Paeds · child-safety-and-social-paediatrics
Children in out-of-home care and foster care
Also known as Looked-after children · Children in foster care · Children in care · Kinship and residential care · Care-experienced children · Out-of-home care health
A fellowship approach to health care for children living in out-of-home (foster, kinship, residential) care: classification of placement and legal status; the heavy cumulative mental-health, developmental, attachment, growth, immunisation, dental and sensory burden and its toxic-stress mechanism; a trauma-informed initial and comprehensive health assessment on entry to care; consent-authority and conditional confidentiality when the state may hold parental responsibility; management of developmental, behavioural, educational and growth needs; permanency and transition planning — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old is brought to your clinic three days after moving into his third foster placement. He will not speak, his carer cannot find his immunisation record, and his caseworker phones to ask "what's wrong with him." This is the everyday work of caring for children in out-of-home care, and the clinical skill it tests is delivering consistent, trauma-aware medicine to a child whose young life has already been disrupted. [1] [4]
Out-of-home care is the arrangement made when a child cannot safely live with their family of origin and is placed, usually under child-protection authority, in the care of relatives, an approved foster family, or a residential setting. It is short-term for some and long-term for others, and for many it ends only when the young person grows up and leaves the care system. [1] [2]
What makes this population clinically distinct is not the placement itself but the accumulated adversity that brought the child there and that often continues as placements move. Mental-health difficulty, developmental and educational delay, attachment disturbance, growth faltering, untreated dental disease and incomplete immunisation are all far more common than in community peers. Recognising that burden — and treating the child rather than the paperwork — is the core task. [3] [6] [7]
The clinician's role is to be the stable, trusted medical home that the chaos of placement moves cannot easily break. You assess on entry, you screen at every contact, you coordinate the team around the child, and you plan for permanency and — for older children — the handover to adult care, so that aging out does not mean dropping out of health. [1]
Classification
Begin with the child in front of you, then classify where they are living and what legal authority governs their care, because the second determines who can consent to your treatment. [1]
Kinship care
Relative or family friend
- Preserves family, culture and identity
- Often the most stable and least disruptive
- Carers may themselves need support and resources
- Still requires the full health-needs lens
Family-based foster
Approved non-relative household
- The most common placement type
- Approved and supervised carers
- Stability varies with carer support and matching
- Higher need accumulates with each placement change
Residential / group
Staffed unit
- Older children and those with complex needs
- Higher rates of mental-health and behavioural difficulty
- Greater exposure to risk and placement turnover
- Needs intensive multidisciplinary input
Therapeutic / treatment
Specialised
- For high medical or behavioural acuity
- Embeds clinical and trauma-informed care
- Often a step-up or step-down from residential
- Plan for step-down to family-based care where possible
The legal or care status runs alongside the placement and matters most at the bedside because it fixes who holds parental responsibility. A placement may be voluntary (the family agrees to temporary care and parents usually retain parental responsibility), statutory or court-ordered (a child-protection authority holds placement decisions), interim or emergency (short-term pending assessment or court), or long-term until majority (permanency not to the family of origin, with aging out typically at 18 to 21). Before you treat, you must know which of these applies, because it tells you whether a parent, a guardian, the state, or — for a capable older child — the young person themselves can consent. [1] [4]
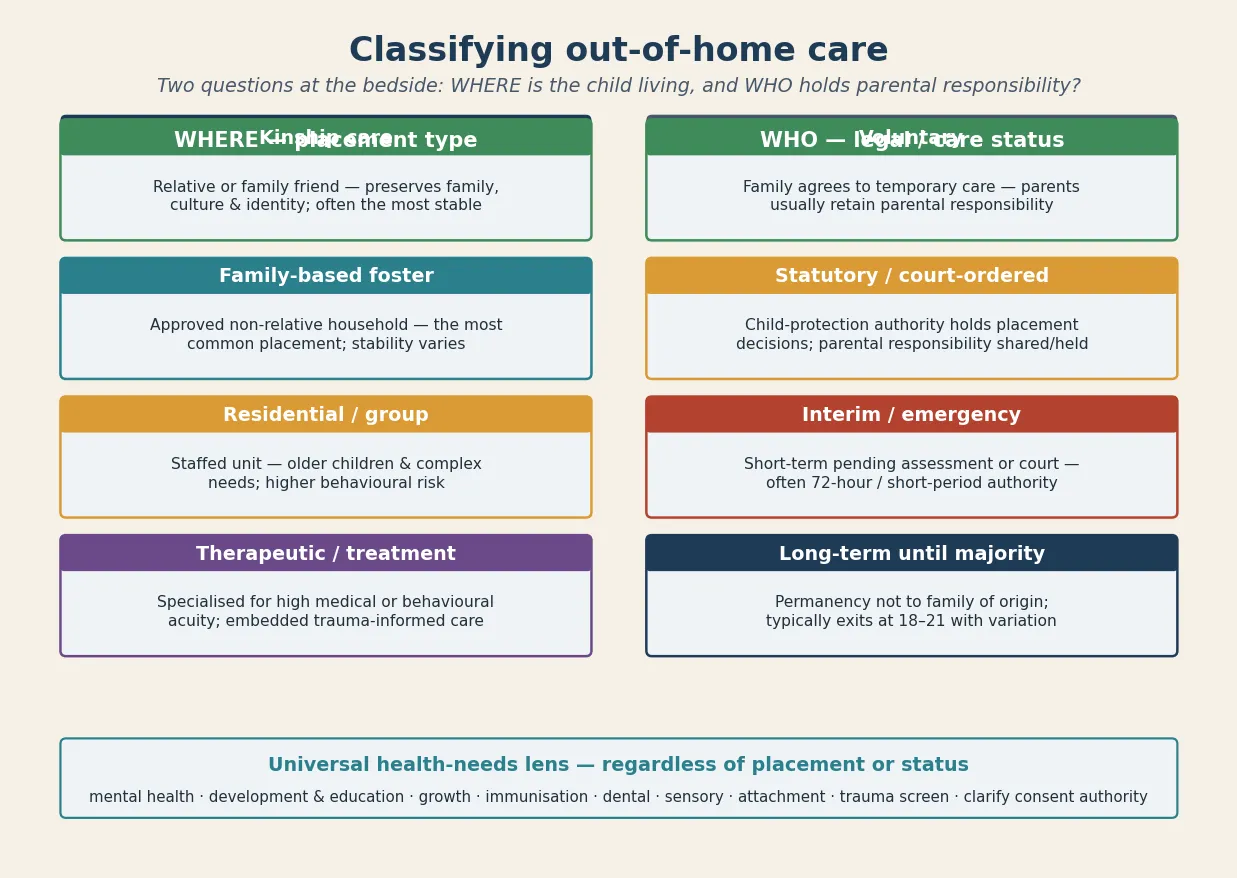
Whatever the placement, the health-needs lens is universal. Every care-experienced child deserves a trauma-informed assessment, a mental-health and developmental screen, attention to attachment, growth, immunisation, dental and sensory health, and a clear statement of who can consent. The placement changes the intensity and the risks; it does not change the bundle. [1] [6]
Epidemiology & Risk Factors
Out-of-home care is common across the English-speaking jurisdictions an examiner will expect you to know. Tens of thousands of children live in care in Australia, the UK, the US and Canada at any time, with entry driven most often by neglect, parental substance use, family violence, parental mental illness, and abuse. [1] [2]
Infants and young children are over-represented among those entering care, which makes the developmental and attachment stakes especially high — the brain and stress-response systems are most plastic in exactly the years these children are most exposed to adversity. [9] [5]
The health burden is not a small upward shift; it is large across nearly every domain an examiner names. Mental-health disorders are several-fold more prevalent in children in foster care than in community peers, and developmental delay, learning difficulty and educational underachievement are markedly more common. [3] [7]
Physical health problems are both more prevalent and harder to address, with well-described barriers to optimal care: fragmented records, moving between clinicians, carers who do not know the history, and systems that treat the placement crisis rather than the child. Growth faltering, untreated dental caries, uncorrected vision and hearing deficits, asthma and other chronic disease are all over-represented. [6] [11]
Adverse childhood experiences are the engine of this burden, and the relationship is dose-responsive: each additional ACE, and each additional placement move, adds to the dose and independently worsens outcome beyond the original maltreatment. This is why placement stability is itself a health intervention. [8] [5]
Subgroups carry the highest risk and are the ones an examiner will probe: infants and young children, those with multiple placements, those in residential or group care, Indigenous and minority children (over-represented in care), children with disability or chronic disease, and those aging out without continuity. [1] [3]
The long-term outcomes for children who grow up in or age out of care — in mental health, education, employment, housing and early mortality — are the measure of whether the system, not just the visit, worked. [8] [16]
Pathophysiology
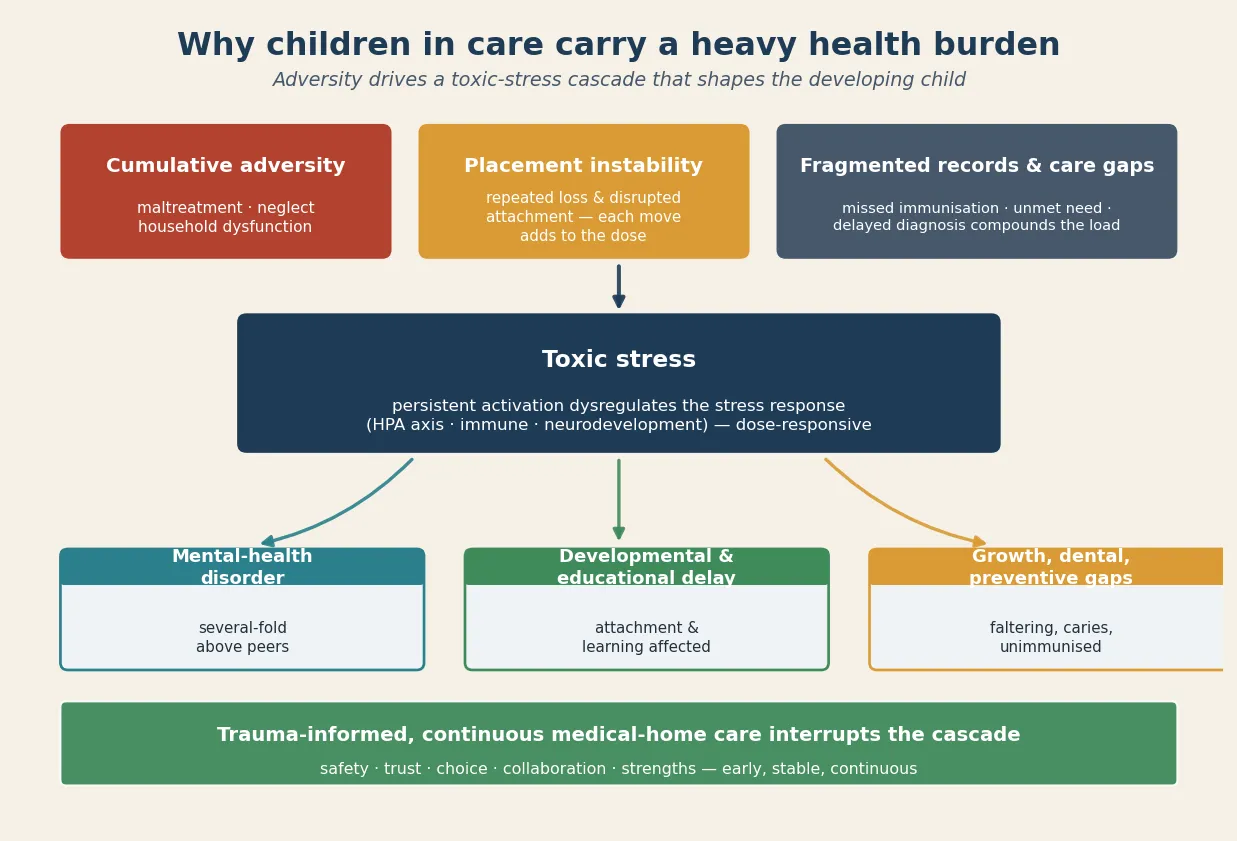
The clinical picture only makes sense once you see how adversity becomes biology. Maltreatment, neglect, parental adversity and the disruption of repeated placement moves accumulate as adverse childhood experiences, and those experiences act on a developing child through a toxic-stress mechanism. [5] [4]
Toxic stress persistently activates and dysregulates the stress response — the HPA axis, immune signalling and neurodevelopment — so that the developing brain is shaped by chronic threat rather than by safety. The relationship is dose-responsive: more cumulative adversity and more disrupted attachment produce more dysregulation, which is why the youngest children, whose brains are most plastic, carry the deepest developmental risk. [9] [5]
Disrupted attachment in infancy and early childhood is its own mechanism of harm. A child who has lost, or never reliably had, a caregiving figure learns that adults are unpredictable, and that learning shows up as hypervigilance, indiscriminate friendliness, watchful compliance, emotional dysregulation or rejection of a new carer — behaviours that are adaptations to chaos, not signs of a primary disorder. [9] [10]
Placement instability worsens outcomes on top of the original adversity because each move severs relationships (with carer, school, clinician and peers), restarts the loss, and fractures the records that continuity depends on. A child who has moved four times in a year has had four chances to fall through the gaps. [4] [8]
Trauma also changes how a child experiences the clinical encounter itself. Authority, separation from the carer, undressing for examination, being asked personal questions, or being told what to do can all read as threat to a child shaped by danger — so hypervigilance, freezing, dissociation or over-compliance in your room are clinical data, not rudeness. [4] [5]
Finally, fragmented records and care discontinuity compound the biological burden by delaying identification and treatment — a child's asthma, hearing loss, developmental delay or unmet immunisation simply goes unrecognised through the moves. [6] [12]
Clinical Presentation
A child may arrive in your orbit in two ways: acutely, in the days around removal, or routinely, for the scheduled entry-to-care assessment. The acute presentation is the emergency — disclosed abuse, a suspicious injury, acute illness, self-harm or severe neglect, including an infant with faltering growth. The routine presentation is the planned visit at which the hidden burden is meant to be found. [1] [4]
Unrecognised mental-health and trauma difficulty shows itself differently in a younger child than in an adolescent. Look for behavioural regression (loss of toilet training, sleep disturbance, feeding difficulty), aggression, withdrawal, somatic complaints, school refusal, and — in older children — self-harm or substance use. None of these is a diagnosis on its own; each is a signal to screen. [7] [3]
Developmental and educational difficulty presents differently across age. An infant may show global delay or poor attachment; a preschooler may have language delay and dysregulated play; a school-age child may present with learning difficulty, inattention and behavioural problems that have been attributed to "naughtiness" rather than to unmet need. [9] [11]
Attachment-related difficulty has a recognisable shape: indiscriminate friendliness with strangers, watchful over-compliance, rejection of or clinginess toward the carer, and rapid emotional escalation that the child cannot settle. These are the behaviours that tempt clinicians and carers to reach for a disruptive-behaviour label before they have assessed the attachment history. [10] [9]
Placement instability presents clinically as a pattern rather than a single event — missed appointments, repeat acute presentations, lost prescriptions, regression after each move, and a child who "was fine until the last placement change." The pattern is the diagnosis. [4] [6]
A trauma history may surface only indirectly. A child who freezes when you reach for them, who flinches at a raised voice, who dissociates during the examination, or who is suspiciously over-compliant is telling you something about safety, and you should document it and act on it. [5] [4]
At the routine entry assessment you will often find the unmet burden made concrete: fragmented or absent immunisation, growth faltering or obesity, untreated dental caries, uncorrected vision or hearing deficits, and developmental delay that no one has yet named. [6] [11] [14]
Differential Diagnosis
The central diagnostic skill in this population is telling apart behaviours and findings that are trauma-driven from those that signal a discrete disorder — and resisting the pull to label too quickly. Attachment-related behaviour and dysregulation can look like a primary mental-health or behavioural disorder, but they are first and foremost adaptations to adversity, and they shift when the child feels safe and attached. [9] [10]
Developmental delay caused by early adversity and neglect must be distinguished from a specific neurodevelopmental disorder such as fetal alcohol spectrum disorder, intellectual developmental disorder or autism. The history matters: neglect, prenatal substance exposure, and a chaotic early environment can each produce delay that improves with stability, so a single assessment on the day of removal undercalls the child's potential. [7] [9]
Trauma-driven hypervigilance, avoidance and inattention overlap with anxiety disorders and ADHD, and the two are often genuinely co-occurring rather than either-or. The useful question is not "trauma or ADHD?" but "what does this child need, in what order, to feel safe enough for an accurate picture to emerge?" [3] [7]
When a care-experienced child presents with a somatic complaint, you must hold two truths at once: physical illness is real and common in this group (and is often missed), and trauma also manifests somatically. Avoid diagnostic overshadowing — never assume a symptom is "just behavioural" until you have excluded organic disease. [6] [4]
Indiscriminate friendliness, the attachment behaviour in which a child seeks comfort from unfamiliar adults without discrimination, must be distinguished from a normally sociable child (who still checks back with a trusted carer) and from a manic or disinhibited presentation. The distinguishing feature is the absence of a preferred, selective attachment figure. [10] [9]
"Non-adherence" in this group is often mislabelled. Before calling it refusal, ask whether the child has moved, whether prescriptions and records followed them, and whether the carer understood the plan. Most apparent non-adherence is a systems failure dressed up as a patient failure. [6] [4]
Finally, a disclosure of abuse or a suspicious injury shifts the frame from differential diagnosis to safeguarding. The decision is whether immediate activation is required now versus continued assessment — and when in doubt, consult child-protection services and document the reasoning. [4] [1]
Clinical & Bedside Assessment
Open every encounter with the trauma-informed principles an examiner will look for: safety, trust, choice, collaboration and strengths. Greet the child first, before the carer; explain what the visit is for; let the child keep a comfort object and the carer close; offer choice about the sequence of the examination; and pace the assessment so the child is not overwhelmed. [4] [5]
Before you assess or treat, clarify and document consent authority. Who holds parental responsibility — parent, guardian, the state — and, for an older child, does the young person have capacity for the decision at hand under the mature-minor principle? Record the answer; it governs every intervention that follows. [1]
[1] [4]Take a reconstructed history when records are fragmented: birth and perinatal history, developmental milestones, educational trajectory, placement history (how many, how long, why each ended), immunisation where it can be found, and a trauma-informed psychosocial history adapted to the child's age. Use a trained interpreter where needed — never the child or an untrained carer for sensitive content. [1] [2]
Examine trauma-informed. Explain what you will do before you do it, let the child say stop, leave underwear on, and prioritise the most important findings first so you do not lose a frightened child's cooperation. Measure growth and plot it; look for signs of neglect, dental caries, and uncorrected vision or hearing; and screen development against age expectations. [4] [6]
Screen for mental-health, trauma and attachment difficulty in a developmentally appropriate way. For younger children this means structured parent- or carer-report measures of behaviour, trauma symptoms and social-emotional development, read alongside the attachment observation; for older children add validated self-report screens for depression, anxiety, PTSD and suicidality. [3] [9]
Document to protect the child and inform the care team lawfully: record what was found, what was disclosed, who holds consent authority, what was shared and why, and the plan — in language that serves the child at the next placement, not only this one. [1] [4]
Investigations
The AAP standard sets the investigation bundle, and examiners expect you to reproduce it. An initial screening within roughly 72 hours of entry triages acute problems — growth, a brief physical and developmental screen, vision and hearing, mental-health and trauma screen, and targeted testing for any acute concern. [1] [13]
The comprehensive assessment within 30 days completes the bundle: growth and puberty, vision and hearing, dental review, developmental and educational screen, mental-health and trauma screen, sexual-health assessment where age-appropriate, immunisation reconstruction with catch-up, and laboratory testing. [1] [4]
What the comprehensive laboratory and screening bundle typically covers
Targeted laboratory testing on entry addresses the common hidden burdens: a full blood count and iron studies, lead level where exposure is plausible, an infection screen (including tuberculosis and, where indicated, blood-borne viruses), and — for age-appropriate and risk-appropriate cases — sexual-health screening and pregnancy testing. Vision, hearing and dental are referral-triggering screens, not optional extras. Reconstruct the immunisation record from every available source and plan catch-up to the national schedule.
Which screening instruments you choose should match the child's age and the setting. For preschool children, standardised parent-report tools for social-emotional development and trauma symptoms read well alongside structured attachment observation; for school-age children, add validated behavioural and educational screens; and arrange a formal developmental or psychoeducational assessment whenever delay or learning difficulty is suspected. [9] [11]
Sensory deficits are common and easily missed. A primary-care medical home for children in foster care finds high rates of previously undiagnosed audiologic, ophthalmologic, developmental and neurologic diagnoses, so test vision and hearing at entry and refer early. [11]
Growth data should be interpreted against the history of deprivation and catch-up needs. Faltering growth may reflect neglect or organic disease (and requires both workup and nutrition rehabilitation), while rapid weight gain after entry can reflect recovery — but also the obesity risk that accompanies early adversity. [6] [2]
Management — Resuscitation
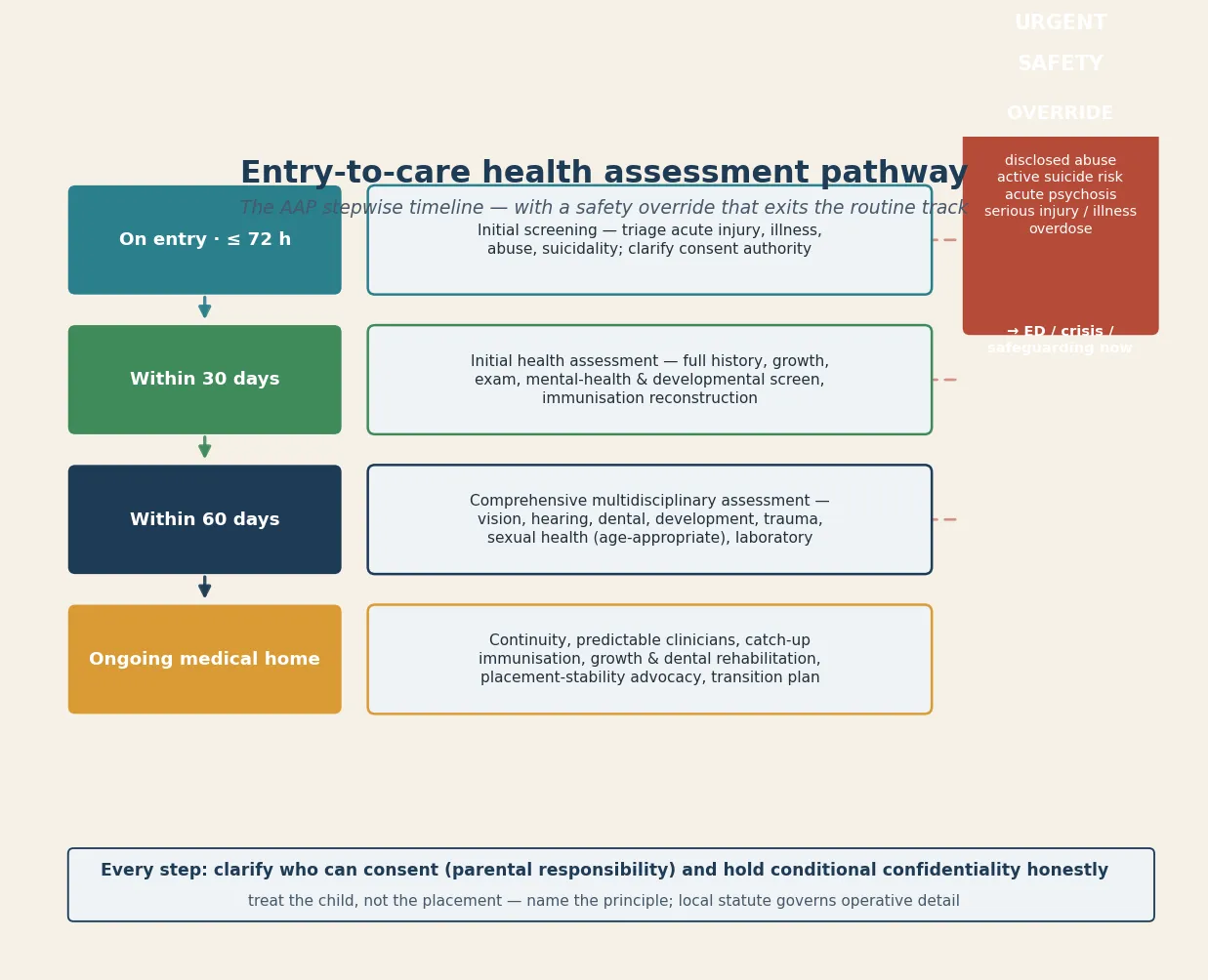
The "resuscitation" step in this topic is the immediate safety override: the things you cannot wait for the routine assessment pathway to address. Disclosed abuse, a suspicious or inflicted injury, an infant with faltering growth, acute serious illness, an overdose, self-harm or active suicide risk all exit the routine pathway and trigger same-day safeguarding, mental-health crisis or ED activation. [4] [1]
Activate the pathway while preserving the therapeutic relationship. Tell the child and the carer what you are doing and why, involve safeguarding or crisis services as required, and stay engaged so the safety action does not read as abandonment. A child who has been removed once already is exquisitely alert to being "passed on." [4] [5]
When consent authority is unclear or held by the state and a time-critical decision is pending, act in the child's best interests while you clarify — but clarify and document as fast as you can, and involve the child-protection authority and any legal guardian. Life- or limb-threatening decisions never wait for paperwork, but everything else should follow the documented authority. [1]
Stabilise and treat the acute physical problem — injury, infection, severe malnutrition or a mental-health crisis — and at the same time begin organising ongoing, placement-appropriate care, because the child will leave your acute encounter into a carer and a system that must be ready to continue. [4] [6]
A disclosure of abuse during the assessment is itself a resuscitation-level event: listen, do not interrogate, record the child's own words, and escalate to child-protection services and forensic assessment as the local pathway requires. Your job is to hear and protect, not to investigate. [1] [4]
Management — Definitive & Stepwise
Definitive management is the AAP stepwise timeline, delivered through a trauma-informed medical home. The timeline to reproduce verbatim is: initial screening on entry (within about 72 hours), initial health assessment within 30 days, and comprehensive multidisciplinary assessment within 30 days. [1]
Entry-to-care health assessment timeline
On entry · ≤ 72 h
Initial screening — triage acute injury, illness, abuse, suicidality; clarify consent authority; begin records reconstruction.
Within 30 days
Initial health assessment — full history, growth, examination, mental-health and developmental screen, immunisation reconstruction.
Within 30 days
Comprehensive multidisciplinary assessment — vision, hearing, dental, development, trauma, sexual health (age-appropriate), laboratory, referrals.
Ongoing
Trauma-informed medical home — continuity, catch-up immunisation, growth and dental rehabilitation, placement-stability advocacy, transition plan.
The written health care plan captures the assessment, the diagnoses, the medications, the immunisation status, the outstanding referrals and the follow-up — and it travels with the child. Specify who receives it (carer, caseworker, primary care, the child's file) so the next placement inherits the work, not the void. [1] [2]
Deliver ongoing care as a medical home: the same clinicians, predictable visits, strengths-based reviews, and a single coordinator who holds the plan across moves. Continuity is the treatment, because fragmented acute-only contact reproduces the instability that made the child unwell. [4] [1]
Coordinate the multidisciplinary team deliberately — paediatrician, mental-health clinician, dental, education and early-intervention services, social work, and the carer — because no single clinician can meet the bundle. Name a coordinator and document the shared plan. [1] [15]
Manage developmental delay, attachment difficulty and behavioural need with evidence-based intervention first. Structured mental-health and wellbeing interventions show measurable effectiveness for care-experienced children and young people, so psychological therapy and trauma-focused approaches are the foundation; reserve psychotropic medication for defined indications under specialist oversight, and avoid the reflexive over-medication of trauma-driven behaviour, especially in young children. [15] [7]
Catch up immunisation to the national schedule, rehabilitate growth and nutrition with the carer, and arrange dental care early — these are concrete, fixable targets that change a child's trajectory. [12] [6]
Support placement stability and the carer, who is parenting a traumatised child and often needs their own guidance and respite. Advocate for the child's educational and developmental needs, and treat carer support as part of the child's treatment plan, not a side issue. [4] [5]
Plan for permanency early, and for older children plan transition to adult care from the mid-teens: a written health summary, an active connection to adult primary and mental-health services, and attention to housing, education and continuity, so that aging out does not collapse care. [16] [8]
Specific Subtypes & Scenarios
Infants and toddlers entering care are the highest-stakes subgroup because attachment and brain development are most vulnerable. Prioritise attachment observation, developmental screen, growth and nutrition, and early-intervention referral; support the carer to build a predictable, responsive caregiving relationship; and reassess development after a period of stability, because a single early snapshot undercalls potential. [9] [5]
The child with multiple placements and severe distrust needs above all a clinician who does not give up. Pace the relationship, keep the same clinician across visits, do not interpret distrust as refusal, and rebuild the assessment as trust allows. Placement instability is the enemy; advocate for stability as a clinical intervention. [4] [8]
Kinship versus residential or group care changes the intensity and the risk. Kinship care tends to be more stable and preserves culture and identity but may strain the carer; residential and group care serves older children and those with complex needs but carries higher behavioural risk and turnover, and needs intensive multidisciplinary input. [1] [3]
A child with a suspected neurodevelopmental disorder or attachment disorder needs careful, staged assessment. Distinguish reactive attachment disorder and disinhibited social engagement disorder (which require a history of grossly pathogenic care and are diagnoses of persistent pattern, not a single clinic visit) from autism, FASD and intellectual developmental disorder; arrange specialist assessment; and treat the attachment environment as part of the treatment. [10] [9]
An Indigenous or minority child requires culturally safe care: respect for family and community decision-making, acknowledgement of the over-representation rooted in colonisation and systemic disadvantage, and locally appropriate services including Aboriginal community-controlled organisations where available. Cultural safety is clinical safety here. [1] [4]
An unaccompanied minor or refugee child brings the psychological legacy of displacement on top of care-experience: take a trauma-informed catch-up history, address missed preventive care, use a trained interpreter, and screen for infectious disease and mental-health need. [1]
A child with complex chronic disease or technology dependence in care needs an especially robust written care plan, carer training and respite, and a named coordinator — because the cost of a fragmented handover is highest for the most medically fragile child. [6] [2]
The child approaching permanency — whether the goal is reunification, long-term care, special guardianship or adoption — needs the health plan locked in before the legal change, so that continuity and identity (including the child's history and heritage) travel with them. [1] [16]
Complications & Pitfalls
The most common pitfall is failing to clarify and document consent authority before acting. Treating a child in care without knowing whether the parent, a guardian or the state holds parental responsibility is both legally unsafe and clinically confused — and it is the first thing an examiner will probe. [1]
Fragmented records and care discontinuity cause direct harm: missed immunisation, duplicate or omitted testing, lapsed prescriptions, and a child whose history has to be retold at every placement. Prevent it by writing a health summary that travels with the child and by naming a coordinator. [6] [12]
Placement instability undermines every treatment plan. A prescription, a therapy referral and a follow-up appointment are only as good as the child's ability to keep them across a move — so build plans that survive moves, and advocate for stability as a clinical intervention. [4] [8]
[15] [7]Diagnostic overshadowing is the mirror image: a physical illness, a developmental need or a sensory deficit is dismissed as "just behaviour" or "just the foster care background," and treatable disease is missed. Hold both truths — trauma is real, and so is organic disease — and investigate appropriately. [6] [11]
A poorly handled safeguarding disclosure or examination can retraumatise the child and breach trust. Listen without interrogating, examine trauma-informed, explain confidentiality overrides in advance, and never use the carer as an interpreter or sole historian for sensitive content. [4] [1]
Finally, failure to plan for permanency and transition leaves a child without continuity of care and, for the aging-out young person, often without an adult clinician, housing or a record of their own history. The drop-off at aging out is where harm concentrates, and it is preventable. [16] [8]
Prognosis & Disposition
Prognosis here means the trajectory of safety, developmental catch-up, mental-health recovery, educational engagement and stable relationships — and it is more modifiable than it looks. Placement stability, early developmental and mental-health support, and a continuous medical home all move the trajectory in the child's favour. [4] [1]
Routine disposition is a stable placement, a completed assessment bundle, a shared written care plan, and a safe child with routine follow-up in the medical home. [1]
Early-review disposition is a new disclosure, a placement move, an incomplete assessment, or a child still building trust — bring them back in days to weeks, not months. [4]
Urgent disposition is active suicide risk, disclosed abuse or exploitation, acute psychosis, medical instability, or severe unmet physical need (including an infant with faltering growth) — use ED, crisis or safeguarding pathways the same day. [3] [1]
Safety-net explicitly: who to call tonight, when to come back sooner, and how confidentiality will work with carer and caseworker after any override. Close the loop after mental-health, safeguarding, education or placement involvement. [1] [4]
Over time, early, trauma-informed, continuous medical-home care improves trajectory compared with fragmented acute-only contact — and the long-term outcomes for care-leavers in mental health, education, employment and housing are the measure of whether the system, not just the visit, worked. [8] [16]
Special Populations
Indigenous children (Aboriginal, Torres Strait Islander, Māori, First Nations). Over-represented in care across all four jurisdictions, a legacy rooted in colonisation and systemic disadvantage; cultural safety, respect for family and community decision-making, and locally appropriate services (including Aboriginal community-controlled organisations) are essential. Racism is a health exposure. [1] [4]
Unaccompanied minors, refugee and asylum-seeking children. Use trained interpreters, take a trauma-informed catch-up history, address missed preventive care and infectious-disease screening, and attend to the psychological legacy of displacement on top of care-experience. [1]
Children with disability, neurodiversity or complex chronic disease. Adapt communication and capacity assessment to ability, use supported decision-making, avoid diagnostic overshadowing, and provide an especially robust written care plan and coordinator — because fragmented handover costs most for the most fragile child. [6] [2]
Infants and toddlers. The developmental and attachment stakes are highest here, so prioritise attachment observation, developmental screen, growth and nutrition, early-intervention referral, and carer support to build a responsive caregiving relationship. [9] [5]
Minority and migrant children. Over-represented and vulnerable; address language, culture, and the intersection of racism and care-experience in the assessment and plan. [1]
Rural and remote children. Fragmented service access and small-community dual relationships threaten confidentiality and continuity; create deliberate pathways including telehealth with a private space. [1]
Children in contact with youth justice. Clarify consent and information-sharing between the care and justice systems, and maintain the same trauma-informed, continuity-based approach — these children carry the compounded burden of both. [4]
Evidence, Guidelines & Regional Differences
The AAP standard. The American Academy of Pediatrics Council on Foster Care, Adoption, and Kinship Care clinical report — Szilagyi and colleagues, 2015 — sets the current practice standard: a medical home, screening on entry, entry screening within 72 hours, comprehensive assessment within 30 days, and coordinated, trauma-informed ongoing care. This is the framework an examiner expects you to know. [1] [2]
The health burden, quantified. Engler's 2022 systematic review establishes the several-fold elevation in mental-health disorder among children in foster care; Deutsch's 2015 reviews lay out the physical health problems and barriers to care and the mental-health, behavioural and developmental issues for youth in care. Together these anchor the high-yield screening bundle. [3] [6] [7]
Attachment and the young child. Vasileva's 2018 meta-analysis links attachment, development and mental health in maltreated preschool children in foster care, and Bruce's 2019 study characterises reactive attachment disorder in maltreated young children in care — evidence that the youngest children carry the deepest developmental and attachment risk and that the environment is part of the treatment. [9] [10]
Hidden sensory and developmental need. Reynoso's 2022 study of a primary-care medical home for children in foster care documents high rates of previously undiagnosed audiologic, ophthalmologic, developmental and neurologic diagnoses — the evidence base for screening vision, hearing and development at entry. [11]
Trubey et al, 2024 — mental-health interventions for care-experienced children and young people
Systematic review and meta-analysis
Population: Children and young people in foster, kinship and residential care
Key finding
Structured mental-health and wellbeing interventions show measurable effectiveness in this population, supporting evidence-based psychological therapy as first-line treatment.
Practice change
Reserve psychotropic medication for defined indications under specialist oversight; offer evidence-based psychological intervention as the foundation of the mental-health plan, especially in young children.
Preventive gaps. Walton and Bedford document incomplete immunisation coverage in looked-after children, and Sarvas documents high unmet dental need — concrete, fixable targets that change a child's trajectory. [12] [14]
Aging out and care-leaving. Rebbe's work links adverse childhood experiences to young-adult health outcomes among youth aging out, and Taylor's 2024 systematic review and meta-analysis identifies the policies and interventions — extended support, preparation, stable relationships — that improve outcomes for young people leaving out-of-home care. [8] [16]
ANZ: each state and territory governs child-protection legislation, care-leaving ages and mandatory-reporting duties; Aboriginal community-controlled services and cultural-safety requirements apply. RCH Melbourne provides clinical guidance for children in care. UK: NICE guidance on looked-after children and young people (NG205) frames assessment and ongoing care; local-authority corporate parenting and the role of the designated doctor and designated nurse for looked-after children apply. US: the AAP foster-care clinical report sets the standard; Medicaid and the Chafee Foster Care Independence Act frame coverage and transition support, and care-leaving typically occurs around 18 to 21 with state variation. Canada: provincial child-welfare legislation governs; Indigenous child and family services and Jordan's Principle apply for First Nations, Inuit and Métis children.
State the principle and check local law. Do not invent a universal care-leaving age or a universal consent rule — they do not exist, and the child-protection authority and local statute govern the operative detail. [1] [4]
Exam Pearls
- Open every answer with trauma-informed principles — safety, trust, choice, collaboration, strengths — then the timing standard: entry screen within 72 hours, comprehensive within 30 days. [1] [4]
- Always clarify and document consent authority (parental responsibility) before treating a child in care. [1]
- Name the high-prevalence needs: mental health, development and education, attachment, growth, immunisation, dental, sensory. [3] [11] [14]
- Distinguish attachment-related behaviour from primary disorder — indiscriminate friendliness and watchful compliance are clues to adversity, not diagnoses of RAD on a single visit. [9] [10]
- Mental-health disorder prevalence is several-fold higher than community peers — screen at every contact, and prefer evidence-based therapy over medication in young children. [3] [15]
- Hold conditional confidentiality honestly — be explicit about what carer and caseworker will and will not be told. [1]
- Plan permanency early and transition to adult care from the mid-teens with a written health summary before the young person leaves care. [16] [8]
References
- [1]Szilagyi MA, Rosen DS, Rubin D, Zlotnik S, Council on Foster Care, Adoption, and Kinship Care, Committee on Adolescence, Council on Early Childhood Health Care Issues for Children and Adolescents in Foster Care and Kinship Care. Pediatrics, 2015.PMID 26416934
- [2]Simms MD, Dubowitz H, Szilagyi MA Health care needs of children in the foster care system. Pediatrics, 2000.PMID 11044143
- [3]Engler AD, Sarpong KO, Van Horne BS, Greeley CS, Keefe RJ A Systematic Review of Mental Health Disorders of Children in Foster Care. Trauma, Violence & Abuse, 2022.PMID 32686611
- [4]Schilling S, Fortin K, Forkey H Medical Management and Trauma-Informed Care for Children in Foster Care. Current Problems in Pediatric and Adolescent Health Care, 2015.PMID 26381646
- [5]Forkey H, Szilagyi M Foster care and healing from complex childhood trauma. Pediatric Clinics of North America, 2014.PMID 25242716
- [6]Deutsch SA, Fortin K Physical Health Problems and Barriers to Optimal Health Care Among Children in Foster Care. Current Problems in Pediatric and Adolescent Health Care, 2015.PMID 26364980
- [7]Deutsch SA, Lynch A, Zlotnik S Mental Health, Behavioral and Developmental Issues for Youth in Foster Care. Current Problems in Pediatric and Adolescent Health Care, 2015.PMID 26409926
- [8]Rebbe R, Nurius PS, Courtney ME, Ahrens KR Adverse Childhood Experiences and Young Adult Health Outcomes Among Youth Aging Out of Foster Care. Academic Pediatrics, 2018.PMID 29709622
- [9]Vasileva M, Petermann F Attachment, Development, and Mental Health in Abused and Neglected Preschool Children in Foster Care: A Meta-Analysis. Trauma, Violence & Abuse, 2018.PMID 27663993
- [10]Bruce M, McDermott JM, Fisher L, Young J, Manning L Reactive Attachment Disorder in maltreated young children in foster care. Attachment & Human Development, 2019.PMID 30021488
- [11]Reynoso M, Hsieh A, Sun S, Marin M, Levine K, Pletcher E, Sarvet B, Szilagyi M, Forkey H, Mackie T Description of Audiologic, Developmental, Ophthalmologic, and Neurologic Diagnoses at a Primary Care Medical Home for Children in Foster Care. Journal of Developmental & Behavioral Pediatrics, 2022.PMID 36040833
- [12]Walton S, Bedford H Immunization of looked-after children and young people: a review of the literature. Child: Care, Health and Development, 2017.PMID 28317146
- [13]Szilagyi M, Schulte E Issues Related to Laboratory Screening for Children and Adolescents Entering Foster Care. Pediatrics, 2017.PMID 29141917
- [14]Sarvas EW, Eckerle JK, Gustafson KL, Freese RL, Shlafer RJ Oral health needs among youth with a history of foster care: A population-based study. Journal of the American Dental Association, 2021.PMID 34090662
- [15]Trubey R, Evans R, McDonald S, Noyes J, Robling M, Willis S, Boffey M, Wooders C, Vinnicombe S, Melendez-Torres GJ Effectiveness of Mental Health and Wellbeing Interventions for Children and Young People in Foster, Kinship, and Residential Care: Systematic Review and Meta-Analysis. Trauma, Violence & Abuse, 2024.PMID 38362816
- [16]Taylor D, Albers B, Mann G, Lewis J, Taylor R, Mendes P, Macdonald G, Shlonsky A Systematic Review and Meta-Analysis of Policies and Interventions that Improve Health, Psychosocial, and Economic Outcomes for Young People Leaving the Out-of-Home Care System. Trauma, Violence & Abuse, 2024.PMID 38828776