Paeds · child-safety-and-social-paediatrics
Intra-oral injury and occult trauma
Also known as Inflicted oral injury · Non-accidental oral trauma · Sentinel oral injury · Occult trauma in suspected child abuse · Torn frenulum in child abuse · Abusive head trauma screening
Fellowship guide to inflicted intra-oral injury and occult trauma in suspected child physical abuse: recognise the sentinel oral signs (torn labial frenum, lip laceration, palatal petechiae, dental trauma), distinguish inflicted from accidental using history consistency and the TEN-4 FACES-B bruising rule, actively screen for occult fractures (skeletal survey under 24 months, repeat at 2 weeks), retinal haemorrhages (dilated ophthalmology), intracranial injury (CT then MRI), and occult abdominal injury (AST/ALT over 80 IU/L triggering CT), cite Maguire and Kemp systematic reviews, Pierce TEN-4 validation, Lindberg transaminase utility, AAP and ACR imaging guidance, and execute the safeguarding pathway with mandatory reporting without discharging the child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
TEN-4 FACES-B — bruising that screams abuse
Overview & Definition
An infant who cannot yet crawl brings a torn upper-lip frenum to the emergency department. The carer says the child fell. The frenum is inside the mouth — an injury a parent cannot see, and one that a hurried clinician may not examine. The question that decides everything is simple and hard: is this accidental, or is this the one visible piece of a larger, hidden pattern of inflicted harm? [3] [5]
Intra-oral injury refers to any injury of the mouth, perioral region, or dental structures — including a torn labial or lingual frenum, lip bruising or laceration (especially the inside surface), palatal or pharyngeal petechiae, buccal mucosal laceration, tongue bite marks, and dental subluxation or avulsion of primary teeth. The American Academy of Pediatrics Committee on Child Abuse and Neglect affirms that oral injuries, particularly a torn frenum, are a recognised manifestation of physical abuse that every physician must actively look for. [5]
Occult trauma is internal injury that is not apparent on surface examination and must be actively sought whenever abuse is suspected. It includes occult fractures (especially the classic metaphyseal lesion and posterior-lateral rib fracture), retinal haemorrhages of abusive head trauma, intracranial injury (subdural and diffuse axonal), and occult abdominal organ injury (liver, spleen, hollow viscus). These injuries coexist with — and are sometimes revealed by — an oral or sentinel injury. The unifying clinical principle is that a sentinel injury is the visible tip of a hidden iceberg. [2] [3]
Your role as the paediatrician is to recognise the sentinel sign, stabilise any life threat, screen for occult injury with a protocolised workup, and refer through the mandatory safeguarding pathway — without discharging the child to an unsafe environment. [3] [5]
Classification
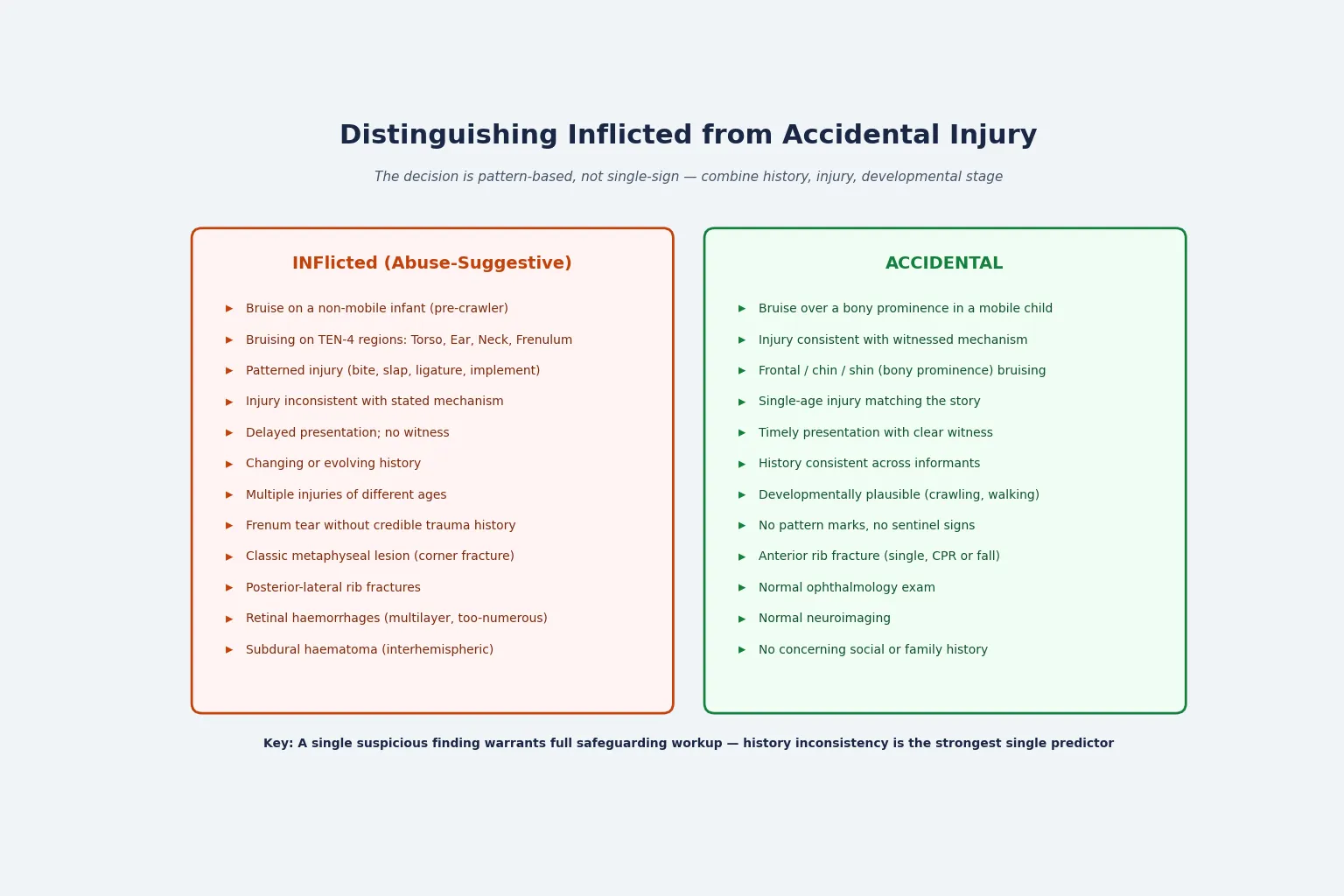
Injuries in suspected child abuse fall into two groups: those you can see (the sentinel or visible injury, which includes the oral injuries) and those you must look for (the occult or hidden injury). The decision between inflicted and accidental is pattern-based: you weigh the history against the injury, the developmental stage, and the constellation of findings. [1] [3]
Sentinel injury types and the occult injuries they demand
Torn labial frenum
- Classic inflicted oral sign from direct blow or forced feeding
- Sentinel: abuse presumed in a non-mobile infant until excluded
- Mimic: accidental dental trauma with a credible mechanism; Riga-Fede disease from natal teeth
- Demands: skeletal survey, head imaging, ophthalmology, liver enzymes, coagulation
Patterned bruising
- TEN-4 FACES-B regions: torso, ear, neck, angle of jaw, cheek, eyelid, sclera
- Any bruise in an infant under 4 months or in a non-mobile child
- Bite marks, slap marks, ligature marks, implement marks
- Demands: full skin exam with body map, occult-trauma screen
Occult fractures
- Highly specific: classic metaphyseal lesion (corner or bucket-handle), posterior-lateral rib, scapular, spinous, sternal
- Detected on skeletal survey in approximately 1 in 5 children under 2 years with concern for abuse
- Repeat skeletal survey at 2 weeks reveals fractures not initially visible
- Demands: full skeletal survey, paediatric radiology review
Abusive head trauma
- Subdural haematoma (often interhemispheric or multilayer), diffuse axonal injury, cervical cord injury
- Multilayer, too-numerous-to-count retinal haemorrhages extending to periphery
- PredAHT score (Cowley 2015) estimates abuse probability from six clinical features
- Demands: CT head acutely, MRI brain and spine for dating and subtle injury, dilated ophthalmology
Occult abdominal injury
- Liver or spleen laceration without external bruising; duodenal haematoma or hollow viscus rupture
- AST or ALT over 80 IU/L is the screen triggering abdominal CT (Lindberg 2009, 2013)
- May present with minimal external signs and delayed shock
- Demands: AST, ALT, lipase, urinalysis; abdominal CT if transaminases raised
Gagging and asphyxia
- Palatal or pharyngeal petechiae, lingual frenum injury, facial plethora
- Subconjunctival haemorrhage from Valsalva or smothering
- Hypoxic-ischaemic injury may be delayed in onset
- Demands: neuroimaging, ophthalmology, respiratory and metabolic assessment
Epidemiology & Risk Factors
Child physical abuse is common and under-recognised. Infants under one year carry the highest rates of abusive head trauma and child homicide, and the pre-verbal, pre-mobile stage is the window in which abuse is easiest to inflict and hardest to detect. Oral injuries are found in a substantial proportion of physically abused children — surveys report oral or perioral injury in up to half or more — yet they are frequently missed because the mouth is not routinely examined or the injury is attributed to a minor accident. [4] [5] [6]
Why oral and occult injury matter — the numbers an examiner rewards
Risk clusters in the child, the carer, and the context. Child risk factors include young age (especially infancy), prematurity, disability or neurodevelopmental condition, and a prior unexplained injury. Carer risk factors include mental illness, substance use, family violence, social isolation, and unrealistic developmental expectations. Contextual factors include socioeconomic stress, housing instability, and lack of support. The single most important clinical signal is a prior sentinel injury that was attributed to accident and not investigated — a recurring theme in child-death reviews and a marker for escalating harm. [3]
Pathophysiology
Inflicted force produces a recognisable map of injury. A direct blow to the face or mouth — a slap, a strike, or forced feeding — tears the delicate maxillary labial frenum, bruises or lacerates the lip, and may subluxate or avulse primary teeth. A gag or object forced into the mouth injures the lingual frenum, palate, or pharynx, producing petechiae and mucosal laceration. The oral cavity is small and the tissues are vascular and unsupported, so even modest force leaves a visible injury. [5] [6]
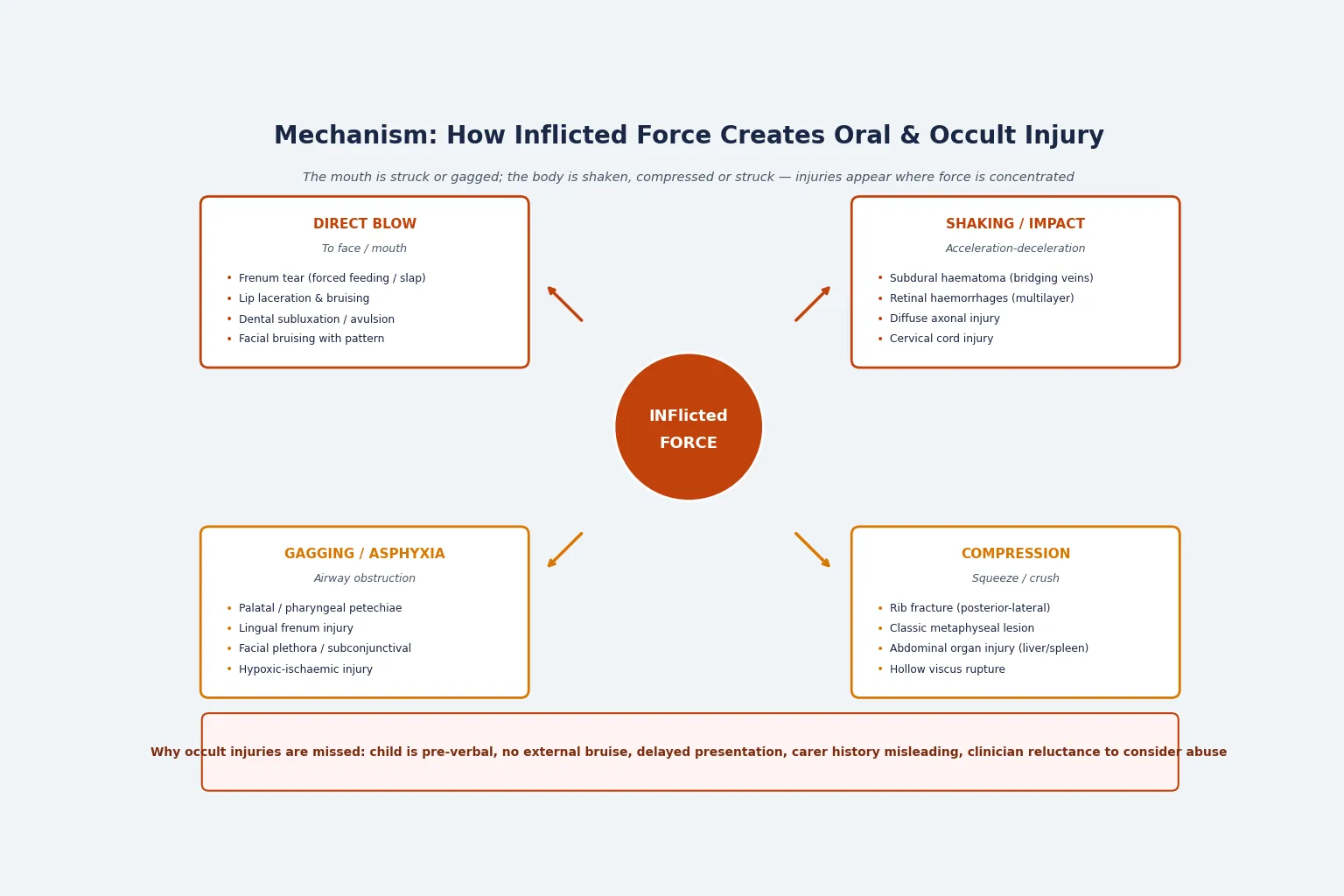
The same episode that injures the mouth often disperses force through the body. Shaking or impact causes acceleration-deceleration: the brain shifts within the skull, shearing the bridging dural veins to produce a subdural haematoma (often interhemispheric), tearing retinal vessels to produce multilayer retinal haemorrhages, and stretching axons to cause diffuse axonal injury. The cervical spine is a vulnerable hinge and may also be injured. Compression — squeezing or crushing the chest or abdomen — levers the rib head against the transverse process, producing the characteristic posterior-lateral rib fracture, and shears the immature trabeculae at the zone of provisional calcification, producing the classic metaphyseal lesion (the corner or bucket-handle fracture). The liver and spleen are also vulnerable to compression without external bruising. [2] [11]
Occult injuries are missed because the child is pre-verbal, there is no external bruise, the presentation is delayed, the carer's history is misleading, or the clinician does not consider abuse. The principle that ties oral and occult injury together is that the visible oral injury is often the only accessible clue to a hidden, life-threatening pattern of harm. [3] [5]
Clinical Presentation
The oral injury is often the presenting complaint, but it may also be an incidental finding during a general examination. Inspect the labial frenum (upper more commonly torn than lower) by gentle retraction of the upper lip; a torn, bruised, or scarred frenum in a non-mobile infant is a sentinel sign. Look for lip bruising or laceration, paying attention to the inside surface of the lip, which may be injured by the teeth from a blow. Palatal or pharyngeal petechiae suggest gagging or forced insertion of an object. Buccal mucosal laceration and tongue bite marks may be visible on careful inspection. Dental trauma — subluxation, luxation, or avulsion of a primary tooth — may accompany direct facial trauma. [4] [5] [6]
Sentinel bruising follows the TEN-4 FACES-B pattern: a bruise on the torso (chest, abdomen, back, buttocks), ear, or neck; any bruise in an infant under 4 months; a frenulum tear; bruise at the angle of the jaw, cheek (corner of mouth), eyelid, or sclera; or bruising in any non-mobile child. A single positive item is a red flag. Bruises are rare in pre-mobile infants — the Maguire systematic review found that any bruise in a non-mobile child is highly suggestive of abuse. [1] [7] [8]
Occult fractures present with no focal sign — a child with suspected abuse but no tender limb may nonetheless have rib, classic metaphyseal, scapular, spinal, or sternal fractures detectable only on skeletal survey. Occult head injury may present with poor feeding, lethargy, irritability, vomiting, seizures, or apnoea — sometimes subtle enough to be attributed to gastroenteritis or sepsis. Occult abdominal injury may present with minimal external signs and delayed shock. The atypical presentation is the trap: a neurologically devastated infant may present only with nonspecific signs, and the carer may attribute it to a minor fall. [3]
Differential Diagnosis
The differential has two jobs: separate inflicted from accidental injury, and exclude medical mimics. Missing a mimic causes a false accusation and devastates a family; missing abuse risks re-injury and death. [3] [5]
| Differential | Discriminators | Why it matters |
|---|---|---|
| Accidental dental or oral trauma | Credible witnessed mechanism; age-appropriate (cruising toddler); bony prominence; single-age injury; consistent history | Over-diagnosis harms an innocent family |
| Bleeding diathesis (ITP, haemophilia, Von Willebrand) | Petechiae, mucosal bleeding, prolonged bleeding history, abnormal coagulation or FBC | Exclude with coagulation and FBC before attributing bruising to abuse |
| Riga-Fede disease | Traumatic ulceration of the ventral tongue or lingual frenum from natal or neonatal teeth; infant age | A recognised non-abuse mimic of lingual frenum injury |
| Osteogenesis imperfecta | Recurrent fractures, blue sclera, family history, characteristic radiographs | A mimic of inflicted fracture; genetic and radiographic evaluation |
| Cultural practices (cupping, coining, moxibustion) | Patterned marks matching the practice; corroborated history | Take a sensitive history; do not accuse prematurely |
| Oral infection (candidiasis, herpetic gingivostomatitis) | Diffuse mucosal involvement, fever, characteristic lesions | Differentiate clinically; culture or swab if unclear |
| Accidental rib fracture (CPR, major fall) | Single anterior rib fracture; witnessed resuscitation or high-energy mechanism | Multiple, posterior, or different-age fractures favour inflicted injury |
Clinical & Bedside Assessment
Assessment begins with the history, not the injury. Take separate interviews of each carer and document their account verbatim with quotations. The most powerful discriminator is a history that is inconsistent with the injury or the child's developmental stage: a pre-crawling baby cannot sustain a frenum tear from rolling; a toddler's fall does not explain posterior rib fractures. Record the stated mechanism, the timing, any delay in presentation, and any inconsistencies between informants or across visits. [3] [8]
Perform a full head-to-toe skin examination including the oral cavity, ears, behind the ears, scalp, frenum, genitalia, and skin folds. Use a body map and photo-document every injury. The oral examination requires gentle retraction of the lips and cheeks to inspect the labial frenum (upper and lower), the inside of the lips, the buccal mucosa, the palate, the tongue, and the oropharynx. Apply the TEN-4 FACES-B bruising rule: bruise on torso, ear, or neck; any bruise under 4 months; frenulum tear; angle of jaw, cheek, eyelid, or sclera; bruising in any non-mobile child. Any positive item is a red flag. [5] [7]
Assess the child's developmental stage explicitly: can the child roll, sit, crawl, cruise, or walk? A bruised, non-mobile infant is a red flag regardless of the stated mechanism. Record the growth parameters and examine for signs of neglect, failure to thrive, or prior injury (scars, old bruises in different colours). [3]
Investigations
Investigations in suspected abuse serve two purposes: to detect occult injury that is not visible on examination, and to exclude medical mimics. The workup is protocolised — it is not optional or guided only by clinical suspicion, because occult injuries are the ones that are missed and that carry the highest morbidity. [2] [14]
The skeletal survey is a complete radiographic series (approximately 20 views including oblique ribs) indicated for all children under 24 months with suspected physical abuse. The AAP Section on Radiology (2009) and the ACR Appropriateness Criteria (2017) reinforce this. A repeat skeletal survey at 2 weeks reveals occult fractures not visible initially — callus formation brings previously occult fractures into view, and the repeat study improves yield substantially. The highest yield is in infants under 6 months (McNamara 2024). [14]
Neuroimaging is indicated for any child with suspected abusive head trauma, altered consciousness, or any abusive injury in an infant under 6 months. CT head is the acute test for subdural haematoma and acute haemorrhage; MRI brain and spine is obtained for injury dating, diffuse axonal injury, and subtle or chronic subdural collections once the child is stable. [11] [13]
Dilated ophthalmology by a specialist is mandatory in suspected abusive head trauma. The characteristic finding is multilayer, too-numerous-to-count retinal haemorrhages extending to the periphery — a pattern rarely seen in accidental injury. [11]
Abdominal screening: AST or ALT over 80 IU/L triggers abdominal CT to detect occult liver injury (Lindberg 2009, 2013). Add lipase for pancreatic injury and urinalysis for genitourinary injury. [9] [10]
Coagulation and FBC exclude bleeding diathesis (ITP, haemophilia, Von Willebrand, leukaemia) before attributing bruising to abuse. Additional tests — toxicology, metabolic, septic — are ordered as the clinical picture demands. [3]
The occult-trauma screen — what every sentinel injury demands
Skeletal survey (approximately 20 views including oblique ribs) for all children under 24 months with suspected abuse — repeat at 2 weeks for occult fractures not initially visible
CT head acutely if suspected abusive head trauma, altered consciousness, or infant under 6 months with any abusive injury; follow with MRI brain and spine when stable
Dilated specialist ophthalmology in all suspected abusive head trauma — look for multilayer retinal haemorrhages extending to the periphery
AST and ALT — if either is over 80 IU/L, perform abdominal CT for occult liver injury; add lipase and urinalysis
Coagulation screen and FBC to exclude bleeding diathesis before attributing bruising to abuse
Additional tests as indicated: toxicology, metabolic, septic workup
Management — Resuscitation
Stabilise the airway, breathing, and circulation first. Oral trauma may compromise the airway by bleeding, oedema, or aspiration; control oral bleeding with direct pressure and position. Occult abdominal or intracranial injury may cause haemorrhagic or neurogenic shock — resuscitate before imaging. Treat the life threat before the safeguarding investigation. [3]
The threshold for a mandatory report is reasonable suspicion, not certainty. In most jurisdictions a treating doctor has a statutory duty to report suspected child abuse to child protection services. Do not wait for the full workup to report — the threshold is met at the point of reasonable concern. Notify a senior clinician and the local safeguarding or child-protection team. Do not confront the carer or make an accusation; the clinician's role is to document, investigate, and report. [5]
Management — Definitive & Stepwise
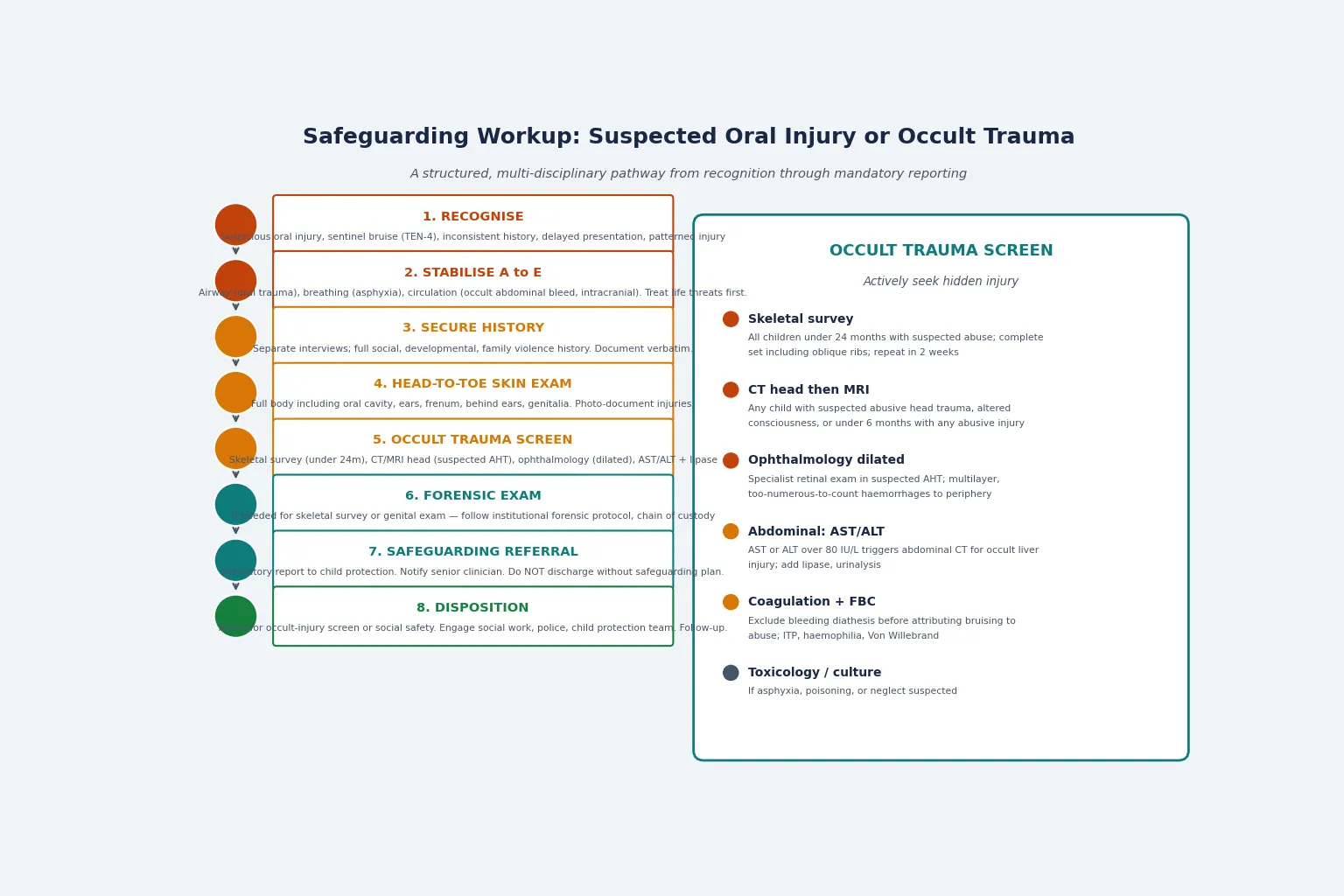
The definitive management is the safeguarding pathway. It runs from recognition through stabilisation, the structured history and skin examination, the occult-trauma screen, the forensic examination if needed, the mandatory report, and the disposition with multi-agency coordination. [3] [14]
The eight-step safeguarding pathway
Step 1 — Recognise: suspicious oral injury, sentinel bruise (TEN-4 FACES-B), inconsistent or changing history, delayed presentation, patterned injury
Step 2 — Stabilise A to E: airway (oral trauma), breathing (asphyxia), circulation (occult abdominal or intracranial bleed)
Step 3 — Secure the history: separate interviews; full social, developmental, family violence and past-mechanism history; document verbatim with quotations
Step 4 — Head-to-toe skin examination including oral cavity, ears, frenum, behind the ears, genitalia; photo-document on a body map
Step 5 — Occult-trauma screen: skeletal survey under 24 months (repeat at 2 weeks), CT head then MRI (suspected AHT), dilated ophthalmology, AST/ALT over 80 IU/L triggering abdominal CT, coagulation and FBC
Step 6 — Forensic examination: if needed for skeletal survey or genital exam, follow institutional forensic protocol with chain of custody
Step 7 — Safeguarding referral: mandatory report to child protection, notify senior clinician, engage social work and police; do not discharge without a plan
Step 8 — Disposition: admit for occult-injury screen or social safety; coordinate multi-agency case conference; schedule follow-up
The PredAHT score (Cowley 2015) estimates the probability of abusive head trauma from six clinical features — intracranial haemorrhage, retinal haemorrhage, rib fracture, long-bone fracture, apnoea, and head or neck bruising — and may guide the threshold for further investigation. It is a probability tool, not a diagnostic label, and must be interpreted in context. [13]
Treat specific injuries in parallel: dental trauma is managed by a dental or oral-maxillofacial team (reimplantation or splinting as appropriate for avulsed teeth); oral lacerations may require repair; fractures are managed by orthopaedics. But the safeguarding pathway runs alongside the medical treatment — it is never deferred to a later visit. [5]
Specific Subtypes & Scenarios
Torn labial frenum. A classic inflicted oral sign, most commonly the maxillary frenum, resulting from a direct blow or forced feeding. In a non-mobile infant, abuse is presumed until excluded. The mimic is Riga-Fede disease — traumatic ulceration of the lingual frenum from natal or neonatal teeth — which is developmental, not inflicted. Exclude accidental dental trauma with a credible mechanism. The frenum tear is one of the "F" items in TEN-4 FACES-B. [5] [8] [12]
Abusive head trauma with retinal haemorrhages. Shaking or impact causes subdural haematoma (often interhemispheric or multilayer), multilayer retinal haemorrhages extending to the periphery, diffuse axonal injury, and possible cervical cord injury. The RCPCH 2018 critique affirms that the abusive head trauma "triad" (subdural haematoma, retinal haemorrhage, encephalopathy), in context, supports a shaking mechanism but must be interpreted with the full clinical picture and not in isolation. [11] [13]
Occult abdominal injury. Liver or spleen laceration without external bruising may present with delayed shock; a duodenal haematoma or hollow viscus rupture is rare but lethal. AST or ALT over 80 IU/L is the screen (Lindberg 2009, 2013) and triggers abdominal CT. [9] [10]
Occult fractures. The classic metaphyseal lesion (corner or bucket-handle fracture) and posterior-lateral rib fracture are highly specific for inflicted injury (Kemp 2008). A repeat skeletal survey at 2 weeks reveals fractures not visible initially (Ravichandiran 2010, McNamara 2024). [2] [14]
Gagging and asphyxia. Palatal or pharyngeal petechiae, lingual frenum injury, facial plethora, and subconjunctival haemorrhage suggest airway obstruction by smothering or gagging. Hypoxic-ischaemic injury may be delayed in onset and subtle in presentation. [3]
Complications & Pitfalls
The most dangerous pitfall is the missed sentinel injury: a torn frenum or a single bruise in a non-mobile infant is dismissed as accidental, the child returns to an unsafe environment, and suffers serious or fatal re-injury. The reciprocal error is over-diagnosis: attributing oral injury or bruising to abuse before excluding a bleeding diathesis, osteogenesis imperfecta, Riga-Fede disease, or an accidental mechanism with a credible history — the family suffers significant and lasting harm. [1] [3]
Other pitfalls include an inadequate occult-trauma screen (failing to obtain a skeletal survey, ophthalmology exam, or liver enzymes in a child with a sentinel injury), discharging before the safeguarding plan is complete, failing to make the mandatory report, and confronting the carer before child protection is engaged. The clinician's role is to document, investigate, and report — not to accuse or investigate criminally. [5]
Prognosis & Disposition
Missed abuse carries a high risk of re-injury and death; a prior sentinel injury is a strong predictor of subsequent serious or fatal abuse. Abusive head trauma carries a heavy burden of long-term disability: cognitive impairment, epilepsy, visual loss, and motor deficits. Early, sustained, multi-agency intervention improves both immediate safety and long-term outcome. [3]
Disposition follows the safeguarding pathway: admit the child for occult-injury screening or for social safety while the plan is made; coordinate a multi-agency case conference involving paediatrics, social work, police, and child protection; and schedule medical, developmental, and safeguarding follow-up. The safety-net is a clear written plan, a follow-up appointment, and a named contact for the family and the child-protection team. [5]
Special Populations
Infants under 6 months carry the highest yield of occult fractures on skeletal survey and warrant the lowest threshold for neuroimaging and ophthalmology — a non-mobile infant with any bruise or oral injury demands full workup. Pre-verbal children cannot give a history; the clinician must rely on injury pattern, carer-history consistency, and active occult-trauma screening. Children with disability or neurodevelopmental conditions have a higher baseline risk of abuse and atypical communication that may mask distress — maintain a high index of suspicion. [3] [14]
Indigenous, migrant, refugee, and asylum-seeker families require culturally safe care, interpreter use, and trauma-informed assessment; avoid bias while maintaining safeguarding vigilance. Children in out-of-home care or youth justice have a higher baseline risk; coordinate with the relevant agency and document carefully. [5]
Evidence, Guidelines & Regional Differences
ANZ. General paediatric and emergency practice follows a structured safeguarding pathway with mandatory reporting under state and territory child-protection legislation (e.g. the relevant Children, Youth and Families Acts in Australia, the Oranga Tamariki Act in New Zealand). RACP and RCPCH child-protection evidence underpin the bruising, fracture, and oral-injury pattern data. Cite local mandatory-reporting thresholds (reasonable suspicion) and institutional child-protection team pathways. Do not invent foreign section numbers — name the jurisdiction's own legislation and tools. [1] [3]
Named evidence stack for viva: bruising patterns (Maguire 2005); skeletal fracture patterns (Kemp 2008); injuries indicating abuse (Maguire 2010); oral and dental aspects of abuse (Kellogg 2005, AAP); orofacial manifestations (Jessee 1995); head, face, mouth injury in abused children (Cairns 2005); TEN-4 FACES-B validation (Pierce 2010, 2021); hepatic transaminase utility (Lindberg 2009, 2013); abusive head trauma triad critique (Debelle and RCPCH 2018); torn frenulum and non-accidental injury (Teece 2005); PredAHT score (Cowley 2015); diagnostic imaging of child abuse (AAP Section on Radiology 2009). [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14]
Exam Pearls
- A torn labial frenum in a non-mobile infant is abuse until excluded — it is the classic sentinel oral sign (Teece 2005, Kellogg 2005). [5] [12]
- TEN-4 FACES-B — Torso, Ear, Neck, under 4 months, Frenulum, Angle of jaw, Cheek, Eyelid, Sclera, Bruising in non-mobile child — validated by Pierce 2010 and 2021. [7] [8]
- Skeletal survey for all children under 24 months with suspected abuse; repeat at 2 weeks for occult fractures (AAP 2009, McNamara 2024). [14]
- Posterior-lateral rib fractures and classic metaphyseal lesions are highly specific for inflicted injury (Kemp 2008). [2]
- AST or ALT over 80 IU/L triggers abdominal CT for occult liver injury (Lindberg 2009, 2013). [9] [10]
- Riga-Fede disease is the non-abuse mimic of lingual frenum injury — caused by natal or neonatal teeth in infants. [3]
- Do not discharge a child with a sentinel injury without a safeguarding plan and a mandatory report; reasonable suspicion, not certainty, is the threshold. [3] [5]
References
- [1]Maguire S, Mann MK, Sibert J, Kemp A. Are there patterns of bruising in childhood which are diagnostic or suggestive of abuse? A systematic review. Arch Dis Child, 2005.PMID 15665178
- [2]Kemp AM, Dunstan F, Harrison S, Morris S, Mann M, Rolfe K, Datta S, Thomas DP, Sibert JR, Maguire S. Patterns of skeletal fractures in child abuse: systematic review. BMJ, 2008.PMID 18832412
- [3]Maguire S. Which injuries may indicate child abuse? Arch Dis Child Educ Pract Ed, 2010.PMID 20926622
- [4]Jessee SA. Orofacial manifestations of child abuse and neglect. Am Fam Physician, 1995.PMID 7484693
- [5]Kellogg N, American Academy of Pediatrics Committee on Child Abuse and Neglect. Oral and dental aspects of child abuse and neglect. Pediatrics, 2005.PMID 16322187
- [6]Cairns AM, Mok JY, Welbury RR. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int J Paediatr Dent, 2005.PMID 16128994
- [7]Pierce MC, Kaczor K, Lorenz DJ, et al. Validation of a Clinical Decision Rule to Predict Abuse in Young Children Based on Bruising Characteristics. JAMA Netw Open, 2021.PMID 33852003
- [8]Pierce MC, Kaczor K, Aldridge S, O'Flynn J, Lorenz DJ. Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics, 2010.PMID 19969620
- [9]Lindberg DM, Shapiro RA, Blood EA, Steiner RD, Berger RP. Utility of hepatic transaminases in children with concern for abuse. Pediatrics, 2013.PMID 23319537
- [10]Lindberg D, Makoroff K, Harper N, Laskey A, Bechtel K, Deye K, Berger R. Utility of hepatic transaminases to recognize abuse in children. Pediatrics, 2009.PMID 19620197
- [11]Debelle GD, Maguire S, Watts P, et al. Abusive head trauma and the triad: a critique on behalf of RCPCH of 'Traumatic shaking: the role of the triad in medical investigations of suspected traumatic shaking'. Arch Dis Child, 2018.PMID 29510999
- [12]Teece S, Crawford I. Best evidence topic report. Torn frenulum and non-accidental injury in children. Emerg Med J, 2005.PMID 15662069
- [13]Cowley LE, Morris CB, Maguire SA, Farewell DM, Kemp AM. Validation of a Prediction Tool for Abusive Head Trauma. Pediatrics, 2015.PMID 26216332
- [14]Section on Radiology, American Academy of Pediatrics. Diagnostic imaging of child abuse. Pediatrics, 2009.PMID 19403511