Paeds · child-safety-and-social-paediatrics
Kinship care, adoption and permanency health assessments
Also known as Health of children in out-of-home care · Looked-after children health assessment · Foster care health assessment · Kinship care health assessment · Adoption and permanency paediatric assessment · Children in statutory care
Fellowship-level guide to the health assessment of children in kinship care, foster care, adoption and other permanency placements: the staged, repeatable assessment schedule, the developmental-trauma mechanism behind the high health burden, consent and guardianship in statutory care, and the specific needs of Aboriginal and Torres Strait Islander children governed by the Child Placement Principle.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old who has just been placed with his grandmother overnight, after his mother was admitted and the home was judged unsafe. He arrives in your clinic with no health record, an unknown immunisation history, and behaviour his grandmother describes as 'wild'. This is the prototypical child in out-of-home care, and the encounter that follows is what this topic is about. [1]
Out-of-home care (OOHC) is the statutory arrangement of a child's living situation away from their parents when the child cannot safely remain at home — usually because of abuse, neglect, parental substance use, parental mental illness or family violence. It is an umbrella term that covers kinship care, foster care, residential or group care, and pre-adoptive placements, and it exists in every developed child-protection system under different names: 'out-of-home care' in Australia, 'care' or 'custody' under Oranga Tamariki in Aotearoa New Zealand, 'looked-after children' in the United Kingdom, and children in 'foster care' in the United States and Canada. [1] [9]
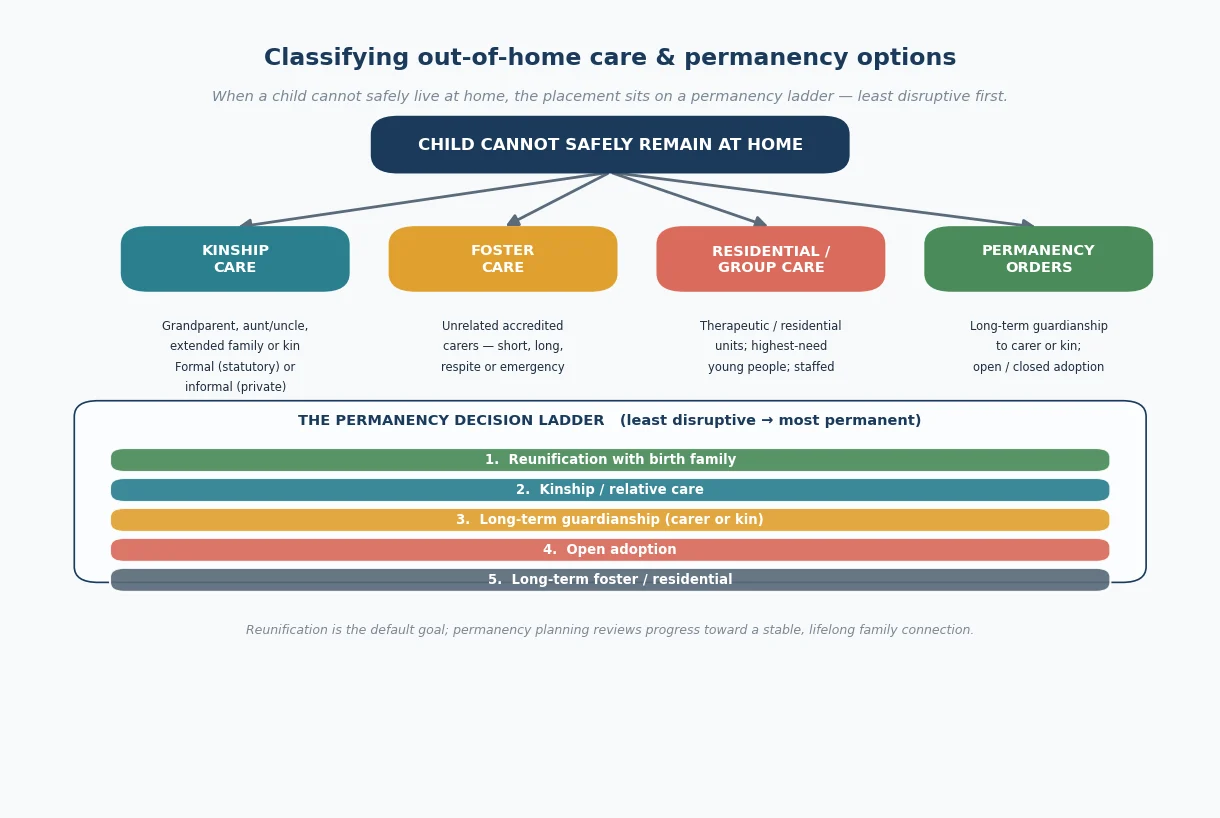
The word permanency carries the clinical weight here. Permanency is the goal of giving a child a stable, lifelong family connection — and it sits on a ladder rather than a binary switch. Reunification with the birth family is the default first goal; if that cannot be achieved safely, the system moves toward kinship care, then long-term guardianship, then adoption, then long-term foster or residential care. The paediatrician does not decide the placement, but the health assessment feeds directly into the permanency plan, because a child's health, developmental and attachment needs determine what kind of placement will hold. [1] [11]
The clinical task is the health assessment — a structured, staged evaluation of the child's physical, developmental, mental-health and educational needs, translated into a written care plan. The AAP Council on Foster Care, Adoption, and Kinship Care clinical report frames it plainly: children enter care sicker than their peers, their needs are frequently unrecognised at entry, and a single 'medical' at entry is not enough — the schedule must repeat. [1] [2]
Classification
Classify the population by the type of placement, because the placement type predicts the child's likely health profile, the support the carer needs, and the consent pathway. All of these arrangements sit on the permanency ladder, ordered from least to most disruptive of the child's existing family connections. [1]
Kinship care places the child with a relative or member of the child's extended family or community — most often a grandparent. It may be formal (statutory, under a child-protection order, with the agency holding some guardianship and the carer assessed and supported) or informal (a private family arrangement without statutory oversight). Kinship care preserves identity and connection and is the preferred option after reunification, but kinship carers are frequently older, on lower incomes, and dealing with their own grief and family conflict — supports that birth-parent and non-relative foster placements receive are often thinner for kin. [1] [9]
Foster care places the child with unrelated, accredited carers in their family home. It spans short-term, long-term, respite, emergency and therapeutic foster care. Therapeutic or treatment foster care is a higher-intensity model with additional training and support for carers looking after children with complex trauma-related needs. [1]
Residential or group care places the child in a staffed facility, usually reserved for the highest-need older young people whose behaviours cannot be managed in a family setting. It carries the highest risk profile of any placement type and increasingly uses structured therapeutic models. [1]
Adoption legally transfers parental responsibility from the birth to the adoptive family and is the most permanent option. It may be domestic infant adoption, special-needs adoption (of an older child or sibling group from care), intercountry adoption, and — where the law permits — open (with ongoing contact with birth family) or closed. In the Australian context adoption is rare and historically freighted, particularly for Aboriginal and Torres Strait Islander children, for whom adoption is contested and the Child Placement Principle hierarchy applies first. [1] [9]
Placement types compared — what the paediatrician needs to know
Epidemiology & Risk Factors
Children in out-of-home care are common, and the population is growing. In Australia, roughly one in thirty-three children is the subject of a child-protection notification in a given year, and tens of thousands of children are in OOHC at any time — a rate that has risen over the past decade. The median age at entry has fallen, and a substantial proportion of children in care are under five, which matters because younger entry both raises the developmental risk and widens the window for intervention. [9]
The single most important epidemiological fact for an ANZ examiner is the over-representation of Aboriginal and Torres Strait Islander children. Indigenous children are around ten times more likely to be in OOHC than non-Indigenous children, and this disparity is not a contemporary accident — it flows from the Stolen Generations, intergenerational trauma, structural disadvantage, and the legacy of colonisation. The Aboriginal and Torres Strait Islander Child Placement Principle exists precisely to counter this, and applying it is a clinical and ethical duty, not an optional cultural flourish. [9]
The reasons children enter care are themselves a map of the health burden. Neglect is the most common ground, followed by emotional and physical abuse and exposure to domestic violence; parental substance use and parental mental illness are the dominant underlying drivers. These are the same exposures that produce developmental trauma, so by the time a child reaches care the neurodevelopmental insult has often accumulated over years. [1] [4]
Turney and Wildeman's analysis of a large US dataset quantified the consequence starkly: children in foster care have rates of mental-health problems, asthma, obesity and other chronic conditions several-fold higher than the general child population, and the gap is not closing. Leslie and colleagues' national study of children entering foster care showed that comprehensive assessment routinely uncovered multiple unmet health and developmental needs that the entry presentation had not captured. [2] [4]
Pathophysiology
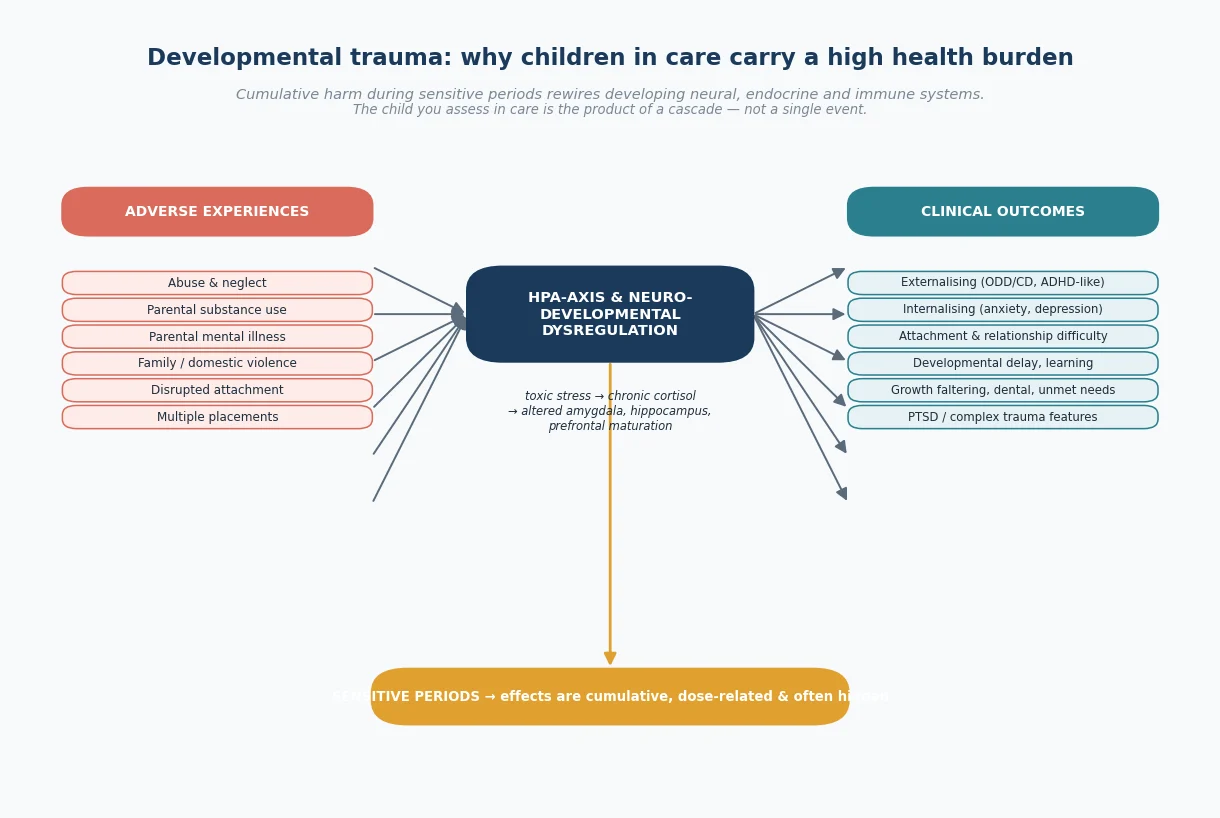
There is no single lesion in a child in care, but there is a mechanism, and understanding it is the difference between a clinician who pathologises behaviour and one who treats it. The mechanism is developmental trauma — the cumulative rewiring of developing neural, endocrine and immune systems by chronic adversity during sensitive periods. [8]
The cascade begins with chronic activation of the stress response. A child exposed to ongoing abuse, neglect, parental substance use and family violence lives in a persistent state of threat. The hypothalamic–pituitary–adrenal (HPA) axis is repeatedly activated, exposing the developing brain to chronically elevated cortisol. Over time this alters the maturation of the amygdala, hippocampus and prefrontal cortex — the very structures that govern threat detection, memory, emotional regulation and executive function. This is the biology behind the clinical observation that children in care are easily triggered, struggle to regulate, and find learning hard. [8]
Disrupted attachment compounds the neurobiology. A child needs at least one consistently available, attuned caregiver to develop secure attachment and a regulated stress response. Maltreatment, neglect and the placement moves that follow entry to care each rupture that process, so the child arrives in care with an attachment system already shaped by unpredictability. This is why attachment-focused, rather than purely behavioural, intervention is central to management. [5]
Developmental trauma is conceptually distinct from single-event post-traumatic stress disorder, and Ford and colleagues' international survey of clinicians showed strong support for a developmental trauma disorder diagnosis that captures the complex presentation of children with chronic interpersonal trauma — affect dysregulation, attachment difficulty, somatic preoccupation and behavioural dyscontrol. The point for the clinician is that the symptom cluster is real, mechanistic and treatable, and it is not synonymous with ADHD, ODD or autism even though it overlaps them clinically. [8]
Prenatal substance and alcohol exposure adds another layer. A significant minority of children entering care — particularly those adopted internationally or removed for parental substance use — were exposed in utero, which contributes a neurodevelopmental and, with alcohol, a teratogenic profile captured under fetal alcohol spectrum disorder (FASD). FASD is over-represented and under-diagnosed in the care population, and it is one of the most important differentials to actively seek. [1] [7]
The clinical pay-off of this mechanism is dose-response. The more adverse exposures, the earlier, and the longer the duration, the greater the neurodevelopmental impact — and the greater the benefit of stable, attuned, trauma-informed care. This is why removal alone does not heal, and why the health assessment must look past the presenting behaviour to the cumulative history. [6] [8]
Clinical Presentation
A child in care rarely presents with the index problem that brought them into care. The presentation is the accumulated health debt, and it spans physical, developmental, mental-health and educational domains — which is exactly why a single-system assessment misses so much. [2]
Physical health problems are over-represented at every contact. Growth faltering is common, particularly in children removed for neglect or with prenatal exposure; untreated dental caries, vision and hearing deficits, skin conditions (eczema, scabies, pediculosis), uncontrolled asthma and other chronic disease, and incomplete or absent immunisation are all routine findings on a careful entry assessment. Leslie and colleagues showed that systematic assessment uncovers physical-health problems in a majority of children entering care that were not identified at presentation. [2]
Developmental and educational presentations are equally common. Global developmental delay, speech and language disorder, learning difficulty and school disengagement each occur at rates well above the general population, and they are often the first signal that the child's neurodevelopmental trajectory has been affected. A school-age child in care who is failing academically and 'acting out' is presenting with a developmental and trauma history, not a discipline problem. [1]
Mental-health and behavioural presentations dominate the clinical picture and consume most of the clinician's attention. Tarren-Sweeney and Hazell's study of children in foster and kinship care in New South Wales found that a majority scored in the clinical range for mental-health problems — rates several-fold higher than community samples — with externalising behaviours, attachment-related difficulty, anxiety and trauma-related symptoms the most prominent. The behavioural presentation (aggression, defiance, sexualised behaviour, emotional withdrawal, food hoarding) is the surface manifestation of the mechanism above. [5]
Attachment insecurity and disordered attachment present behaviourally in ways that are easy to misread. A child who is indiscriminately friendly with strangers, who cannot accept comfort, who controls the interaction, or who recoils from physical closeness is showing an attachment system shaped by unpredictability. These behaviours often surface in the placement itself and bring the child back to clinic. [5] [7]
The presentation changes with placement instability. A child who has moved multiple times often shows escalating dysregulation, withdrawal and mistrust — and the worsening is situational rather than diagnostic. Rubin and colleagues showed that placement instability itself independently worsens behavioural wellbeing, so a deteriorating child may be telling you about the system around them, not a new pathology. [3]
Differential Diagnosis
When a child in care presents with behavioural dysregulation, developmental concern or learning difficulty, the central diagnostic task is to avoid collapsing a complex, mechanistic presentation into a single primary label — because the wrong label leads to the wrong treatment. [7] [8]
| Surface presentation | What it usually is | Must-not-miss alternative to consider |
|---|---|---|
| Inattention, impulsivity, overactivity | Developmental trauma / attachment dysregulation | Primary ADHD (may co-exist; needs collateral history across settings) |
| Social difficulty, rigidity, meltdowns | Attachment insecurity; trauma-related avoidance | Autism spectrum disorder (assess reciprocity, routines, sensory profile) |
| Aggression, defiance, rule-breaking | Trauma-driven externalising in a chaotic system | Conduct disorder; untreated pain or unmet need |
| Learning difficulty, school failure | Cumulative neglect; disrupted schooling | Specific learning disorder; FASD; hearing or vision deficit |
| Withdrawal, flat affect, anxiety | Trauma; insecure attachment | Depression; anxiety disorder; autistic burnout |
The most common and most consequential error is mistaking developmental trauma or attachment difficulty for primary ADHD. Both produce inattention, impulsivity and overactivity, and they genuinely co-occur — but a child whose dysregulation resolves with stability and attunement was not primarily hyperactive, and stimulants alone will not treat a child whose nervous system is in survival mode. Distinguish them by taking a collateral history across settings, by asking whether the behaviour is constant or triggered, and by observing the effect of a stable, attuned relationship. [7] [8]
The second trap is confusing attachment insecurity with autism spectrum disorder. Indiscriminate friendliness, social wariness and relational control can all resemble autistic social difficulty. The discriminator is the quality of reciprocity and the presence of restricted, repetitive interests and sensory differences — which is why a structured developmental assessment, not a clinic impression, is the right next step when ASD is genuinely suspected. [7]
The third is missing FASD. Neurodevelopmental impairment with a history of prenatal alcohol exposure is common in the care population, frequently unrecognised, and shapes the long-term plan. Send the child for formal FASD assessment when there is a credible exposure history and a sentinel neurodevelopmental profile, rather than attributing the picture to 'complex trauma' alone. [1]
Finally, distinguish a situational deterioration from a new primary disorder. A child who decompensates after a placement move, a birth-family contact, or a school transition is responding to context, and the intervention is to stabilise the context, not to escalate psychotropic medication. Chambers and colleagues remind us that the assessment of a child coming into care is itself an intervention, and that over-pathologising at the first contact does lasting harm. [10]
Clinical & Bedside Assessment
Open every care health assessment by confirming who the child is placed with, how the placement arose, and — before you plan any intervention — who holds parental responsibility and can consent. In statutory care, parental responsibility may rest with the birth parent, be shared with the child-protection agency, or be held wholly by the agency under a care or guardianship order. The order determines who can consent to immunisation, surgery, mental-health treatment and even routine blood tests, so you confirm it first and record it in the plan. [1]
Take a trauma-informed history that moves at the child's pace. The pre-care history is often incomplete, contested or unavailable, so you gather what you can from the carer, the agency file and (developmentally) the child, without forcing disclosure or conducting an investigative interview. Ask about prenatal exposures, developmental milestones, past illness, hospitalisations, medications, immunisation, schooling and any prior trauma — and record honestly what is known and what is unknown. [1] [10]
Perform a full top-to-toe examination, including accurate growth parameters (weight, height, BMI, head circumference in the under-twos) plotted on appropriate charts, a skin examination looking for signs of past injury or abuse and for neglected skin disease, a dental inspection, and a systems examination for unmet chronic disease. Examine with the child's permission, explain what you are doing, and pace the examination — a child whose body has been the site of harm will read a clinical examination as a threat unless it is handled with care. [1]
Assess developmental status and school functioning directly. Use an age-appropriate developmental screen, and for school-age children ask specifically about reading, attention, friendships and school attendance — and request the school's view, because the teacher often holds the most reliable collateral. Developmental and educational need is frequently the most actionable finding of the assessment. [2]
Assess attachment and carer-child interaction clinically. Observe how the child and carer seek and receive comfort, how the child responds to a stranger (you), whether interaction is reciprocal or controlling, and how the carer describes the child. These observations are not a formal attachment diagnosis, but they shape the management plan and flag where carer support is the intervention. [5]
Assess mental health with a validated tool rather than impression alone. The Strengths and Difficulties Questionnaire (SDQ) is a widely used screen; the Tarren-Sweeney Assessment Checklist for Children (ACC) and Brief Assessment Checklist were developed specifically for children in care and capture the attachment- and trauma-related presentations that generic screens miss. A positive screen is a trigger for referral, not a diagnosis. [5] [7]
Investigations
There is no single confirmatory test for the health of a child in care, but there is a defined screening set that the comprehensive assessment rests on. These investigations address the domains the history and examination flag, and their results belong in the written care plan. [1] [2]
Routine screening at the comprehensive assessment covers growth (accurate measurements and plotting), vision and hearing (formal assessment, not bedside impression), dental review, a developmental screen, and a mental-health screen (SDQ and, where indicated, the ACC). A baseline full blood count and iron studies identify the iron deficiency and anaemia that are common in neglected children; urinalysis and, where indicated, a sexual-health screen (in adolescents and in any child where abuse history raises concern) complete the core set. [1] [2]
Immunisation status must be verified on the national immunisation register, not assumed. Children entering care frequently have incomplete or undocumented records; where the record is genuinely unavailable, the safe approach is to treat as potentially unimmunised and plan a catch-up schedule in line with the national immunisation programme. Confirm hepatitis B status, and ensure MMR, HPV (adolescents) and the routine childhood schedule are complete and documented on the register. [1]
Mental-health screening tools validated for the care population include the SDQ as a broad screen and the Tarren-Sweeney ACC and Brief Assessment Checklist for the attachment- and trauma-related presentations that generic instruments under-detect. A positive screen is a referral trigger; the formal developmental, neuropsychological or trauma assessment that follows is where the diagnosis is made. [5] [7]
Intercountry adoptees require additional infectious-disease and growth screening. Depending on the country of origin, this includes screening for tuberculosis, hepatitis B and C, HIV, syphilis, intestinal parasites, and sometimes malaria and thyroid dysfunction, alongside a careful review of growth and development against the child's likely prenatal and early-life history. Early catch-up growth is expected; persistent faltering warrants investigation. [1]
When the developmental or mental-health picture is complex, the correct 'investigation' is a specialist referral — to a developmental paediatrician for suspected FASD, developmental delay or ASD, or to a child mental-health service for trauma- and attachment-focused assessment. Over-investigating with repeated bloods and imaging in a child whose behaviours reflect cumulative harm retraumatises without adding information. [7] [10]
Management — Resuscitation
When a child newly enters care, the first clinical question is whether there is an unmet acute need that predates the placement. A neglected child may arrive with an untreated infection, an unrecognised injury, an acute mental-health crisis, or — in the neonate removed for parental substance use — neonatal abstinence syndrome. Treat these on their merits, the way you would treat any child, because placement does not pause physiology. [1]
Secure the child's immediate safety. Confirm the legal basis of the placement and that the carer present is authorised; if the child has arrived without medication, equipment or medical information, arrange urgent transfer of records. For a neonate with prenatal substance exposure, assess and manage withdrawal using a validated scoring tool and the local protocol. [1]
Manage a behavioural crisis or dysregulation at entry with a trauma-informed, not punitive, approach. The child who is aggressive, self-harming or absconding on the first night is in a survival state; the immediate response is to reduce stimulation, ensure physical safety, support the carer, and avoid escalation. Reserve pharmacological or restrictive intervention for immediate danger, and arrange urgent mental-health review for any child expressing suicidality or severe distress. [7]
Recognise when safeguarding escalation is required at entry — for example, fresh injuries suggesting ongoing harm, disclosure of abuse not yet reported, or a placement that is itself unsafe. A newly placed child remains a child at risk, and the duty to report a new concern does not change because the child is already known to the system. [1]
Management — Definitive & Stepwise
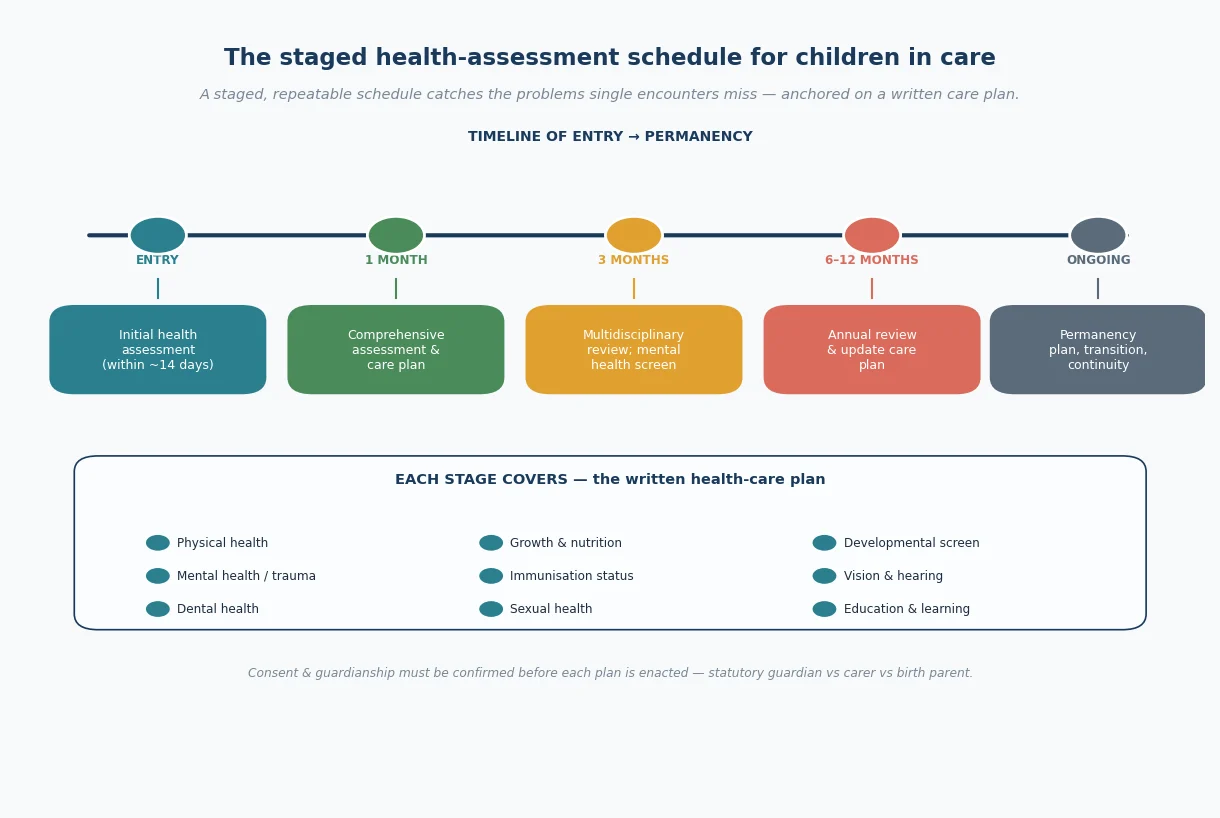
The definitive management of a child in care is a staged, repeatable assessment schedule translated into a written care plan that follows the child. The AAP clinical report sets the structure: an initial health assessment shortly after entry, a comprehensive assessment within the first month, and periodic review (commonly every six months for the first few years and at least annually thereafter). Each contact updates the plan. [1]
The staged health-assessment schedule
Entry assessment (within ~14 days) — screen for acute unmet need, injury, safeguarding concern; confirm placement and consent authority
Comprehensive assessment (within ~1 month) — full history, examination, growth, developmental and mental-health screen, immunisation review, vision, hearing, dental
Care plan written — named clinician, identified needs, referrals, portable record; shared with carer, agency and (where appropriate) birth family and school
Periodic review (commonly 6-monthly early, then annual) — re-screen, update plan, review placement stability and progress toward permanency
Ongoing — continuity of care, education plan, trauma-informed mental-health support, and transition planning as the child approaches aging out
The written care plan is the deliverable, not the assessment itself. It records the child's identified physical, developmental, mental-health and educational needs, the named clinician responsible for coordinating care, the referrals made, the immunisation and medication plan, and the consent authority — and it travels with the child. A portable, accurate record is the single most effective defence against the fragmented, episodic care that plagues this population. [1]
Build the management around a trauma-informed, attachment-focused multidisciplinary team. The evidence base for children in care favours trauma-focused and attachment-based interventions delivered to the carer-child dyad, rather than generic individual therapy; carer training and support are themselves the intervention, because a regulated, attuned carer is the child's most powerful therapeutic resource. Tarren-Sweeney has argued forcefully that mental-health services for children in care must be redesigned around this population's specific attachment- and trauma-related profile rather than generic community pathways. [6] [7]
Address educational needs explicitly. Initiate or update the child's education or learning plan, liaise with the school, and ensure the child has access to learning support — because educational engagement is both an outcome and a protective factor, and it is frequently the most modifiable. [1]
Handle consent for substantive interventions carefully. For immunisation, routine treatment and most mental-health care, the day-to-day authority usually rests with the carer or guardian under the order; for major surgery, contested treatment, or where the order reserves decisions to the birth parent or the court, confirm and document the authority before proceeding. When in doubt, consult the child-protection agency and your medical defence organisation rather than improvising. [1]
Specific Subtypes & Scenarios
Kinship care. The grandparent carer is the prototype. Kinship placements preserve identity and family connection and are preferred after reunification, but kinship carers are often older, on lower incomes, and dealing with their own grief, family conflict and the burden of caring without the supports that foster carers receive. The health assessment here must include a carer needs assessment, because supporting the carer is supporting the placement — and Shmerling and colleagues emphasise that the disadvantage of kinship carers is itself a health determinant for the child. [1] [9]
Long-term foster care versus adoption. Both can provide permanency, but they differ in identity, contact and legal finality. Open adoption (with ongoing birth-family contact) is increasingly preferred where reunification is not possible, but in the Australian context adoption of Aboriginal children is contested and rare. The paediatric task is to support the child's identity work, clarify and sustain appropriate birth-family contact, and ensure continuity of health care through the legal transition. [1] [11]
Intercountry adoption. The intercountry adoptee arrives with a specific screening agenda — infectious-disease screen for tuberculosis, hepatitis B and C, HIV, syphilis and parasites; growth and developmental catch-up assessment; and a careful reconstruction of prenatal and early-life history, including the possibility of institutional deprivation and prenatal exposure. Early medical review after arrival is essential, and developmental catch-up should be monitored over the first year. [1]
Residential or group care. Reserved for the highest-need older young people, residential care carries the highest risk profile and the most fragmented health care. Structured therapeutic models, consistent staff relationships, and assertive health and mental-health outreach — bringing the service to the child rather than waiting for engagement — are the management principles. [1]
Aboriginal and Torres Strait Islander children in care. This is the scenario the ANZ examiner will probe. Apply the Aboriginal and Torres Strait Islander Child Placement Principle — a hierarchy that places a child with kin, then within the child's community, then within another Aboriginal or Torres Strait Islander family, before any non-Indigenous placement — and ensure ongoing connection to family, culture, community and Country. Work with the local Aboriginal community-controlled health and child and family services, recognise the Stolen Generations legacy, and never present adoption as the default permanency option for this population. [9]
Adolescents aging out of care. The young person approaching the age at which care ends faces elevated risks of mental-ill health, homelessness, unemployment, early pregnancy and justice-system contact. The management is a planned transition: ensure health-record continuity, transfer to adult or youth-friendly services, address mental health and housing explicitly, and maintain a single trusted adult through the transition. Aging out without a plan is a known harm. [1]
Children with disabilities in care. Children with disabilities are over-represented in OOHC and at heightened risk of unmet need and diagnostic overshadowing — behavioural change attributed to the disability rather than investigated. Maintain a high index of suspicion, involve carers who know the baseline, and attend carefully to consent, which may be complex where capacity is in question. [1]
Neonates entering care after prenatal substance exposure. These infants may present with neonatal abstinence syndrome requiring scored, protocolised management, carry elevated FASD risk, and arrive at the very age when attachment is forming — so the early placement, carer support and developmental surveillance in the first year are disproportionately consequential. [1]
Complications & Pitfalls
- Placement breakdown and multiple placements independently worsen behavioural wellbeing and compound attachment injury; track the number of placements and treat instability as a clinical problem, not an administrative one. [3]
- Misdiagnosis — labelling developmental trauma or attachment difficulty as primary ADHD, ASD or ODD at the first contact — leads to the wrong treatment and obscures the real mechanism. [7] [8]
- Fragmented, episodic care — lost records, missed immunisations, repeated unnecessary investigations, a different clinician at each contact — is the default failure mode of health care for this population and is exactly what the portable care plan exists to prevent. [1] [2]
- Consent failures — treating, immunising or operating without confirming who holds parental responsibility — expose the child and the clinician and can be avoided by a routine first-question check. [1]
- Over-investigation and retraumatisation — conducting repeated, invasive, unexplained assessments on a child whose behaviours reflect cumulative harm — adds harm without information. [10]
- Failing the Child Placement Principle — placing or managing an Aboriginal or Torres Strait Islander child in a way that severs cultural connection — causes measurable, lifelong identity harm. [9]
Prognosis & Disposition
The long-term outlook for adults who spent time in care is sobering and is itself the argument for investing in the assessment and care described here. Adults with a care history have elevated rates of mental-ill health, lower educational attainment, higher rates of unemployment, homelessness, early parenthood and contact with the justice system compared with the general population — outcomes that track closely with placement instability, unmet health need and disrupted education. [1] [3]
The prognosis is powerfully modifiable. Placement stability is the single strongest predictor: Rubin and colleagues showed that each additional move independently worsens behavioural wellbeing, and conversely that stability protects it. Permanency — a stable, lifelong family connection — closes much of the gap. Continuity of health care, sustained educational engagement, and the presence of at least one stable, trusted adult each add independent protection. [3] [11]
Tarren-Sweeney's prospective study complicated the picture in an important way: over seven to nine years in long-term care, only a minority of children showed clinically meaningful improvement in mental-health symptoms, which is evidence both that care alone does not heal and that active, trauma- and attachment-focused intervention is needed — not passive placement. [6]
The disposition after each assessment is therefore active: update the care plan, make the referrals, confirm the placement is stable and moving toward permanency, and arrange the next review. The safety-net is the named clinician and the portable record; without them, the next crisis starts from zero. [1]
Plan the transition out of care early. Aging out should be a staged handover with health-record continuity, an identified adult services pathway, and explicit attention to mental health, housing and education — not a cliff-edge at a statutory birthday. [1]
Special Populations
Aboriginal and Torres Strait Islander children. Over-representation, the Child Placement Principle, cultural safety, and the Stolen Generations context make this the central special population in ANZ practice. Work with community-controlled services, ensure connection to Country and culture, and apply the placement hierarchy at every decision point. The duty of health assessment does not change; the way it is delivered does. [9]
Children with disabilities and chronic illness. Over-represented, frequently under-served, and at risk of diagnostic overshadowing and complex consent. The assessment must actively seek unmet need, involve those who know the baseline, and address capacity and substitute decision-making where relevant. [1]
Refugee, asylum-seeker and unaccompanied minors. These children carry pre-flight trauma, displacement and loss on top of the care experience, and require infectious-disease screening, trauma-informed mental-health care, and language-appropriate assessment with professional interpreters. [1]
Adolescents and the transition to adulthood. The aging-out young person is a special population in their own right, with transition planning the defining clinical task. [1]
LGBTQI+ young people in care. Over-represented in care and at heightened risk of placement breakdown and mental-ill health; ensure placement is affirming and that mental-health support is attuned to identity. [1]
Rural and remote children. Distance from specialist assessment and therapeutic services compounds every other barrier; telehealth outreach, regional visiting services and a single coordinating clinician are the practical answers. [1]
Evidence, Guidelines & Regional Differences
The AAP Council on Foster Care, Adoption, and Kinship Care clinical report (Szilagyi and colleagues, 2015) is the international reference for the staged health assessment, recommending an initial assessment within days of entry, a comprehensive assessment within thirty days, and periodic follow-up, with a coordinated, continuous medical home and a written care plan. It frames the field and is the source examiners expect. [1]
Leslie and colleagues' 2003 national study established empirically that comprehensive assessment of children entering foster care routinely uncovers multiple unmet physical, developmental and mental-health needs — the evidence base for the staged schedule. Turney and Wildeman's 2016 analysis quantified the several-fold elevation in mental- and physical-health morbidity in children in foster care, grounding the claim that this is a high-needs population by definition. [2] [4]
On placement, Rubin and colleagues' 2007 study established that placement instability independently worsens behavioural wellbeing — the evidence for stability as the central modifiable predictor. Spieker and colleagues' randomised-trial follow-up showed that a parenting intervention in toddlers in child welfare improved permanency outcomes two years later, evidence that early, attachment-focused intervention changes the trajectory. [3] [11]
On mental health, Tarren-Sweeney's body of work — the New South Wales prevalence study with Hazell, the long-term change study, and the call to redesign services — defines the attachment- and trauma-related profile of children in care and the case for population-specific mental-health services rather than generic pathways. Chambers and colleagues and Ford and colleagues round out the assessment-process and developmental-trauma-diagnosis evidence respectively. [5] [6] [7] [8] [10]
In Australia, out-of-home care operates under state and territory child-protection legislation, so the legal orders, consent pathways and agency names vary across jurisdictions. The Aboriginal and Torres Strait Islander Child Placement Principle applies nationwide and is the defining framework for Indigenous children in care; the Australian Institute of Health and Welfare's annual Child Protection Australia report is the source for current numbers and Indigenous over-representation. The Royal Children's Hospital Melbourne guidance on the health of children in out-of-home care is a widely used clinical reference. In Aotearoa New Zealand, care operates under Oranga Tamariki and the obligations of the Treaty of Waitangi frame practice for Maori tamariki. State the principles — staged assessment, the portable care plan, consent under the order, and the Child Placement Principle — and defer to current AIHW data and local statute for operational thresholds and exact figures. Never invent a specific act name or section number. [9]
Exam Pearls
PERMANENT
References
- [1]Szilagyi MA, Rosen DS, Rubin D, Zlotnik S, et al; Council on Foster Care, Adoption, and Kinship Care; Committee on Adolescence; Council on Early Childhood Health care issues for children and adolescents in foster care and kinship care. Pediatrics, 2015.PMID 26416941
- [2]Leslie LK, Hurlburt MS, Landsverk J, Rolls JA, Wood PA, Kelleher KJ Comprehensive assessments for children entering foster care: a national perspective. Pediatrics, 2003.PMID 12837879
- [3]Rubin DM, O'Reilly AL, Luan X, Localio AR The impact of placement stability on behavioral well-being for children in foster care. Pediatrics, 2007.PMID 17272624
- [4]Turney K, Wildeman C Mental and physical health of children in foster care. Pediatrics, 2016.PMID 27940775
- [5]Tarren-Sweeney M, Hazell P Mental health of children in foster and kinship care in New South Wales, Australia. Journal of Paediatrics and Child Health, 2006.PMID 16509906
- [6]Tarren-Sweeney M Rates of meaningful change in the mental health of children in long-term out-of-home care: a seven- to nine-year prospective study. Child Abuse & Neglect, 2017.PMID 28734200
- [7]Tarren-Sweeney M It's time to re-think mental health services for children in care, and those adopted from care. Clinical Child Psychology and Psychiatry, 2010.PMID 20923907
- [8]Ford JD, Grasso D, Greene C, Levine J, Spinazzola J, van der Kolk B Clinical significance of a proposed developmental trauma disorder diagnosis: results of an international survey of clinicians. Journal of Clinical Psychiatry, 2013.PMID 24021504
- [9]Shmerling E, Creati M, Belfrage M, Jeffery HE, Ward M, Schmied V The health needs of Aboriginal and Torres Strait Islander children in out-of-home care. Journal of Paediatrics and Child Health, 2020.PMID 31517415
- [10]Chambers MF, Saunders AM, New BD, Williams-Beckis J, Strohm B Assessment of children coming into care: processes, pitfalls and partnerships. Clinical Child Psychology and Psychiatry, 2010.PMID 20923900
- [11]Spieker SJ, Oxford ML, Fleming CB Permanency outcomes for toddlers in child welfare two years after a randomized trial of a parenting intervention. Children and Youth Services Review, 2014.PMID 25125769