Paeds · child-safety-and-social-paediatrics
Female genital mutilation or cutting
Also known as FGM · Female genital cutting · Female circumcision · Infibulation · WHO Type I–IV FGM/C
A fellowship approach to recognising and managing female genital mutilation or cutting in children and adolescents: understanding the WHO Type I–IV classification and why every type performed on a minor is child abuse, identifying the at-risk girl through history and community risk, conducting a trauma-informed and culturally safe examination, managing the acute and lifelong complications from urinary retention to obstetric fistula, arranging deinfibulation and reconstructive care, and fulfilling the mandatory-reporting and safeguarding duties that fall on every paediatrician.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old girl is brought to your clinic with dysuria and recurrent urinary tract infections. Her family recently migrated from a country in the Horn of Africa. On examination you find that her external genitalia show scarring and a narrowed vaginal opening consistent with Type III infibulation. The mother is present, watchful, and speaks limited English. Your first responsibility in this moment is not to judge the mother, who may herself be a survivor of cutting. Your responsibility is to recognise what you are seeing, safeguard the child, investigate for complications, and begin the safeguarding and reporting duties that follow. [8] [1]
Female genital mutilation or cutting comprises all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs, for non-medical reasons. The World Health Organization, UNICEF, and UNFPA jointly define it as a violation of the human rights of girls and women, reflecting deep-rooted inequality between the sexes and constituting an extreme form of discrimination. When performed on a child — as the majority of cases are — it is child abuse under every paediatric safeguarding framework in the world. [8]
The term "mutilation" versus "cutting" deserves a moment. The WHO and UN agencies adopted "FGM" to signal the gravity of the practice, while many community-engagement programmes use "female genital cutting" or "FGC" to reduce stigma and keep dialogue open with practising communities. Both terms describe the same act. What matters clinically is that the practice has no health benefit, causes immediate and lifelong harm, and is never justified by culture, religion, or consent of the family. [8]
Classification
The WHO classification is the single most examinable framework in this topic, because it predicts complications and drives management decisions. The classification runs from Type I through Type IV, with severity and complication burden rising sharply at Type III. Every fellowship candidate should be able to name each type, describe what tissue is removed, and identify Type III as the most severe form. [8] [1]
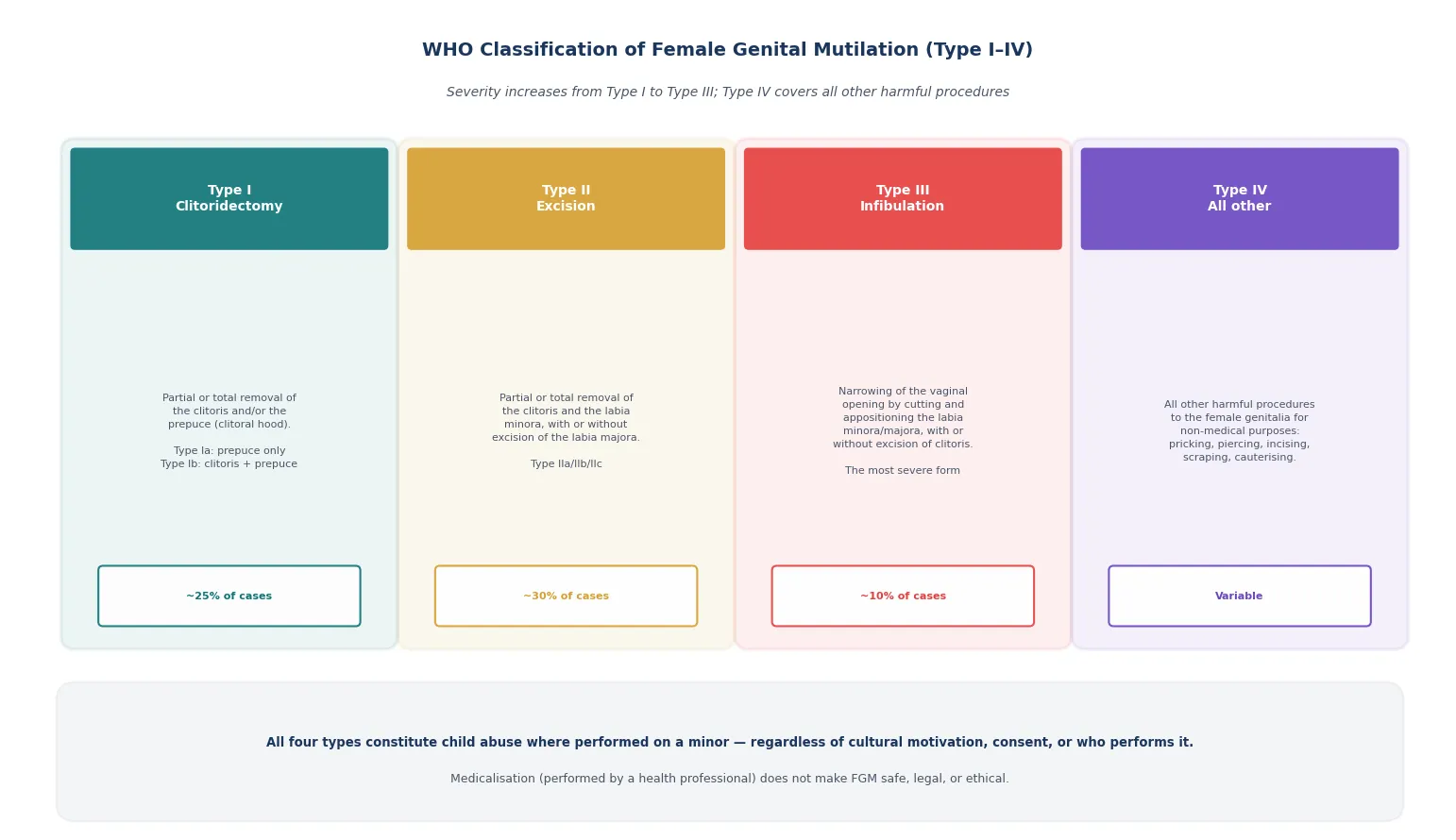
Type I
Clitoridectomy
- Partial or total removal of the clitoris and or the prepuce
- Type Ia: prepuce only
- Type Ib: clitoris and prepuce
- Approximately one quarter of cases worldwide
Type II
Excision
- Partial or total removal of the clitoris and labia minora
- With or without excision of the labia majora
- Subtypes IIa, IIb, IIc by tissue involved
- Approximately one third of cases worldwide
Type III
Infibulation
- Narrowing of the vaginal opening by cutting and appositioning the labia
- With or without excision of the clitoris
- The most severe form — highest complication burden
- Approximately one in ten cases, concentrated in the Horn of Africa
Type IV
All other
- All other harmful procedures for non-medical purposes
- Pricking, piercing, incising, scraping, cauterising
- Variable prevalence; includes symbolic nicking
- Still child abuse when performed on a minor
Medicalisation — the performance of FGM by a health-care provider — does not make any type safe, legal, or ethical. The WHO has taken a clear position that medicalised FGM must be actively opposed, because a medical provider performing the act legitimises it within the community and breaches every professional and ethical duty. [9]
Epidemiology & Risk Factors
Over 200 million girls and women alive today have undergone FGM, concentrated in a band of countries across Africa, the Middle East, and parts of Asia. A systematic review and meta-analysis of African prevalence data confirms that cutting remains common in many practising countries, with rates above 80 per cent in Somalia, Guinea, Djibouti, and Egypt, though secular declines are now visible in several nations where communities are abandoning the practice. [6]
In ANZ, the UK, Canada, and other countries with migrant communities from practising regions, FGM is encountered in two settings. The first is the girl who has already been cut overseas and presents to a clinician with complications or is identified on routine examination. The second — and the one where the paediatrician has the greatest power to prevent harm — is the girl at imminent risk of being cut, often during a trip to the family's country of origin. Identifying this girl before the trip is the single highest-yield preventive act. [8] [9]
The risk factors are community and family based rather than individual. A girl is at elevated risk if she belongs to a community that practises FGM, if a mother or sister has been cut, if the family is planning travel to a high-prevalence country, or if an older female relative is visiting from overseas. These factors let you screen proactively rather than waiting for a disclosure that may never come, because most cut girls do not disclose — they are cut too young to remember, or they are socialised not to speak about it. [8]
Pathophysiology
The external female genitalia are richly innervated and vascularised tissue, which is why FGM produces immediate severe pain and bleeding and why the long-term complications cluster around nerve injury, scar formation, and anatomical distortion. Understanding this tissue-level damage is what connects the WHO classification to the complications you will manage. [1] [5]
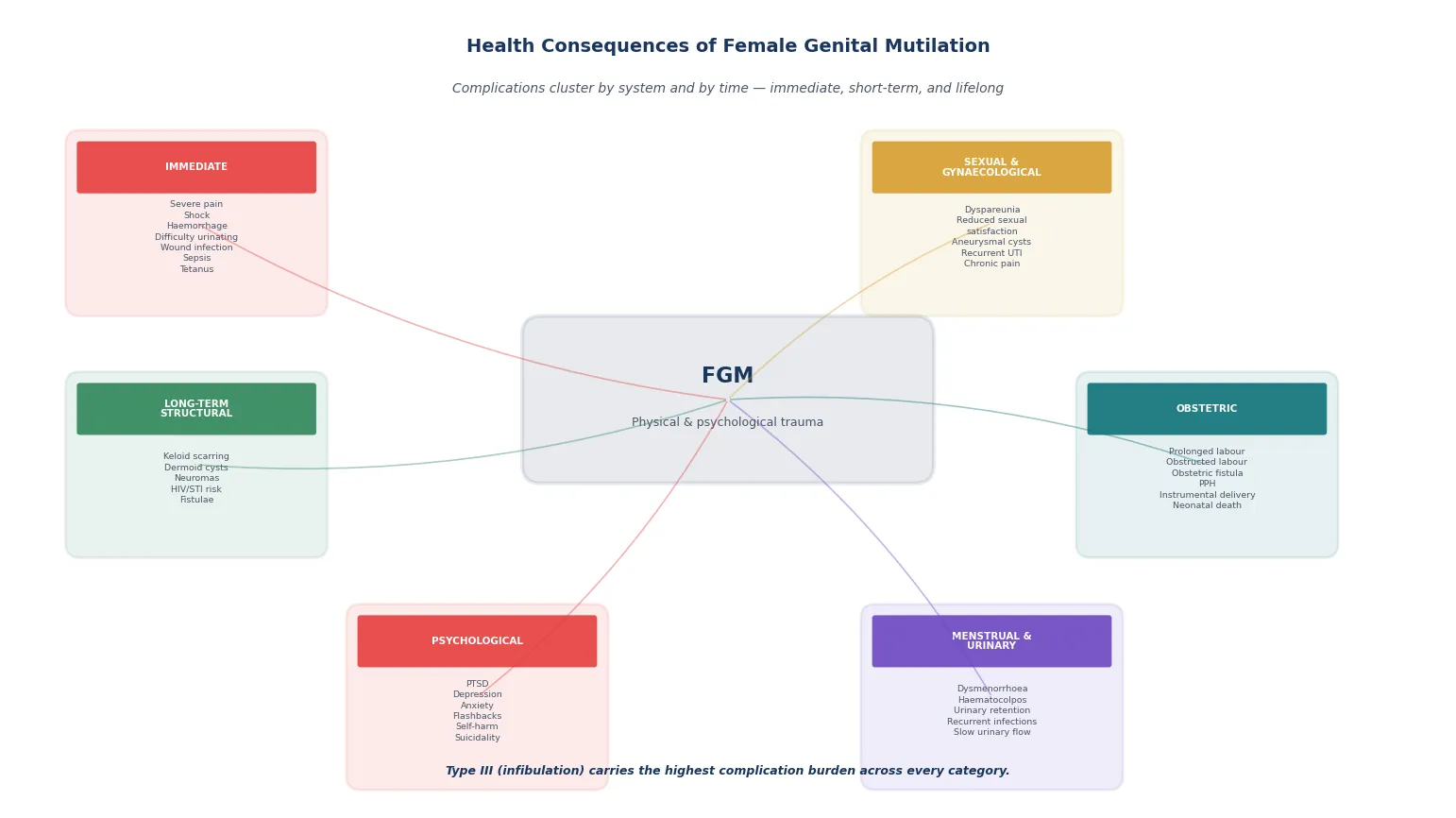
The immediate injury is mechanical. Cutting the clitoris, labia, or vaginal opening severs arteries, nerves, and mucosa. In Type III infibulation, the raw labial edges are apposed and bound together, leaving only a tiny opening for urine and menstrual blood. The wound heals by secondary intention because the raw surfaces are held together without suturing technique or sterility in traditional settings, producing dense scar tissue that narrows the introitus permanently. This scar is the structural basis for nearly every long-term complication — dyspareunia, haematocolpos, obstructed labour, and recurrent infection. [1] [10]
The long-term damage extends beyond the genitalia. Neuromas form in transected nerve endings and drive chronic pain. Keloid scarring and dermoid cysts arise from epithelial debris buried in the wound. The narrowed introitus causes urinary stasis, recurrent urinary tract infection, and difficulty passing menstrual blood, which in severe cases leads to haematocolpos — a distended vagina filled with retained menstrual blood that can present as an abdominal mass in an adolescent. Sexual function is impaired through both the physical narrowing and the nerve damage, and a meta-analysis confirms significantly reduced sexual function scores and increased dyspareunia across cut women. [5] [1]
The psychological injury is independent of the physical damage. A systematic review found that women who have undergone FGM have higher rates of post-traumatic stress disorder, depression, anxiety, and somatic complaints than uncut women from the same communities, even after adjusting for other adversities. The cutting event itself — the pain, the restraint, the betrayal by trusted adults — is a traumatic experience that shapes mental health for decades. [3]
Clinical Presentation
A cut child rarely presents with a clean disclosure. The more common scenario is the girl who presents with a complication — dysuria, recurrent infections, abdominal pain, or behavioural change — and the cutting is found on examination, inferred from community risk, or disclosed tentatively by the child or a sibling. Recognising these presentations is what turns the paediatrician from a passive observer into a safeguarding clinician. [8] [1]
Acute presentation
Within days of cutting
- Severe pain, bleeding, or shock
- Acute urinary retention — the narrowed opening blocks flow
- Local or systemic infection — cellulitis, sepsis, tetanus
- Behavioural change — withdrawal, regression, fear of urination
Late presentation
Months to years later
- Recurrent UTI or dysuria from chronic stasis
- Dysmenorrhoea or haematocolpos in adolescence
- Dyspareunia or apareunia in sexually active women
- Identified incidentally on routine or antenatal examination
Risk presentation
Before cutting occurs
- Planned overseas trip to a practising country
- Older female relative visiting from overseas
- Mother or sister already cut
- Family discussion of 'becoming a woman' or a ceremony
The adolescent who presents in pregnancy deserves particular attention, because her FGM may first be identified at the antenatal booking visit. This is a critical opportunity to plan antenatal deinfibulation, prepare for the obstetric risks of prolonged and obstructed labour, and arrange the multidisciplinary care that reduces perinatal harm. A cohort study of obstetric outcomes found that women with FGM, particularly Type III, have significantly higher rates of instrumental delivery, postpartum haemorrhage, extended hospital stay, and adverse neonatal outcomes compared with uncut women. [2] [1]
The girl at imminent risk presents not with symptoms but with circumstance. A family from a practising community planning an extended trip overseas, or a visit from a grandmother who traditionally performs the cutting, is the presentation the paediatrician must learn to identify through sensitive, routine inquiry. This is primary prevention at the bedside — the act that stops the harm before it happens. [9] [8]
Differential Diagnosis
When a girl has a genital finding that could represent FGM, the task is to distinguish cutting from other causes of genital scarring, narrowing, or anatomical change. The discriminating features are the pattern and location of the scarring, the community context, and the history. Most of the time the finding is unambiguous once you think of FGM; the pitfall is not thinking of it at all. [8] [1]
Lichen sclerosus
Mimic
- Pale atrophic 'figure-of-eight' plaques around vulva and perianal area
- Pruritus, fissuring, bruising, bleeding
- Prepubertal girls; scarring can narrow the introitus
- Responds to topical corticosteroid; biopsy confirms if uncertain
Straddle injury
Accidental
- External, anterior, asymmetric injury to labia or perineum
- Clear history of fall onto a hard edge
- Does not produce the symmetrical scarring of Type III
- Heals without the dense appositional scar
Congenital variant
Anatomical
- Imperforate hymen or labial adhesions present from birth
- Labial adhesions are common in prepubertal girls
- No scarring or tissue loss
- Oestrogen cream resolves labial adhesions in most cases
Vulvovaginitis
Common mimic
- Discharge, erythema, dysuria without structural change
- Poor hygiene, irritants, pinworms, candidiasis
- No scarring or narrowing of the introitus
- Treat the underlying cause
Two principles resolve most of the differential. First, the pattern of tissue loss discriminates: FGM produces symmetrical, deliberate removal or apposition of tissue in a pattern that matches the WHO classification, whereas accidental injury and inflammatory conditions produce asymmetric, irregular changes. Second, the community context is not incidental: a girl from a practising community with genital scarring has FGM until proven otherwise, and a girl from a non-practising community with similar findings warrants investigation for lichen sclerosus, trauma, or other causes. [8] [1]
Clinical & Bedside Assessment
The assessment is trauma-informed, culturally safe, and child-paced from the moment the child arrives. The setting is quiet and private. The examiner is competent and — wherever possible — female, because many cut girls and their families have strong preferences about who examines the genital area. A chaperone is always present. An interpreter is used when needed, but never a family member, because the safeguarding implications make family-member interpretation unsafe. [8] [4]
The structured assessment, in order
Safety first — address acute complications: pain, urinary retention, bleeding, infection
Sensitive history with the child alone where age-appropriate, then with the family
Establish community risk factors, travel history, and family cutting status
General examination including growth, skin, and signs of other maltreatment
Genital examination by a competent examiner with chaperone — classify the WHO type
Photo-documentation for peer review with explicit consent
Investigations guided by complications: urinalysis, STI screen if indicated, ultrasound for haematocolpos
Safeguarding response: mandatory report, safety plan, and multi-agency referral before the child leaves
The history must cover the cutting event itself when the child is old enough to recall it — the age, the setting, who performed it, and whether there were complications afterwards. Equally important is the family history: has the mother been cut, have older sisters been cut, and is there a plan for younger siblings? These questions, asked without judgement and with cultural humility, are how you identify the at-risk sibling and prevent the next cutting. [9] [8]
The genital examination classifies the WHO type and documents the complications. Look for the pattern of tissue loss, the presence and size of any scar, the patency of the vaginal opening, and signs of acute or chronic infection. In Type III, the labia majora are fused, leaving a small opening that may be too small for a finger or a speculum. Photo-documentation with colposcopy provides a record for peer review and reduces the need for repeat examinations, which re-traumatise the child. [10] [1]
In Australia, FGM is a criminal offence in all states and territories, with penalties including imprisonment. Mandatory reporting of a child at risk of or who has undergone FGM applies to medical practitioners. In Aotearoa New Zealand, FGM is prohibited under the Crimes Act, and the Children's Act requires reporting of any child at risk of harm. Specialist FGM clinics operate in major centres, providing deinfibulation, counselling, and community engagement. [8]
Investigations
Investigations in a girl with known or suspected FGM are driven by the complications she presents with, not by a blanket protocol. The girl who is acutely unwell after recent cutting needs a septic workup, urinalysis, and a screen for tetanus and blood-borne viruses. The girl who is well and identified electively needs a targeted assessment of urinary, gynaecological, and psychological health. [1] [8]
Acute cutting
Recent procedure
- Urinalysis and urine culture for infection
- Full blood count and inflammatory markers if sepsis suspected
- Tetanus status assessment — tetanus prophylaxis if contaminated
- HIV, hepatitis B and C baseline if instrument-sharing suspected
Chronic complications
Established FGM
- Urinalysis for recurrent UTI and stasis
- Pelvic ultrasound for suspected haematocolpos or cysts
- STI screening if sexually active or post-pubertal
- Mental-health screening — PHQ-9, GAD-7, or PTSD checklist
Pregnancy
Antenatal
- Classify the WHO type at booking
- Plan antenatal deinfibulation timing
- Obstetric ultrasound for fetal and placental assessment
- Multidisciplinary review with obstetrics and midwifery
The key decision in the acutely presenting girl is whether she has a complication that needs urgent intervention. Urinary retention from the narrowed opening of Type III may require catheterisation or even an episiotomy-like incision to relieve the obstruction. Sepsis from wound infection is a life-threatening complication that needs intravenous antibiotics and surgical debridement. Haemorrhage from an artery severed at cutting can be fatal and may require urgent surgical ligation. [1]
In the girl identified electively, a pelvic ultrasound is the single most useful investigation, because it can detect haematocolpos, dermoid cysts, and other structural complications without another genital examination. Mental-health screening is equally important, because the psychological burden is often the largest unaddressed harm and the one most amenable to intervention. [3] [8]
Management — Resuscitation
The first question in the acute presentation is whether the child is medically safe now. A girl who presents within days of cutting may have severe pain, haemorrhage, urinary retention, or sepsis, any of which can be life-threatening. Resuscitation follows the standard paediatric ABCDE approach, with early analgesia and senior surgical or gynaecology involvement for significant bleeding or urinary obstruction. [1]
Pain control is paramount and is often undertreated. The cutting itself causes severe pain, and the examination and any procedures add to it. Adequate analgesia — including opiates where needed — is part of basic humane care, and it also makes the examination and any necessary intervention possible without further traumatising the child. [1]
Wound infection and sepsis require intravenous antibiotics covering skin and genital flora, with tetanus prophylaxis if the cutting was performed with an unsterile instrument. Blood-borne virus transmission is a risk if instruments were shared, and baseline serology for HIV, hepatitis B and hepatitis C should be sent with follow-up serology at the appropriate intervals, because seroconversion takes weeks to months. [1] [8]
Management — Definitive & Stepwise
Definitive management runs on two parallel tracks: the clinical management of the physical and psychological complications, and the safeguarding and reporting response. Both tracks must run simultaneously, because treating the child without reporting leaves the siblings at risk and fails the legal duty, while reporting without treating abandons the child to preventable complications. [8] [9]
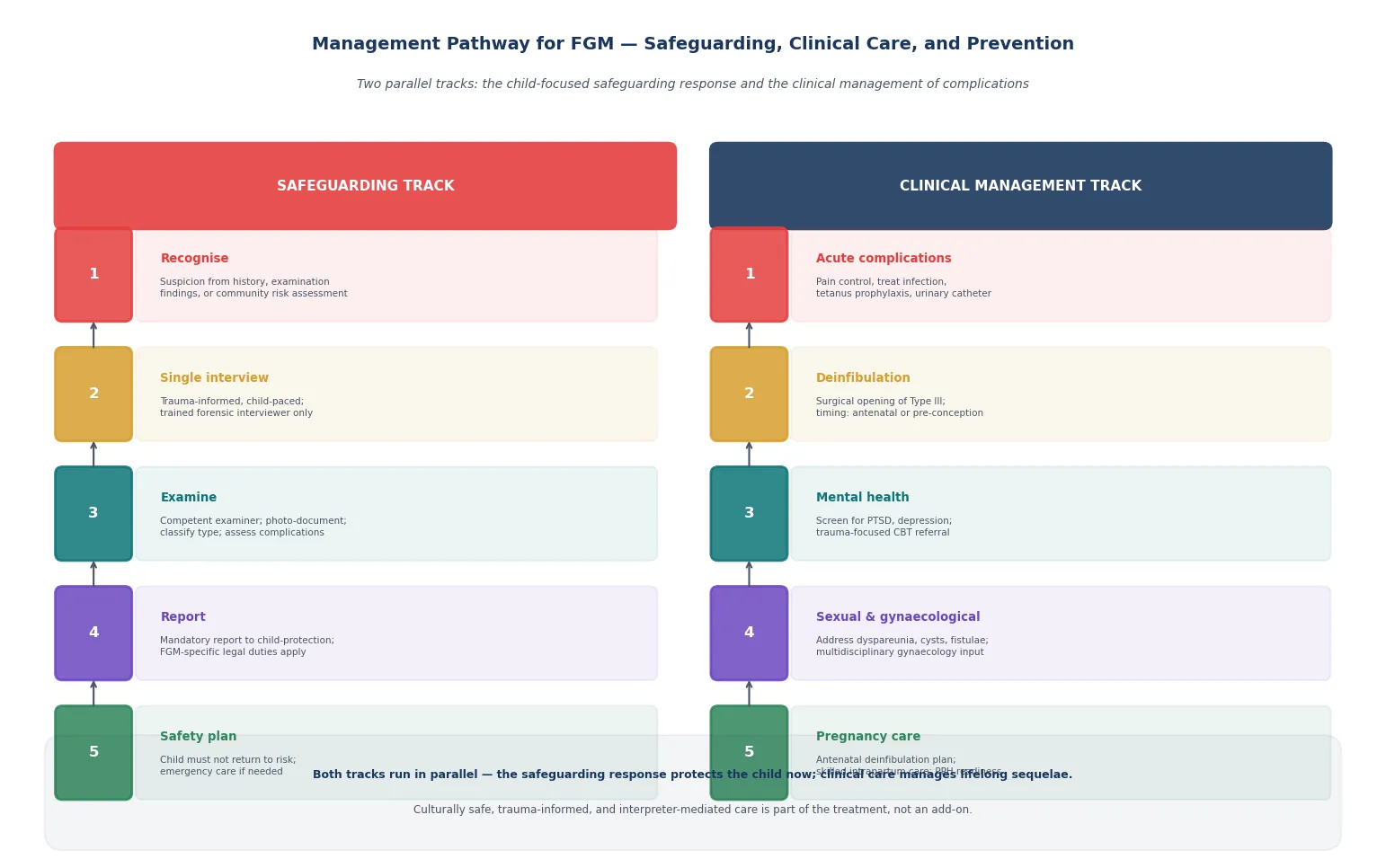
Deinfibulation is the definitive surgical procedure for Type III, in which the scar tissue is opened to restore a functional vaginal opening. The timing is critical. A systematic review of deinfibulation counselling found that antenatal deinfibulation — performed in the second trimester — improves obstetric outcomes and reduces the need for intrapartum cutting, while pre-conception deinfibulation allows the woman to heal before pregnancy and addresses sexual and menstrual complications. Deinfibulation should be offered to every woman with Type III, with counselling that addresses her fears, her partner's role, and the cultural meaning of the procedure for her. [4] [10]
Reconstructive surgery goes beyond deinfibulation to restore clitoral anatomy and function. A multidisciplinary approach — combining the surgical reconstruction with psychological support, physiotherapy, and sexual counselling — produces the best outcomes. Restaino and colleagues describe a model in which the reconstructive surgeon, the psychologist, and the sex therapist work as a team, addressing the anatomical, emotional, and sexual dimensions of the harm together. This is the standard of care for the woman seeking restoration, not merely an opening of the scar. [7]
Mental-health care is not optional. The systematic review evidence links FGM to elevated rates of PTSD, depression, and anxiety, and these conditions are treatable. Trauma-focused cognitive behavioural therapy has the strongest evidence for PTSD, and early referral to a psychologist or psychiatrist with experience in FGM and trauma can change the long-term trajectory. Screening every identified girl or woman for mental-health symptoms should be routine, because the psychological harm is often invisible and untreated. [3]
Safeguarding and mandatory reporting close the definitive bundle. FGM performed on a child triggers mandatory reporting in ANZ, the UK, and most jurisdictions. The report goes to child-protection services, and where a child is at imminent risk of being cut — for example, a planned trip overseas — an emergency protection order or its equivalent may be needed. The paediatrician's role is to make the report, agree a multi-agency safety plan, and ensure that every sibling in the family is screened, because cutting is familial. [9] [8]
Pregnancy care for the woman with FGM requires a planned, multidisciplinary approach. Classify the type at booking, offer antenatal deinfibulation for Type III, prepare for the obstetric risks of prolonged labour and postpartum haemorrhage, and ensure a skilled birth attendant is present. The obstetric evidence shows that planned antenatal deinfibulation significantly reduces intrapartum complications compared with leaving the infibulation intact or performing a reactive intrapartum cut. [2] [4]
Specific Subtypes & Scenarios
The at-risk girl before a trip overseas is the highest-yield scenario for prevention. A family from a practising community planning an extended trip to their country of origin, with a daughter who has not yet been cut, is the setting where a paediatrician can prevent lifelong harm. The response is a sensitive conversation about the legal and health consequences of FGM, a referral to community engagement services, and — if there is reasonable belief the girl will be cut — a safeguarding referral and potentially an emergency protection order or FGM protection order. [9] [8]
The pregnant adolescent with Type III infibulation is the scenario most likely to appear as a long-case or OSCE stem. The candidate must plan antenatal deinfibulation, prepare for obstetric complications, arrange mental-health support, and address the safeguarding implications for any daughters she may have in future. The multi-agency plan is essential, because her care spans obstetrics, gynaecology, mental health, and safeguarding. [2] [4]
The sibling of an identified girl is easily missed and must not be. If one girl in a family has been cut, every sister is at risk, and the paediatrician must screen each one, document the findings, and include them in the safeguarding plan. This is the familial nature of FGM — it travels through families, and missing the siblings is failing them. [8] [9]
The non-verbal or disabled girl carries higher baseline risk and cannot disclose. The threshold to examine is lower, not higher, because her inability to report means her protection depends entirely on the clinician's vigilance. Behavioural change — distress on urination, withdrawal, or regression — may be the only signal, and a competent genital examination is warranted on a lower threshold than for a neurotypical child. [8]
The girl identified in a non-acute setting — at a routine health check, an immigration medical, or a school examination — is the scenario where the paediatrician's index of suspicion matters most. The cutting may have happened years ago, the complications may be silent, and the opportunity to intervene depends entirely on recognising what the findings mean and asking the right questions. [8] [1]
Complications & Pitfalls
The most dangerous pitfall is failing to recognise FGM when it is in front of you. A girl from a practising community with recurrent UTI, dysmenorrhoea, or behavioural change may have her symptoms attributed to common causes without anyone examining the genitalia or asking about cutting. The result is a missed diagnosis, untreated complications, and unprotected siblings. The defence against this error is simple: examine the genitalia and think of FGM whenever a girl from a practising community presents with relevant symptoms. [8] [1]
Recognition failure
Most dangerous
- Not examining the genitalia of an at-risk girl
- Attributing symptoms to common causes without considering FGM
- Missing the diagnosis and the safeguarding opportunity
- Screen proactively in at-risk communities
Safeguarding deferral
Cultural error
- Deferring reporting out of misplaced cultural sensitivity
- Accepting the practice as a cultural variant
- Failing to protect siblings
- Child safety is absolute — culture informs communication, not the threshold
Re-traumatisation
Procedural
- Repeated examinations without photo-documentation
- Using a family member as interpreter
- Male examiner without female preference offered
- One examination, one interview, with images for peer review
Missed deinfibulation
Clinical
- Not offering deinfibulation to Type III women
- Leaving infibulation intact in pregnancy
- Reactive intrapartum cutting instead of planned antenatal
- Plan deinfibulation early — second trimester or pre-conception
The "cultural sensitivity" trap deserves naming explicitly, because it is the error that lets children be harmed. Cultural sensitivity means communicating with respect, using interpreters, understanding the family's perspective, and engaging the community. It does not mean deferring the safeguarding response, accepting the practice, or failing to report. The child's right to bodily integrity is absolute, and no cultural argument overrides it. A clinician who defers reporting "out of respect for the family" has failed the child. [9] [8]
The procedural pitfalls — using a family member as interpreter, performing repeated examinations without photo-documentation, or assigning a male examiner without offering a female — compound the trauma and erode trust. Every one of these is avoidable with a protocol, and the protocol is part of the treatment. [10] [8]
Prognosis & Disposition
The long-term consequences of FGM span physical, sexual, psychological, and obstetric domains, and they are substantial. The systematic review and meta-analysis evidence links FGM to higher rates of dyspareunia and sexual dysfunction, prolonged and obstructed labour, obstetric fistula, postpartum haemorrhage, recurrent urinary infection, PTSD, depression, and anxiety. Type III carries the heaviest burden across every category. [1] [3] [5]
Disposition is decided by safety first. The child who has been cut must not return to an environment where further harm is possible, and the siblings must be screened and protected. The multi-agency plan — child-protection services, police where indicated, community engagement, and the clinical follow-up — is what keeps the child safe over time. The paediatrician owns the medical follow-up: the deinfibulation referral, the mental-health pathway, the obstetric planning for the future, and the longitudinal relationship. [9] [8]
What determines a good outcome is less the single act of recognition and more whether the child received comprehensive care — deinfibulation or reconstruction where indicated, trauma-focused therapy for the psychological injury, and protection of her siblings. The general paediatrician who holds the child and her family over months and years, engaging the community and preventing the next cutting, is often the most important determinant of long-term outcome. [9] [7]
Special Populations
Migrant, refugee, and asylum-seeking girls from practising communities are the primary at-risk group in ANZ, the UK, and Canada. The assessment must be culturally safe, interpreter-mediated (never by a family member), and connected to community engagement services. These families may have complex experiences of displacement, trauma, and cultural transition, and the clinician who builds trust over time is better placed to protect the child than one who arrives only with a mandate. [8] [9]
Children with disability, especially non-verbal children, are at higher risk of all forms of abuse including FGM, and they disclose less. The threshold to examine is lower, the examination is adapted to the child's communication and sensory needs, and a familiar carer and communication aids are used. Behavioural change may be the only signal. [8]
Adolescents bring consent and confidentiality dimensions. A mature minor can consent to examination, deinfibulation, and mental-health treatment. The limits of confidentiality — including mandatory reporting — are stated before the assessment, and the adolescent is kept as the primary decision-maker wherever she is competent. Youth-friendly, non-judgemental conduct is part of the treatment. [8]
Aboriginal and Torres Strait Islander, Māori, and Pacific children are not from practising communities in the FGM sense, but they may be in settings where migrant families from practising communities are neighbours or peers. The principles of culturally safe care — respect, communication, community engagement, and avoidance of re-traumatisation — are shared, and the clinician trained in one is better equipped for the other. [8]
Evidence, Guidelines & Regional Differences
The operational evidence base for this topic rests on the WHO guidelines on the management of health complications from FGM, which set out the clinical approach to deinfibulation, obstetric care, and mental-health management. The systematic review evidence — Lurie and colleagues on painful gynaecologic and obstetric complications, Abdalla on mental health, and Nzinga on sexual health — quantifies the complication burden and supports the management recommendations. These sources, with the local child-protection statute, are the framework a fellowship candidate should name. [1] [3] [5]
Regional differences are real and the examiner expects them to be named. In ANZ, FGM is a criminal offence in all Australian states and territories and under the New Zealand Crimes Act, with mandatory reporting of a child at risk of or who has undergone FGM applying to medical practitioners. Specialist FGM clinics operate in major centres. In the UK, the Female Genital Mutilation Act 2003 (and its 2015 amendment) criminalises FGM, introduces FGM Protection Orders, and mandates reporting of known FGM in under-18s to the police by regulated health and social-care professionals. In the US, federal law criminalises FGM and the practice is also banned by state statute in most states. [8] [9]
The live controversies are familiar. Should deinfibulation be offered antenatally or pre-conception, and who should perform it? How should mandatory reporting interact with therapeutic relationships in communities that fear state intervention? What is the role of the medicalised provider, and does harm-reduction have any place? And the central tension — how to protect the child without alienating the community — is a continuing challenge that requires both clinical competence and cultural humility. [9] [8]
Exam Pearls
CIRCUMS
Other high-yield facts: over 200 million girls and women are affected worldwide, with most cut before age 15; Type III carries the highest complication burden and the greatest obstetric risk; deinfibulation counselling improves outcomes and should be offered to every woman with Type III; reconstructive surgery in a multidisciplinary model addresses anatomy, psychology, and sexual function together; and the girl at imminent risk during a planned overseas trip is the single highest-yield prevention opportunity the paediatrician has. [6] [7]
References
- [1]Lurie JM, Weidman A, Huynh S, Delgado D, Eastaugh E, Choma K, Baskin L, Magaña C Painful gynecologic and obstetric complications of female genital mutilation/cutting: A systematic review and meta-analysis. PLoS Medicine, 2020.PMID 32231359
- [2]Bonavina G, Kaltoud R, Ruffolo AF, Maggiore ULR, Carriero C, Ferrazzi E Female Genital Mutilation and Cutting and Obstetric Outcomes. Obstetrics & Gynecology, 2022.PMID 35849461
- [3]Abdalla SM, Galea S Is female genital mutilation/cutting associated with adverse mental health consequences? A systematic review of the evidence. BMJ Global Health, 2019.PMID 31406589
- [4]Bello S, Ogugbue M, Chibuzor M, Irurhe O, Olowu R, Ogunfowokan O Counselling for deinfibulation among women with type III female genital mutilation: A systematic review. International Journal of Gynaecology and Obstetrics, 2017.PMID 28164284
- [5]Nzinga AM, De Andrade Castanheira S, Hermann J, Pino FL, Onyenwe O Consequences of Female Genital Mutilation on Women's Sexual Health - Systematic Review and Meta-Analysis. Journal of Sexual Medicine, 2021.PMID 33618990
- [6]Ayenew AA, Mol BW, Bradford B, Gidey G, Teshome D, Asefa A Prevalence of female genital mutilation and associated factors among women and girls in Africa: a systematic review and meta-analysis. Systematic Reviews, 2024.PMID 38217004
- [7]Restaino S, Pellecchia G, Driul L, Londero AP, Bertozzi S, Monica S Reconstructive surgery after Female Genital Mutilation: a multidisciplinary approach. Acta Bio-Medica, 2022.PMID 35765892
- [8]Xu Z, Chen X, Yu J, Liu Y, Wang Q Female Genital Mutilation/Cutting: A Systematic Review of Global Patterns, Sociocultural Drivers, and Health Consequences. Journal of Pediatric and Adolescent Gynecology, 2026.PMID 41038307
- [9]Ehiri JE Health systems approaches and other multisectoral efforts for primary prevention of female genital mutilation and clinical management of its complications. International Journal of Gynaecology and Obstetrics, 2026.PMID 41582678
- [10]Paliwal P, Ali S, Bradshaw S, Hughes A, Jolly K Management of type III female genital mutilation in Birmingham, UK: a retrospective audit. Midwifery, 2014.PMID 23747293