Paeds · child-safety-and-social-paediatrics
Inflicted fractures and other non-accidental musculoskeletal injury
Also known as Non-accidental skeletal injury · Inflicted skeletal injury · Child abuse fractures · Classic metaphyseal lesion (corner / bucket-handle fracture) · Posterior rib fractures of abuse · Skeletal survey for suspected physical abuse
Fellowship guide to inflicted (non-accidental) musculoskeletal injury: the high-specificity fracture patterns — classic metaphyseal lesion, posterior rib, scapular, spinous and sternal fractures — alongside the moderate- and low-specificity patterns; the shearing and lever biomechanics (Tsai finite-element; Lonergan radiologic-pathologic correlation); the AAP and ACR skeletal-survey protocol with the mandatory follow-up survey; the bone-fragility and rickets differentials; and the safeguarding-first, multi-domain assessment in which no single fracture is pathognomonic and specificity outranks sensitivity — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-month-old who cannot yet crawl is brought with a swollen, irritable thigh. The story is a "roll off the sofa," yet the femur is spiralled and the infant has not moved independently once in her life. That is the consultation this topic is about: an injury whose mechanism does not fit the child, the story, or the developmental stage, and that therefore demands you convert from treating a fracture to investigating possible inflicted injury. [1] [2]
Inflicted or non-accidental musculoskeletal injury covers skeletal injury caused by inflicted force or by failure to protect — recognised through fracture patterns whose specificity for abuse runs from high to low. Kemp's systematic review remains the anchor: rib fractures (especially posterior), the classic metaphyseal lesion, and fractures of the scapula, sternum and spinous process carry the highest specificity for abuse, while clavicular and linear skull fractures sit near the common, low-specificity end. [1] [16]
Two framing principles govern everything that follows, and the candidate who omits either mis-states the topic. First, no fracture is pathognomonic — a high-specificity pattern raises concern, it does not by itself prove abuse, and the diagnosis rests on a balanced assessment of the history, the mechanism, the pattern, the developmental stage and the family context. Second, specificity outranks sensitivity: the question for an examiner is never "is this fracture seen in abuse?" but "how strongly does this fracture, in this child, point away from an accidental explanation?" [1] [3]
This leaf owns the fracture patterns, the biomechanics, the skeletal-survey protocol and the multi-domain assessment. Cross-link the safeguarding-recognition leaf for the forensic and mandatory-reporting pathway, the abusive-head-trauma leaf for the intracranial and retinal injury that travels with skeletal injury, and the bone-fragility leaf for the osteogenesis imperfecta differential — do not clone those chapters here. [4] [8]
Classification
Classify the fracture before you classify the child, and rank every fracture along three axes: how specific the pattern is for abuse, what mechanism would produce it, and what the child's developmental stage allows. A spiral femur fracture means one thing in a non-ambulatory infant and quite another in a cruising toddler. [1] [5]
By fracture specificity for abuse
| Specificity | Fracture patterns | Why |
|---|---|---|
| High | Classic metaphyseal lesion (corner / bucket-handle); posterior or postero-lateral rib; scapula; spinous process; sternum | Rare in accidental trauma; classic inflicted-force mechanism |
| Moderate | Multiple fractures; bilateral fractures; fractures of differing age; complex or wide skull fracture | Volume and pattern exceed a single accidental event |
| Low (common) | Clavicular (birth / positional); linear parietal skull; femur in cruising toddler; supracondylar humerus | Frequently accidental; concerning only with an incompatible history |
The high-specificity row is the heart of the topic. Kemp's systematic review placed posterior rib fractures and the classic metaphyseal lesion at the top of the specificity ladder; Karmazyn's series of 930 surveyed children confirmed that uncommon fractures — scapular, spinous, sternal — cluster in the abused population and should prompt a search rather than reassurance. [1] [12]
By mechanism
| Mechanism | Typical fracture | Biomechanics |
|---|---|---|
| Shearing / acceleration-deceleration | Classic metaphyseal lesion | Limb grasped and shaken; shear across the zone of provisional calcification |
| Direct blow or thoracic squeeze | Rib, scapular, sternal | Compression; rib levers over the transverse process |
| Traction and twisting | Spiral / oblique long-bone | Rotational force along the shaft |
| Short fall onto a flat surface | Simple linear parietal skull | Low-energy impact; rarely a high-specificity pattern |
A mechanism classification protects you from two errors. It stops you labelling a plausible, low-energy fall as suspicious simply because a fracture exists, and it stops you accepting an impossible mechanism for a high-specificity pattern. The fracture must match the force, and the force must match the child's mobility. [2] [16]
By the child's developmental stage
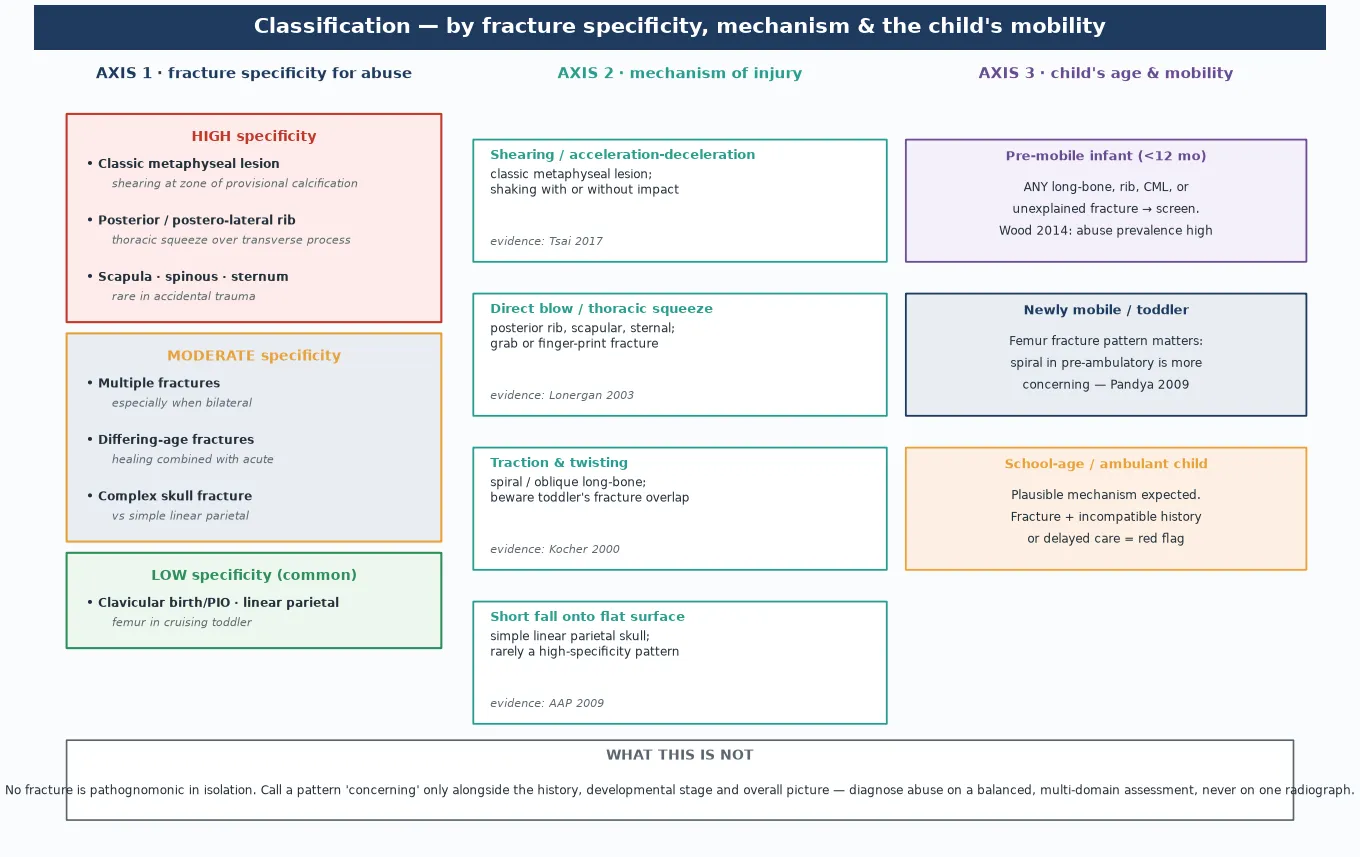
A pre-mobile infant cannot generate the force to fracture a long bone, so any unexplained fracture in a non-ambulatory child carries weight. A spiral femur in a pre-ambulatory infant is far more concerning than a transverse femur in a school-age child who fell from a bike. The developmental stage is not a footnote — it is a diagnostic test in itself. [5] [10]
Pre-mobile infant versus the ambulant child
- Cannot generate sufficient force to break bone
- Any unexplained long-bone, rib or metaphyseal fracture is concerning
- Femur fracture: high abuse prevalence in this group
- Skeletal survey and head imaging are indicated
- Plausible mechanisms exist for many fractures
- Pattern and history become the discriminators
- Toddler's fracture and supracondylar humerus are common and often accidental
- Concerning only with an incompatible or changing story
Epidemiology & Risk Factors
Fractures are the second commonest manifestation of physical abuse after bruising. Across the literature, roughly one in three abused children has a fracture at some point, and a substantial fraction present with the fracture as the first recognised injury — the sentinel presentation that, if missed, is followed by more severe injury. The candidate who treats the fracture and forgets the child has failed the topic. [1] [16]
The site and pattern of the fracture carry the epidemiological signal, not the fracture itself. Rib fractures — especially posterior and postero-lateral — and the classic metaphyseal lesion carry the highest specificity; the Kemp review found that the more posterior a rib fracture, the higher the probability of inflicted cause. Simple linear skull fractures and clavicular fractures are common in accidental and birth trauma and add little specificity in isolation. [1] [3]
Long-bone fractures in the very young deserve particular caution. Wood's systematic review confirmed that the prevalence of abuse among young children presenting with a femur fracture falls steeply with age: the younger and less mobile the child, the higher the likelihood that the fracture is inflicted. A femur fracture in a non-ambulatory infant is a mandate to evaluate for abuse, not an incidental finding. [10]
What amplifies concern from "a fracture exists" toward "this is likely inflicted"? Repeated injury, fractures of differing age, an inconsistent or changing history, delay in presentation, injury in a pre-mobile child, the presence of other inflicted-injury markers such as patterned bruising, and a family context of domestic violence or supervisory neglect. Protective alternative explanations — a witnessed, developmentally plausible mechanism with a consistent history — must be weighed, not assumed. [1] [16]
The yield of a skeletal survey is itself age-dependent. Lindberg's multicentre data showed that the yield of occult fractures on skeletal survey is high in infants under two years referred to abuse specialists and falls with age, which is why the survey is recommended for any child under 24 months with suspected inflicted injury and considered selectively in older children. [11]
Pathophysiology
Return to the six-month-old. The mechanism that produced her spiralled femur was not a sofa roll; it was a rotational force applied to a limb while she was held. Understanding how inflicted force creates the hallmark lesions is what lets a candidate defend a high-specificity reading of a radiograph, rather than merely naming it. [2] [7]
The classic metaphyseal lesion
The classic metaphyseal lesion (CML) — historically the "corner" or "bucket-handle" fracture — is a shearing injury through the zone of provisional calcification, the weak cartilaginous interface between the physis and the primary spongiosa of the metaphysis. When the limb is grasped and accelerated or decelerated — as in shaking — the immature metaphysis shears off a fragment of bone, producing the radiographic corner or bucket-handle fragment. [3] [7]
Tsai and colleagues used a finite-element model of the immature skeleton and showed that the lesion is reproduced only by the acceleration-deceleration forces of shaking, not by simple falls. That biomechanics paper is the single strongest evidence the candidate can cite that the CML is an inflicted-force lesion, and it anchors the mechanism in physics rather than assertion. [7]
The CML must be distinguished from the radiographic mimic of rickets and metabolic bone disease. Perez-Rossello's study of infants with fatal abusive head trauma and classic metaphyseal lesions found frank rachitic change to be absent — which is the evidence the candidate cites against the reflexive "it was rickets" defence without dismissing genuine bone fragility where it exists. [8] [9]
Posterior rib fractures
Posterior rib fractures arise from thoracic compression. When the chest is squeezed or compressed during shaking, the rib is levered over the transverse process of the vertebra, fracturing it at the rib neck — the postero-lateral and posterior arc. This lever mechanism explains why the more posterior the rib fracture, the higher its specificity for abuse, and why the anterior rib fractures of cardiopulmonary resuscitation occupy a different, lower-specificity position. [3] [6]
Maguire's systematic review addressed the forensic question directly: cardiopulmonary resuscitation, even when performed correctly and repeatedly, rarely causes rib fractures in children. The candidate who is challenged with "could CPR have done this?" cites that review and answers that posterior rib fractures in an infant without a credible high-force explanation remain highly concerning. [6]
Healing, dating and the differing-age fracture
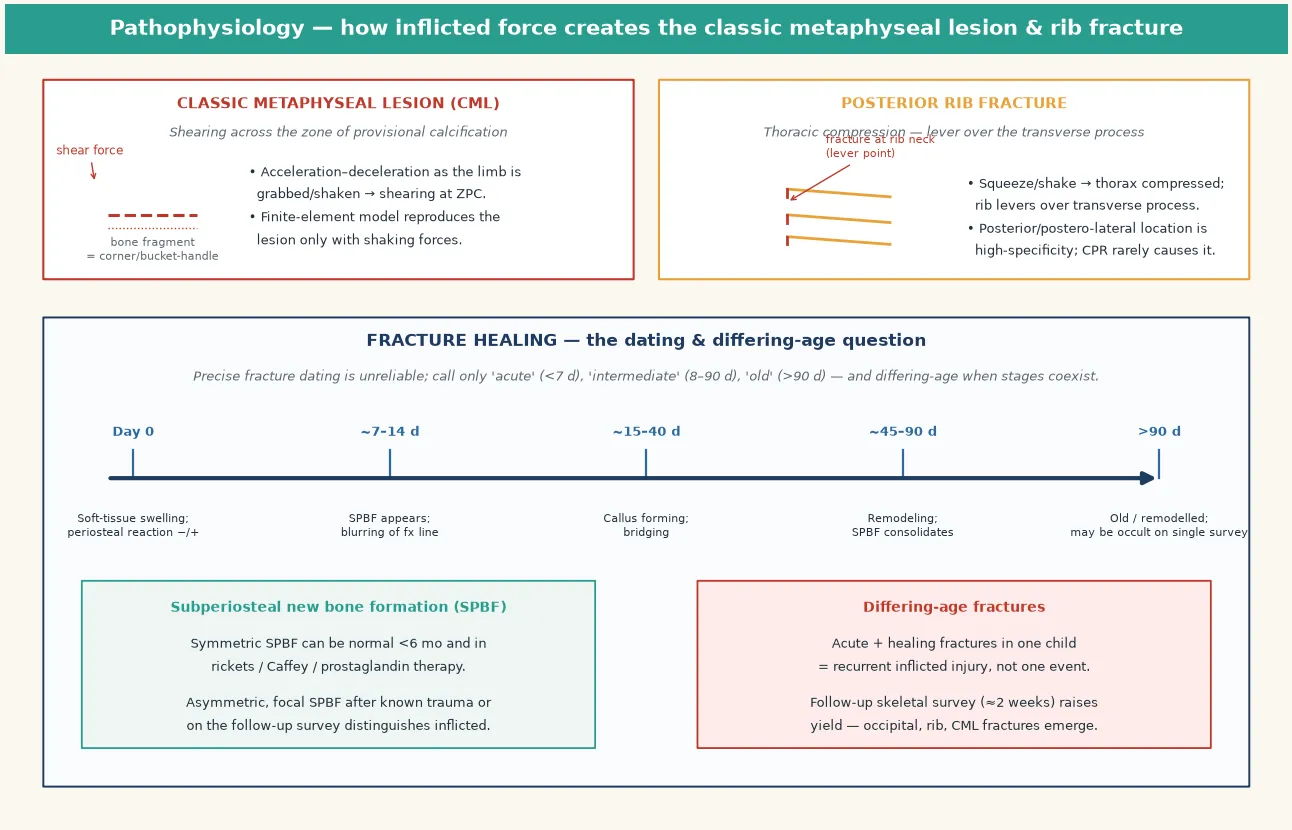
Fracture healing follows a sequence the candidate must know in outline: soft-tissue swelling in the first days, subperiosteal new bone formation from about seven to fourteen days, callus formation over the following weeks, and remodelling over months. The clinical point is not to date a fracture to the day — precise dating is unreliable — but to separate fractures into acute (under a week), intermediate (one to three months) and old, and crucially to recognise differing-age fractures when healing and acute lesions coexist. [3] [14]
Differing-age fractures — an acute fracture alongside a healing one in the same child — are the radiographic signature of recurrent inflicted injury, not a single event. They raise concern precisely because two injuries at different healing stages cannot come from one accidental moment, which is why the follow-up skeletal survey, which reveals fractures that mature into visibility, is part of the protocol rather than an afterthought. [14] [15]
Clinical Presentation
Children with inflicted skeletal injury do not present with "I have been hurt"; they present with the injury and its story, and your job is to weigh the two. The hallmarks are a fracture whose mechanism does not fit, a history that is absent, changing, or inconsistent between carers, and a delay in seeking care for a painful injury that a vigilant carer would have brought earlier. [1] [16]
The developmental mismatch is the most powerful single clue. A non-ambulatory infant with a long-bone, rib, or metaphyseal fracture has an injury that exceeds what their own mobility can generate. A spiral long-bone fracture in a pre-mobile child implies a rotational force applied to the limb — a force that must have come from outside the child. The story must explain how an external rotational force reached a child who cannot move. [2] [10]
Look deliberately for the company the fracture keeps. Patterned or staged bruising, a torn frenulum, retinal haemorrhages, an altered conscious state, or abdominal signs point to additional inflicted injury — abusive head trauma and intra-abdominal injury travel with skeletal injury, and the fracture may be the most visible of several injuries. A child who looks well may still harbour an occult head or abdominal injury. [4] [5]
Sentinel presentations matter. An apparently minor injury — a single bruise in a non-mobile infant, a torn frenulum, an oral injury — that precedes a fracture is evidence of escalating inflicted injury over time, and a missed sentinel is a missed opportunity to prevent the next, more severe injury. Always ask about and document previous injuries, presentations, and welfare contacts. [1] [16]
Differential Diagnosis
Build the differential in layers: the bone-fragility and metabolic disorders, the normal variants, the accidental mechanisms, and the medical conditions that radiographically mimic inflicted injury. Excluding these honestly is what distinguishes a defensible safeguarding assessment from a reckless accusation. [2] [8]
| Differential | Favours | Distinguishing feature |
|---|---|---|
| Osteogenesis imperfecta | Recurrent fractures, blue sclera, family history, osteopenia | Genetic testing; type and distribution differ; rarely produces a posterior rib or classic metaphyseal lesion pattern |
| Rickets / vitamin D deficiency | Broad metaphyseal fraying, cupping, osteopenia, dietary risk | Biochemistry (calcium, phosphate, ALP, vitamin D); rachitic change, not discrete CML |
| Preterm osteopenia of prematurity | Extremely preterm infant, fractures after minimal handling | History of extreme prematurity, mineralisation failure |
| Infantile cortical hyperostosis (Caffey) | Irritability, swelling, systemic features, mandibular involvement | Bilateral, symmetric cortical thickening; self-limiting |
| Normal variant physiologic SPBF | Symmetric, fine, under six months, well infant | Symmetric and non-focal; no discrete fracture line |
| Accidental trauma in a mobile child | Witnessed, plausible, consistent mechanism | Mechanism matches force and developmental stage |
| Birth trauma | Clavicular or humeral fracture in a newborn | Resolves; no ongoing pattern; documented birth detail |
Osteogenesis imperfecta is the differential most often raised in defence and the one the candidate must address with precision. The brittle-bone diseases produce recurrent fractures, but the fracture distribution, the presence of osteopenia, the family history, the blue sclera and dentinogenesis imperfecta, and genetic testing all help separate genuine OI from inflicted injury. A high-specificity pattern such as a posterior rib fracture or a classic metaphyseal lesion in an otherwise well, non-osteopenic infant points away from OI. [8] [9]
The rickets defence is the other common claim and must be met with evidence rather than assertion. Perez-Rossello's histomorphometric study showed rachitic change to be absent in infants with fatal abusive head trauma and classic metaphyseal lesions — which means the reflexive "the fractures are rachitic" argument is not supported when the radiograph shows discrete CMLs rather than diffuse metaphyseal fraying. Genuine rickets has a biochemical and dietary footprint; investigate it where the picture fits. [8]
Clinical & Bedside Assessment
The assessment is multi-domain by design: the history, the developmental assessment, the injury and skin examination, the family and social context, and the search for associated injuries. No single domain makes or breaks the diagnosis — the balanced assessment does. [1] [5]
History
Take the history from each carer separately where possible and document it verbatim. The mechanism described must be weighed against the force required to produce the fracture and against the child's developmental stage. Probe for a changing story, an absent witness, a delay in presentation, and previous injuries or welfare contact. A history that does not fit the fracture is itself a finding. [2] [16]
Examination
Examine the whole child, not only the injured limb. Chart every bruise, abrasion and scar on a body map — patterned bruising, grab-mark bruising, and bruising in a non-mobile infant are themselves concerning. Look in the mouth for a torn frenulum or oral injury, examine the abdomen for tenderness suggesting visceral injury, and assess the nervous system for any sign of abusive head trauma. Record growth, demeanour, and the interaction between child and carer. [4] [5]
Developmental and social assessment
Anchor the mechanism to the child's developmental stage explicitly. A child who cannot crawl cannot "fall down stairs" alone. Take a focused social history — household composition, carers and their supervision, domestic violence, substance use, prior child-protection contact — without turning the clinical encounter into an interrogation. Your role is to assess and to document objectively; the child-protection team determines thresholds. [1] [16]
What to weigh in the assessment
Investigations
Imaging is the core investigation, and the skeletal survey is the single most important study. Treat it as a forensic examination performed to a protocol, not a casual set of films — done badly, it misses the occult fractures the diagnosis depends on. [4] [13]
The skeletal survey
The complete skeletal survey comprises separate frontal and oblique views of every bone — skull, chest (with oblique rib views), spine, pelvis, and each long bone, hand and foot — performed by a radiographer experienced with infants. The American Academy of Pediatrics and the ACR Appropriateness Criteria both set this as the standard for any child under 24 months with suspected inflicted injury, and selectively in older children. [4] [13]
The yield of occult fractures on a skeletal survey is highest in the youngest infants. Lindberg's multicentre study showed the yield falls with age, which is why the survey is mandatory in the under-twos and discretionary beyond, and why an apparently "single" fracture in an infant is never the end of the imaging story. [11] [12]
The follow-up skeletal survey
The follow-up skeletal survey, performed at about two weeks, is not optional. Harper's study of child-abuse paediatricians confirmed that repeat surveys are widely used and add diagnostic information; Hansen's work showed that even a limited-view follow-up survey detects fractures that mature into visibility as they heal — occult rib, classic metaphyseal and extremity fractures that were invisible on the initial films. [14] [15]
The mechanism is fracture healing: an undisplaced or subtle fracture that is radiographically occult on day one becomes visible as subperiosteal new bone and callus form. A single initial survey therefore under-counts injuries, and the differing-age fractures that emerge on the follow-up study are themselves diagnostic of recurrent inflicted injury. [3] [14]
Neuroimaging, ophthalmology and laboratory differentials
In every infant under 12 to 24 months with suspected inflicted injury, add a CT head to exclude abusive head trauma and a dilated retinal examination by ophthalmology to look for retinal haemorrhages — these travel with skeletal injury and may be occult. Laboratory tests exclude the differential rather than confirm the diagnosis: calcium, phosphate, alkaline phosphatase and vitamin D for rickets; a screen for osteogenesis imperfecta where the picture fits; and inflammatory markers where infection is plausible. [4] [8]
Management — Resuscitation
The fracture may be the presenting problem, but the child may carry a more dangerous hidden injury. Resuscitation comes first: airway, breathing and circulation, adequate analgesia, splinting or immobilisation of the fracture, and a focused search for abusive head trauma and intra-abdominal injury that can kill while the limb is being cast. [2] [5]
Treat the orthopaedic injury on its merits — reduction, immobilisation, and specialist orthopaedic care exactly as you would for an accidental fracture of the same type. The fact that an injury may be inflicted does not diminish the child's right to expert musculoskeletal management; it adds the safeguarding layer on top. [2]
A fractured infant is a vulnerable infant in a vulnerable family. Ensure a safe place of care during the workup — admission if there is any doubt about safety, supervision, or the reliability of follow-up — and do not discharge an infant with a high-specificity fracture before the skeletal survey is complete and a safety plan is in place. [4] [13]
Management — Definitive & Stepwise
The definitive pathway runs from recognition through to a closed safeguarding loop. Each step has a named owner, and the loop is not closed until the child has a safe disposition, a completed imaging workup, and a follow-up plan. [4] [13]
The safeguarding pathway
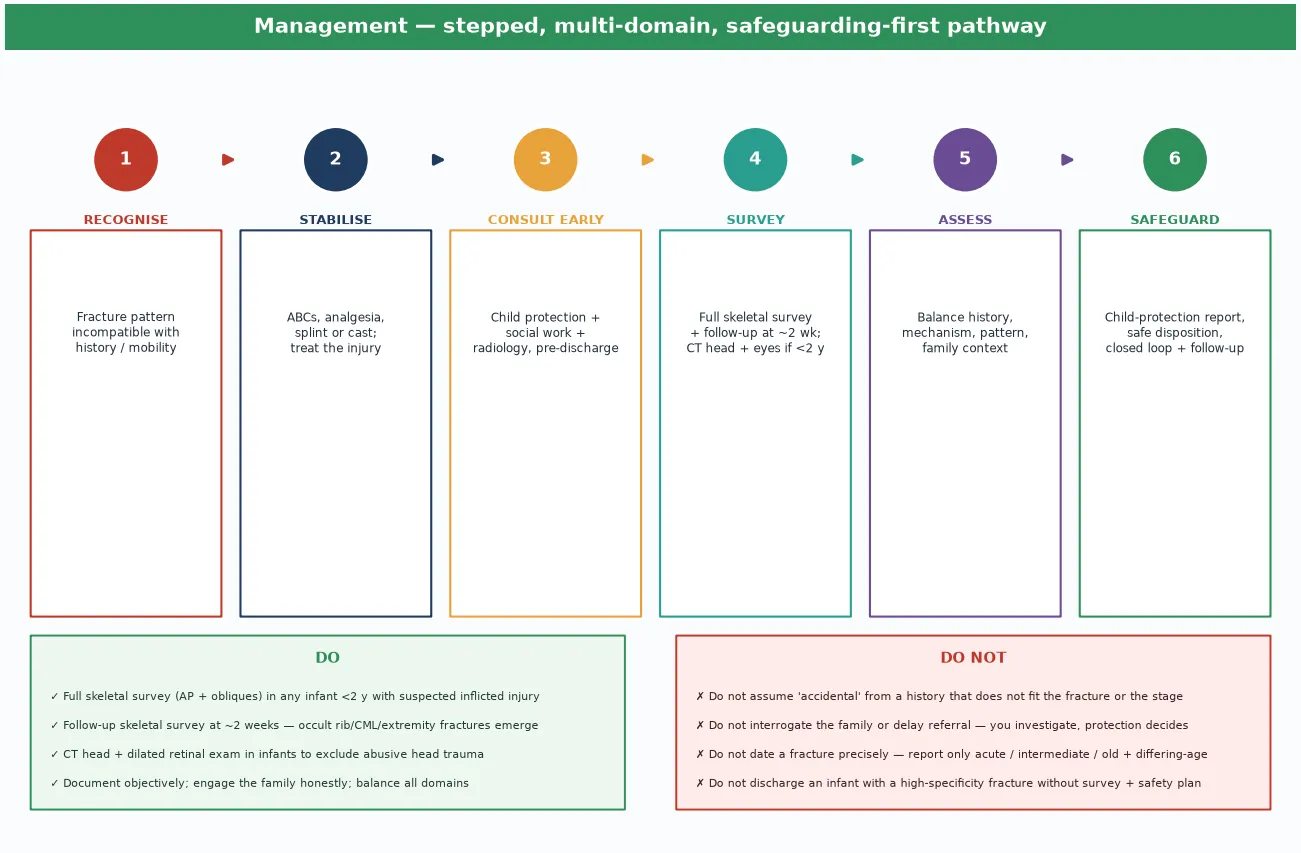
Engage the family honestly and without accusation. Explain that the injury pattern requires further tests to ensure the child is safe and that child-protection involvement is a standard part of that process. Do not interrogate, do not coach, and do not delay referral while waiting for certainty — the threshold for a child-protection referral is concern, not proof. [1] [16]
Exclude the differentials in parallel, not in series. Run the bone-fragility and rickets biochemistry alongside the imaging workup so that a genuine medical diagnosis is neither missed nor used as a reflexive defence. Document the differential reasoning explicitly; a balanced assessment that excludes OI and rickets on evidence is far stronger than one that ignores them. [8] [9]
Specific Subtypes & Scenarios
The classic metaphyseal lesion
The CML is the radiographic signature of shearing inflicted force at the metaphysis, seen as a corner or bucket-handle fragment at the distal femur, proximal or distal tibia, or proximal humerus. In an infant, it is a high-specificity lesion; cite the Tsai finite-element work for the mechanism and the Perez-Rossello study against the rickets defence. [7] [8]
Posterior rib fractures
A posterior or postero-lateral rib fracture in an infant is among the most specific skeletal indicators of abuse, produced by the lever mechanism of thoracic compression. Distinguish it from the anterior rib fractures occasionally seen with prolonged or repeated CPR, and cite Maguire's systematic review that CPR rarely fractures ribs in children. [3] [6]
The femur fracture in the pre-mobile infant
A femur fracture in a non-ambulatory infant mandates an abuse evaluation. Wood's systematic review established the age-dependent abuse prevalence; the pattern matters — spiral in a pre-ambulatory child implies rotational force applied externally — and the developmental stage, not the fracture type alone, drives the level of concern. [5] [10]
Skull fractures
A simple linear parietal skull fracture from a short fall onto a flat surface is low-specificity and common; a complex, wide, depressed, or growing fracture, or a fracture with an incompatible mechanism, raises concern. Always pair the skull radiograph with neuroimaging in the infant to exclude abusive head trauma. [3] [4]
The occult fracture on the follow-up survey
A fracture that is invisible on the initial skeletal survey and emerges on the two-week follow-up is common and important. These occult fractures — ribs, classic metaphyseal lesions, and subtle extremity fractures — change both the fracture count and the differing-age pattern, and a follow-up survey that is never booked is a follow-up survey that fails the child. [14] [15]
Sibling assessment
When one child in a household is identified with inflicted injury, the siblings must be assessed — including a skeletal survey for infant siblings — because inflicted injury is a household phenomenon, not an individual one. The ExSTRA and sibling-screening data underpin this practice. [11]
Complications & Pitfalls
The complications fall into two camps: the harm done by missing the diagnosis, and the harm done by getting it wrong. A missed inflicted fracture is followed, too often, by a more severe injury or a fatality that the sentinel fracture could have prevented. An over-called case damages a family, erodes trust, and delays the right diagnosis if a medical condition was the true cause. [1] [16]
The commonest investigative pitfall is relying on a single, incomplete skeletal survey. An inadequate survey under-counts fractures, misses the occult rib and classic metaphyseal lesions, and forfeits the differing-age pattern that secures the diagnosis. The follow-up survey is the corrective, and omitting it is a recognised system failure. [14] [15]
The commonest diagnostic pitfalls are twin and opposite. The first is accepting an implausible mechanism because a fracture "could" occur in accidental trauma, ignoring that the question is specificity, not possibility. The second is reflexively labelling a low-specificity fracture as inflicted because abuse is "common," without weighing the mechanism, the developmental stage, and the differentials. Both errors collapse the balanced assessment the topic demands. [1] [8]
Missing the company the fracture keeps is a third pitfall. Treating the limb and discharging the child without a CT head, a retinal examination, and an abdominal assessment leaves abusive head trauma and intra-abdominal injury undiscovered — injuries that carry the mortality the fracture does not. The fracture is often the most visible of several injuries, and it is the entry point to a whole-child assessment. [4] [5]
Prognosis & Disposition
The prognosis of an individual fracture is usually good — children's bones heal, and most inflicted fractures unite with appropriate orthopaedic care. The prognosis of the child, however, is governed by whether the inflicted-injury process is recognised and interrupted. A recognised sentinel fracture followed by a closed safeguarding loop offers the chance to prevent recurrence; a missed one does not. [1] [14]
Recurrence risk is the central prognostic fact. An infant sent home from a fracture encounter without recognition of inflicted injury carries a real risk of further, more severe injury, and the follow-up skeletal survey often reveals fractures of differing age that reframe the original presentation as a recurrent pattern rather than a single event. [14]
Disposition is safeguarding-led and multidisciplinary. A safe place of care is confirmed before discharge — admission, supervised contact, or an alternative carer as the assessment requires — and the plan names the responsible clinician, the child-protection report, the booked follow-up survey, and the return precautions. An open-loop discharge is the disposition failure to avoid. [4] [13]
Special Populations
Preterm and osteopenic infants
Preterm infants, particularly those born extremely early, may have osteopenia of prematurity and sustain rib and long-bone fractures from minimal handling. The fracture pattern, the extreme-prematurity history, the biochemical and radiographic osteopenia, and the clinical context separate genuine osteopenia-related fractures from inflicted injury — and a preterm infant is not exempt from abuse, so the two must be weighed together. [2] [8]
Children with disability and non-ambulatory older children
Children with cerebral palsy, neuromuscular disorders, or profound disability who remain non-ambulatory into older childhood share the developmental-stage logic of the pre-mobile infant: an injury that their own mobility cannot generate demands an external mechanism, and the safeguarding threshold is correspondingly lower. Osteopenia from immobility adds a fragility layer that must be assessed honestly. [2]
Out-of-home care and prior welfare contact
Children in out-of-home care, and those with prior child-protection contact, carry a heightened baseline risk, and a fracture in this group is assessed with a lower threshold for a skeletal survey and a safeguarding pathway. The history of placement, supervision, and prior injury is part of the assessment, not background colour. [1] [16]
Indigenous, migrant and socioeconomically disadvantaged families
Indigenous children are over-represented in child-protection data across ANZ, North America and Canada, a product of colonial history, socioeconomic disadvantage, and systemic bias. Migrant and refugee families may face language, trust, and navigation barriers. The candidate must hold two truths at once: safeguarding thresholds apply equally to every child, and the assessment must be culturally safe, interpreter-supported, and free of the bias that over-calls abuse in some families and under-calls it in others. [1]
Siblings and the household
Inflicted injury is a household phenomenon. When one child is identified, the siblings — especially infant siblings — must be assessed and surveyed, because the discovery in one child is evidence about the environment in which the others live. [11]
Evidence, Guidelines & Regional Differences
The evidence base is unusually strong for a safeguarding topic, anchored by the Kemp systematic review of fracture patterns and refined by biomechanical, multicentre and survey-yield studies. The candidate should know where the evidence is robust and where it is deliberately hedged. [1] [13]
Guidelines
The American Academy of Pediatrics statement on diagnostic imaging of child abuse sets the skeletal-survey standard — a complete survey for any child under 24 months with suspected inflicted injury, selectively in older children, with a follow-up survey at about two weeks. The ACR Appropriateness Criteria for suspected physical abuse in a child align with and extend this, specifying when to add CT and MRI. [4] [13]
The Royal College of Radiologists and RCPCH guidance in the United Kingdom, and the equivalent ANZ guidance, converge on the same protocol — a complete, high-quality skeletal survey with oblique rib views and a repeat survey — with minor regional differences in the precise age cut-offs and the use of radionuclide bone scans as an adjunct. The protocol is the candidate's to reproduce; the jurisdiction-specific reporting thresholds are the child-protection team's to apply. [4] [14]
Controversies
Two honest controversies belong in a fellowship answer. The first is fracture dating: precise dating is unreliable, and radiology reports should confine themselves to acute, intermediate, old, and differing-age rather than a spurious exact date. The second is the role of the radionuclide bone scan, which is sensitive for early stress fractures but less specific and operator-dependent, and has been largely superseded by the high-quality skeletal survey plus follow-up. [3] [14]
Regional differences
Mandatory-reporting law varies by jurisdiction — mandated in some ANZ states and Canadian provinces, discretionary in others — but the clinical threshold to refer does not. The candidate names the local pathway and the principle: where there is concern for inflicted injury, a child-protection referral is made, and the legal mandate follows rather than leads the clinical duty. [1] [16]
[4] [13]Exam Pearls
- No fracture is pathognomonic — call specificity, not diagnosis; the balanced multi-domain assessment makes the call. [1]
- Specificity ladder: classic metaphyseal lesion, posterior rib, scapula, spinous process, sternum at the top; clavicular and linear skull at the bottom. [1] [12]
- Pre-mobile infant: any unexplained fracture in a non-ambulatory child demands a skeletal survey and an abuse evaluation — developmental stage is a diagnostic test. [10] [11]
- The follow-up survey is mandatory — occult rib, CML and extremity fractures emerge at two weeks and reveal the differing-age pattern. [14] [15]
- CML mechanism: shearing at the zone of provisional calcification, reproduced only by shaking in the finite-element model (Tsai). [7]
- Posterior rib mechanism: thoracic compression levers the rib over the transverse process; CPR rarely fractures ribs (Maguire). [3] [6]
- Femur fracture in a young child: abuse prevalence falls with age — highest in the non-ambulatory infant (Wood). [10]
- Rickets defence: histomorphometry shows rachitic change is absent in fatal AHT with CMLs — meet the defence with evidence (Perez-Rossello). [8]
- Skeletal survey age cut-off: mandatory under 24 months, selective beyond; yield falls with age (Lindberg). [11]
- Whole-child assessment: CT head, retinal examination, abdominal assessment — the fracture is the entry point, not the whole story. [4] [5]
- You investigate; child protection decides — document objectively, never interrogate, and close the loop with a named owner. [16]
References
- [1]Kemp AM, Dunstan F, Harrison S, Morris S, Mann M, Rolfe K, Datta S, Thomas DP, Sibert JR, Maguire S Patterns of skeletal fractures in child abuse: systematic review. BMJ, 2008.PMID 18832412
- [2]Kocher MS, Kasser JR Orthopaedic aspects of child abuse. J Am Acad Orthop Surg, 2000.PMID 10666649
- [3]Lonergan GJ, Baker AM, Morey MK, Boos SC From the archives of the AFIP. Child abuse: radiologic-pathologic correlation. Radiographics, 2003.PMID 12853657
- [4]Section on Radiology, American Academy of Pediatrics Diagnostic imaging of child abuse. Pediatrics, 2009.PMID 19403511
- [5]Pandya NK, Baldwin K, Wolfgruber H, Christian CW, Drummond DS, Hosalkar HS Child abuse and orthopaedic injury patterns: analysis at a level I pediatric trauma center. J Pediatr Orthop, 2009.PMID 19700994
- [6]Maguire S, Mann M, John N, Ellaway B, Sibert JR, Kemp AM Does cardiopulmonary resuscitation cause rib fractures in children? A systematic review. Child Abuse Negl, 2006.PMID 16857258
- [7]Tsai A, Coats B, Kleinman PK Biomechanics of the classic metaphyseal lesion: finite element analysis. Pediatr Radiol, 2017.PMID 28721473
- [8]Perez-Rossello JM, McDonald AG, Rosenberg AE, Tsai A, Kleinman PK Absence of rickets in infants with fatal abusive head trauma and classic metaphyseal lesions. Radiology, 2015.PMID 25688889
- [9]Thackeray JD, Wannemacher J, Adler BH, Lindberg DM The classic metaphyseal lesion and traumatic injury. Pediatr Radiol, 2016.PMID 26902299
- [10]Wood JN, Fakeye O, Mondestin V, Rubin DM, Localio R, Feudtner C Prevalence of abuse among young children with femur fractures: a systematic review. BMC Pediatr, 2014.PMID 24989500
- [11]Lindberg DM, Berger RP, Reynolds MS, Alwan RM, Harper NS, Examining Siblings To Recognize Abuse Investigators Yield of skeletal survey by age in children referred to abuse specialists. J Pediatr, 2014.PMID 24630357
- [12]Karmazyn B, Lewis ME, Jennings SG, Hibbard RA, Hicks RA The prevalence of uncommon fractures on skeletal surveys performed to evaluate for suspected abuse in 930 children: should practice guidelines change? AJR Am J Roentgenol, 2011.PMID 21700979
- [13]Wootton-Gorges SL, Soares BP, Alazraki AL, Anupindi SA, Blount JP, Booth TN, Cassady CI, Coley BD, Garber M, Hayes LL, Karmazyn B, Kearns SC, Meyer JS, Palasis S, Roberts CC, Rozzelle CJ, Saigal G, Sokoloff AE, Tatum GH, Expert Panel on Pediatric Imaging ACR Appropriateness Criteria Suspected Physical Abuse-Child. J Am Coll Radiol, 2017.PMID 28473090
- [14]Harper NS, Lewis T, Eddleman S, Lindberg DM, ExSTRA Investigators Follow-up skeletal survey use by child abuse pediatricians. Child Abuse Negl, 2016.PMID 26342432
- [15]Hansen KK, Keeshin BR, Flaherty E, Newton A, Passmore S, Prince JS, Puffer RC Sensitivity of the limited view follow-up skeletal survey. Pediatrics, 2014.PMID 25070311
- [16]Maguire S Which injuries may indicate child abuse? Arch Dis Child Educ Pract Ed, 2010.PMID 20926622