Paeds · child-safety-and-social-paediatrics
Homelessness and housing instability
Also known as Housing insecurity in children · Family homelessness and child health · Housing as a social determinant of child health · Unstable housing and developmental harm · Overcrowding, eviction and child wellbeing
Fellowship-level guide to homelessness and housing instability as a paediatric health problem: the housing continuum from stable to crisis, the toxic-stress mechanism that embeds harm biologically, the five domains of clustered morbidity (physical, growth and nutrition, developmental and educational, mental and behavioural, and access and continuity), the screening-to-housing pathway, the portable summary that protects continuity, and the paediatrician's role as screener, treater, linker and housing advocate.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old girl brought to your clinic for an asthma exacerbation. Her mother has missed two appointments in the last month, the address on file is wrong, and when you ask gently whether they have a stable place to live, her mother's eyes fill with tears. She tells you they have been sleeping on her sister's lounge room floor for six weeks since an eviction. This child's asthma is not a separate problem from her housing — it is part of the same problem, and your job is to recognise that. [4] [5]
Housing instability is the continuum of housing-related distress that runs from insecurity — falling behind on rent, overcrowding, frequent moves, couch surfing — through to overt homelessness, where a family has no fixed address and may be sleeping rough, in a car, or in crisis accommodation. Homelessness is the visible tip; housing instability is the far larger, hidden iceberg beneath it, and it is where most paediatric harm accumulates. [1] [3]
The load-bearing principle is that housing is a determinant of child health. Stable, safe, adequate housing is not a welfare issue handed to a social worker beyond the clinic door — it is a clinical vital sign that predicts physical illness, developmental delay, mental-health difficulty and educational underachievement. Lal and Slopen's 2024 synthesis in JAMA Pediatrics framed housing instability as a measurable, modifiable driver of children's health and education outcomes, reframing the paediatrician's role to include screening, linking and advocacy. [2]
The second principle is the continuum, not the event. Children move in both directions along the housing pathway, and a family may oscillate between stable housing, insecurity and crisis several times in a year. The harm is cumulative — each move, each period of overcrowding, each night of cold or fear adds to a toxic-stress load — and the paediatric encounter can happen anywhere along the continuum, not only at the crisis end. [3] [4]
Classification
Think of housing instability by where the family sits on the continuum, because that shapes what you will find and what you must do. The useful clinical taxonomy sorts families by the degree of housing security, from stable through to overt homelessness, and recognises that the slide between categories is fluid and often bidirectional. [1] [4]
The categories overlap heavily. A single family may be overcrowded, behind on rent and couch-surfing in the same month, then enter crisis accommodation, then return to insecure private rental. The taxonomy is a clinical map, not a fixed label — use it to gauge severity and plan the response, and expect movement. [3]
The housing continuum — what you find, what you do
Epidemiology & Risk Factors
Housing instability among children is far more common than the visible face of rough sleeping suggests. Lebrun-Harris and colleagues' 2024 nationally representative study in JAMA Pediatrics found that a substantial proportion of US children had experienced unstable housing, and that unstable housing was strongly associated with poor child and caregiver health. The hidden iceberg of insecurity — overcrowding, frequent moves and arrears — dwarfs the visible tip of overt homelessness. [1]
Bess and colleagues' scoping review synthesised the global evidence on the health effects of housing insecurity on children, documenting a consistent relationship across settings between insecure housing and worse physical, developmental and mental-health outcomes. The review stressed that the harm is dose-dependent — more moves, more crowding and more insecurity produce more harm — and that it clusters with poverty, food insecurity and other adversities. [3]
The burden falls hardest on the youngest children. Cutts and colleagues' foundational study of very young children found that housing insecurity was associated with worse health, developmental risk and food insecurity in infants and toddlers — a particularly vulnerable window because the brain is developing rapidly and the toxic-stress load is being laid down. [5]
Sandel and colleagues' renter-family study in Pediatrics showed that unstable housing was independently associated with worse caregiver and child health, even after adjusting for income. The key insight is that housing instability is a health determinant in its own right, not merely a marker of poverty — it adds harm above and beyond socioeconomic status. [4]
Rose-Jacobs and colleagues found that housing instability is markedly elevated among families of young children with special health care needs — a group already carrying high health complexity. The dual burden compounds: a medically complex child is harder to house stably, and unstable housing makes the medical complexity harder to manage. [6]
Domestic and family violence is a central driver. Families fleeing violence are overrepresented among those presenting to crisis services, and housing instability and violence are tightly entangled — a family may become homeless because of violence, and homelessness may expose a family to further violence. The two must be screened for together. [3] [15]
Indigenous children and families carry a disproportionate burden of housing instability in Australia and New Zealand, reflecting the structural legacy of colonisation, dispossession and intergenerational disadvantage. Sivertsen and colleagues' nurse-practitioner-led service documented the high housing mobility of Aboriginal families and the consequent fracture of primary-care continuity. [14]
Pathophysiology
There is no single disease here — there is a toxic-stress pathway in which housing instability becomes biological harm through chronic activation of the stress response, disruption of the caregiving environment, and the embedding of that harm in developing physiology. Understanding the pathway tells you where to intervene. [4] [8]
Housing instability generates chronic, unpredictable stress. Overcrowding, cold, damp, noise, frequent moves, food insecurity and the constant threat of eviction activate the stress response repeatedly, without the buffering of a predictable, safe environment. The parent is stressed, and a stressed parent is less able to co-regulate a child — the caregiver buffer is the single most powerful protective factor, and housing instability erodes it. [4] [11]
Suglia, Duarte and Sandel showed that poor housing quality and instability are associated with worse maternal mental health, and that maternal depression mediates much of the child harm. The pathway runs through the parent: when a mother's mental health collapses under housing stress, the child loses the relational buffer that protects development. [11]
The harm becomes biologically embedded. Keen and colleagues' 2024 study in Brain, Behavior, and Immunity showed that adolescent housing insecurity predicts elevated inflammation over time — a measurable biological signature of the social adversity, consistent with the toxic-stress framework of HPA-axis dysregulation and chronic low-grade inflammation. This is not soft harm; it is measurable, cumulative physiology. [8]
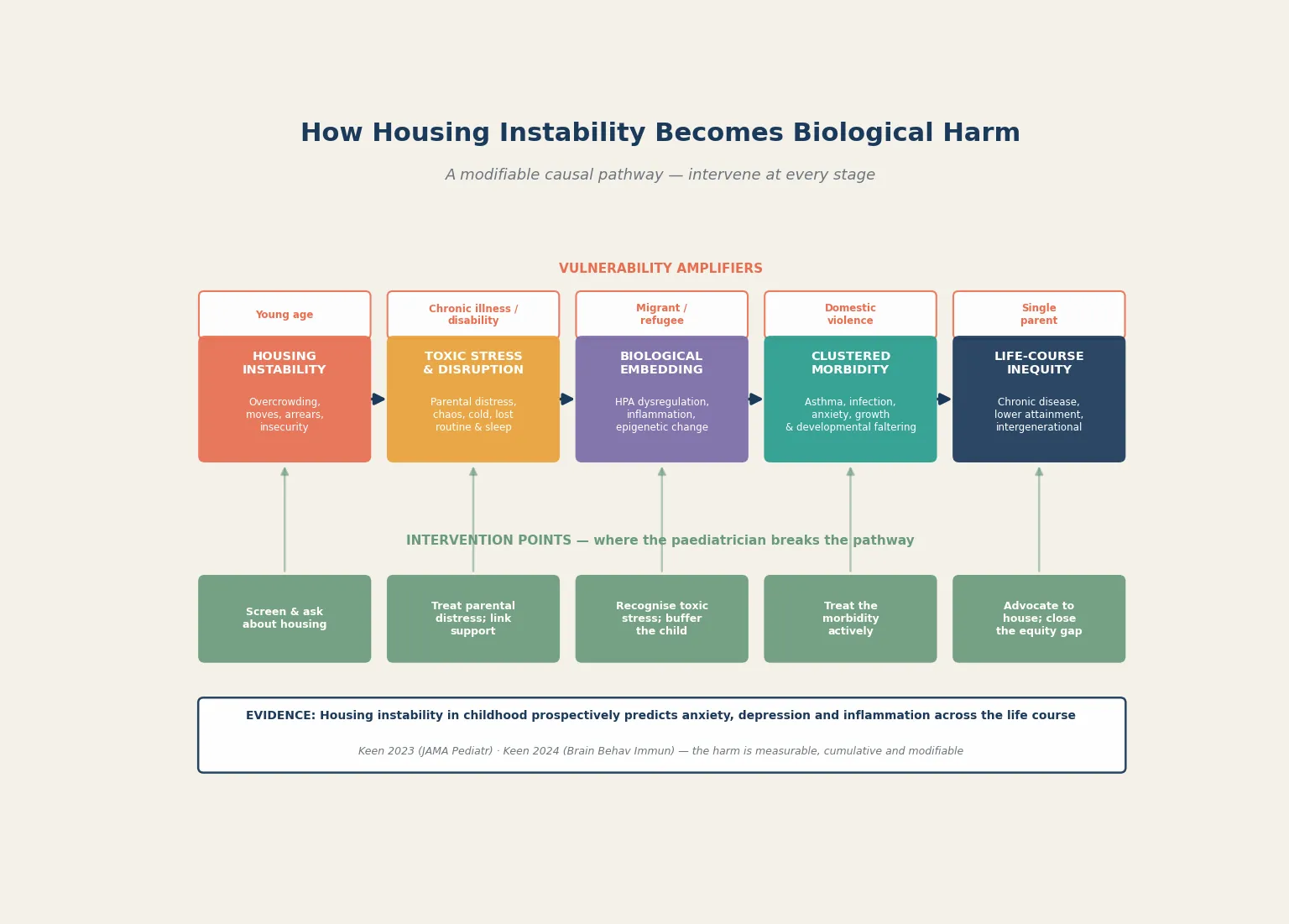
The mental-health embedding is profound and long-lasting. Keen and colleagues' prospective study in JAMA Pediatrics found that childhood housing insecurity predicted anxiety and depression symptoms not only in childhood but into adulthood — the harm tracks across the life course, decades after the housing instability itself. Hatem and colleagues showed that food and housing insecurity in early childhood predict adolescent mental-health problems. [7] [9]
The developmental mechanism is the disruption of the caregiving and learning environment. A child who moves school repeatedly, who sleeps poorly in an overcrowded room, who is hungry, and whose parent is depressed cannot build the cognitive and emotional scaffolding that early childhood requires. The result is developmental delay, lower educational attainment and the behavioural dysregulation that compounds into school exclusion and adolescent difficulty. [2] [3]
Crisis amplifies the harm. Coughlin, Sandel and Stewart's analysis of homelessness, children and COVID-19 documented how a pandemic-era crisis deepened the housing emergency for families, exposing how quickly housing instability can tip into overt homelessness when protective scaffolding — schools, extended family, informal supports — is withdrawn. [15]
Clinical Presentation
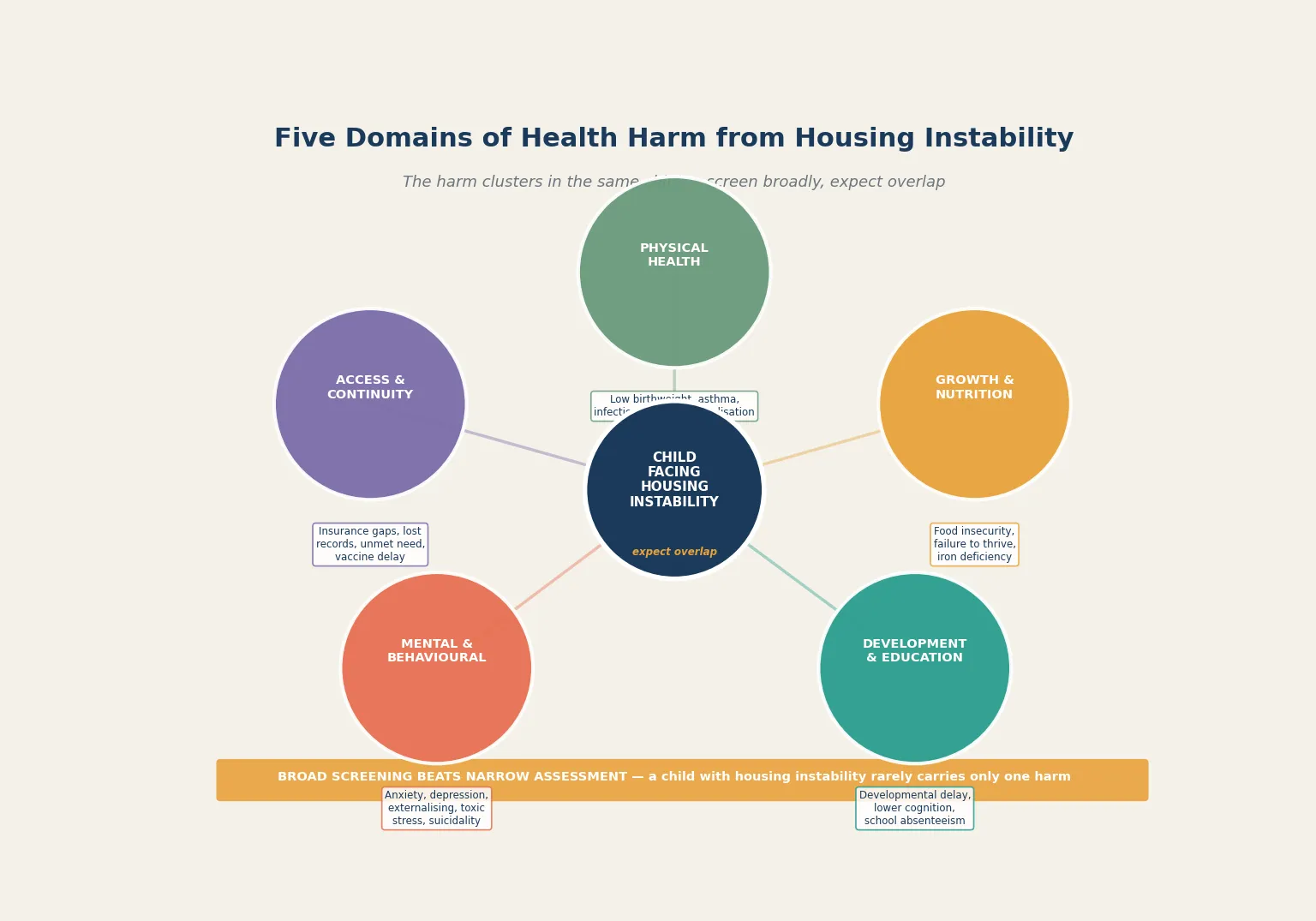
A child facing housing instability rarely presents with a housing complaint. They present with asthma, an infection, a developmental concern, a behavioural difficulty, a missed appointment or an emergency — and the housing instability is the upstream driver hiding beneath the presenting problem. Your job is to ask, because the family will rarely volunteer it. [3] [4]
The physical-health presentation is varied and reflects the crowded, cold and unstable environment: recurrent respiratory infections, asthma exacerbations (mould, damp, dust mites and smoke exposure), skin infections (scabies, impetigo in overcrowding), injuries, and exacerbations of chronic disease such as epilepsy or diabetes when medications and routines are disrupted. [2] [5]
The growth and nutrition presentation reflects the food insecurity that travels with housing instability. Faltering growth, iron-deficiency anaemia, and poor dietary quality are common, and the youngest children are most affected. Cutts' foundational data linked housing insecurity to food insecurity and developmental risk in very young children. [5]
The developmental and educational presentation is the slow-burn harm. Developmental delay, speech and language difficulty, school absenteeism, behavioural dysregulation and lower educational attainment accumulate over years of instability. Lal and Slopen's synthesis framed housing instability as a driver of educational underachievement that compounds across the school years. [2]
The mental-health and behavioural presentation is among the most consequential. Anxiety, depression, externalising behaviour, sleep disturbance, school refusal and, in adolescents, self-harm and suicidality are all elevated in children facing housing instability. Keen's prospective data showed the anxiety and depression track into adulthood, and the toxic-stress mechanism means the presentation can persist long after rehousing. [7] [9]
The access and continuity presentation is the fracture that deepens all the others. A family that moves frequently loses their general practitioner, their specialist referrals, their prescriptions and their records. Carroll and colleagues showed that housing instability is associated with health-insurance gaps — children lose coverage when addresses change, and the administrative friction of reinstating care is often insurmountable for a family in crisis. [10]
Differential Diagnosis
When you encounter a child with housing instability, the first task is to distinguish the upstream driver from the downstream symptoms. What looks like a behavioural problem, recurrent asthma or developmental delay may all be downstream of the same housing instability — reframe the presentation before you chase each symptom in isolation. [3] [4]
Distinguish toxic-stress-driven behavioural difficulty from primary neurodevelopmental disorder. A child who is dysregulated, inattentive and oppositional in the context of housing instability and parental distress may be expressing a stress response rather than a primary ADHD or conduct disorder. The distinction matters: rehousing, parental support and trauma-informed intervention may resolve the behavioural picture, whereas a premature diagnostic label may not. [7] [8]
Separate food-insecurity-related faltering growth from organic disease. A child with poor weight gain in the context of housing and food insecurity needs a nutritional and social assessment before extensive organic work-up — though coexisting organic disease must not be missed. Address the food insecurity first, and re-measure. [5]
Differentiate environmentally driven respiratory disease from primary asthma. A child with recurrent wheeze in damp, mouldy, overcrowded housing may have environmental exposure driving the symptoms. Treating the child with escalating asthma medication without addressing the housing is managing the symptom, not the cause. [2] [15]
Distinguish safeguarding-relevant housing crisis from socioeconomic housing difficulty. A family sleeping rough with children, or a family fleeing domestic violence, may meet child-protection thresholds that demand immediate, structured intervention — the housing difficulty has become a safety issue. Recognise when the situation has crossed from social need into safeguarding. [3] [15]
Tell apart acute crisis from chronic instability. A family newly evicted this week has different immediate needs from a family who has been chronically insecure for years. The acute crisis demands same-day safety and emergency housing; the chronic instability demands a sustained linkage and advocacy strategy. [3]
Clinical & Bedside Assessment
The clinical encounter with a child facing housing instability must be structured, trauma-informed and broad. Treat every encounter as an opportunity to screen, because housing is a vital sign and the family will rarely raise it themselves. [1] [4]
Ask about housing routinely. Use a validated, brief screening question — "Do you have a stable place to live?" or a standardised social-needs tool — at health-supervision visits and at acute presentations. Normalising the question removes stigma and surfaces hidden instability. Lebrun-Harris' data showed that screening in clinical settings identifies instability that would otherwise be missed. [1]
Take a trauma-informed, strengths-based history. Explain why you are asking, what you will do with the information, and the limits of confidentiality. Use open, non-judgemental language, pace the interview for the family's distress, and recognise that shame and fear may limit disclosure. Ask about the housing, the moves, the food, the safety, the school and the parent's own wellbeing — but follow the family's lead on pace and depth. [3] [14]
Screen broadly across the five domains. Once you identify housing instability, do not stop at the presenting complaint. Assess growth (plot and trend), development (validated screen), mental health and behaviour (parent and child), physical health (respiratory, skin, chronic disease), and access and continuity (GP, specialist, prescriptions, vaccines, records). The broad screen is the defensible default. [6]
Examine the child thoroughly. Measure and plot growth, examine the respiratory system (wheeze, signs of chronic exposure), the skin (infection, scabies, eczema), the developmental status, and any chronic disease. Check the vaccination record — gaps are common and catch-up is part of the encounter. Dental health is frequently neglected. [5] [6]
Assess the parent and the caregiving environment. Parental mental health is the mediator of much of the child harm, and a depressed, overwhelmed parent cannot buffer a child through instability. Ask the parent how they are coping, screen for depression, and recognise that supporting the parent is supporting the child. [4] [11]
Investigations
Investigations follow the clinical questions the broad screen raises, not a blanket protocol. The goal is to bring the standard of assessment up to community equivalence — to run the work-up any child with these findings would receive, regardless of the housing chaos. [1] [6]
Growth and nutritional investigation targets the food-insecurity-driven findings. Plot weight, height and BMI against age-appropriate standards, trend them, and investigate faltering growth and anaemia as you would in any child — full blood count and iron studies where indicated, with a nutritional and social assessment to identify the upstream driver. [5]
Developmental and cognitive assessment is warranted when the screen flags delay. Validated developmental screening tools (such as the ASQ or PEDS), and referral for formal developmental or educational psychology assessment, address the slow-burn harm that accumulates across years of instability. Lal and Slopen stressed the educational dimension of the harm. [2]
Mental-health assessment is central, given the strength of the prospective evidence. A child or young person with anxiety, depression, externalising behaviour or self-harm in the context of housing instability needs a structured mental-health assessment and a trauma-informed care plan. Keen's data show the symptoms can persist long after rehousing, so treat them actively. [7] [9]
Physical-health investigation targets the findings of the examination. Spirometry for recurrent wheeze, swabs for skin infection, chronic-disease monitoring, and vaccination catch-up address the common gaps. For children with special health care needs, coordinate the full specialist work-up and protect it through moves. [6] [10]
Investigations that are not helpful include those ordered defensively without a clinical question, blanket panels that generate false reassurance, and any work-up that delays the more important intervention of linking the family to housing and support. Every investigation should serve the child's care plan. [3]
Management — Resuscitation
The resuscitation phase addresses the acute risks that threaten the child's safety or health in the immediate term. Identify them, act on them, and document what you did — but recognise that acute medical crisis in this setting is usually driven by the housing instability, and the real resuscitation includes same-day housing and safety action. [2] [15]
Acute medical emergencies — severe asthma exacerbation, sepsis, diabetic ketoacidosis, status epilepticus — are managed as they would be in any child, with the standard resuscitation pathway. The difference is recognising that the precipitant may be a disrupted medication supply, a damp and mouldy environment, or an infection acquired in overcrowding, and that addressing the precipitant is part of preventing recurrence. [2] [5]
Safeguarding and safety emergencies are managed through the child-protection and domestic-violence pathways. A family sleeping rough with children, a child at risk in crisis accommodation, or a family fleeing violence need immediate, structured safety action — child-protection notification, domestic-violence service engagement, and emergency housing. Do not defer safety to a routine follow-up. [3] [15]
Acute mental-health crisis in an adolescent — self-harm, suicidality, acute behavioural dysregulation — is managed as a mental-health emergency. Risk assessment, safety planning, and urgent mental-health involvement apply as they would for any young person, with the added recognition that housing instability is a potent stressor driving the crisis. [7] [12]
Allocate roles so that clinical care and the housing-and-safety response run in parallel. Your job is to advocate for the medical priority, communicate clearly with social work, housing and child-protection services, and document the clinical reasoning. When clinical and administrative agendas collide, the child's safety and health come first. [3]
Management — Definitive & Stepwise
Once the acute risks are managed, the definitive phase builds a comprehensive, community-equivalent care plan, links the family to housing and support services, and protects continuity through the chaos of instability. This is where the encounter becomes a health-improving intervention rather than a holding operation. [1] [13]
Screening-to-stable-housing pathway
Screen — ask about housing at every encounter using a validated brief tool; normalise the question
Assess — broad five-domain review: growth, development, mental health, physical, access and continuity
Treat — evidence-based care to community standard; do not lower the bar; address toxic stress and parental mental health
Link — social work, housing services, financial and food support; warm referral, not a phone number
House — advocate for stable, safe housing; the upstream intervention that medicine alone cannot deliver
Follow up — portable summary, confirmed appointment, continuity protection; close the equity gap
Treat what you find. Every domain of harm — faltering growth, developmental delay, mental-health difficulty, chronic disease, vaccination gaps — receives an evidence-based management plan to the community standard. The defensible principle is equivalence of care: the child receives the same quality of assessment and treatment regardless of housing status. [4] [6]
Support the parent to buffer the child. Because parental mental health mediates much of the child harm, treating parental depression and distress, linking the parent to support, and recognising the parent as the protective buffer is a direct child-health intervention. Suglia's data showed that housing quality and instability shape maternal mental health, which in turn shapes child health. [11]
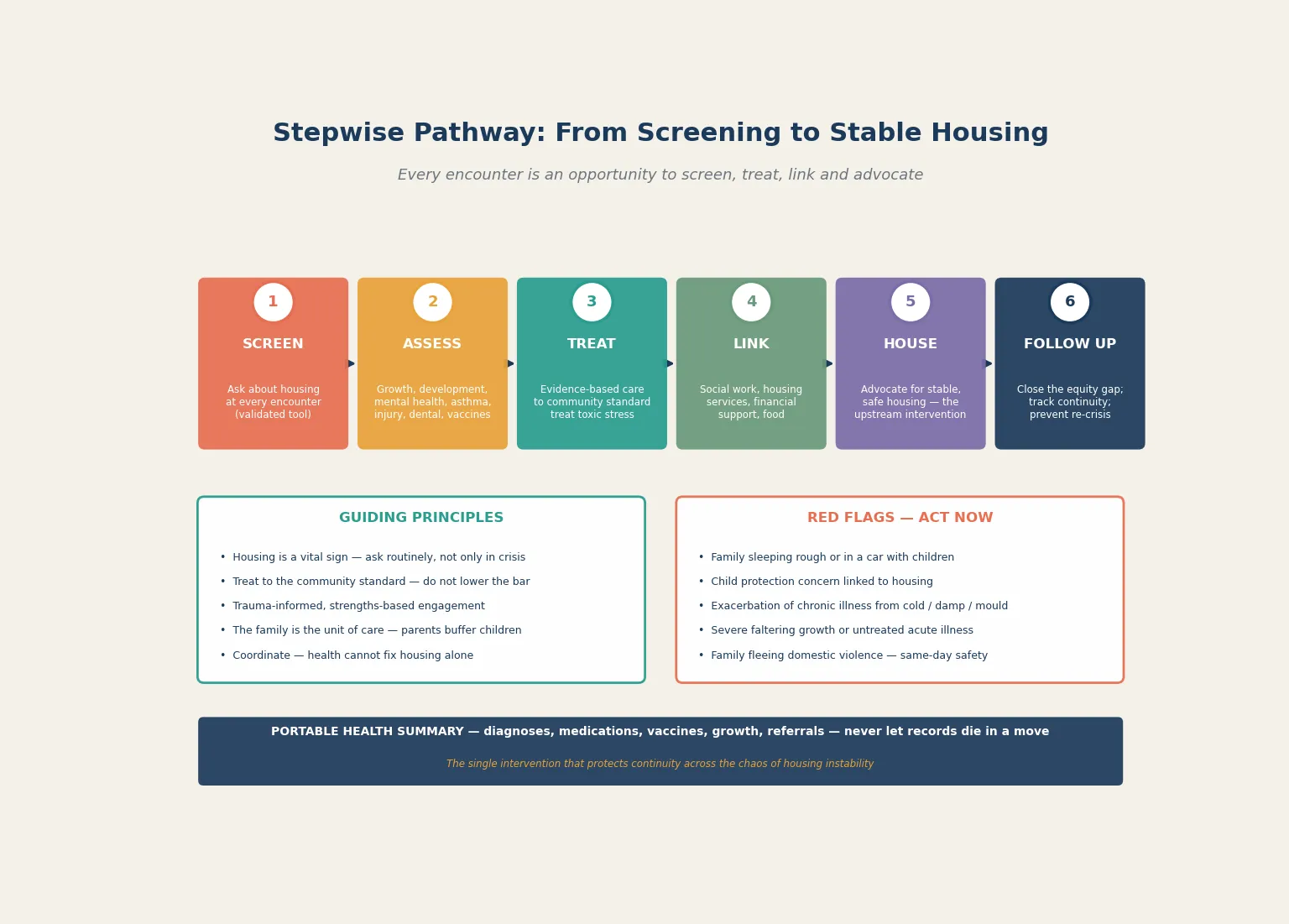
Build and protect a portable health summary. The single most practical continuity intervention is a portable record — diagnoses, medications, vaccinations, growth, allergies, referrals and the care plan — that travels with the family through moves. Carroll's data on insurance gaps show how administrative fracture destroys continuity; the portable summary is the paediatrician's counter-measure. [10]
Link warmly, do not just refer. A phone number handed to a family in crisis is rarely actioned. Warm referral — a direct handoff to a named social worker, housing officer or support service, with the family's consent and a confirmed contact — converts referral into action. Sivertsen's nurse-practitioner-led service demonstrated the value of proactive, relational linkage for highly mobile Aboriginal families. [14]
Advocate for housing as the upstream intervention. Bovell-Ammon and colleagues' pilot randomised trial in Health Affairs showed that a housing intervention for medically complex families was associated with improved family health. Housing is healthcare, and advocating for stable, safe housing is clinical advocacy — refer to housing services, support applications, and where systems allow, contribute medical letters that document the health case for priority housing. [13]
Specific Subtypes & Scenarios
The infant with faltering growth and housing instability. A six-month-old with weight tracking below the third centile, born to a mother in crisis accommodation, presents the classic convergence. Assess feeding, plot growth, check for iron deficiency and organic disease, and address the food and housing insecurity as the upstream driver. Nutritional supplementation, food-bank linkage and housing advocacy are the treatment alongside any medical work-up. [5]
The school-age child with recurrent asthma and damp housing. A seven-year-old presenting repeatedly with wheeze, living in a damp, mouldy private rental, illustrates the environmental driver. Treat the asthma to guideline standard, escalate preventer therapy, but also document the housing as a medical issue — an advocacy letter to the housing authority or landlord, supporting the family's case for rehousing, is part of the medical management. [2] [15]
The family fleeing domestic violence into homelessness. A mother and two children presenting to the emergency department after fleeing violence, now with no fixed address, demand a same-day, multi-agency response. Activate the domestic-violence and child-protection pathways, arrange emergency housing and safety planning, assess the children for injury and psychological harm, and build the portable summary so continuity survives the crisis. [3] [15]
The child with special health care needs and housing instability. Rose-Jacobs' data show that children with special health care needs are at markedly elevated risk of housing instability, and the dual burden compounds. A technology-dependent or medically complex child needs protected specialist continuity, reliable equipment and supply chains, and a housing situation that can accommodate the medical complexity — advocate fiercely and proactively. [6]
The adolescent transitioning from out-of-home care into homelessness. Chikwava and colleagues' linked-data cohort study showed that young people transitioning from out-of-home care have high rates of homelessness and housing instability, strongly associated with mental-health disorders. This group needs proactive transition planning, housing linkage before exit from care, and mental-health support — the period around leaving care is the highest-risk window. [12]
The Aboriginal or Torres Strait Islander family with high housing mobility. Apply trauma-informed, culturally safe practice, acknowledge the structural legacy of dispossession and the overrepresentation of Indigenous families in housing instability, and engage with community-controlled services wherever possible. Sivertsen's nurse-practitioner-led model demonstrated the value of outreach and relational continuity for highly mobile Aboriginal families. [14]
The family recently rehoused after a period of homelessness. Rehousing is not the end of the clinical story — it is the beginning of the catch-up phase. Address the accumulated morbidity (developmental delay, untreated chronic disease, mental-health difficulty), re-establish continuity with a GP and specialists, support the parent, and monitor for the residual toxic-stress effects that Keen's data show can persist. [7] [13]
Complications & Pitfalls
- Treating housing instability as a welfare problem handed to social work, not a health problem the paediatrician owns. [4]
- Asking about housing only in crisis — it is a vital sign that should be screened at every encounter. [1]
- Missing the clustering of harm — a child with unstable housing rarely carries only one problem; screen broadly across the five domains. [3] [6]
- Lowering the clinical standard because the family is chaotic — equivalence of care means the same evidence-based work-up and treatment as any child. [4]
- Letting records die in a move — the portable health summary is the single intervention that protects continuity. [10]
- Conflating housing instability with parental failure — recognise the structural drivers, including domestic violence and poverty, and respond without judgement. [3]
- Forgetting that housing is the upstream intervention — advocating for stable, safe housing is clinical advocacy, not work beyond scope. [13]
- Missing safeguarding and domestic-violence risk that crosses from social need into child-protection territory. [15]
- Treating the downstream symptom (asthma, behaviour, faltering growth) without addressing the upstream housing driver. [2]
- Failing to support the parent — parental mental health mediates much of the child harm, and an unsupported parent cannot buffer a child. [11]
Prognosis & Disposition
The prognosis for a child facing housing instability depends less on the presenting complaint than on whether the housing instability is recognised, the harm treated, and the family linked to stable housing and support. A child whose housing is stabilised, whose toxic-stress load is reduced, and whose accumulated morbidity is actively treated has a far better trajectory than one whose needs are managed symptom by symptom. [3] [4]
The mental-health prognosis is the most sobering. Keen's prospective data showed that childhood housing insecurity predicts anxiety and depression into adulthood — the harm is durable and tracks across the life course. This is not a reason for therapeutic nihilism; it is a reason to treat the mental-health harm actively and early, and to recognise that the benefit of intervention may unfold over years rather than weeks. [7] [9]
The immediate disposition depends on the assessment. Acute crisis may require emergency housing, hospital admission for acute medical or mental-health need, or child-protection action. Chronic needs are managed in the community with linkage, a portable summary, and a confirmed follow-up plan. The principle is the least disruptive, safest setting consistent with the child's health. [2] [15]
Housing intervention changes the prognosis. Bovell-Ammon's pilot randomised trial showed that housing medically complex families was associated with improved family health, confirming that housing is a clinical intervention with measurable health return. Advocating for housing is not advocacy beyond medicine — it is the upstream treatment. [13]
Longer-term, children who experience housing instability carry elevated risks of chronic disease, mental illness, educational underachievement and intergenerational disadvantage. Early recognition, active treatment of the clustered morbidity, parental support and housing advocacy are the interventions that bend the curve — and they are the paediatrician's contribution across the continuum. [1] [8]
Special Populations
Infants and very young children. The youngest children carry the heaviest developmental burden, because the brain is developing rapidly and the toxic-stress load is being laid down. Cutts' data linked housing insecurity to developmental risk and food insecurity in very young children — prioritise this group for screening, growth monitoring and early developmental support. [5]
Children with special health care needs. Rose-Jacobs' study showed that families of young children with special health care needs have markedly elevated rates of housing instability, compounding the medical complexity. Protected specialist continuity, reliable equipment and supply chains, and proactive housing advocacy are essential for this group. [6]
Adolescents transitioning from out-of-home care. Chikwava's cohort study documented high rates of homelessness and housing instability among young people leaving care, strongly associated with mental-health disorders. Proactive transition planning, pre-exit housing linkage and sustained mental-health support address the highest-risk window. [12]
Aboriginal and Torres Strait Islander families. Apply trauma-informed, culturally safe care, acknowledge the structural drivers of housing instability in Indigenous communities, and engage with community-controlled services. Sivertsen's outreach model demonstrated the value of relational continuity for highly mobile Aboriginal families, where conventional clinic-based models fracture. [14]
Migrant, refugee and asylum-seeking families. Language barriers, uncertain legal status, disrupted documentation and prior trauma complicate both housing need and access. Use professional interpreters, pace for trauma, and advocate for services that recognise the additional layers of vulnerability. [3]
Families experiencing domestic violence. Housing instability and violence are tightly entangled — violence drives homelessness, and homelessness exposes families to further violence. Screen for both together, activate the safety pathway, and recognise that housing stability is inseparable from safety. [15]
Evidence, Guidelines & Regional Differences
The evidence base on housing instability and child health has matured rapidly, driven by the Children's HealthWatch network and the social-determinants movement in paediatrics. Sandel and colleagues' 2018 renter-family study in Pediatrics established that unstable housing is an independent health determinant, not merely a marker of poverty. [4]
Cutts and colleagues' 2011 foundational study in the American Journal of Public Health documented the health and developmental impact of housing insecurity on very young children, establishing the dose-response relationship and the particular vulnerability of the youngest. [5]
The mental-health and biological-embedding evidence has transformed the field. Keen and colleagues' 2023 JAMA Pediatrics prospective study showed that childhood housing insecurity predicts anxiety and depression into adulthood, and their 2024 Brain, Behavior, and Immunity study showed that adolescent housing insecurity predicts elevated inflammation — together establishing that the harm is measurable, cumulative and biologically embedded. [7] [8]
The intervention evidence is the most actionable. Bovell-Ammon and colleagues' 2020 pilot randomised trial in Health Affairs showed that housing intervention for medically complex families was associated with improved family health — the first-line evidence that housing is healthcare and that advocacy changes outcomes. [13]
In Australia, housing instability and family homelessness are addressed through state and territory housing authorities, specialist homelessness services, and community organisations, with the Australian Institute of Health Welfare reporting national data. Aboriginal and Torres Strait Islander families are disproportionately affected, and culturally safe, community-controlled services are central to an effective response. The Royal Australasian College of Physicians advocates for housing as a child-health determinant. In Aotearoa New Zealand, Kāinga Ora and the Ministry of Housing and Urban Development administer social housing, with obligations under Te Tiriti o Waitangi and attention to the overrepresentation of Māori and Pasifika families. State the principle — screen, treat, link, advocate — and apply current state, territory or national housing and health guidance to the local model. [14] [3]
Exam Pearls
SHELTR
References
- [1]Lebrun-Harris LA, Sandel M, Sheward R, Caffery C, Bagalman E, Henke RM, et al. Prevalence and Correlates of Unstable Housing Among US Children. JAMA Pediatrics, 2024.PMID 38767882
- [2]Lal A, Slopen N Housing Instability and Children's Health and Education. JAMA Pediatrics, 2024.PMID 39186283
- [3]Bess KD, Miller AL, Mehdipanah R The effects of housing insecurity on children's health: a scoping review. Health Promotion International, 2023.PMID 35134939
- [4]Sandel M, Sheward R, Ettinger de Cuba S, Coleman SM, Heeren TC, Black MM, et al. Unstable Housing and Caregiver and Child Health in Renter Families. Pediatrics, 2018.PMID 29358482
- [5]Cutts DB, Meyers AF, Black MM, Casey PH, Chilton M, Cook JT, et al. US Housing insecurity and the health of very young children. American Journal of Public Health, 2011.PMID 21680929
- [6]Rose-Jacobs R, Ettinger de Cuba S, Bovell-Ammon A, Black MM, Heeren TC, Cutts DB, et al. Housing Instability Among Families With Young Children With Special Health Care Needs. Pediatrics, 2019.PMID 31292218
- [7]Keen R, Chen JT, Slopen N, Newman OI, Jackson JS, Williams DR, et al. Prospective Associations of Childhood Housing Insecurity With Anxiety and Depression Symptoms During Childhood and Adulthood. JAMA Pediatrics, 2023.PMID 37338896
- [8]Keen R, Chen JT, Slopen N, Belsky DW The biological embedding of social adversity: How adolescent housing insecurity impacts inflammation over time. Brain, Behavior, and Immunity, 2024.PMID 38714268
- [9]Hatem C, Lee CY, Zhao X, Reesor-Oyer L, Lopez NV Food insecurity and housing instability during early childhood as predictors of adolescent mental health. Journal of Family Psychology, 2020.PMID 32191051
- [10]Carroll A, Corman H, Curtis MA, Noonan K Housing Instability and Children's Health Insurance Gaps. Academic Pediatrics, 2017.PMID 28232258
- [11]Suglia SF, Duarte CS, Sandel MT Housing quality, housing instability, and maternal mental health. Journal of Urban Health, 2011.PMID 21647798
- [12]Chikwava F, O'Donnell M, Ferrante A, Pakpahan E, Crawford S, McIntyre G, et al. Patterns of homelessness and housing instability and the relationship with mental health disorders among young people transitioning from out-of-home care: Retrospective cohort study using linked administrative data. PLoS One, 2022.PMID 36054257
- [13]Bovell-Ammon A, Mansilla C, Poblacion A, Mudo C, James T, Sandel M Housing Intervention For Medically Complex Families Associated With Improved Family Health: Pilot Randomized Trial. Health Affairs, 2020.PMID 32250672
- [14]Sivertsen N, Parry Y, Willis E, Kendall S Aboriginal children and family connections to primary health care whilst homeless and in high housing mobility: observations from a Nurse Practitioner-led service. Primary Health Care Research and Development, 2022.PMID 35307050
- [15]Coughlin CG, Sandel M, Stewart AM Homelessness, Children, and COVID-19: A Looming Crisis. Pediatrics, 2020.PMID 32747589