Paeds · child-safety-and-social-paediatrics
Intimate partner violence and its impact on children
Also known as Domestic violence and children · Child exposure to intimate partner violence · Family violence and child outcomes · Coercive control and child harm · Witnessing domestic abuse
Fellowship topic on intimate partner violence (IPV) and its impact on children: the four pathways of exposure (direct witness, auditory, aftermath, coercive control), global prevalence and the 30 to 70 percent co-occurrence with child maltreatment, the toxic-stress / HPA-axis cascade that makes witnessing violence an adverse childhood experience with a dose-response to adult disease, the heterogeneous presenting patterns (externalizing, internalizing, somatic, developmental, direct co-victimization), the differential from ADHD, ODD, ASD and anxiety, trauma-informed enquiry and validated screening (HARK, HITS), the immediate safety assessment with lethal-means restriction, the child-protection reporting threshold, referral of the non-offending parent to IPV services without blame, trauma-focused therapy (TF-CBT), the buffering-adult recovery model, and ANZ/UK/US/Canada guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seven-year-old boy is referred to your clinic for "behavioural problems and possible ADHD." His teacher reports aggression, distractibility, and emotional outbursts that began six months ago. His mother seems tense and deflects questions about home life. During a separate interview, the boy asks quietly whether you can "make the shouting stop at night." That single sentence reframes the entire presentation — this is not ADHD; this is a child living with intimate partner violence, and the behavioural symptoms are the trauma speaking through his body. [2] [9]
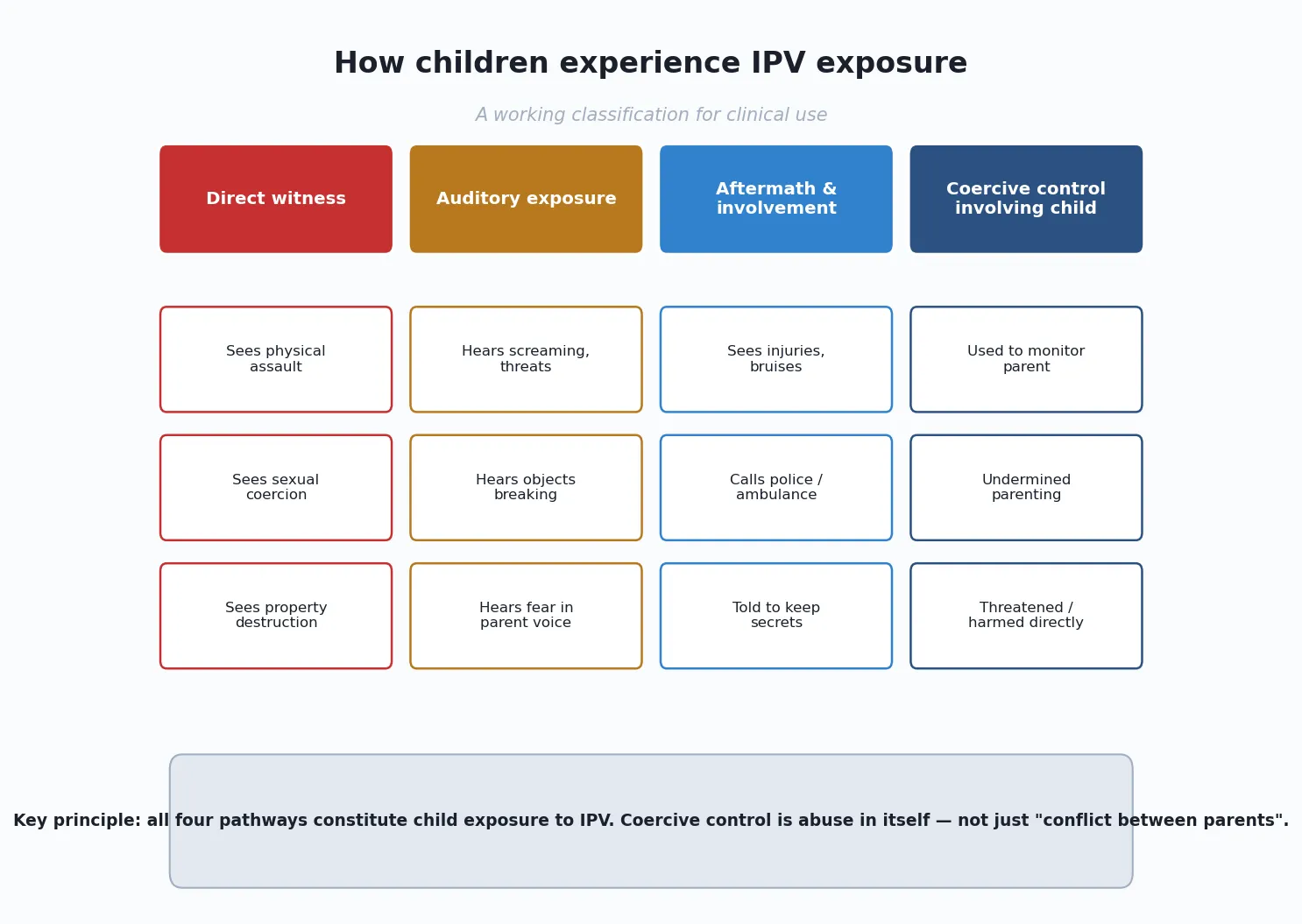
Intimate partner violence is any behaviour within an intimate relationship that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse, and controlling behaviours. The controlling behaviours — isolating the partner from friends and family, monitoring their movements, controlling finances, threatening, humiliating — are called coercive control, and they are abuse in themselves. When we say a child is "exposed" to IPV, we mean something broader than witnessing a physical assault. The child may see it directly, hear it from another room, see the aftermath (injuries, fear, broken objects, police), or be used as an instrument of coercive control — forced to monitor the victim, carry messages, or witness the degradation of their parent. [1] [2]
Why should a paediatrician care about something that happens "between the parents"? Three reasons. First, the co-occurrence rate of IPV and direct child maltreatment is 30 to 70 per cent — the violence rarely stays between the adults. Second, the exposure itself is harmful: witnessing IPV is classified as an ACE because it activates the same toxic-stress cascade as being hit, and it carries a dose-response relationship to adult disease. Third, the presentations are common and heterogeneous — behavioural, developmental, somatic, psychiatric — and the child will reach your clinic through the front door of those symptoms long before anyone names the violence. [2] [11] [12]
Classification
Sort the exposure by which pathway brought the harm to the child, because the pathway determines both the child's risk profile and your documentation. The child does not need to be in the same room, and does not need to see the assault, for the exposure to be real and damaging. [2] [9]
The four working pathways are the taxonomy to hold. Direct witness means the child sees the physical or sexual assault, the destruction of property, or the verbal humiliation in person. Auditory exposure means the child hears the violence — screaming, threats, objects breaking — from another room, often at night, and may lie awake terrified without ever seeing the event. Aftermath involvement means the child sees the consequences: the parent's injuries and bruises, the fear and hypervigilance, the police visit, the broken furniture, the hurried departure. Coercive control involving the child means the perpetrator weaponises the child — forcing them to monitor the victim, undermining the victim's parenting authority, turning the child against the victim, or directly threatening or harming the child as leverage. [2] [9]
Two further distinctions matter. The first is direct co-victimization: in many IPV homes, the child is also physically or sexually abused, and the boundary between "exposure" and "direct maltreatment" dissolves. The second is the severity and chronicity of the exposure: a single acute episode carries a different risk profile from years of coercive control, and both are harmful. The deepest classification question is whether the child is safe now — and that is the question the safety-assessment section is built to answer. [10] [13]
Epidemiology & Risk Factors
How common is IPV, and how many children live in its shadow? The global prevalence is large and the under-detection gap is the central epidemiological fact. A WHO multi-country meta-analysis estimated that roughly one in three women worldwide experience physical or sexual IPV in their lifetime, with regional variation but no region spared. In high-income countries, a substantial minority of children are exposed to IPV each year — US survey data from the National Survey of Children's Exposure to Violence showed that a significant proportion of children and adolescents had witnessed or been exposed to partner violence in the home. [1] [8]
The co-occurrence data are what should change a clinician's practice. Where IPV is present in the home, the rate of direct child maltreatment — physical abuse, sexual abuse, neglect, emotional abuse — is 30 to 70 per cent, depending on the study and the definition. The reverse is also true: where child maltreatment is identified, the rate of co-occurring IPV is high. This bidirectional co-occurrence is the epidemiological basis for the rule that finding one mandates looking for the other. A clinician who identifies IPV but does not screen the children, or who identifies child abuse but does not assess the parental relationship, is missing a large proportion of the harm. [2] [12]
Risk clusters at multiple levels, and none of these factors is diagnostic or causal in itself — most families with risk factors never experience IPV. Parent and family factors include a perpetrator's attitudes justifying control, substance use, and a personal history of witnessing or experiencing violence in childhood (the intergenerational thread). Community and structural factors include poverty, housing instability, neighbourhood violence, social isolation, and gender inequality. The structural framing matters clinically: IPV is not caused by a parent's "choice of partner" or a family's socioeconomic status. It is caused by the perpetrator's behaviour, and the clinician's job is to hold the perpetrator accountable while supporting the victim and protecting the child. [1] [12]
Why this matters for prognosis is the dose-response relationship. The more forms and the more chronic the adversity — including witnessing IPV — the worse the adult health outcome, and that relationship is the epidemiological bridge to the mechanism below. [11] [13]
Pathophysiology
Why does hearing your parent being hurt harm a child for life? The answer is the biology of toxic stress, and it is the mechanism an examiner must hold because it explains why a child who was "never hit" can carry lifelong cost. [11] [9]
A child's stress response is healthy when it is brief and buffered. When a threat passes and a responsive adult comforts the child, the cortisol and adrenergic surge settles, and the brain records a safely mastered challenge. IPV removes the buffer in the most damaging way possible: the threat comes from within the caregiving environment, and the adult the child would turn to for comfort is the victim, unavailable or unable to protect. The stress response stays activated for months and years. That sustained activation is toxic stress, and it recalibrates the developing hypothalamic-pituitary-adrenal (HPA) axis, produces chronically elevated or dysregulated cortisol, dysregulates the immune system, and alters the architecture of the brain — especially the limbic circuits governing fear and emotion, and the prefrontal circuits governing attention, impulse control and executive function. [11] [9]
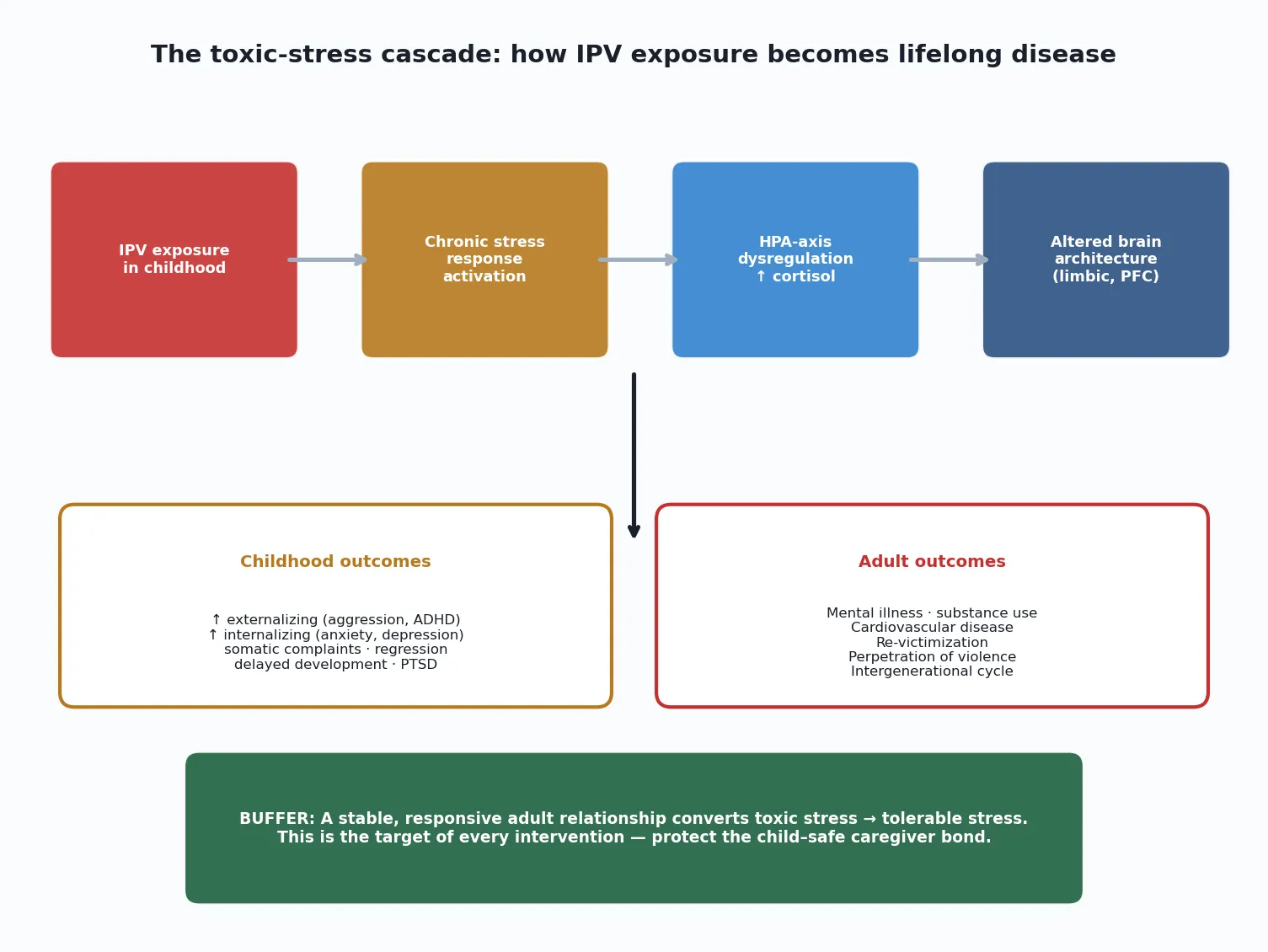
The same cascade produces the adult disease associations that make the ACE literature so consequential. The Adverse Childhood Experiences study showed a graded relationship between the ACE score — which counts witnessing a mother being treated violently — and the leading causes of adult death, including ischaemic heart disease, as well as mental illness, substance use and suicide risk. The mechanism is dose-response: more cumulative adversity, including more exposure to IPV, means more downstream disease. The poly-victimisation literature adds that children exposed to IPV are at elevated risk of multiple other forms of victimisation, compounding the dose. [11] [13] [10]
The most important therapeutic implication is that a stable, responsive adult relationship is the buffer that converts toxic stress into tolerable stress. In the IPV context, that adult is usually the non-offending parent. That is why the response to IPV exposure is not only to stop the violence but to protect and support the bond between the child and the safe caregiver — through supporting the non-offending parent, securing safety, and arranging trauma-focused therapy. Mechanism and management meet here: the biology of harm is also the biology of recovery. [11] [9]
Clinical Presentation
What you will see is heterogeneous, and the absence of a single "signature" presentation is itself the key clinical fact. A child exposed to IPV may present through behavioural, developmental, somatic, psychiatric, or direct-injury pathways — and the same child may cycle through several of these over years. The cardinal rule is to take a trauma history before assigning a primary diagnosis. [2] [9]
Externalizing presentations are the most common reason for referral. The child shows aggression toward peers and adults, conduct problems, impulsivity, inattention, and difficulty with emotional regulation. These children are frequently referred for "ADHD" or "ODD" assessment, and the trauma history is the thing that distinguishes a trauma-driven phenotype from a primary neurodevelopmental one. The symptoms often emerged or worsened after a period of family stress, are worse in certain settings, and coexist with hypervigilance, exaggerated startle, and sleep disturbance. [3] [4]
Internalizing presentations include anxiety, depression, social withdrawal, low self-esteem, and emotional regression. The child may become clingy, fearful, or emotionally flat, and younger children may show regression in toileting, speech or sleep. Somatic presentations include recurrent headaches, abdominal pain, enuresis, sleep disturbance, and nonspecific complaints that bring the child to primary care repeatedly without an organic cause. Developmental presentations include delayed milestones, language delay, and school difficulties — the child may be falling behind academically because chronic stress impairs attention, sleep, and learning. [2] [9]
Direct co-victimization is the presentation that must never be missed. The child who is exposed to IPV may also be directly physically or sexually abused, and the injury or disclosure brings the family to attention. Disclosure may come from the child — a sentence like "daddy hits mummy" or "I hear shouting at night" — or from the non-offending parent. Record any disclosure verbatim, do not interrogate, and take it at face value. The atypical presentations are deliberately examined: a well-looking child may be living in chronic fear; an adolescent girl's new risk-taking may signal re-victimization; and a non-offending parent's evasiveness may reflect active coercive control rather than disinterest. [8] [13]
Differential Diagnosis
The differential is the gate that protects both directions of the error: missing the trauma by labelling it ADHD or ODD, and over-attributing primary neurodevelopmental conditions to trauma when both may coexist. The aim is to separate by features you can test at the bedside and on careful history. [2] [9]
Versus ADHD. Primary ADHD is persistent across all settings from early childhood, with no temporal link to family stress and no trauma history. Trauma-driven inattention and impulsivity often emerged or worsened after family stress, are situational, and coexist with hypervigilance, sleep disturbance, and regression. The two can coexist, so taking a trauma history does not exclude ADHD — but failing to take one means you may treat the symptom while the cause continues. [2] [4]
Versus ODD and conduct disorder. Primary ODD is a persistent pattern of negativistic, defiant and hostile behaviour toward authority figures. Trauma-driven aggression is often episodic, linked to triggers that echo the traumatic context (loud noises, perceived threat, separation), and may coexist with anxiety, hypervigilance and emotional dysregulation rather than pure defiance. [9]
Versus anxiety disorder, ASD, and learning disability. Anxiety disorders, ASD, attachment disorders, and learning disability may all present with overlapping features (inattention, social withdrawal, rigidity, school difficulty). The discriminating features are the temporal relationship to family stress, the presence of trauma-specific features (hypervigilance, re-experiencing, avoidance), the developmental history, and the family context. A child with ASD can also be exposed to IPV — the diagnoses are not mutually exclusive, and holding both is the clinical skill. [2] [9]
Clinical & Bedside Assessment
The assessment must be trauma-informed, unhurried, and structured to allow disclosure without endangering the non-offending parent or the child. Three principles govern the encounter: screen privately, document safely, and never press in front of the partner. [2] [9]
Interview the parent alone and the child alone. The non-offending parent will rarely disclose IPV in front of the perpetrator, and a child will rarely disclose if they fear consequences. Separation is a prerequisite for honest disclosure, not an option. Use open, non-judgemental framing: "Many families experience stress or conflict at home, and I ask all families about this because it affects children's health. Has anything like this been happening in your family?" [2]
H.A.R.K. — four questions that open the door to disclosure
Document safely. Never write a disclosure of IPV in a record that the perpetrator can access (a shared patient portal, a letter given to the family, or notes that the perpetrator may demand to see). Use the child's record, note that the information is sensitive, and coordinate with social work and child protection before any documentation reaches the family. A disclosure that triggers retaliation against the non-offending parent or child is a clinical failure as serious as missing the disclosure. [2] [9]
Assess immediate safety. Ask: Is the violence escalating? Are there weapons or firearms in the home — the single strongest predictor of intimate partner homicide? Has the child been directly threatened or harmed? Does the non-offending parent have a safe place to go? Does the parent have an escape plan? The answers determine whether the child and parent leave the encounter to a place of safety or return to an assessed risk. [5] [2]
Investigations
IPV exposure is a clinical diagnosis. There is no blood test or scan that confirms it, and the role of investigations is to identify co-occurring harm, exclude mimics, and establish a baseline for developmental and mental-health follow-up. Never delay safety or reporting to complete investigations. [2]
Core assessment when IPV exposure is identified in a child
Screen for direct child maltreatment: take a full trauma-informed history, examine top-to-toe for injuries, and apply the TEN-4-FBCP bruising rule to any bruise in a young child.
Perform developmental screening (e.g. ASQ, M-CHAT as age-appropriate) to establish a baseline and detect delay.
Screen mental health with a validated tool such as the Strengths and Difficulties Questionnaire (SDQ) to quantify externalizing and internalizing burden.
Arrange a skeletal survey if there is any suspicion of direct physical abuse, following the same protocol as for suspected non-accidental injury.
Screen the non-offending parent for acute injury and unmet health need, and offer STI screening and pregnancy testing where relevant.
Establish whether the child and parent have a safe place to go and whether an escape plan exists.
The rationale for each stream is specific. Screening for direct maltreatment is driven by the 30 to 70 per cent co-occurrence rate: you are looking for the abuse that travels with the exposure. Developmental screening establishes a baseline because chronic toxic stress impairs development, and serial screening tracks recovery. Mental-health screening quantifies the symptom burden, supports referral to trauma-focused therapy, and gives you an outcome measure. Skeletal survey follows the standard non-accidental-injury protocol when there is any suspicion of direct physical abuse — the threshold is the same as for any suspected abuse presentation. [12] [9]
Management — Resuscitation
The immediate priority is physical safety for the child and the non-offending parent. If the perpetrator is present or nearby, if weapons are accessible, or if the child has been directly threatened or harmed, the encounter moves from assessment to safety intervention without delay. [2] [5]
Lethal-means restriction is the single most time-critical act. Ask about firearms and other weapons in the home. If present, work with the family, social work and, where necessary, law enforcement to remove or secure them before the family leaves the encounter. The presence of firearms in an IPV home dramatically raises the risk of fatal outcome for the victim and the children, and this risk is modifiable. [5]
Ensure a safe disposition. If the child or non-offending parent is in immediate danger, they should not return to the home. Engage social work, the IPV advocacy service, and child protection to arrange a place of safety, and document the reasoning explicitly. If the family is safe to leave, agree a written safety plan: where they will go if violence escalates, who they will call, and a code word or signal the child can use. Provide the local IPV helpline number and the national domestic-violence line in a form the perpetrator will not see. [2] [9]
Do not require the non-offending parent to leave the relationship as a condition of your support. Leaving is the period of highest danger for IPV victims, and the decision is theirs. Your job is to offer options, reduce the lethal-means risk, protect the child, and stay engaged — not to impose a timeline on a parent who is under coercive control. [2]
Management — Definitive & Stepwise
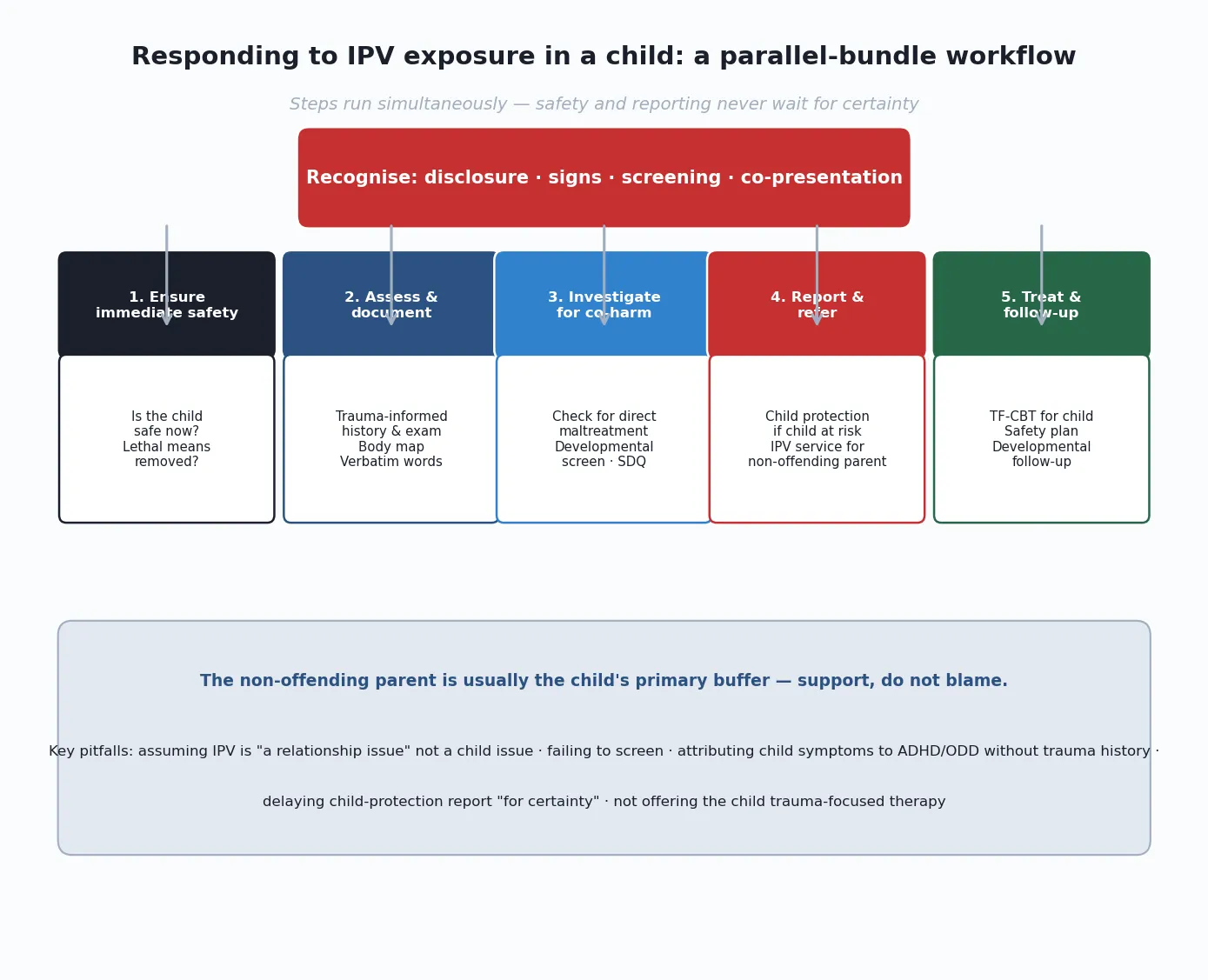
The definitive response is a bundle run in parallel. Ensure safety, assess and document, investigate, report and refer, treat and follow up — these proceed at the same time, and the two that examiners most often see delayed are the child-protection report (left until "after certainty") and the referral of the non-offending parent to advocacy services (left until "after the relationship ends"). Neither waits. [2] [9]
Make the child-protection report when you form a reasonable belief that the child is at risk of significant harm. Exposure to IPV is itself a form of harm — the toxic-stress cascade is the mechanism — and in many jurisdictions the threshold is met when a child is living in a home with ongoing IPV, particularly where there is coercive control, escalation, weapons, or direct threats to the child. Know your local statute and threshold, but hold the clinical principle: reporting rests on a reasonable belief of risk, not on diagnostic certainty, and the child's safety is not negotiable while you wait for proof. [12] [2]
Refer the non-offending parent to IPV advocacy services. Advocacy services — refuges, counselling, legal support, safety planning — are among the most effective interventions for IPV victims, and they are the parent's route to safety. Offer the referral without blame, without requiring the parent to leave the relationship, and in a way the perpetrator cannot intercept. Supporting the non-offending parent is supporting the child, because the parent is usually the child's primary buffer. [2] [5]
Arrange trauma-focused therapy for the child. Trauma-focused cognitive behavioural therapy (TF-CBT) is the first-line, evidence-based therapy for children who have experienced trauma, including IPV exposure. It targets the trauma-specific features (re-experiencing, avoidance, negative cognitions, arousal) and works with the safe caregiver to rebuild the buffering relationship. Arrange developmental and mental-health follow-up, engage the school, and document the plan with explicit handover to the named professionals who carry it. [9] [2]
In Australia and New Zealand, mandatory-reporting obligations for child exposure to IPV vary by state and territory. The RACP and the colleges hold all paediatricians to a duty to report a reasonable belief that a child is at risk of significant harm, and exposure to ongoing IPV with coercive control, escalation, weapons, or direct threats to the child meets that threshold in most jurisdictions. Notify the statutory child-protection authority, involve the hospital social work and child-protection team, and refer the non-offending parent to the state or national family-violence service (1800 RESPECT in Australia, 0800 456 450 Shine Safehouse or Are You OK in Aotearoa New Zealand). [2]
Specific Subtypes & Scenarios
IPV exposure in an infant or toddler presents as regression, feeding difficulty, sleep disturbance, excessive crying, and developmental delay. The infant is too young to disclose verbally, so the presentation is through the caregiver (who may be the victim) and through the developmental trajectory. The key is to take a trauma history whenever a young child presents with unexplained regression or distress, and to screen the parent for IPV in a private interview. The buffering adult is especially critical at this age because the brain is most plastic. [7] [9]
IPV exposure in a preschooler brings magical thinking and self-blame: the child may believe the fighting is their fault, and this cognition drives shame, withdrawal and aggression. Trauma-focused therapy at this age targets the self-blame cognition and works through the safe caregiver. [9]
IPV exposure in a school-age child presents through behaviour and school performance. The child may be aggressive, inattentive, anxious, or socially withdrawn, and is frequently referred for ADHD or ODD assessment. Taking a trauma history is the discriminator, and misattributing trauma to a primary neurodevelopmental diagnosis is the classic exam-stem error. [2] [4]
IPV exposure in an adolescent carries the additional risk of dating violence and re-victimization. Adolescent girls exposed to IPV are at elevated risk of experiencing violence in their own relationships, and adolescents of both genders may show risk-taking, substance use, self-harm, running away, and school disengagement. Balance confidentiality with the duty to protect, and address the adolescent's own relationship safety directly. [8] [10]
The non-offending parent who is reluctant to disclose or leave is the scenario examiners reward most. Coercive control makes disclosure dangerous, and leaving is the period of highest risk. Do not press, do not blame, do not set leaving as a condition of your support. Offer the advocacy referral, reduce the lethal-means risk, protect the child, document safely, and stay engaged over time. The parent's readiness to act is not the trigger for your duty to the child. [2]
Pregnancy and the postnatal period are high-risk windows for IPV escalation, and screening every pregnant adolescent and young parent is recommended. IPV during pregnancy is associated with adverse maternal and infant outcomes, including preterm birth, low birthweight, and impaired attachment. The antenatal and postnatal encounter is an opportunity for identification and referral that should not be missed. [7]
Complications & Pitfalls
Missing the trauma by labelling the symptoms is the most common and most consequential pitfall. A child with aggression, inattention, or anxiety is referred for ADHD, ODD or anxiety assessment, the trauma history is never taken, and the child receives a neurodevelopmental or psychiatric label while the cause — ongoing IPV — continues. The defence is the routine trauma history: ask every child with behavioural, developmental, or emotional symptoms about family stress and safety. [2] [9]
Treating IPV as "a relationship issue" rather than a child-safety issue is the parallel failure. IPV in the home is not merely conflict between adults; it is a toxic-stress exposure for the child, a strong predictor of co-occurring maltreatment, and a child-protection concern. Failing to frame it as a child issue means the child is left in the exposure. [2] [12]
Documentation that endangers the non-offending parent is a pitfall that is easy to cause and devastating in effect. A disclosure recorded in a shared portal or a letter the perpetrator can access can trigger retaliation. Document in the child's record, mark it sensitive, and coordinate with social work before any information reaches the family. [2]
Delaying the child-protection report to "be certain" is a recurring and serious error. Reporting rests on a reasonable belief of risk, and the child's safety is not negotiable while you wait for proof. Report, complete the workup in parallel, and document. [12] [2]
Failing to screen for co-occurring maltreatment misses the 30 to 70 per cent of IPV homes where the child is also directly abused. Finding IPV mandates examining the child for injuries, applying the bruising rule, and ordering a skeletal survey when suspicion is raised. [12]
Prognosis & Disposition
The protective factor with the strongest evidence is a stable, responsive adult relationship, and in the IPV context that adult is usually the non-offending parent. Intervention is designed to protect and support that bond: securing safety, supporting the parent through advocacy services, and arranging trauma-focused therapy that works through the caregiver. Where the child cannot remain safely with the non-offending parent, placement with kin or a foster family preserves the relational buffer better than an institutional setting. [11] [9]
The long-term prognosis follows the dose-response curve of cumulative adversity: more forms and more chronic exposure predict worse adult mental and physical health, including mental illness, substance use, cardiovascular disease, and re-victimization. Intergenerational transmission is a real risk: children who witness IPV are at elevated risk of perpetrating or experiencing IPV in adulthood. But timely recognition, consistent support, and trauma-focused therapy improve the trajectory, and the buffering-adult mechanism is where the biology of harm meets the biology of recovery. [11] [10]
Disposition spans place-of-safety placement when home is unsafe, structured outpatient follow-up for developmental and mental-health needs, school engagement, and a clear re-presentation pathway. The safety-net is explicit: a written safety plan, the IPV helpline, primary-care and school engagement, and a fixed follow-up date so that deterioration is caught early. [2] [9]
Special Populations
Aboriginal and Torres Strait Islander, Maori and other Indigenous children are over-represented among children exposed to family violence, reflecting structural determinants including colonisation, intergenerational trauma, socioeconomic disadvantage, and under-resourced services. Provide culturally safe, trauma-informed care, engage Indigenous health workers and family, and do not conflate disadvantage with individual risk. The violence is the perpetrator's behaviour; the response addresses both the immediate safety and the structural context. [2]
Refugee and migrant families may face additional barriers to disclosure and help-seeking, including language, immigration status, fear of authorities, and isolation. Use professional interpreters (never a family member), and be aware that the perpetrator may use immigration status as a tool of coercive control. [2]
Children with disability or chronic illness are over-represented among children exposed to IPV and may be less able to disclose or self-protect. Recognise behavioural change and distress as the equivalent of disclosure, adapt assessment to the child's communication, and hold a higher index of suspicion rather than attributing distress to the disability. [12]
Rural and remote families face reduced access to refuges, advocacy services, and child-protection response, and the perpetrator's social isolation is amplified by geography. Telehealth follow-up, coordination with local services, and explicit safety planning are essential. [2]
Adolescents require a careful balance of confidentiality and the duty to protect. Screen for dating violence in adolescents of both genders, address relationship safety directly, and manage the consent, confidentiality and sexual-health needs that arise. Adolescent girls exposed to IPV are at elevated risk of re-victimization and warrant targeted support. [8] [10]
Evidence, Guidelines & Regional Differences
The evidence base for the impact of IPV on children rests on a coherent body of meta-analytic and epidemiological work. The Kitzmann meta-analysis of child witnesses to domestic violence found that exposed children showed worse outcomes than non-exposed children across social, emotional and behavioural domains, at a magnitude comparable to children who were directly physically abused. The Wolfe meta-analysis and critique reached similar conclusions while noting methodological limitations in the early literature, particularly around defining exposure and controlling for co-occurring maltreatment. The Holt review of the literature synthesised the evidence across age groups and outcome domains, establishing the breadth and dose-response of the impact. [3] [4] [2]
The health-services and cost evidence reinforces the clinical case. Rivara and colleagues showed that children living in homes with IPV had higher health-care utilisation and costs than children in non-violent homes, and Bonomi and colleagues showed the adult health burden in women with IPV exposure. The ACE study and its successors established that witnessing IPV in childhood is an adverse childhood experience with a graded, dose-response relationship to the leading adult causes of death, and the poly-victimisation literature showed that IPV exposure rarely occurs in isolation. [5] [6] [11] [10]
Kitzmann meta-analysis: child witnesses to domestic violence
Population: Children exposed to interparental violence, compared with non-exposed and directly abused children
Key finding
Exposed children showed significantly worse social, emotional and behavioural outcomes than non-exposed children, at a magnitude comparable to directly abused children.
Practice change
Witnessing IPV is not a benign 'secondhand' exposure — it carries a harm burden approaching direct abuse. The child does not need to be hit to be harmed.
The regional guideline structure is consistent in principle and varies in statute. In ANZ, the RACP provides family-violence guidance, each jurisdiction sets its own mandatory-reporting law and threshold, and national services (1800 RESPECT in Australia, Shine/Are You OK in Aotearoa New Zealand) provide advocacy. In the UK, the RCPCH safeguarding framework and the statutory "Working Together" guidance set the standard, and the Domestic Abuse Act 2021 recognises children exposed to IPV as victims in their own right. In the US, the AAP recommends routine IPV screening in paediatric settings, and state-by-state mandated-reporter laws apply. In Canada, the RCPSC holds a child-maltreatment competency, and each province imposes a duty to report a child at risk. In every region the clinical trigger is the same: a reasonable belief that the child is at risk of harm. [2] [12]
The controversies are real and must be managed with evidence and multidisciplinary review. Universal versus targeted IPV screening in paediatric settings remains debated: the evidence for screening itself is mixed, but the evidence for identification and referral improving outcomes is stronger, and most guidelines recommend at least routine enquiry. The balance between the non-offending parent's confidentiality and the duty to report the child's risk is jurisdiction-specific and ethically demanding. The evidence base for TF-CBT in IPV-exposed children is strong but access-limited, and the gap between evidence and service availability is a systems failure the paediatrician must navigate. [2] [9]
Exam Pearls
- IPV exposure is an adverse childhood experience — witnessing a mother being treated violently counts in the ACE score even when the child is never directly hit. [11]
- The co-occurrence rate of IPV and child maltreatment is 30 to 70 per cent — finding one mandates looking for the other. [2] [12]
- The non-offending parent is usually the child's strongest buffer — support, do not blame, and never set leaving the relationship as a condition of your support. [2]
- HARK asks Humiliation, Afraid, Rape, Kick — four items that open the door to disclosure in a private interview. [2]
- TF-CBT is the first-line evidence-based therapy for trauma-exposed children, and it works through the safe caregiver. [9]
- Firearms in the home are the single strongest predictor of intimate partner homicide — ask and act on lethal means. [5]
- The most common exam-stem error is attributing a trauma-exposed child's symptoms to primary ADHD or OCD without taking a trauma history. [2] [4]
- Pregnancy is a high-risk period for IPV escalation — screen every pregnant adolescent and young parent. [7]
- Never document IPV disclosure in a record the perpetrator can access — it can trigger retaliation. [2]
- In the UK, the Domestic Abuse Act 2021 recognises children exposed to IPV as victims in their own right, not merely as witnesses. [2]
References
- [1]Devries KM; Mak JY; Garcia-Moreno C; et al The global prevalence of intimate partner violence against women. Science, 2013.PMID 23788730
- [2]Holt S; Buckley H; Whelan S The impact of exposure to domestic violence on children and young people: a review of the literature. Child Abuse & Neglect, 2008.PMID 18752848
- [3]Kitzmann KM; Gaylord NK; Holt AR; Kenny ED Child witnesses to domestic violence: a meta-analytic review. Journal of Consulting and Clinical Psychology, 2003.PMID 12699028
- [4]Wolfe DA; Crooks CV; Lee V; McIntyre-Smith A; Jaffe PG The effects of children's exposure to domestic violence: a meta-analysis and critique. Clinical Child and Family Psychology Review, 2003.PMID 14620578
- [5]Rivara FP; Anderson ML; Fishman P; et al Intimate partner violence and health care costs and utilization for children living in the home. Pediatrics, 2007.PMID 18055676
- [6]Bonomi AE; Anderson ML; Rivara FP; Thompson RS Health outcomes in women with physical and sexual intimate partner violence exposure. Journal of Women's Health, 2007.PMID 17903075
- [7]Huth-Bocks AC; Levendosky AA; Bogat GA The effects of domestic violence during pregnancy on maternal and infant health. Violence and Victims, 2002.PMID 12033553
- [8]Finkelhor D; Turner HA; Ormrod R; Hamby SL Prevalence of childhood exposure to violence, crime, and abuse: results from the National Survey of Children's Exposure to Violence. JAMA Pediatrics, 2015.PMID 26121291
- [9]Osofsky JD The impact of violence on children. The Future of Children, 1999.PMID 10777999
- [10]Turner HA; Shattuck A; Finkelhor D; Hamby S Polyvictimization and youth violence exposure across contexts. Journal of Adolescent Health, 2016.PMID 26598060
- [11]Felitti VJ; Anda RF; Nordenberg D; et al Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 1998.PMID 9635069
- [12]Gilbert R; Widom CS; Browne K; Fergusson D; Webb E; Janson S Burden and consequences of child maltreatment in high-income countries. Lancet, 2009.PMID 19056114
- [13]Turner HA; Finkelhor D; Ormrod R Poly-victimization in a national sample of children and youth. American Journal of Preventive Medicine, 2010.PMID 20171535
- [14]Finkelhor D; Ormrod RK; Turner HA Polyvictimization and trauma in a national longitudinal cohort. Development and Psychopathology, 2007.PMID 17241488