Paeds · child-safety-and-social-paediatrics
Expert reports and court evidence in child protection
Also known as Expert witness testimony in child protection · Medico-legal reports in child abuse · Court reports and giving evidence · Paediatrician as expert witness · Forensic medical evidence in child protection · Reasonable medical certainty and the courts
Fellowship-level guide to expert reports and court evidence in child protection: the paediatrician's distinct roles as witness of fact, professional witness and expert witness; how to structure a defensible expert report; the standards of certainty (balance of probabilities, reasonable medical certainty); how to prepare for and survive cross-examination; the duty owed to the court above any instructing party; and the personal impacts of giving evidence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture yourself, three months from now, sitting in a witness box while opposing counsel reads back a sentence from your report and asks whether you were "really sure." The work you do at the bedside today — the quality of the history, the precision of the examination, the discipline of the documentation — is what makes that moment survivable. An expert report and the oral testimony that follows it are the point at which your clinical reasoning is translated into a form a court can use to decide a child's future. [1]
A court report (also called a medico-legal report, expert's report, or statement) is a written document prepared by a clinician for use in legal proceedings. It sets out what was found, what was done, the clinician's reasoning, and — when the clinician is instructed as an expert — the opinion that arises from that reasoning. The report is the primary vehicle by which medical evidence reaches the court; in many cases the matter resolves on the written reports alone, and oral testimony is never given. [2]
Court evidence is the body of information a court is permitted to consider in reaching its decision. Medical evidence is one part of it, alongside the accounts of parents, witnesses, police and social workers. The paediatrician's evidence contributes the objective clinical substrate — the injuries found, their pattern, the differential, and the reasoned opinion about causation — but it never determines the legal outcome alone. The court weighs the medical evidence with all the other evidence before it. [6]
The expert witness is a clinician instructed because of specialised knowledge the court does not possess, who offers an opinion the court could not form for itself. This is the key distinction from an ordinary witness, who may only state facts within their direct observation. Skellern framed it plainly: the medical expert's role is to safeguard children by giving the court the best available medical understanding, while simultaneously safeguarding the profession and the public by refusing to overstate what the evidence supports. [6]
[1] [6]Classification
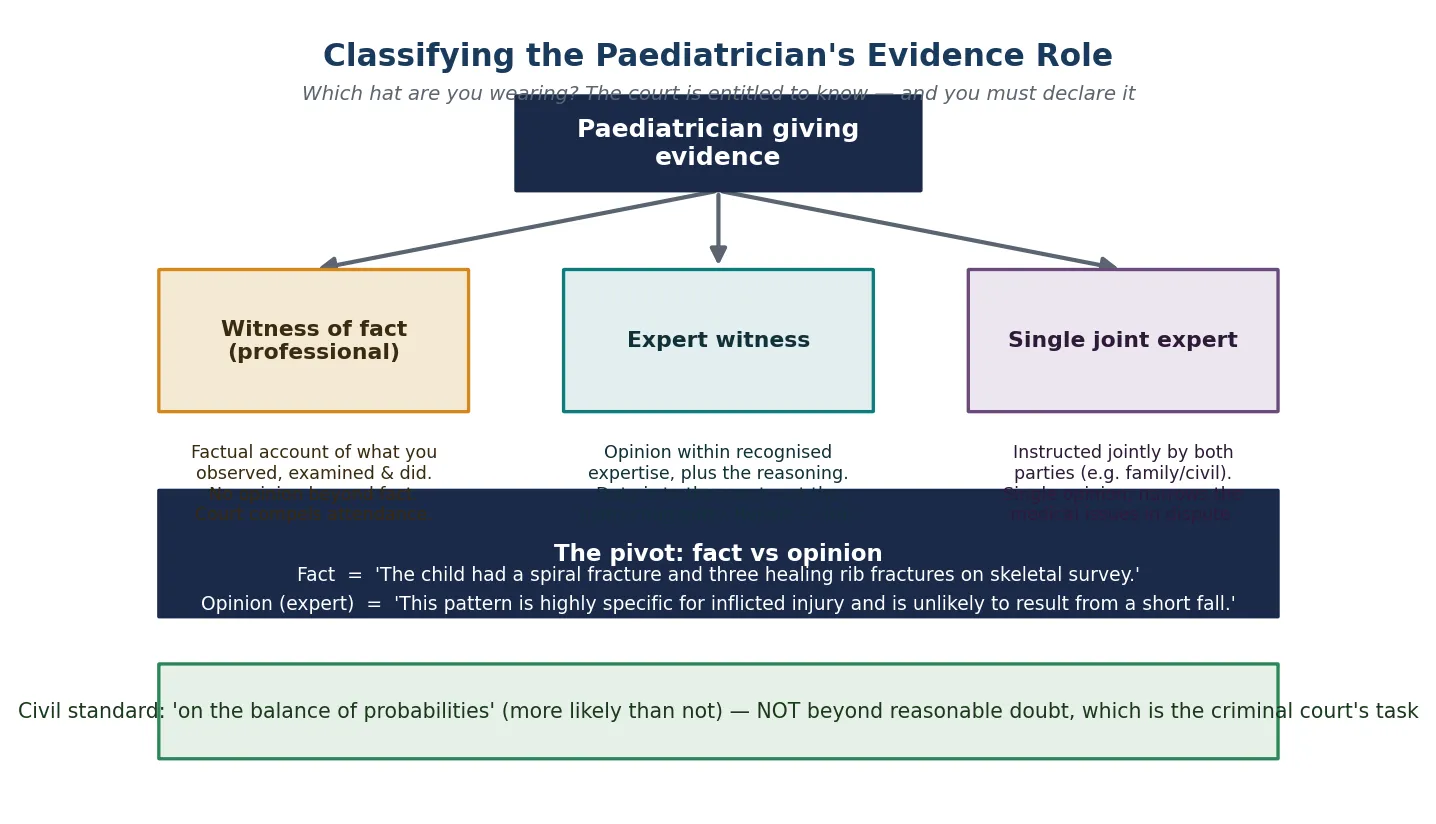
Start from which role you occupy, because the role dictates what you may say and how the court receives it. The same clinician can be all three across a career, and sometimes across a single case — so the classification is about function, not title. [2]
A witness of fact (sometimes called a professional witness of fact) gives a factual account of what they observed, examined and did. The treating paediatrician who admitted the child, examined the injuries and ordered the skeletal survey is a witness of fact when called to describe those actions. A witness of fact may not offer opinion evidence in most circumstances; they confine themselves to what they personally perceived. [2]
A professional witness occupies the middle ground: a clinician who made a diagnosis or carried out treatment in the course of ordinary care, and who reports that work. The distinction from a pure witness of fact is thin in practice, but a professional witness may state a diagnosis they reached in the course of treatment (for example, "this is a fracture") without needing to be formally instructed as an expert, because the diagnosis arose from the clinical encounter itself. [2] [6]
An expert witness is instructed to provide opinion evidence beyond fact — interpretation, causation, mechanism, prognosis, and the weighing of differentials. The expert's opinion must lie within a recognised field of expertise, be based on a logical foundation, and be supported by the material. In some jurisdictions a single joint expert is instructed jointly by both parties to narrow the medical issues in dispute; the duty to the court is identical, but the procedural position differs. [2]
The three evidence roles compared
Epidemiology & Risk Factors
There is no incidence figure for "expert reports written," but the volume is substantial and growing. Child-protection proceedings, criminal trials of alleged perpetrators, and family-law disputes over residence and contact all draw on paediatric evidence, and the number of cases in which a clinician is asked for a report or called to testify has risen as the legal system has come to rely more heavily on specialised medical opinion. Horstman and colleagues' systematic scoping review documented that paediatricians across jurisdictions are called to give evidence in child-maltreatment cases with increasing frequency, and that the experience is widespread rather than confined to a subspecialty few. [4]
A parallel problem is the shortage of clinicians willing and able to act as expert witnesses. Oates and colleagues' position statement from the British Society of Paediatric Radiology identified a critical shortage of paediatric radiologists prepared to give expert evidence in suspected physical abuse cases — a gap that risks leaving courts without the radiological interpretation they need, or forcing a small group to carry an unsustainable load. The problem is not unique to radiology; child-protection paediatricians and forensic physicians face similar pressures. [10]
The legal outcomes of reported cases hinge substantially on the quality and availability of medical evidence. Hendrix and colleagues examined the legal outcomes of suspected maltreatment cases evaluated by a child-abuse paediatrician within a multidisciplinary team, finding that structured medical evaluation contributed materially to case resolution — whether through substantiation, prosecution, or the narrowing of disputed issues. Where the medical evidence is strong, coherent and well-presented, the legal system can act; where it is absent or equivocal, children are left less protected. [5]
The risk factors for a poor evidentiary outcome cluster around the clinician rather than the child: inexperience with report-writing and testimony, lack of preparation, working outside recognised expertise, and the emotional burden of testifying. Horstman's review found that the personal impact on paediatricians — stress, anxiety, moral distress, and reputational concern — is itself a barrier to participation, and may deter clinicians from engaging with the medico-legal process at all. [4]
Pathophysiology
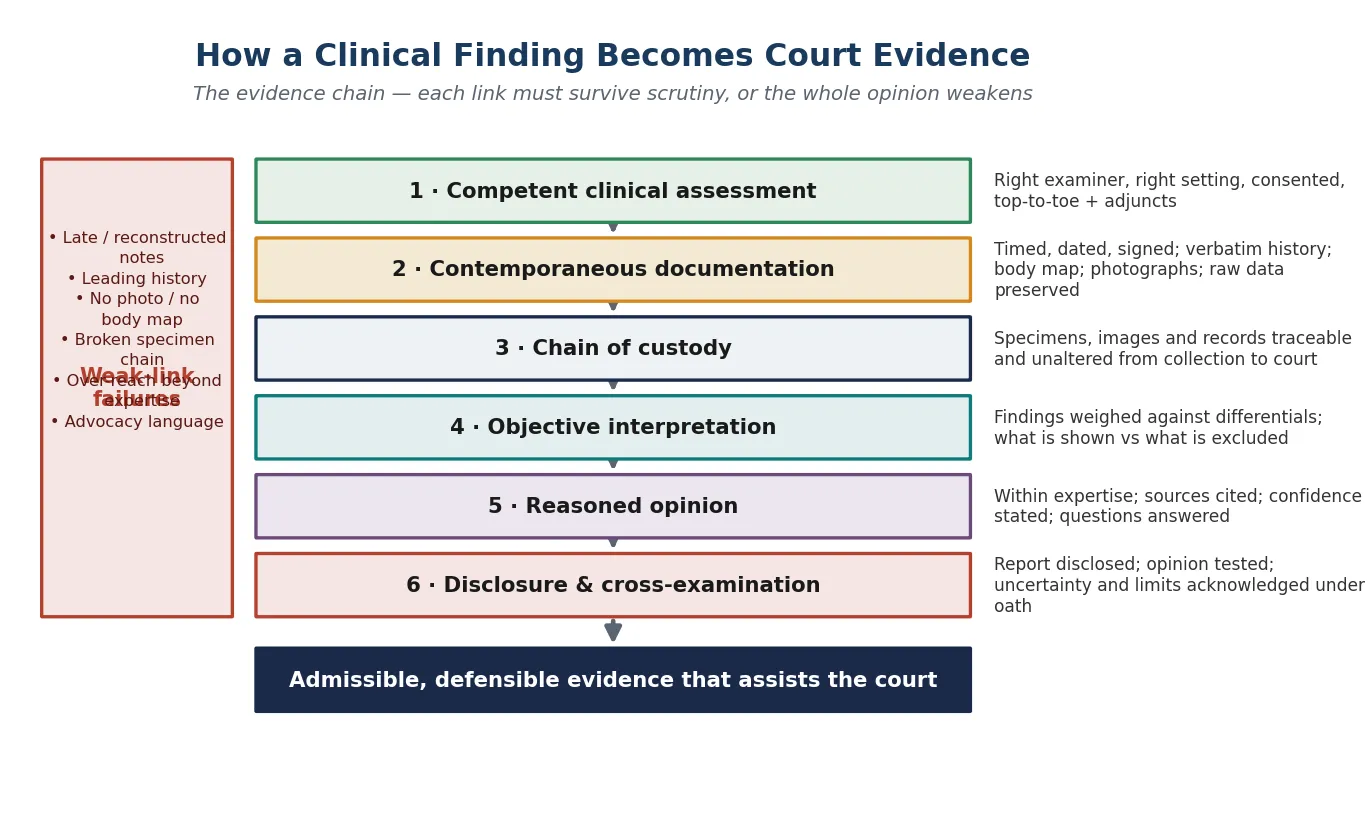
There is no enzyme for admissibility, but there is a mechanism: how a clinical finding at the bedside becomes evidence a court may rely upon. Understanding this chain explains why some opinions withstand cross-examination and others collapse under it. [1]
The chain begins with a competent clinical assessment — the right examiner, in the right setting, with consent obtained and the appropriate adjuncts (skeletal survey, neuroimaging, laboratory work). Everything downstream depends on the quality of this step, because an opinion cannot be stronger than the data it rests on. A rushed or incomplete examination produces findings that an opposing expert will expose, and a report built on them will not survive. [2]
The assessment is fixed in a contemporaneous record — timed, dated, signed notes, a verbatim history, a body map, photographs, and the raw imaging and laboratory data preserved. The contemporaneous record is the evidentiary anchor: it demonstrates what was found at the time, before any party's account could influence it, and it protects against the accusation that findings were reconstructed or embellished after the fact. A note written late, or back-dated, is a weak link that compromises the whole chain. [1]
Where specimens, images or records are collected for forensic purposes, a chain of custody preserves their integrity from collection to court. Each transfer is documented, so the court can be satisfied that the material examined is the material described, unaltered and unambiguous. A broken chain of custody can render otherwise compelling physical evidence inadmissible or substantially weakened. [1]
The clinician then forms an objective interpretation — what the findings show, what they exclude, and how they weigh against the differential. This step is where over-reach most often occurs: asserting that a finding "proves abuse" when it only supports abuse among several possibilities. Dias and colleagues showed that medical experts themselves struggle to define what level of certainty their words convey, which is why the disciplined weighing of differentials — stating both what is shown and what is excluded — is the safeguard against overstatement. [3]
The interpretation is delivered as a reasoned opinion in the report, within the clinician's expertise, with sources cited and confidence stated. And finally the opinion is tested through disclosure and cross-examination — the report is exchanged between parties, challenged, and the clinician must answer questions under oath, acknowledging uncertainty and the limits of the evidence. An opinion that has never been stress-tested may look robust on paper and fragment in the witness box. [1] [2]
Clinical Presentation
"Presentation" in this topic is not a symptom complex but the set of encounters in which a clinician is drawn into the evidentiary process. Recognising which encounter you are in tells you what is expected of you and how to prepare. [1]
The first encounter is the request for a report. You receive a letter of instruction — from a child-protection authority, a legal representative, or the court — asking you to prepare a statement or expert report. The instruction should set out the questions you are asked to address, the material provided, and the deadline. Your first task is to read it carefully and ask whether the questions fall within your expertise; if they do not, you decline or narrow the scope at the outset. [2]
The second encounter is the examination for the report, if one is required. In some cases you examine the child afresh; in others you rely on the records and imaging collected during the acute presentation. If you examine, you obtain consent, use a chaperone, and document contemporaneously — because this examination's record becomes the evidentiary substrate for your opinion. If you rely on prior records, you read them in full, identify gaps, and state explicitly that your opinion rests on material collected by others. [2]
The third encounter is the pre-meeting with legal counsel before testimony. Counsel may wish to discuss the case, clarify your opinion, and identify areas of likely challenge. This meeting is proper and expected — you are not being coached to say something you do not believe — but you must retain ownership of your opinion and refuse to adopt a framing that misrepresents it. Strouse and colleagues described this preparation as essential, and distinguished it from the improper pressure to alter an opinion to suit a party's case. [1]
The fourth encounter is giving oral evidence itself — examination-in-chief by the party who called you, cross-examination by the opposing party, and re-examination. The courtroom environment is adversarial and unfamiliar, and the experience is often stressful. Horstman's review documented the emotional and professional toll on paediatricians, including anxiety before testimony, distress during hostile cross-examination, and rumination afterward. Recognising this as a normal response to an abnormal environment is part of surviving it. [4]
The fifth encounter is the post-testimony debrief — returning to clinical work after giving evidence, often carrying the weight of the case and uncertainty about the outcome. Horstman's work and the broader literature suggest that structured debrief and peer support mitigate the lasting impact, and that institutions should treat the wellbeing of clinicians who testify as a legitimate concern rather than a private burden. [4]
Differential Diagnosis
When you are asked to give an opinion on causation, the central intellectual task is the differential — not as a list to recite, but as a disciplined weighing of what the findings show against what else could explain them. Courts and opposing experts live in the space between a conclusion and its alternatives. [8]
Distinguish a diagnosis of exclusion from a pattern diagnosis. Some inflicted-injury findings are diagnoses of exclusion — you can only conclude abuse once you have ruled out the alternatives, and the report must document that exclusion. Others are pattern diagnoses, where the combination of findings is itself so specific that it points to inflicted injury without requiring every alternative to be individually excluded. Conflating the two overstates the certainty of an exclusion-based conclusion or understates the strength of a pattern-based one. [8]
Separate the medical differential from the explanatory differential. The medical differential asks what disease or condition could produce the finding (a bleeding disorder, osteogenesis imperfecta, a metabolic bone disease). The explanatory differential asks what mechanism could account for the finding as observed (a fall, a seizure, a birth injury). A complete report addresses both, because the court is weighing not only whether the finding is organic but whether the account offered is consistent with it. [1] [8]
Weigh the mimic carefully. Brown framed the ethical core of the differential in child abuse: the harm of a misdiagnosis runs in both directions. Falsely labelling an accidental or disease-related finding as inflicted tears a family apart and may lead to wrongful prosecution or removal. Falsely dismissing inflicted injury as accidental returns a child to danger. The differential is not a pedantic exercise; it is the mechanism by which you protect against both harms, and the report must show the court that you have taken it seriously. [8]
Discriminate what you can exclude from what you cannot. A bleeding screen that is normal does not exclude a mild bleeding diathesis entirely; it lowers its probability. The report must state the residual uncertainty honestly rather than claiming an exclusion the test cannot deliver. Debelle and Oates argued that the child-protection system needs greater methodological rigour in how certainty is expressed, precisely because overstated exclusion misleads the court as much as overstated accusation. [9]
[1] [8] [9]Clinical & Bedside Assessment
The bedside assessment that underpins a later report is performed with the knowledge that it may be scrutinised line by line months later. That does not change what you do — it raises the standard of how you record it. [2]
Obtain consent for the examination and document it, including who consented and on what authority (parent, guardian, the child themselves if a competent minor, or the court). Use a chaperone and record their identity. If the child is examined under a court order or in circumstances where the usual consent framework is altered, state the legal basis for the examination in the note. [2]
Take a non-leading history and record the child's and carers' exact words in quotation marks. Note discrepancies between accounts and between the history and the injury, because these discrepancies are themselves findings the court may rely on. Do not conduct an investigative interview — that is the role of trained police or child-protection interviewers — but capture faithfully what is said in the clinical encounter. [1]
Perform a full top-to-toe unclothed examination and document findings with a body map and clinical photographs. Record injury type, location, size, age and pattern. State the developmental stage and whether the mechanism described is developmentally plausible. Preserve the raw imaging, laboratory results and any specimens according to chain-of-custody protocol where forensic examination is involved. [2]
Arrange the appropriate adjuncts — skeletal survey in the under-two (with a repeat at 11 to 14 days), neuroimaging if abusive head trauma is possible, and a targeted laboratory screen for the differential. These investigations are part of clinical care and belong in the medical record; their results strengthen or allay the concern and provide the substrate on which the report's opinion will rest. [2]
Consult the child-protection team and senior colleagues. A second opinion on injury interpretation is not a sign of uncertainty to be hidden — it is good practice that strengthens the assessment and the report. The multidisciplinary team evaluation that Hendrix and colleagues studied showed that structured, team-based assessment improves the coherence of the medical evidence that reaches the court. [5]
Investigations
The investigations that feed a report are the same ones that guide clinical care — but their selection, performance and reporting carry added weight because they may be re-examined by an opposing expert and tendered as exhibits. [2]
A skeletal survey remains the core investigation for suspected physical abuse in children under two years. It identifies occult fractures — particularly healing posterior rib fractures, classic metaphyseal lesions, and scapular, sternal or spinous process fractures — that are highly specific for inflicted injury. A repeat skeletal survey at 11 to 14 days captures fractures not visible acutely. The images must be of diagnostic quality and retained, because an opposing radiologist may reinterpret them. [2] [10]
Neuroimaging is indicated when abusive head trauma is suspected. CT head is the acute modality; MRI brain adds sensitivity for parenchymal injury, diffuse axonal injury and extra-axial collections. Ophthalmology assessment for retinal haemorrhages is part of the workup. The radiological interpretation of these studies is itself a field of expertise — Oates and colleagues' position statement stressed that courts require appropriately qualified paediatric radiologists to interpret and testify on these images, and that the shortage of such witnesses is a systemic risk. [10]
Laboratory investigations address the differential: a bleeding screen (coagulation studies, full blood count, von Willebrand panel) for bruising; bone health and metabolic markers for unexplained fractures; toxicology if ingestion is suspected. The report should state what was tested, what was normal, and what residual uncertainty remains — a normal screen lowers but does not always eliminate a differential diagnosis. [2]
A forensic examination for suspected sexual abuse should be performed by a clinician trained in forensic paediatric examination, within the evidence-gathering window, with consent and chain-of-custody protocol. Colposcopic photographs, swabs and clothing are collected and preserved; the examination serves both clinical (injury identification, infection screening, emergency contraception) and evidentiary purposes. [2]
Visual aids may strengthen the presentation of findings to the court. Barrera and colleagues demonstrated that three-dimensionally printed models of the rib cage in children with non-accidental injury served as effective visual aids, helping lay participants — judge, jury, counsel — grasp the location and pattern of fractures that are difficult to convey from two-dimensional images. Such aids do not change the opinion; they make the existing opinion more accessible. [11]
[2] [10] [11]Management — Resuscitation
In this topic, "resuscitation" is not an airway intervention but the immediate, time-critical work of preserving the evidentiary value of the encounter while you care for the child. The two run in parallel; neither waits for the other. [2]
Treat the acute injury first. A fractured femur, a burn, an intracranial bleed demands the same resuscitation and stabilisation as any trauma — the possibility of infliction does not change your immediate clinical priorities, and a child who is not stabilised cannot be examined, investigated or protected. [2]
Secure the contemporaneous record at the time of the acute encounter, because the note written during resuscitation and early assessment is the strongest evidence of what was found before any account could be revised. Record the history verbatim as it is given, note the time of presentation, and document the findings as they are discovered. The note made in the emergency department at 2 a.m. is worth more at trial than the polished summary written a week later. [1]
Preserve specimens, clothing and images. If forensic material is collected, begin the chain of custody immediately — who collected what, when, and where it was stored. Clothing removed from the child is bagged and labelled, not discarded. Imaging is archived and retrievable. These steps, taken in the acute moment, cannot be reconstructed later. [2]
Allocate roles so that clinical care and evidentiary preservation proceed together. One clinician leads resuscitation, another documents, a third supports the child and family. The child-protection team and social work are involved early. If a forensic examination is indicated and you are not the trained examiner, you arrange it rather than perform it inadequately. [2]
Communicate honestly with the family. Explain what you are doing and why, in terms that do not accuse but do not conceal. The family will learn of the report and the process; how you frame it in the acute encounter shapes their engagement with what follows. [1]
Management — Definitive & Stepwise
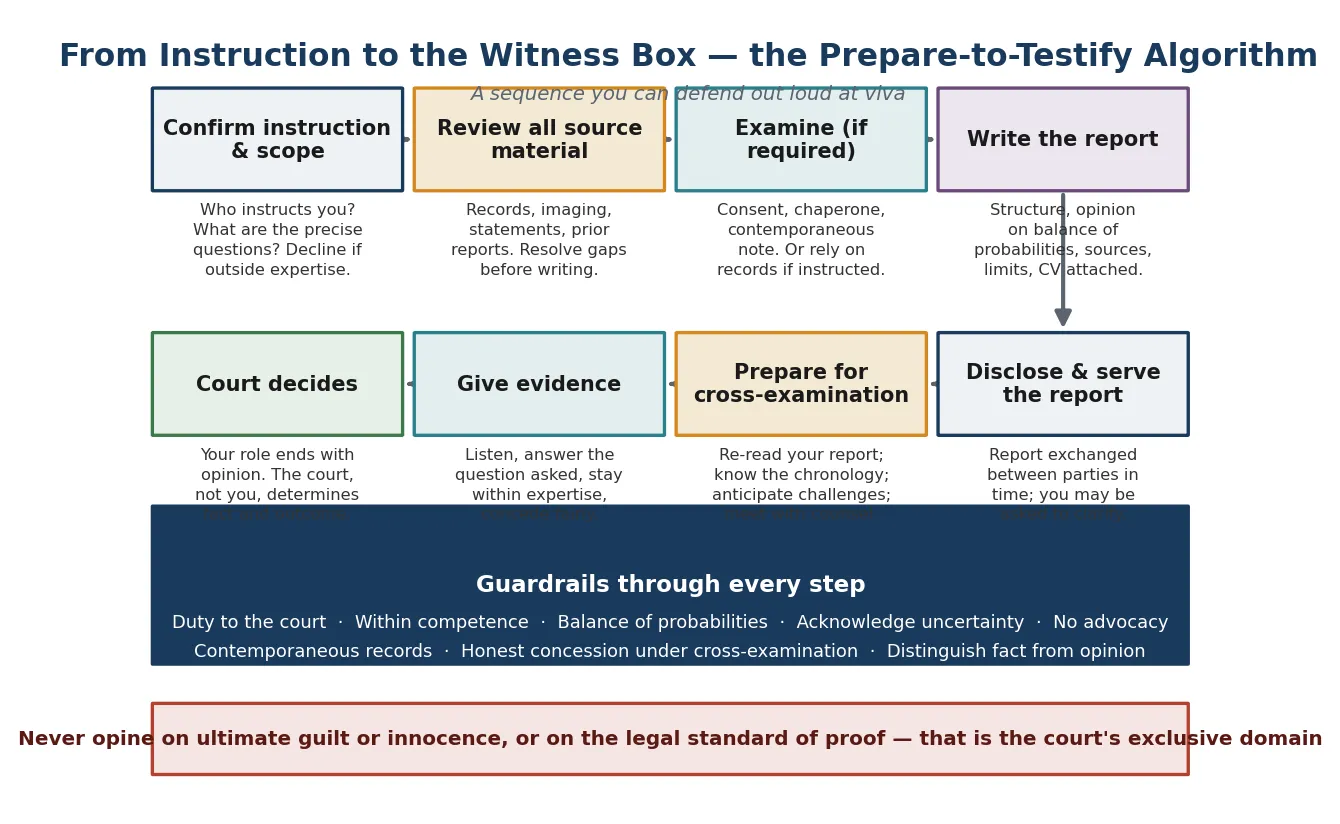
The definitive work is the report itself and the testimony that follows. Use a sequence you can defend out loud — from the letter of instruction to the witness box — anchored on the duty to the court and the limits of your expertise. [1] [2]
The prepare-to-testify algorithm
Confirm the instruction and scope — who instructs you, what are the precise questions, and do they fall within your expertise
Review all source material — medical records, imaging, prior reports, statements — and resolve gaps before writing
Examine the child if required — with consent, chaperone and contemporaneous note — or rely on prior records if instructed
Write the structured report — findings, differential, opinion on the balance of probabilities, sources cited, limits stated, CV attached
Disclose and serve the report in time — it is exchanged between parties and you may be asked to clarify
Prepare for cross-examination — re-read your report, know the chronology, anticipate challenges, meet with counsel
Give evidence — listen, answer the question asked, stay within expertise, concede fairly, do not advocate
Recognise that the court decides — your role ends with opinion; the court determines fact and outcome
Structure the report so a court can follow it. A defensible expert report carries a consistent architecture: the instruction (who asked, what questions), the material reviewed (records, imaging, examinations), the background and history, the findings, the differential and its weighing, the opinion with reasoning, the conclusion, and a statement of the limits and uncertainty. Attach your CV to establish your expertise. State the standard of proof at which your opinion is offered. [2]
State the opinion at the correct level of certainty. Dias and colleagues explored what clinicians mean when they say they are certain in court, and found disturbing variability — the same words carried different weights for different experts, and the phrase "reasonable medical certainty" itself lacked a stable shared meaning. The disciplined response is to express opinion in the terms the proceeding requires: in a civil or family matter, on the balance of probabilities (more likely than not); in a criminal matter, in language the court can map to its own standard. Never borrow a criminal standard ("beyond reasonable doubt") for a medical opinion you cannot support at that threshold. [3]
Acknowledge uncertainty and the limits of the evidence. A report that concedes what it cannot show is more persuasive than one that claims more than the data deliver, because the court and the opposing expert can see that you have been honest. Debelle and Oates argued that the child-protection system must move toward greater methodological rigour in how certainty is expressed — and that begins with the individual report refusing to overstate. [9]
Specific Subtypes & Scenarios
The abusive-head-trauma report and contested causation. Abusive head trauma is among the most heavily litigated diagnoses in child protection, and the expert report must navigate a genuinely contested evidence base. Tibballs and Bhatia examined the role of expert witness testimony in shaken-baby or abusive-head-injury cases and a recent case development, illustrating how the triad of subdural haemorrhage, retinal haemorrhage and encephalopathy — once treated as near-pathognomonic — has been scrutinised, and how courts weigh competing expert accounts of causation. The defensible report states what the findings show, acknowledges the debate where it exists, and offers a reasoned opinion without overstating the certainty the evidence can bear. [7]
The radiology expert report. Imaging interpretation in suspected abuse is a subspecialty expertise, and the report on a skeletal survey or neuroimaging study should come from, or be reviewed by, a paediatric radiologist with experience in inflicted injury. Oates and colleagues documented that the shortage of such witnesses threatens the quality of radiological evidence reaching the court. If you are not the radiologist, your report references the radiological opinion rather than independently re-interpreting images outside your field. [10]
The single joint expert in family proceedings. When both parties jointly instruct a single expert, the procedural aim is to narrow the medical dispute and avoid a battle of experts. Your duty is identical — to the court — but you must be scrupulous in addressing the questions both parties have framed, and in avoiding any drift toward the perspective of the party whose account is more sympathetic. The single joint expert's neutrality is under particular scrutiny. [2]
The treating clinician called as witness of fact. You cared for the child acutely and are now called to describe what you found. Your evidence is factual, and the temptation to drift into opinion must be resisted — if an opinion is needed, an expert is instructed separately. Prepare by reviewing your own contemporaneous notes, because you will be asked to confirm them, and any discrepancy between your testimony and your note will be probed. [1]
The report on a child with disabilities. Interpretation is harder when communication barriers, behavioural presentations and diagnostic overshadowing complicate the history and examination. The report must acknowledge these complicating factors explicitly rather than papering over them, and the differential must include the conditions associated with the child's disability that could mimic or mask injury. Over-attributing findings to the disability is as much an error as failing to consider it. [8]
The historical-abuse report. An adolescent or adult discloses abuse from years earlier, and you are asked to report. The physical evidence may have resolved, and the report rests on the history, any residual findings, and the consistency of the account with known patterns. The report must be honest about what can and cannot be concluded from a delayed presentation, and must not equate absence of physical evidence with absence of abuse. [2]
The clinician facing a challenge to expertise. Opposing counsel questions whether you have the qualifications to offer the opinion. Your CV, attached to the report, is your defence — but it must be accurate and current. If the challenge has merit, you concede; an opinion offered outside recognised expertise is inadmissible and damages your credibility on the opinions you are qualified to give. [2]
Complications & Pitfalls
- Advocating for a party rather than assisting the court — the single most damaging error, because it compromises the impartiality that is the expert's defining duty. [2] [6]
- Straying beyond recognised expertise — opining on radiology, neurology or forensic science without the qualifications, or on legal questions that are the court's domain. [2] [10]
- Overstating certainty — claiming exclusion a test cannot deliver, or treating a diagnosis of exclusion as a pattern diagnosis. [3] [9]
- Omitting the differential — a report that asserts a conclusion without weighing alternatives invites the accusation that the clinician did not consider them. [8]
- Late or reconstructed documentation — the contemporaneous record is the anchor; notes written after the fact, or back-dated, are fatally weak. [1]
- Failing to preserve the chain of custody — specimens, images and records that cannot be traced are vulnerable to challenge. [1]
- Misusing "reasonable medical certainty" — deploying a phrase whose meaning is jurisdiction-dependent without knowing what standard it conveys. [3]
- Undergoing cross-examination unprepared — not re-reading the report, not anticipating the chronology, not having met with counsel. [1] [4]
- Opining on ultimate guilt or innocence — the legal verdict is the court's exclusive province. [2]
- Neglecting the personal impact — carrying the stress of testimony without debrief or peer support, and allowing it to erode willingness to engage with the process. [4]
Prognosis & Disposition
For the child at the centre of the case, the quality of the medical evidence is a determinant of the legal outcome, and therefore of safety. Hendrix and colleagues showed that structured, multidisciplinary medical evaluation contributes materially to case resolution — and that when the medical evidence is coherent, well-documented and honestly presented, the system is better able to protect the child. A weak or overreaching report, by contrast, can mislead the court in either direction and leave a child unprotected or a family wrongly torn apart. [5]
For the clinician, the disposition after testimony is a return to clinical work carrying the emotional weight of the encounter. Horstman's scoping review established that the impacts on paediatricians — stress, anxiety, distress, reputational concern — are real and common, and that they can deter future participation. Structured debrief, peer support, and institutional recognition of the burden are the appropriate disposition, not silent endurance. [4]
The report itself has a life beyond the immediate case. It may be cited in subsequent proceedings, relied upon by other clinicians, or revisited if the matter returns to court. A well-written report is therefore an investment in the child's ongoing protection and in the integrity of the record; a poorly written one is a liability that persists. [1]
Follow-up includes the clinician's own professional development — reflecting on what the testimony revealed about the strengths and weaknesses of the report, and using it to improve the next one. The Helfer Society's ethical-testimony guidelines frame giving evidence as a learnable clinical skill, honed by experience and reflection, not an innate talent. [2]
Special Populations
Pre-mobile infants. The interpretation of injuries in non-ambulant infants carries particular evidentiary weight because the differential of accidental injury is narrow, and a single sentinel finding may anchor the entire report. The report must document the developmental stage explicitly and address whether the described mechanism is developmentally plausible. [2]
Children with disabilities. Communication barriers, behavioural presentations and co-morbid conditions complicate both the examination and the differential. The report must acknowledge these factors, involve carers who know the child's baseline, and avoid both over-attributing findings to the disability and failing to consider disability-related mimics. [8]
Adolescents. When an adolescent is the subject of the report, their own account and emerging autonomy carry weight, and the report may need to address consent, confidentiality and the mature-minor framework alongside the clinical findings. A historical disclosure requires honest handling of what physical evidence can and cannot show after delay. [2]
Indigenous and migrant families. Cultural context, language and prior experience with statutory systems shape both the clinical encounter and how the report is received. Use professional interpreters, document cultural factors where relevant, and ensure the report does not encode assumptions that would mislead a court unfamiliar with the family's context. [6]
Children in out-of-home care. These children may be the subject of reports concerning current or historical maltreatment across multiple placements. The report must establish the timeframe of the findings relative to the placements and avoid attributing injuries to a period or a carer without the evidence to support it. [5]
The clinician themselves. The paediatrician who gives evidence is a population at risk of occupational stress and deserves the same duty of care from their institution that they extend to the child. Horstman's work positions clinician wellbeing as a legitimate concern of the medico-legal system, not a private irrelevance. [4]
Evidence, Guidelines & Regional Differences
The foundational comparative and ethical literature frames the expert's role across jurisdictions. Skellern's 2008 analysis of medical experts and the law set out the clinician's duties — to the child, the court and the profession — and remains a touchstone for how paediatricians should understand their evidentiary function. [6]
The Helfer Society guidelines on ethical testimony, published by Miller and colleagues in 2020, codified the principles that should govern expert evidence in suspected child maltreatment: honesty, objectivity, staying within expertise, acknowledging uncertainty, and the overriding duty to the court. They are the most influential statement of professional standards for paediatric expert testimony and the reference examiners expect a candidate to know. [2]
Strouse and colleagues' 2021 paper on preparing for court testimony translated those principles into practical guidance — how to review material, structure the report, meet with counsel and survive cross-examination. Read alongside the Helfer guidelines, it gives the clinician a complete preparation framework. [1]
The certainty problem was dissected by Dias and colleagues, who showed empirically that "reasonable medical certainty" lacks a stable meaning among medical experts — a finding with direct implications for how reports should express opinion. Debelle and Oates extended the argument, calling for greater methodological rigour in how the child-protection system handles certainty. Together these papers establish that the language of certainty is itself a clinical skill the report-writer must master. [3] [9]
The systemic and personal dimensions were addressed by Horstman and colleagues' systematic scoping review of the impacts on paediatricians who testify, and by Oates and colleagues' position statement on the shortage of radiology expert witnesses. These papers situate expert evidence within the real constraints of the workforce that produces it. [4] [10]
On contested evidence, Tibballs and Bhatia's analysis of expert testimony in abusive head trauma illustrates how the courts weigh competing expert accounts, and Brown's essay on the harm of misdiagnosis frames the ethical stakes of the differential. Hendrix and colleagues provide the outcome data linking structured multidisciplinary evaluation to legal resolution, and Barrera and colleagues demonstrate how visual aids can make expert evidence more accessible to the court. [5] [7] [8] [11]
Australian courts apply a harmonised expert witness code of conduct, articulated in Federal Court and state court practice notes and derived from the principles in the Ikarian Reefer case. The code requires the expert to acknowledge the overriding duty to the court, to state opinion within expertise, to identify the factual basis and reasoning, and to address the questions in dispute. A report that does not comply with the code may be ruled inadmissible or carry little weight. In Aotearoa New Zealand, the High Court Rules set out parallel duties for expert witnesses, including the requirement to assist the court impartially and to address the code of conduct. State the principle — the expert's duty runs to the court, governed by a code of conduct with which the report must comply — and verify the current practice note and rules for the specific court. Do not invent a rule number or citation you cannot verify. [6]
Exam Pearls
EVIDENCE
References
- [1]Strouse PJ, Moreno JA, Dias MS, Narang SK Preparing for court testimony. Pediatric Radiology, 2021.PMID 33999250
- [2]Miller AJ, Narang S, Scribano P, Greeley C, Berkowitz C, Leventhal JM, Frasier L, Lindberg DM Ethical Testimony in Cases of Suspected Child Maltreatment: The Ray E. Helfer Society Guidelines. Academic Pediatrics, 2020.PMID 32068125
- [3]Dias MS, Boehmer S, Johnston-Walsh L, Levi BH Defining 'reasonable medical certainty' in court: What does it mean to medical experts in child abuse cases? Child Abuse & Neglect, 2015.PMID 26589362
- [4]Horstman A, Smith JAS, Bassed RB, Bugeja L The impacts on paediatricians testifying in cases of child maltreatment: A systematic scoping review. Child Abuse & Neglect, 2025.PMID 40073689
- [5]Hendrix AD, Conway LK, Baxter MA Legal Outcomes of Suspected Maltreatment Cases Evaluated by a Child Abuse Pediatrician as Part of a Multidisciplinary Team Investigation. Journal of Forensic Sciences, 2020.PMID 32501610
- [6]Skellern C Medical experts and the law: Safeguarding children, the public and the profession. Journal of Paediatrics and Child Health, 2008.PMID 19166533
- [7]Tibballs J, Bhatia N Shaken Baby Syndrome/Abusive Head Injury: The Role of Expert Witness Testimony and a Recent Case Development. Journal of Bioethical Inquiry, 2025.PMID 40392472
- [8]Brown SD Ethical challenges in child abuse: what is the harm of a misdiagnosis? Pediatric Radiology, 2021.PMID 33999247
- [9]Debelle G, Oates A Making the case for greater certainty in child protection. Archives of Disease in Childhood, 2022.PMID 35379606
- [10]Oates A, Halliday K, Offiah AC, Landes C, Stoodley N, Jeanes A, Johnson K, Chapman S, Stivaros SM, Fairhurst J, Watt A, Paddock M, Giles K, McHugh K, Arthurs OJ Shortage of paediatric radiologists acting as an expert witness: position statement from the British Society of Paediatric Radiology (BSPR) National Working Group on Imaging in Suspected Physical Abuse (SPA). Clinical Radiology, 2019.PMID 31126587
- [11]Barrera CA, Silvestro E, Calle-Toro JS, Scribano PV, Wood JN, Henry MK, Andronikou S Three-dimensional printed models of the rib cage in children with non-accidental injury as an effective visual-aid tool. Pediatric Radiology, 2019.PMID 30877337