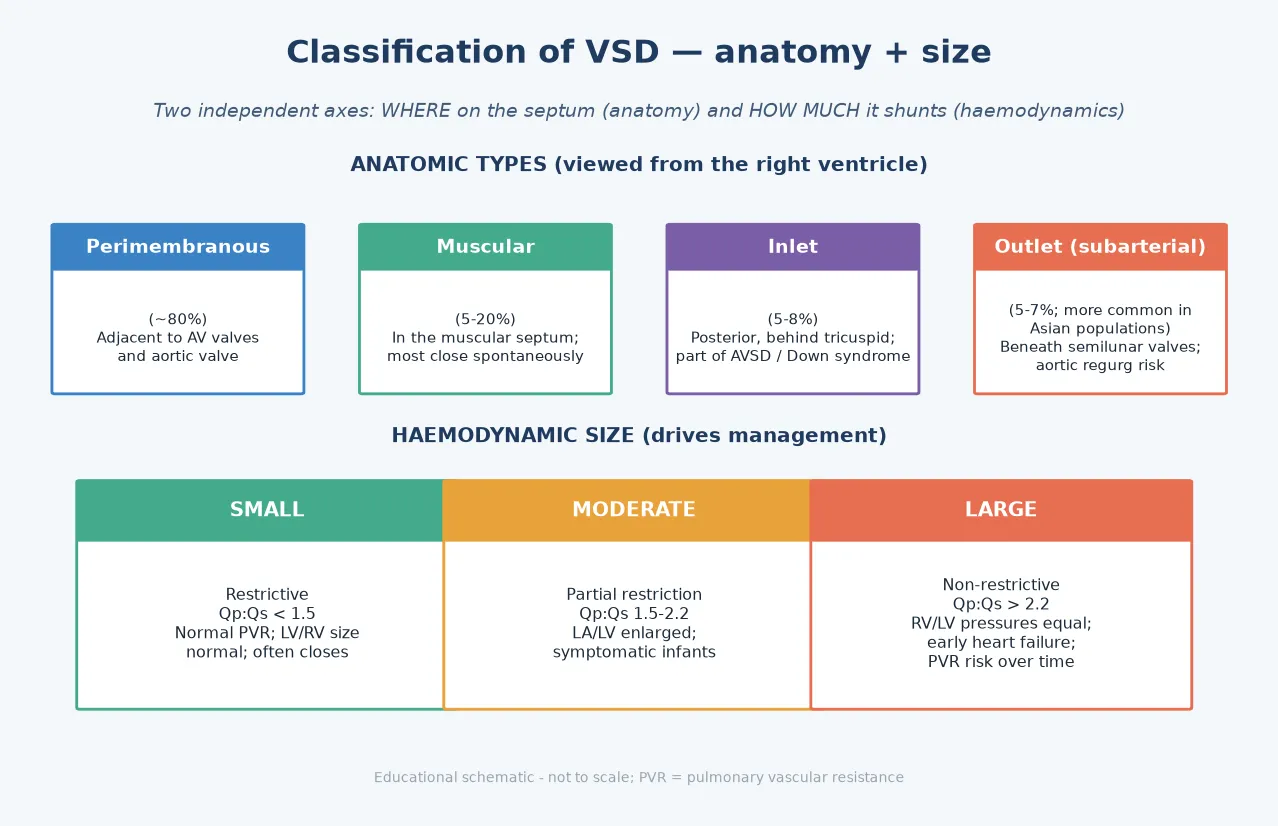
The haemodynamic size is what governs management and prognosis, and it is judged on echocardiography. A small (restrictive) defect has a Qp:Qs under 1.5, a large pressure gradient across it, normal chamber sizes, and is usually asymptomatic. A moderate defect partially restricts flow, has a Qp:Qs of roughly 1.5 to 2.2, dilates the left atrium and left ventricle, and typically causes symptomatic overcirculation in infancy. A large (non-restrictive) defect allows right and left ventricular pressures to equalise, has a Qp:Qs over 2.2, and causes early heart failure with a real risk of progressive pulmonary vascular disease if left unrepaired. [1] [9]
Epidemiology & Risk Factors
The VSD is the commonest congenital heart defect at birth. The worldwide birth prevalence meta-analysis of van der Linde and colleagues put ventricular septal defect at the top of the structural heart lesions, with a prevalence that rises sharply when tiny muscular defects detected by sensitive echocardiography are included. Hoffman and Kaplan's landmark incidence review established that the VSD accounts for roughly thirty to forty percent of all congenital heart disease, with an incidence around three to four per thousand live births for clinically significant lesions. [1] [2]
A meaningful proportion of children with a VSD have an associated chromosomal anomaly, syndrome, or extracardiac malformation. Meberg's population study found that among infants with congenital heart defects, chromosomal and syndromic associations and extracardiac malformations were common enough to mandate a careful dysmorphology examination and, where indicated, genetic testing. Trisomy 21 is strongly associated with inlet and atrioventricular septal defects; 22q11 deletion is associated with outlet and conotruncal defects; and Turner, Noonan and Holt-Oram syndromes each carry their own cardiac signature. [10]
The modifiable and non-modifiable risk factors are mostly genetic and environmental. A family history of congenital heart disease roughly triples the recurrence risk. Maternal diabetes, rubella infection, alcohol and certain anticonvulsant exposures all raise the risk. Prematurity increases the chance of detecting a muscular VSD, which then usually closes. The practical point for counselling is that a VSD in a syndromic infant demands a genetics referral, while an isolated small VSD in an otherwise well child carries a near-normal outlook. [10]
Pathophysiology
The shunt direction in a VSD is set by the pressure difference between the ventricles. The left ventricle pumps at systemic pressure and the right ventricle at much lower pulmonary pressure, so blood flows left to right across the defect throughout systole. The volume of that shunt depends on two things: the size of the hole, and the pulmonary vascular resistance. Both change over the first weeks of life, which is why a VSD that looks quiet at birth can declare itself dramatically a month later. [1]
The left-to-right shunt floods the pulmonary circulation and returns extra blood to the left atrium and left ventricle. The left ventricle is the chamber that does the work of pumping blood to the body and then again across the defect to the lungs, so it is the left ventricle that dilates and fails. This is the volume-load physiology of a VSD, and it explains why the infant in overcirculation shows signs of left-heart failure: tachypnoea from pulmonary congestion, poor weight gain from the metabolic cost of the extra work, and sweating with feeds. [1] [9]
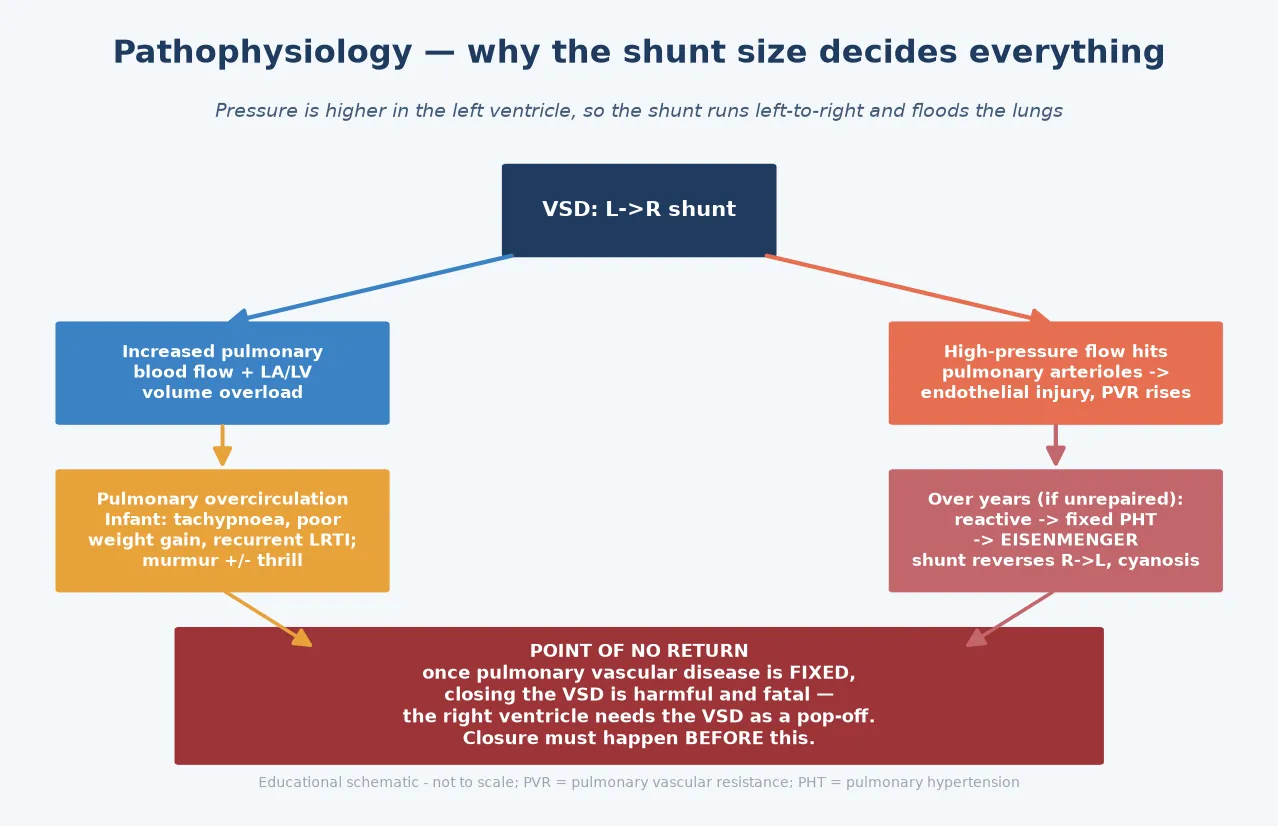
The pulmonary vascular story is the part that carries the gravest long-term consequence. A large non-restrictive shunt drives high-pressure, high-flow blood through the pulmonary arterioles. Over years this causes endothelial injury, medial hypertrophy and eventually irreversible remodelling. The pulmonary vascular resistance rises, first reversibly and then fixed. When resistance exceeds systemic, the shunt reverses to right-to-left and the child becomes cyanotic: this is Eisenmenger syndrome. The cruel fact is that once the disease is fixed, the right ventricle relies on the defect as a pressure pop-off, and closing it is harmful and can be fatal. [6] [9]
Clinical Presentation
The presentation depends almost entirely on shunt size. A small restrictive VSD presents with a murmur and nothing else: a loud, harsh, holosystolic murmur at the lower left sternal border (third or fourth intercostal space), often with a thrill, picked up at the six-week check or a routine examination. The child feeds well, grows normally, and is never symptomatic. This is the maladie de Roger presentation, and it is the commonest scenario in primary care. [1]
A moderate or large VSD presents with signs of pulmonary overcirculation and left-heart failure. The infant is tachypnoeic, particularly with feeds, sweats and tires during feeding, gains weight poorly, and may have recurrent lower respiratory infections. On examination there is a pansystolic murmur at the lower left sternal border, an apical mid-diastolic murmur of increased mitral inflow (the flow rumble), a hyperactive precordium, and hepatomegaly. The louder and more harsh the murmur, the smaller the defect tends to be; a large defect with equal ventricular pressures produces a softer, shorter murmur because the gradient is low. [1] [9]
A large VSD that has progressed to pulmonary hypertension shows a right ventricular heave and a loud pulmonary component of the second heart sound. Once Eisenmenger physiology develops the picture changes again: the systolic murmur softens or disappears as the shunt equalises, the child or adolescent becomes cyanosed and clubbed, and they describe exertional dyspnoea, haemoptysis and syncope. Eisenmenger syndrome is now rare in countries with early diagnosis and repair, but it remains the dominant concern for anyone presenting with a large unrepaired VSD in adolescence or adulthood. [6] [9]
Differential Diagnosis
The murmur of a VSD must be distinguished from the other systolic murmurs of childhood, and the key discriminator is the character and radiation of the murmur rather than the mere presence of one. An innocent (Still's) murmur is a short, vibratory, low-pitched ejection murmur at the lower left sternal border that changes with position and has no thrill or signs of overload. A VSD murmur, by contrast, is harsh, holosystolic, and fixed. [1]
Mitral regurgitation produces a pansystolic murmur too, but it radiates to the axilla and is loudest at the apex, not the sternal border. Subvalvar (subaortic) stenosis and hypertrophic obstructive cardiomyopathy give ejection systolic murmurs that change with maneuvres, not pansystolic murmurs. A small patent ductus arteriosus gives a continuous murmur, and tetralogy of Fallot contains a VSD but adds a pulmonary stenosis murmur and, when severe, cyanosis. Tricuspid regurgitation is rare as an isolated lesion in children but produces a pansystolic murmur at the lower left sternal border with prominent v waves. [1] [9]
For the infant presenting in failure, the differential of pulmonary overcirculation is a VSD, a PDA, an atrioventricular septal defect, or a large aortopulmonary shunt. Echocardiography resolves all of these definitively. The trap to avoid is assuming that a well-looking neonate with a murmur needs no investigation: any pansystolic murmur with a thrill needs an echo, because a small VSD is managed very differently from early critical obstruction. [1]
Clinical & Bedside Assessment
Bedside assessment starts with the murmur and moves to the growth, feeding and perfusion that reveal the shunt's haemodynamic weight. Characterise the murmur precisely: site (lower left sternal border for most VSDs, apex for a muscular defect near the moderator band), timing (holosystolic), quality (harsh), grade, and the presence of a thrill. Then listen for the apical mid-diastolic flow rumble that signals a large left-to-right shunt, and split the second heart sound to check for a loud pulmonary component suggesting pulmonary hypertension. [1] [9]
Growth and feeding are the most sensitive markers of a significant shunt. Ask specifically about feeding: volume per feed, time taken, sweating, breath-holding or colour change, and the trend in weight centiles. A previously thriving infant crossing weight centiles downward over weeks has a significant shunt until proven otherwise. Look for tachypnoea and subcostal recession, a hyperactive precordium, and hepatomegaly as signs of heart failure, and assess the pulses and perfusion — a collapsing (bounding) pulse suggests a run-off lesion such as a PDA rather than a VSD. [1]
A syndromic examination completes the assessment. Look for the features of Down syndrome (inlet and atrioventricular septal defects), the palatal, thymic and calcium features of 22q11 deletion (outlet and conotruncal defects), and the stigmata of Turner, Noonan and Holt-Oram syndromes. Any syndromic finding mandates a genetics referral, because it changes the prognosis, the counselling, and the surveillance for associated lesions. [10]
Investigations
Echocardiography is the definitive investigation for a VSD, and in almost every child it is the only imaging needed. It defines the location and number of defects, measures the size and the shunt, estimates the Qp:Qs, and — critically — estimates the pulmonary artery pressure from the tricuspid regurgitation jet and from the gradient across the defect. It also identifies associated lesions and assesses the aortic valve for cusp prolapse and regurgitation, which changes management. [1] [4]
The electrocardiogram is supportive rather than diagnostic. A small VSD shows a normal ECG. A moderate VSD shows left atrial and left ventricular overload (deep S in V1, tall R in V6). A large VSD with pulmonary hypertension shows biventricular hypertrophy and right-axis deviation. The chest radiograph mirrors the shunt: a small VSD has a normal film, a moderate-to-large shunt shows cardiomegaly with pulmonary plethora and increased vascular markings, and established Eisenmenger physiology shows oligoemic (pruned) lung fields as the resistance rises. [1] [9]
Cardiac catheterisation is reserved for selected cases. It is used to measure the pulmonary vascular resistance directly and to test vasoreactivity in an older child or adult with a large shunt, to decide whether closure is safe. Closing a defect in the face of fixed, high pulmonary vascular resistance is dangerous, so a catheter-derived resistance is the final arbiter of operability when the echo is borderline. Blood tests are directed at the consequences and the context: a full blood count for the anaemia that worsens failure, iron studies in cyanotic Eisenmenger patients prone to iron deficiency, and genetic testing in syndromic infants. [9]
Management — Resuscitation
The resuscitation scenario is the infant presenting in heart failure from overcirculation at four to eight weeks. The priority is to relieve pulmonary congestion and improve feeding and growth while the definitive plan is made. Give a loop diuretic such as furosemide at 1 to 2 mg/kg/day, add an angiotensin-converting-enzyme inhibitor such as captopril or enalapril to reduce the afterload on the left ventricle and therefore the shunt, and increase caloric density of the feeds to overcome the metabolic cost of the extra cardiac work. [1]
Oxygen is used cautiously. Because oxygen is a pulmonary vasodilator, giving it freely lowers pulmonary vascular resistance and can actually increase the left-to-right shunt and worsen failure; oxygen should be reserved for the genuinely hypoxic infant and titrated to saturations. Treat any intercurrent infection or anaemia promptly, as both precipitate decompensation. A small number of infants with severe failure need admission, nasogastric or continuous feeding, and occasionally non-invasive respiratory support or intubation while awaiting surgical closure. [1]
Furosemide (heart-failure bridge in infant overcirculation)
Loading dose
1 mg/kg PO/IV
Maintenance dose
1–2 mg/kg/day in 1–2 divided doses
Immediate management of the overcirculating infant
Assess ABC, perfusion and feeding; weigh and plot growth
Start a loop diuretic (furosemide 1–2 mg/kg/day) for pulmonary congestion
Add an ACE inhibitor (captopril/enalapril) to reduce afterload and shunt
Increase caloric density of feeds; consider nasogastric supplementation
Use oxygen only if hypoxic; treat intercurrent infection and anaemia
Urgent echocardiogram to size the defect and estimate pulmonary pressure
Refer to paediatric cardiology for a closure plan within the first year
Management — Definitive & Stepwise
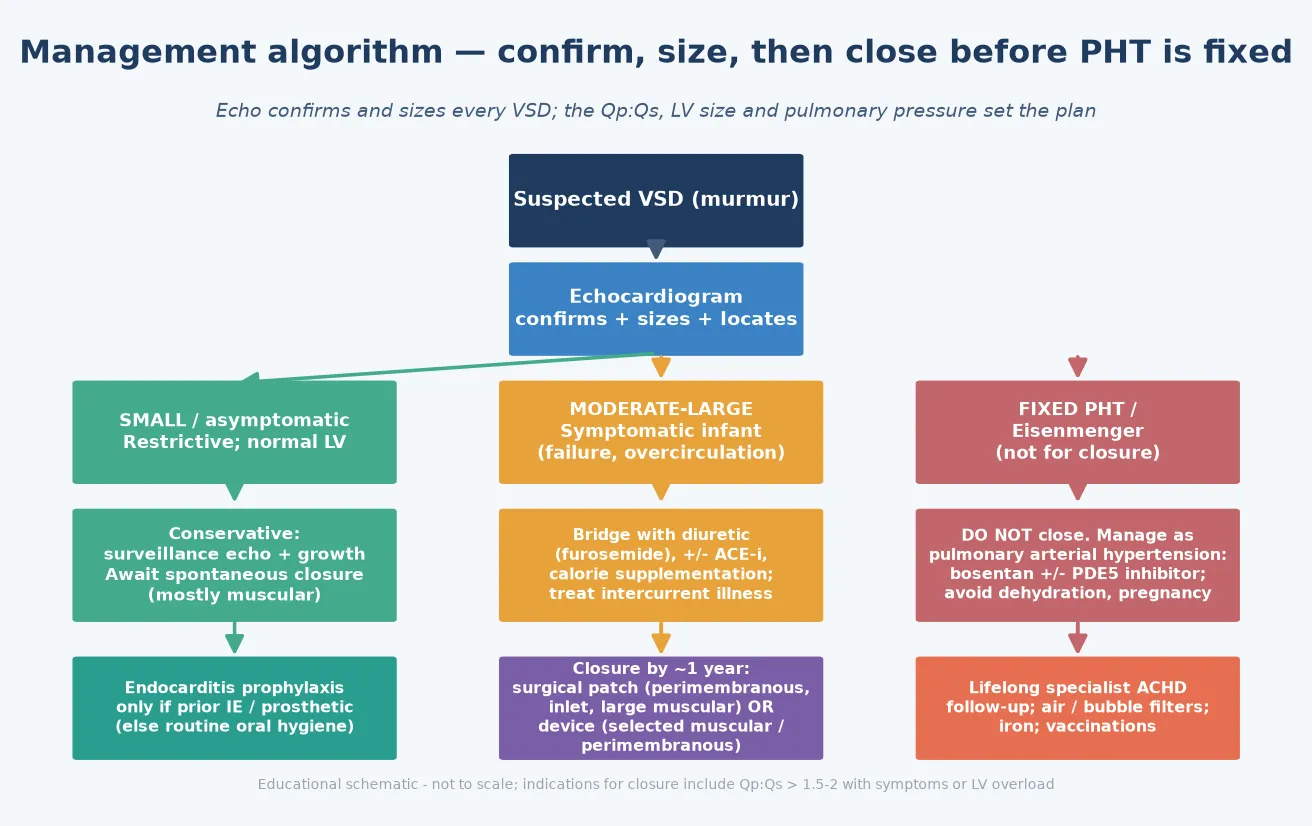
Definitive management is stratified by the haemodynamic size. A small restrictive VSD needs no intervention: arrange surveillance echocardiography every one to two years, reassure the family that many defects close spontaneously (especially muscular ones), and allow normal activity. The Du and Roguin study of muscular defects detected in neonates confirmed that the majority of small muscular VSDs close in the first years of life, which underpins the conservative strategy. [3]
A moderate or large symptomatic VSD is managed with a medical bridge followed by closure, usually within the first year. The aim is to close the defect before pulmonary vascular disease becomes fixed, and to relieve the failure that is blunting growth. Surgical closure with a prosthetic patch remains the standard for most perimembranous, inlet and large muscular defects. Transcatheter device closure, established by the Carminati and Butera series using the Amplatzer occluders, is an alternative for selected muscular defects and for perimembranous defects with favourable anatomy, though it carries a small risk of atrioventricular block and aortic regurgitation that must be weighed. [4] [5]
The indications for closure are a symptomatic child with a significant shunt, a Qp:Qs above roughly 1.5 to 2 with left ventricular overload, recurrent infective endocarditis, or aortic regurgitation from cusp prolapse — which can be an indication even when the shunt itself is small. In a tiny or very sick infant who is not yet a candidate for definitive repair, pulmonary artery banding can be used as a palliative bridge to restrict pulmonary flow and protect the lungs until the child grows enough for a complete repair. [1] [9]
A VSD with Eisenmenger syndrome is never closed. The pulmonary vascular disease is fixed, the right ventricle depends on the defect as a pop-off, and closure is harmful. Instead, these patients are managed as pulmonary arterial hypertension with targeted therapy. The BREATHE-5 randomised trial of Galiè and colleagues showed that bosentan, an endothelin-receptor antagonist, improved pulmonary vascular resistance and exercise capacity in Eisenmenger syndrome, with longer-term benefit confirmed in the open-label extension reported by Gatzoulis and colleagues. These patients require lifelong adult congenital heart disease care. [6] [7]
[4] [6] [9]Specific Subtypes & Scenarios
The perimembranous VSD is the type an examiner most often expects you to discuss in depth. It sits beneath the aortic valve, which means the right or non-coronary cusp can prolapse into the defect. This prolapse can reduce the shunt but causes progressive aortic regurgitation, so a perimembranous VSD with even mild aortic regurgitation is followed closely and often closed early to protect the valve before the regurgitation becomes severe. [1] [4]
The muscular VSD is the type most likely to close spontaneously. The Du and Roguin neonatal series showed that the majority of small muscular defects identified in the newborn period close within the first one to two years, and even moderate muscular defects can shrink. Multiple muscular defects, sometimes described as a Swiss-cheese septum, can be challenging to close surgically and may be amenable to staged transcatheter device closure. [3] [5]
The inlet VSD is the ventricular component of an atrioventricular septal defect and is strongly associated with Down syndrome. It sits behind the tricuspid valve and involves the atrioventricular valves, so the surgical repair is more complex than a simple patch closure, and these children need assessment for a primum atrial defect, a cleft mitral valve, and the characteristic unbalanced atrioventricular canal. The outlet (subarterial, doubly-committed) VSD is more common in Asian populations and carries a particularly high risk of aortic cusp prolapse and regurgitation, prompting early closure. [10]
Across Australia, New Zealand and the United Kingdom, surgical patch closure remains the standard for most perimembranous, inlet and large muscular defects. Transcatheter device closure is offered in specialist centres for selected muscular defects and for perimembranous defects with favourable rims and no aortic-valve involvement, after the Carminati and Butera evidence. Pulmonary artery banding as a bridge is reserved for small, sick infants not yet fit for a complete repair. Local paediatric cardiology network protocols guide the device-versus-surgery decision and the timing of referral. [4] [5]
Complications & Pitfalls
The complications of a VSD are haemodynamic, infectious and iatrogenic. The dominant haemodynamic complication is pulmonary vascular disease progressing to Eisenmenger syndrome in a large unrepaired defect. The infectious complication is infective endocarditis, which seeds on the high-velocity jet at the defect edge or on the right ventricular wall opposite. The iatrogenic complications of surgical closure include complete heart block from atrioventricular node injury, residual or recurrent VSD, and pericardial effusion; device closure adds the risks of device embolisation, aortic regurgitation, and late atrioventricular block. [1] [8]
The pitfalls are about timing and about not over-treating. The first pitfall is to miss the four-to-eight-week presentation of overcirculation by attributing poor feeding to reflux or poor weight gain to feeding technique. The second is the opposite error: over-investigating and over-treating a small asymptomatic VSD that has a loud murmur but no haemodynamic consequence, when surveillance and reassurance are the correct strategy. The third is to close, or to allow progression toward closure in, a defect whose pulmonary vascular disease is already fixed — the irreversible error. [1] [9]
Prognosis & Disposition
The prognosis of a VSD is excellent when the defect is appropriately stratified and managed. A small restrictive VSD has a normal life expectancy, with the majority of muscular defects and a meaningful proportion of perimembranous defects closing spontaneously in the first years of life. A moderate or large VSD repaired in infancy, before the onset of fixed pulmonary hypertension, also has an excellent long-term outlook, with most children achieving normal growth, activity and quality of life. [1] [3]
The prognosis darkens sharply once Eisenmenger syndrome is established. Advanced pulmonary vascular disease reduces exercise capacity, raises the risk of arrhythmia, haemoptysis, thromboembolism, and the maternal mortality of pregnancy, and shortens life expectancy. Targeted pulmonary vasodilator therapy with bosentan, confirmed by the BREATHE-5 trial and its extension, improves functional capacity and symptoms but does not reverse the disease. This is why the entire strategy of paediatric VSD care is to prevent Eisenmenger syndrome by closing the defect in time. [6] [7]
Disposition follows the severity. Every child with a confirmed or suspected VSD is referred to paediatric cardiology for echocardiographic sizing and a management plan. A small VSD is followed in the outpatient clinic; a moderate-to-large symptomatic VSD is managed with the cardiology and surgical team in a tertiary centre; and any adolescent or adult with Eisenmenger physiology is transitioned to lifelong adult congenital heart disease care. Endocarditis prophylaxis is no longer routine for most VSDs — the 2021 American Heart Association statement restricts it to prosthetic valves, prior endocarditis, and certain complex unrepaired or repaired lesions — so the emphasis shifts to good oral hygiene and prompt evaluation of unexplained fever. [8] [9]
Special Populations
The syndromic infant is the first special population. Down syndrome carries a high rate of atrioventricular and inlet septal defects; 22q11 deletion carries outlet and conotruncal defects; and each syndrome brings extracardiac issues — immunodeficiency, hypocalcaemia, airway anomalies, developmental needs — that shape perioperative care. A confirmed VSD in a dysmorphic infant mandates a genetics assessment, because the diagnosis changes the surveillance, the counselling, and sometimes the surgical timing. [10]
The preterm infant is the second. Premature babies frequently have a PDA and may also have a muscular VSD, both of which often close as the infant matures. The preterm infant with a significant shunt is managed by balancing the haemodynamic load against the risk of intervention in a small, fragile patient, and the threshold for medical versus surgical closure is set by the local neonatal and cardiology team. [1]
The adolescent with Eisenmenger syndrome is the third and the most vulnerable. Pregnancy carries a substantial maternal mortality, so reliable contraception and pre-conception counselling are central to the consultation. Dehydration, altitude, and invasive procedures with air or particulate emboli are dangerous because of the right-to-left shunt, so intravenous lines need filters and careful air exclusion. These patients are best served in a dedicated adult congenital heart disease service with pulmonary hypertension expertise. [6] [9]
Evidence, Guidelines & Regional Differences
The evidence base for VSD management is strongest on natural history, device closure, and Eisenmenger therapy. Hoffman and Kaplan established the incidence, and van der Linde's meta-analysis established the worldwide birth prevalence, confirming the VSD as the commonest congenital heart lesion. The Du and Roguin neonatal series underpinned the expectant management of small muscular defects by documenting a high spontaneous closure rate. [1] [2] [3]
The device-closure evidence comes from the Carminati and Butera series, which established the feasibility and the early and long-term results of transcatheter closure of perimembranous and muscular defects with Amplatzer occluders, including their complication profile of block and aortic regurgitation. The Eisenmenger evidence rests on the BREATHE-5 randomised trial of bosentan by Galiè and colleagues, with the Gatzoulis extension confirming sustained functional benefit. Together these trials shifted Eisenmenger syndrome from a condition with only supportive care to one with disease-modifying therapy. [4] [5] [6] [7]
The guideline landscape is shared between the American and European congenital cardiology bodies. The 2020 European Society of Cardiology guidelines for adult congenital heart disease, summarised by Baumgartner and De Backer, set the framework for the transition and lifelong care of repaired and unrepaired VSDs, including the thresholds for closure and the management of Eisenmenger syndrome. The 2021 American Heart Association infective endocarditis statement restricted antibiotic prophylaxis to high-risk groups only, which removed routine endocarditis prophylaxis from most VSD care and placed the emphasis on oral hygiene and prompt fever evaluation. [8] [9]
Across ANZ, the United Kingdom, Europe and North America, the consensus is identical in principle: a significant VSD is closed during infancy, before pulmonary vascular resistance becomes fixed. The thresholds for device versus surgery, the timing of surveillance echocardiography, and the endocarditis-prophylaxis rules vary in detail by guideline body and centre, but the central strategy — size the defect, close the symptomatic and the moderate-to-large, and never close an Eisenmenger defect — is uniform across high-resource settings. [4] [8] [9]
Exam Pearls
VSD management lanes — 'SMALL-MED-IRREVERSIBLE'
References
- [1]Hoffman JI; Kaplan S The incidence of congenital heart disease. J Am Coll Cardiol, 2002.PMID 12084585
- [2]van der Linde D; Konings EE; Slager MA; Witsenburg M; Helbing WA; Takkenberg JJ; Roos-Hesselink JW Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol, 2011.PMID 22078432
- [3]Du ZD; Roguin N; Wu XJ Spontaneous closure of muscular ventricular septal defect identified by echocardiography in neonates. Cardiol Young, 1998.PMID 9855105
- [4]Butera G; Carminati M; Chessa M; Piazza L; Abella R; Biondi-Zoccai GG; Negura DG; Magro F; Pantaleo A; Amin Z Transcatheter closure of perimembranous ventricular septal defects: early and long-term results. J Am Coll Cardiol, 2007.PMID 17868812
- [5]Carminati M; Butera G; Chessa M; Drago M; Negura D; Piazza L Transcatheter closure of congenital ventricular septal defect with Amplatzer septal occluders. Am J Cardiol, 2005.PMID 16399093
- [6]Galiè N; Beghetti M; Gatzoulis MA; Granton J; Berger RM; Lauer A; Chiossi E; Landzberg M; Bosentan Randomized Trial of Endothelin Antagonist Therapy-5 (BREATHE-5) Investigators Bosentan therapy in patients with Eisenmenger syndrome: a multicenter, double-blind, randomized, placebo-controlled study. Circulation, 2006.PMID 16801459
- [7]Gatzoulis MA; Beghetti M; Galiè N; Granton J; Berger RM; Lauer A; Chiossi E; Landzberg M Longer-term bosentan therapy improves functional capacity in Eisenmenger syndrome: results of the BREATHE-5 open-label extension study. Int J Cardiol, 2008.PMID 17658633
- [8]Wilson WR; Gewitz M; Lockhart PB; Bolger AF; DeSimone DC; Koenig MJ; Sadhu Lohr J; Miro JM; Padera RF; Prendergast BD; Sexton DJ; Spelman DW; Tleyjeh IM; Van der Meer JTM; Westermann CJL; Whited W; Wojda TR; American Heart Association Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association. Circulation, 2021.PMID 33853363
- [9]Baumgartner H; De Backer J The ESC Clinical Practice Guidelines for the Management of Adult Congenital Heart Disease. Eur Heart J, 2020.PMID 33128054
- [10]Meberg A; Hals J; Thaulow E Congenital heart defects--chromosomal anomalies, syndromes and extracardiac malformations. Acta Paediatr, 2007.PMID 17590185