Paeds · child-safety-and-social-paediatrics
Mandatory reporting and jurisdictional child-protection frameworks
Also known as Mandatory reporting of child abuse · Child protection legislation · Jurisdictional child-protection systems · Mandated reporting and child welfare · Child maltreatment reporting laws · Safeguarding and statutory child protection
Fellowship-level guide to mandatory reporting and jurisdictional child-protection frameworks: who must report, the reasonable-belief threshold, how obligations vary across ANZ, UK, US and Canadian jurisdictions, barriers and enablers to reporting, and the defensible bedside sequence from recognition through documentation to notification.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-year-old brought to your emergency department with a spiral femur fracture and a story that keeps changing. Your job is not to prove abuse, and it is not to investigate the family. It is to recognise that this injury pattern meets a threshold, document what you see, and notify the child-protection authority so they can do their job. [8]
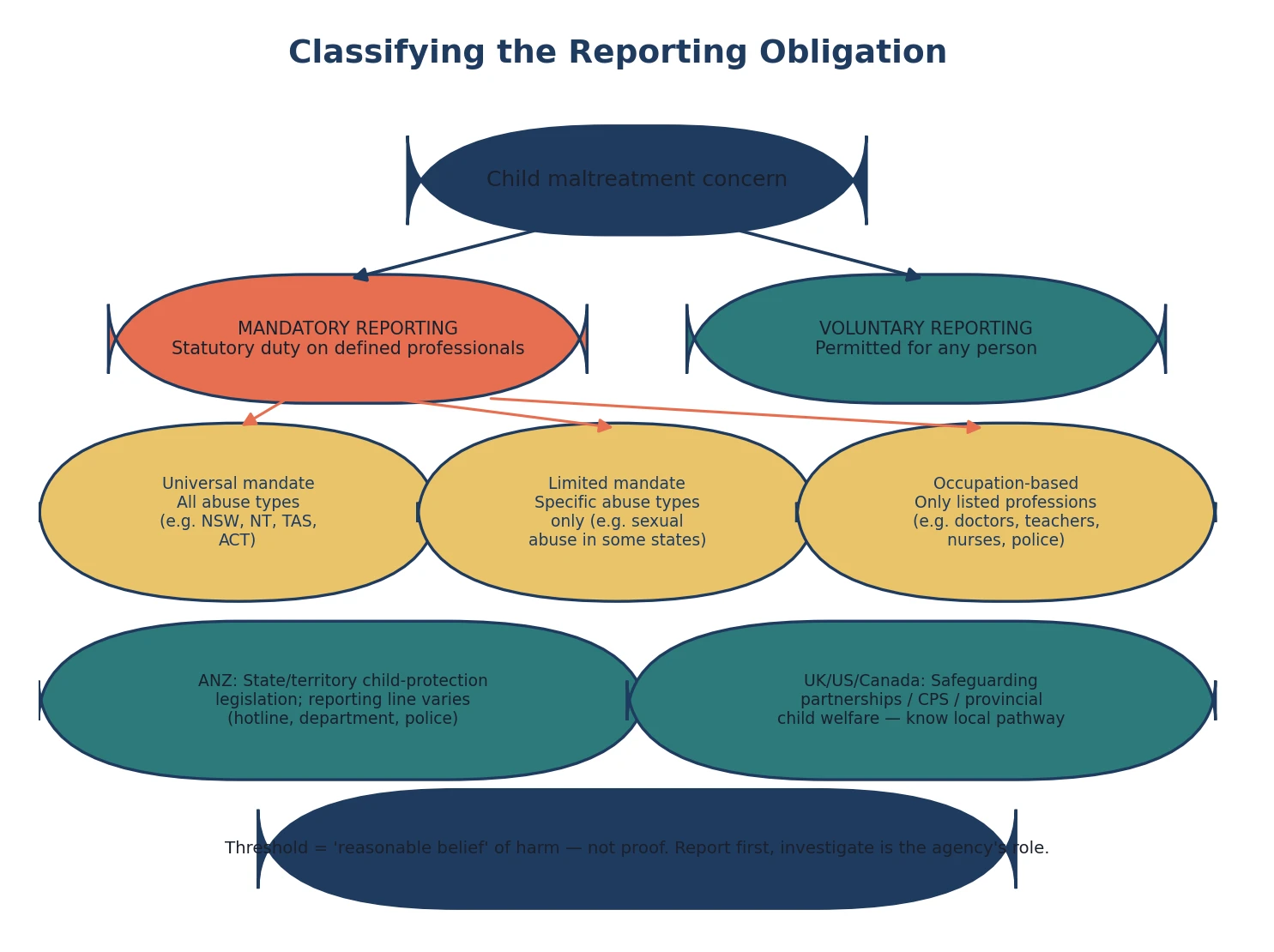
Three terms carry most of the weight. Mandatory reporting is a statutory obligation imposed by legislation on defined persons — usually specified professions — to report a reasonable belief that a child has suffered, or is at risk of, abuse or neglect to a designated child-protection authority. Voluntary reporting is the right of any person to notify the authority of a concern, even when they are not legally mandated to do so. The two coexist, and most jurisdictions encourage voluntary reporting while legally compelling it for a defined group. [1]
A reasonable belief (sometimes called reasonable suspicion) is the threshold for most mandatory-reporting laws: you do not need proof, certainty, or a confession. It means that a reasonable person in your position, holding the information you hold, would form a belief that the child has been or is at risk of harm. This is deliberately set lower than the evidentiary bar a court would require, because the system's goal is early identification, not prosecution. [1] [2]
The child-protection authority is the statutory agency designated by legislation to receive reports, triage them, investigate, and coordinate a response. Its name, structure and powers vary enormously by jurisdiction — a child-protection helpline in New South Wales, a department of child safety in Queensland, children's social care in England, Child Protective Services in the United States. Knowing which agency, which phone number and which form apply where you work is part of your professional duty. [1] [9]
[1] [8]Classification
Start from who is compelled to report what, and in which jurisdiction. The pathway you follow depends on whether your profession falls within the mandatory-reporting mandate, which abuse types are covered, and how the law is framed in the place you practise. [1] [2]
Universal mandatory reporting compels every person, or every person in a defined professional group, to report all forms of child abuse and neglect regardless of the perpetrator or abuse type. Several Australian jurisdictions have moved toward this model, broadening both the pool of mandated reporters and the range of abuse types covered. [1]
Limited or targeted mandatory reporting compels only defined professionals to report, and often only for specific abuse types — most commonly child sexual abuse. In some states, only doctors are mandated; in others, the list includes teachers, nurses, police and childcare workers. The scope of who must report what has expanded progressively over the past two decades but remains jurisdiction-specific. [1] [3]
Occupation-based mandates attach the duty to the professional role rather than to the abuse type alone. A paediatrician may be mandated for all abuse types in one jurisdiction but only for sexual abuse in another. Mathews and Kenny's cross-jurisdictional review documented that the United States, Canada and Australia each structure their mandates differently in who must report, what triggers a report, and what protections and penalties apply. [1]
Reporting obligation by jurisdiction and abuse type
Epidemiology & Risk Factors
Child maltreatment is common and substantially under-reported. Population surveys across developed countries consistently show that official child-protection statistics capture only a fraction of the abuse that children experience, because most maltreatment never reaches a mandated reporter or an agency. [8] [11]
Finkelhor and colleagues' national survey work showed that well over a third of children in the United States had experienced at least one form of direct or witnessed violence, crime or abuse in the past year, and lifetime prevalence is far higher. These figures dwarf the rate of substantiated child-protection cases, underscoring the reporting gap. [11]
Mandatory-reporting legislation does increase the number of reports received by child-protection agencies, and there is evidence it increases identification of specific abuse types. Mathews and colleagues' seven-year time-trend analysis showed that a new mandatory-reporting law for child sexual abuse in Queensland was associated with a sustained increase in reporting and identification of cases that had previously gone unrecognised. [3]
Tonmyr and Mathews' legal-doctrinal review examined whether mandatory reporting actually increases meaningful contact with child-protection systems, finding that while reporting volume rises, the relationship between increased reports and improved child outcomes is complex and not linear — the system must be resourced to respond. [2]
Children with disabilities face a substantially elevated risk of maltreatment, and their abuse is even more likely to go unrecognised and unreported because communication barriers, behavioural presentations and diagnostic overshadowing obscure the signs. Legano and colleagues' clinical report documented that children with disabilities are at least three times more likely to experience abuse than peers without disabilities. [15]
Clinician factors themselves predict whether a concern is reported. Flaherty and Sege showed that paediatricians' identification and reporting rates vary with training, confidence, prior experience with child protection, and the availability of local resources — meaning the same child may be reported by one clinician and missed by another. [6] [7]
Pathophysiology
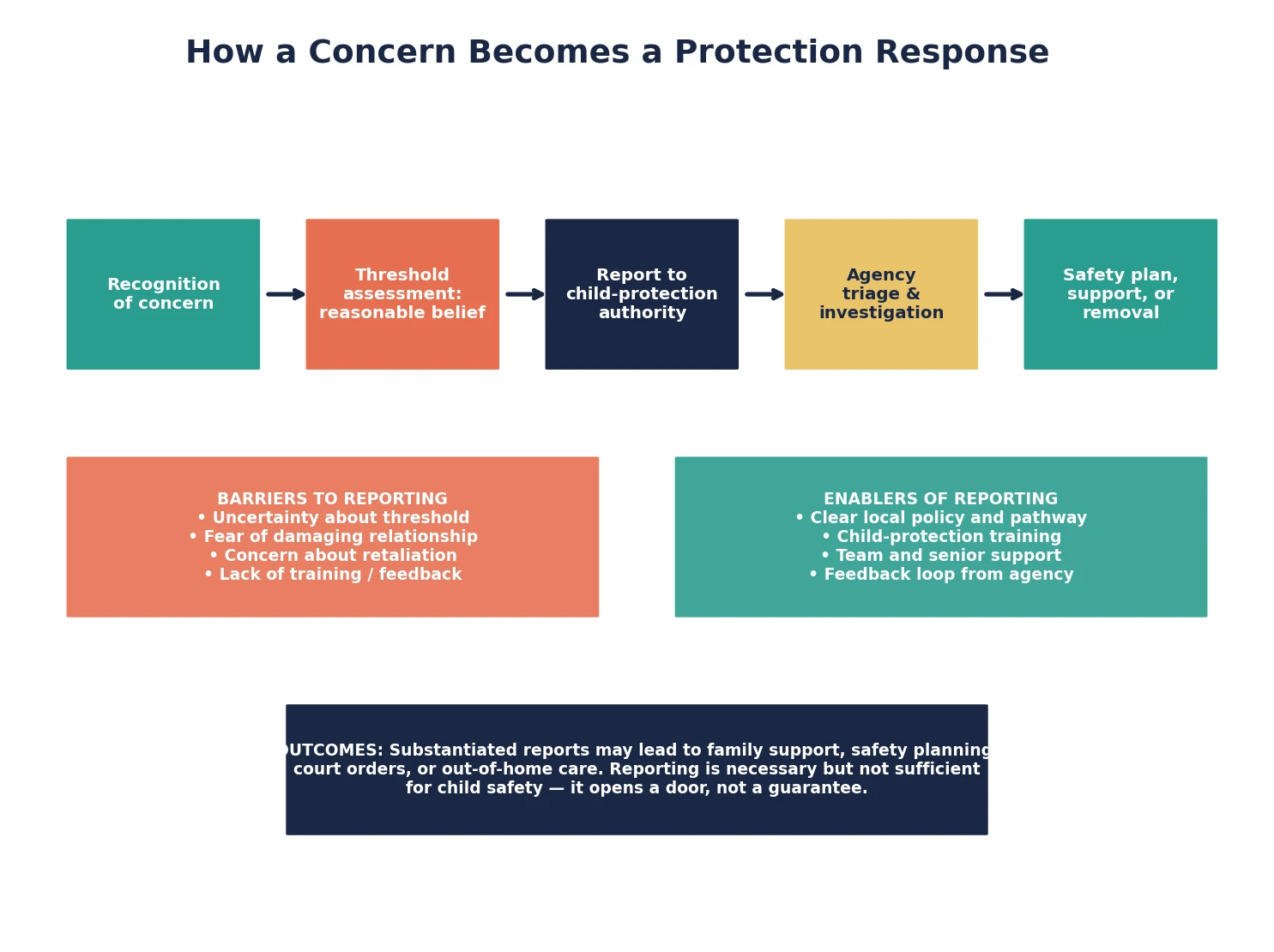
There is no enzyme for a reporting obligation, but there is a mechanism: how a clinical concern travels from recognition through a statutory threshold to a protective response. Understanding this pathway explains why some children are protected and others fall through gaps. [8]
The pathway begins with recognition — a clinician notices an injury pattern, a behavioural sign, a disclosure, or a constellation of risk factors that raises concern. Recognition is the rate-limiting step, because children rarely disclose abuse promptly, and the physical and behavioural signs are often non-specific. Morrison and colleagues' systematic review showed that children delay or avoid disclosing sexual abuse because of fear, shame, loyalty conflicts, and a belief they will not be believed. [16]
Once recognised, the clinician applies the threshold test: would a reasonable person in my position, holding this information, believe this child has suffered or is at risk of significant harm? The threshold is deliberately set low — you do not need to rule out every alternative explanation before reporting, and you do not need to investigate. The distinction between your clinical role (recognise, document, report) and the agency's role (investigate, assess, intervene) is central to how the system is designed. [1] [8]
The report then enters a statutory response pathway: the child-protection authority triages the notification, decides whether to investigate, conducts an assessment, and coordinates a response ranging from family support to court-ordered intervention or removal. Gilbert and colleagues showed that the threshold at which agencies respond, and the types of cases they substantiate, vary markedly between countries — so the same report may produce very different outcomes depending on the jurisdiction. [9]
Barriers operate at every step and explain why the recognition-to-report gap exists. Flaherty and Sege identified clinician uncertainty about what constitutes abuse, fear of damaging the therapeutic relationship, concern about being wrong, lack of feedback from agencies after a report, and time pressures as the principal barriers to physician reporting. Fraser and colleagues found similar patterns in nurses, with reporting more likely when the clinician had received specific training and had access to a child-protection protocol. [5] [6]
The relationship between reporting and outcomes is not straightforward. A report opens a door, but the child-protection system must be resourced to respond, and an overwhelmed system may substantiate fewer cases or offer less support. This is why clinicians must not treat reporting as the endpoint of their responsibility — ongoing clinical care, follow-up, and advocacy for the child remain essential after the notification is made. [2] [9]
Clinical Presentation
From the doorway, a child who needs a report can present in any clinical setting — an emergency department injury, a primary-care behavioural concern, a school-nurse disclosure, or a routine immunisation visit where the pattern of presentation raises a flag. The setting changes your immediate priorities but not your reporting obligation. [8]
A pre-mobile infant with any bruising presents a sentinel-injury scenario. Lindberg and colleagues showed that infants presenting with sentinel injuries — injuries likely to have been inflicted but not yet labelled as abuse — have a substantial rate of occult injury on further investigation, and many are not reported or worked up at the index presentation. A bruise in a non-ambulant infant is a reportable concern until proved otherwise. [13]
An older child with an unexplained or inconsistent injury presents the discrepancy scenario. The injury pattern does not fit the mechanism described, the story changes between informants, or there is an unexplained delay in presentation. These inconsistencies themselves are clinical findings that contribute to a reasonable belief, and they belong in your documentation. [8]
A child who discloses abuse presents the disclosure scenario. A disclosure may be spontaneous, tentative, partial, or retracted, and the child may ask you not to tell anyone. Your job is to listen, believe, document verbatim, and explain honestly that you have a duty to report — you cannot promise secrecy. Morrison and colleagues' review showed that how the first recipient responds to a disclosure powerfully influences whether the child continues to disclose or retreats into silence. [16]
A child exposed to domestic violence presents the family-violence scenario. Cross and colleagues showed that exposure to intimate-partner violence is itself a form of child maltreatment in many jurisdictions, and its reporting and response vary sharply between child-welfare systems. The question is not only whether the child was physically harmed but whether the home environment poses a risk of significant harm. [14]
A child with disabilities presents the overshadowing scenario. Behavioural changes, self-injury, regression or distress may be attributed to the disability rather than investigated as possible maltreatment, and communication barriers make disclosure harder. Legano and colleagues emphasised that a lower index of suspicion is never appropriate here — in fact the opposite is true. [15]
A clinician who is unsure presents the uncertainty scenario. The most common reason a reportable concern goes unreported is that the clinician was not certain enough. The threshold is not certainty — it is reasonable belief — and consulting a senior colleague, the child-protection team or the agency's advice line is the right response to uncertainty, not silence. [6]
Differential Diagnosis
When a clinician senses a child may have been maltreated, the first task is to distinguish what kind of concern is in front of them, because the label changes the reporting pathway and the response. [8]
| Surface presentation | What it might actually be | Must-not-miss alternative |
|---|---|---|
| "I'm not sure it's abuse" | A reportable reasonable-belief threshold met | Waiting for proof while the child remains at risk |
| "The family will be angry" | A concern displaced by clinician discomfort | A child who needs a report, sacrificed to relationship fear |
| "It's probably an accident" | An injury not yet adequately explained | An inflicted injury needing a skeletal survey and report |
| "Social services are overwhelmed" | A clinician rationalising non-reporting | A statutory duty that exists regardless of system capacity |
Discriminate a reasonable belief from a clinical suspicion you have not yet articulated. Many clinicians carry a gut sense that something is wrong but cannot name it, and the reporting threshold never fires because the concern stays unexamined. Naming the concern — writing down what you saw, what was said, and why it worries you — is often what crystallises a reasonable belief. [6]
Distinguish your clinical role from the investigative role. You are not required to confirm abuse, interview the perpetrator, or gather evidence beyond what good clinical care demands. Attempting an investigative interview yourself can contaminate a subsequent forensic process, so you document what arises in clinical care and leave the formal investigation to the agency. [8]
Separate a reportable concern from a family-support need. Some presentations do not meet a threshold for notification but do indicate a family that would benefit from voluntary support services. In these cases, you may offer referral and engage support proactively while remaining vigilant — but when the threshold is met, you report regardless of whether the family would accept support. [1] [2]
When a child presents with an injury that could be inflicted or accidental and the picture is genuinely ambiguous, the correct response is to investigate clinically (skeletal survey, bleeding screen, neuroimaging as indicated), consult the child-protection team, and report if a reasonable belief crystallises during the assessment. An uncertain injury is not a reason to defer — it is a reason to consult and document. [13]
Clinical & Bedside Assessment
Open every encounter where maltreatment is possible by securing the child's immediate safety. If there is an acute danger — a violent parent in the department, an unsafe discharge destination — you involve security or police first, because a report to a child-protection authority is not an emergency response to an immediate physical threat. [8]
Assess the injury or presentation with the same rigour you would bring to any clinical encounter, but with an added lens. Document the injury type, location, age and pattern. Note whether the mechanism described is developmentally plausible — a pre-mobile infant cannot self-inflict a spiral fracture, and a toddler rarely bruises the pinna or torso. The Ten 4-BODY-P pattern (bruising to the torso, ear, neck, or in a pre-mobile infant, any bruise) is a validated screening tool for inflicted injury. [13]
Take a careful, non-leading history. Ask open questions, record the child's and carer's exact words in quotation marks, and note discrepancies between accounts and between the history and the injury. Do not conduct an investigative or forensic interview — that is the agency's role — but do capture what is said in the clinical encounter faithfully and contemporaneously. [8]
Examine the child fully, including an unclothed top-to-toe examination, and document findings with a body map and clinical photographs where possible. Look for sentinel injuries, patterned marks, and signs of neglect. Document the developmental stage, growth parameters, and interaction between child and carer, because these observations contribute to the overall assessment. [8] [13]
Assess for occult injury if an inflicted injury is suspected. A skeletal survey in children under two, neuroimaging if abusive head trauma is possible, and targeted laboratory screening for differential diagnoses are part of the clinical assessment — and their results may strengthen or allay the concern that drives a report. [13]
Consult your senior clinician, the hospital child-protection team or social work before making the notification in non-emergent cases. A second opinion strengthens the assessment, ensures the threshold is met, and builds team consensus — but it does not transfer your individual statutory duty, and you remain the person who must ensure the report is made. [6] [8]
Investigations
There is no blood test for a reasonable belief, but several investigations confirm the scope of injury and the differential diagnosis that a reporting decision and a clinical plan rest on. These investigations are part of clinical care, not part of the child-protection investigation, and their results belong in the medical record. [13]
A skeletal survey is the core investigation for suspected physical abuse in children under two years (some guidelines extend to under three). It identifies occult fractures — particularly healing posterior rib fractures, classic metaphyseal lesions, and scapular, sternal or spinous process fractures — that are highly specific for inflicted injury and may be clinically silent. A repeat skeletal survey at 11–14 days captures fractures that were not visible acutely. [13]
Neuroimaging is indicated when abusive head trauma is suspected. CT head is the acute modality for identifying intracranial injury and is performed promptly in an unstable child; MRI brain adds sensitivity for parenchymal injury, diffuse axonal injury and extra-axial collections, and is performed when the child is stable. Ophthalmology assessment for retinal haemorrhages is part of the workup when head trauma is suspected. [8]
Laboratory investigations address the differential diagnosis rather than diagnosing abuse directly. A bleeding screen (coagulation studies, full blood count, von Willebrand panel) excludes a bleeding diathesis that could explain bruising; bone health markers and a metabolic screen may be considered for unexplained fractures; and a toxicology screen may be indicated if ingestion or poisoning is suspected. [8]
Forensic examination for suspected sexual abuse should be performed by a clinician trained in forensic paediatric examination, within the appropriate evidence-gathering window, and with consent. The forensic examination serves both a clinical purpose (injury identification, sexually transmitted infection screening, emergency contraception, prophylaxis) and an evidentiary purpose, so it follows a chain-of-custody protocol. [8]
A child-protection medical consultation functions as an adjunct to the assessment. A specialist child-protection paediatrician brings expertise in injury interpretation, investigation protocols, and the interface between clinical care and the statutory system, and their involvement strengthens both the clinical and the legal robustness of the case. [8]
When the clinical picture is genuinely ambiguous and the threshold has not yet crystallised, the appropriate 'investigation' is the multidisciplinary discussion itself — a case review with senior colleagues, social work and the child-protection team to decide whether the concern now meets a reportable threshold. [6]
Management — Resuscitation
When a child presents with an acute inflicted injury, you treat the injury first. A fractured femur, a burn, an intracranial bleed or a visceral injury demands the same resuscitation and stabilisation as any trauma — the mechanism of injury does not change your immediate ABC priorities. [8]
Assess and secure the child's immediate physical safety. If the alleged perpetrator is present and poses a risk, involve hospital security or police before further assessment. If the child cannot be safely discharged home, they may need to remain in hospital under a holding arrangement while the child-protection authority is notified and responds. [8]
Distinguish an acute, reversible injury from the ongoing risk. A child with a inflicted burn needs wound care now, but the larger question is whether they can return to the environment where the burn occurred. Your clinical treatment and the safety assessment run in parallel — you do not defer one for the other. [8]
If the child discloses abuse during resuscitation or assessment, listen, acknowledge, and document verbatim. Do not conduct a detailed investigative interview in an acute clinical setting — the priority is clinical stabilisation, with the disclosure recorded faithfully for the child-protection process that will follow. [16]
Allocate roles so that clinical care and the reporting pathway run in parallel. One clinician leads resuscitation, another documents and prepares the notification, and a third supports the child and family. The report should be made promptly once the child is stable — a delay of hours is acceptable for clinical reasons; a delay of days is not. [8]
Reframe the report to the family as an act of care, not accusation. Explain honestly and without judgement that the injury pattern or disclosure has triggered a duty to notify the child-protection authority, that the agency's role is to assess and support, and that you will continue to care for the child throughout. The family's anger is expected and does not change the obligation. [6] [8]
Management — Definitive & Stepwise
Use a sequence you can defend out loud in a viva, anchored on the reasonable-belief threshold and your local reporting protocol. [1] [8]
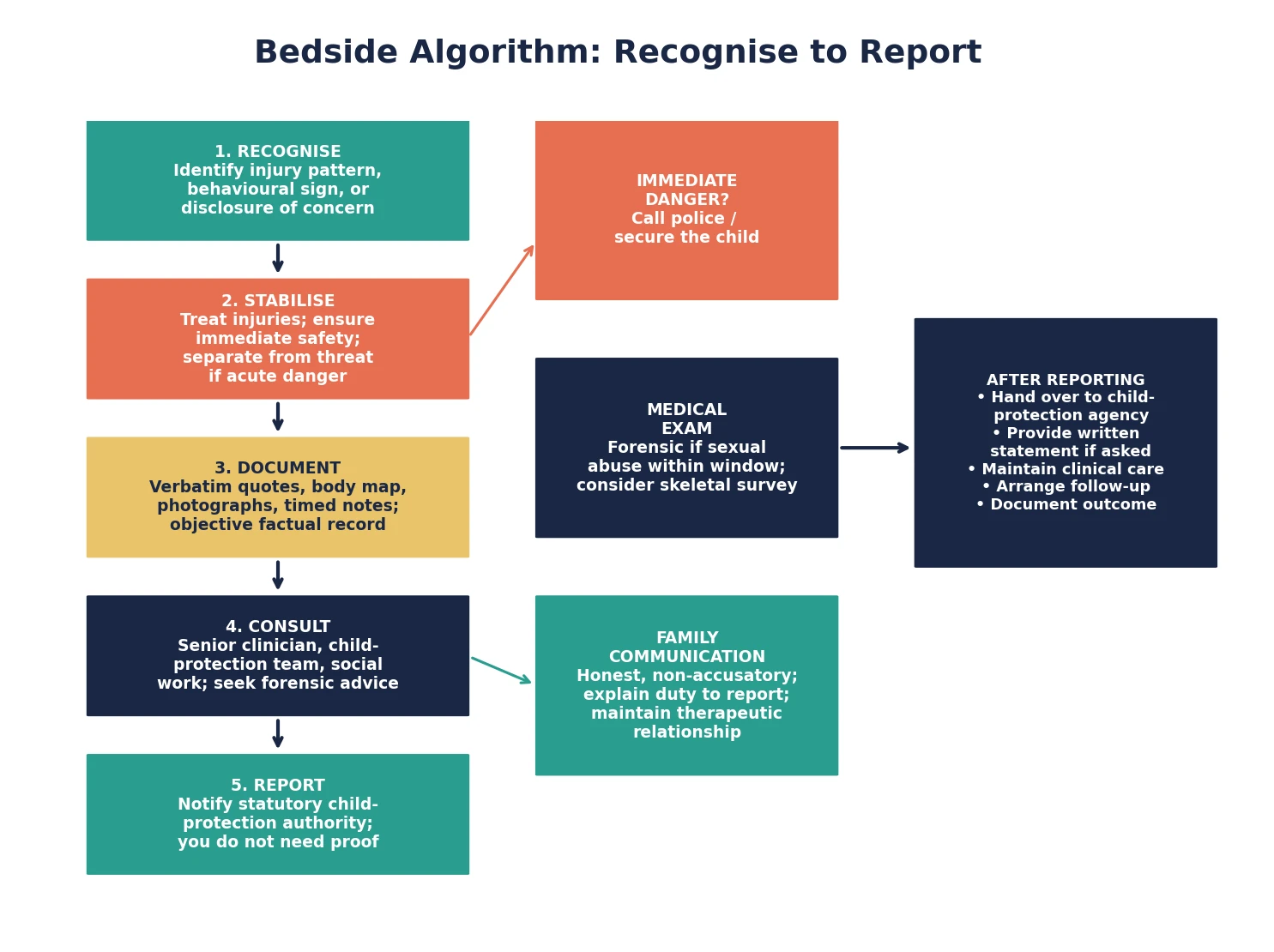
Recognise-to-report algorithm
Recognise the concern — injury pattern, behavioural sign, disclosure, or risk constellation
Stabilise and treat acute injury; secure immediate safety
Document contemporaneously — verbatim quotes, body map, photographs, timed notes
Consult your senior, the child-protection team or social work
Confirm you are a mandated reporter for this abuse type in this jurisdiction
Notify the statutory child-protection authority via the correct local pathway
Communicate honestly with the family — explain the duty and maintain the relationship
Arrange clinical follow-up, psychological support and handover to ongoing care
After the notification, your clinical responsibility continues. Complete the investigation and treatment plan, arrange follow-up, and provide a written report or statement if the agency or the court requests one. Maintain the therapeutic relationship with the child and family, because most children remain in the care of their families after a report, and the clinician who reported may also be the clinician who provides ongoing care. [6]
Document the notification itself — who you spoke to, at what time, what information you provided, and what the agency advised. This record protects you professionally, provides continuity if the case returns, and demonstrates that the statutory duty was discharged. If the agency decides not to investigate, and your concern persists, you may re-report, escalate within the agency, or seek advice from your medical defence organisation. [1] [2]
Handle the family conversation with honesty, respect and without accusation. Avoid conjecture about who caused the injury, because that is for the investigation to determine. State what you are required to do, explain why, and offer to remain involved. A family that feels respected through the process is more likely to engage with support services and less likely to disengage from health care altogether. [6]
Ensure information sharing is lawful and purposeful. Statutory reporting protections generally allow you to share relevant clinical information with the child-protection authority for the purpose of protecting a child, overriding common-law confidentiality obligations. Share what is relevant and necessary, document what you shared and why, and do not share beyond what the protective purpose requires. [1]
Specific Subtypes & Scenarios
Pre-mobile infant with a bruise. Any bruise in a non-ambulant infant is a sentinel injury until proved otherwise. Perform a skeletal survey, consult the child-protection team, and report — the probability that a pre-mobile infant's bruise is inflicted is high enough that deferral is not defensible. Lindberg and colleagues showed that many such infants have occult injuries identified only on further workup. [13]
Inconsistent-injury presentation in a toddler. The mechanism does not fit the developmental stage or the injury pattern. Document the history from each informant separately and verbatim, note the discrepancies, perform a full examination with body map, and report if a reasonable belief crystallises. Consult the child-protection team if the picture is ambiguous. [8]
Child sexual abuse disclosure. Listen, believe, document verbatim, and do not promise secrecy. Arrange a forensic examination by a trained clinician within the evidence-gathering window, offer sexually transmitted infection screening, emergency contraception and prophylaxis as indicated, and report to the child-protection authority. The child's response to the first disclosure powerfully shapes their recovery. [16]
Exposure to domestic violence. Exposure to intimate-partner violence is itself a form of child maltreatment in many jurisdictions. Assess the child's safety in the home, report if the threshold is met, and coordinate with domestic-violence services for the non-offending parent and child. Cross and colleagues showed that child-welfare responses to domestic violence exposure vary sharply between systems. [14]
Child with disabilities and unexplained distress. Behavioural change, regression, self-injury or distress in a child with communication barriers may reflect maltreatment that is being overshadowed by the disability. Maintain a high index of suspicion, involve carers who know the child's baseline, and report if the concern meets the threshold. Legano and colleagues emphasised that this population is at substantially elevated risk and is frequently missed. [15]
Adolescent disclosing historical abuse. An adolescent may disclose abuse that occurred years ago and ask you not to report it. Assess current risk, explain your duty honestly, and involve the young person in decisions about how the report proceeds where it is safe to do so — respecting emerging autonomy while discharging the statutory duty. Consider confidentiality limits and the mature-minor framework where relevant. [16]
Migrant or refugee family with neglect concerns. Poverty, housing insecurity, language barriers and unfamiliarity with local services can present as neglect that is driven by structural disadvantage rather than parental failure. Report if the threshold is met, but also advocate for material support, interpreter access, and culturally appropriate services so that the response addresses the cause, not only the symptom. [8]
Clinician uncertainty at the threshold. You have a concern but are not sure whether it meets the reasonable-belief test. The correct response is to consult — a senior colleague, the child-protection team, or the agency's advice line — and to document the consultation. Silence because of uncertainty is the most common reason a reportable concern goes unreported. [6]
Complications & Pitfalls
- Waiting for certainty or proof before reporting — the threshold is a reasonable belief, not a conviction. [1]
- Conflating the clinical role with the investigative role — you report, the agency investigates. [8]
- Failing to document contemporaneously — late or retrospective notes lose evidentiary value. [8]
- Conducting a leading or investigative interview that contaminates the forensic process. [8]
- Assuming the mandatory-reporting law is uniform across jurisdictions — it is not. [1]
- Promising a child secrecy, or failing to explain the duty to report honestly. [16]
- Not knowing the local reporting pathway, phone number or form before you need it. [6]
- Letting fear of damaging the therapeutic relationship override a threshold belief. [6]
- Treating the report as the endpoint — ongoing clinical care and advocacy continue. [2]
- Sharing information beyond what the protective purpose requires, or failing to share when the threshold is met. [1]
Prognosis & Disposition
A well-made report pays off when it connects a child and family to support, assessment and protection they would otherwise not receive. For the child at acute risk, a report may be the intervention that removes them from danger; for the family under stress, it may be the door to services that strengthen their capacity to care. [2] [9]
The immediate disposition depends on the clinical and safety assessment. A child with an acute inflicted injury may need admission for treatment and observation; a child who cannot safely return home may remain in hospital or be placed in emergency out-of-home care by the agency; a child whose concern does not meet an acute-risk threshold may be discharged with a safety plan, follow-up and a report in train. [8]
A report that the agency decides not to investigate is not necessarily a failure, and it does not end your responsibility. If your concern persists — new injuries, escalating disclosures, a deteriorating developmental trajectory — you re-report, escalate within the agency, or seek advice. The child-protection system is imperfect, and persistent clinical advocacy is part of your role. [2]
Follow-up belongs to the disposition, not an afterthought. Arrange a review appointment, ensure the family knows who to contact, and coordinate with the child-protection authority, general practitioner, school and any support services involved. A child who has been reported needs the same continuity of care as any child with a complex, ongoing problem. [8]
Staff support and debrief matter after a difficult report, particularly when the family is known to the team or the case is emotionally charged. A structured debrief helps clinicians process the encounter, and it reinforces that reporting is a professional duty discharged in the child's interest, not a personal accusation. [6]
Special Populations
Infants and pre-mobile children. Any bruise or injury in a non-ambulant infant is high-risk; the threshold for skeletal survey and report is low. Sentinel injuries in this age group carry a high probability of occult inflicted injury, and deferral is not defensible. [13]
Children with disabilities. Maintain a high index of suspicion — this group is at substantially elevated maltreatment risk, and communication barriers, behavioural presentations and diagnostic overshadowing obscure the signs. Involve carers who know the child's baseline, and do not attribute changes to the disability without assessment. [15]
Adolescents and mature minors. Respect emerging autonomy while discharging the statutory duty. Involve the young person in decisions about how the report proceeds where it is safe to do so, and consider the mature-minor framework and confidentiality limits where relevant. An adolescent who discloses historical abuse needs the same honest explanation of duty as any other patient. [16]
Indigenous families. Apply trauma-informed, culturally safe practice. Acknowledge the history of statutory child-protection systems in Indigenous communities, identify kinship and community supports, and advocate for responses that strengthen rather than fragment family connections. The duty to report remains, but how you communicate and which supports you engage matter profoundly. [8]
Migrant and refugee families. Use professional interpreters, pace the conversation for trauma, and distinguish structural disadvantage (poverty, housing, isolation) from parental failure. Report if the threshold is met, but also advocate for the material and social supports that address the underlying drivers. [8]
Children in out-of-home care. These children are known to the child-protection system but remain vulnerable to further maltreatment. Identify the current statutory guardian for consent and notification purposes, and recognise that a new concern may require a report to the same or a different authority depending on the placement and the guardianship order. [8]
Families affected by domestic violence. Coordinate the child's safety with the non-offending parent's safety. A report that removes a child but leaves a non-offending parent in danger may not serve the family system, so engage domestic-violence services and ensure a coordinated response across child protection and adult services. [14]
Evidence, Guidelines & Regional Differences
Mathews and Kenny's 2008 cross-jurisdictional review remains the foundational comparative analysis of mandatory-reporting legislation across the United States, Canada and Australia, documenting how each country structures who must report, what triggers a report, and what protections and penalties apply. It framed the field and remains the reference examiners expect. [1]
Tonmyr and Mathews' 2018 legal-doctrinal review asked the harder question: does mandatory-reporting legislation actually increase meaningful contact with child-protection systems and improve outcomes? Their answer is nuanced — reporting volume rises, but the link between more reports and better child outcomes depends on system resourcing and response capacity. [2]
Mathews and colleagues' 2016 seven-year time-trend analysis provided empirical evidence that a new mandatory-reporting law for child sexual abuse was associated with sustained increases in reporting and identification, addressing the concern that broader mandates merely generate unsubstantiated notifications. [3]
On the clinician side, Flaherty and Sege identified the barriers to physician identification and reporting, and Flaherty and colleagues documented how paediatrician characteristics — training, confidence, prior experience — predict reporting behaviour. Fraser and colleagues found parallel patterns in nurses, with training and protocol access the strongest enablers. The Walsh and Mathews Cochrane review synthesised the evidence that child-protection training for professionals improves recognition and reporting. [4] [5] [6] [7]
Gilbert and colleagues' Lancet series established the epidemiological and comparative-policy frame: child maltreatment is common and substantially under-reported, and child-protection systems across developed countries vary markedly in their thresholds, substantiation rates and responses. Finkelhor and colleagues' prevalence surveys showed the true population burden of childhood violence and abuse, and Mathews and Finkelhor's 2024 meta-analysis documented the prevalence of child sexual abuse by perpetrator type. [8] [9] [10] [11] [12]
In Australia, mandatory-reporting legislation is enacted at the state and territory level, so the scope of who must report what varies across New South Wales, Victoria, Queensland, Western Australia, South Australia, Tasmania, the Australian Capital Territory and the Northern Territory. Some jurisdictions have universal mandates covering all abuse types for broad professional groups; others limit the duty to specific professions and abuse types. The reporting pathway is to the state or territory child-protection authority, typically via a dedicated helpline or online notification. In Aotearoa New Zealand, reporting is to Oranga Tamariki. State the principle — mandatory reporting is a statutory duty triggered by a reasonable belief, and the scope and pathway vary by jurisdiction — and direct examiners to local statute and hospital policy for operational detail. Never invent a specific section number or a named act. [1] [3]
Exam Pearls
REPORT
References
- [1]Mathews B, Kenny MC Mandatory reporting legislation in the United States, Canada, and Australia: a cross-jurisdictional review of key features, differences, and issues. Child Maltreatment, 2008.PMID 18174348
- [2]Tonmyr L, Mathews B, Shields ME, Hovdestad WE Does mandatory reporting legislation increase contact with child protection? - a legal doctrinal review and an analytical examination. BMC Public Health, 2018.PMID 30115126
- [3]Mathews B, Lee XJ, Norman RE Impact of a new mandatory reporting law on reporting and identification of child sexual abuse: a seven year time trend analysis. Child Abuse & Neglect, 2016.PMID 27155543
- [4]Walsh K, Eggins E, Hine L, Mathews B Child protection training for professionals to improve reporting of child abuse and neglect. Cochrane Database of Systematic Reviews, 2022.PMID 35788913
- [5]Fraser JA, Mathews B, Walsh K, Chen L, Dunne M Factors influencing child abuse and neglect recognition and reporting by nurses: a multivariate analysis. International Journal of Nursing Studies, 2010.PMID 19540493
- [6]Flaherty EG, Sege R Barriers to physician identification and reporting of child abuse. Pediatric Annals, 2005.PMID 15948346
- [7]Flaherty EG, Sege R, Price LL, Christoffel KK, Norton DP, O'Connor KG Pediatrician characteristics associated with child abuse identification and reporting: results from a national survey of pediatricians. Child Maltreatment, 2006.PMID 17043321
- [8]Gilbert R, Kemp A, Thoburn J, Sidebotham P, Radford L, Glaser D, MacMillan HL Recognising and responding to child maltreatment. Lancet, 2009.PMID 19056119
- [9]Gilbert R, Fluke J, O'Donnell M, Gonzalez-Izquierdo A, Brownell M, Gulliver P, Janson S, Sidebotham P, Goldhagen J, Tarren-Sweeney M, Heimpel H Child maltreatment: variation in trends and policies in six developed countries. Lancet, 2012.PMID 22169108
- [10]Finkelhor D, Jones L Trends in child maltreatment. Lancet, 2012.PMID 22656877
- [11]Finkelhor D, Turner HA, Shattuck A, Hamby SL Prevalence of childhood exposure to violence, crime, and abuse: results from the national survey of children's exposure to violence. JAMA Pediatrics, 2015.PMID 26121291
- [12]Mathews B, Finkelhor D, Pacella R, Collin-Vezina D, Fallon B, Gerber N, Hébert M, Plourde C, Thorpe D Child sexual abuse by different classes and types of perpetrator: prevalence and trends from a meta-analysis of Australian studies. Child Abuse & Neglect, 2024.PMID 38061281
- [13]Lindberg DM, Beaty B, Juarez-Colunga E, Wood JN, Runyan DK Testing for abuse in children with sentinel injuries. Pediatrics, 2015.PMID 26438705
- [14]Cross TP, Mathews B, Tonmyr L, Scott D, Ou S Child welfare policy and practice on children's exposure to domestic violence. Child Abuse & Neglect, 2012.PMID 22425164
- [15]Legano LA, Desch LW, Messner SA, McHugh MT, Wilson MD, Lai JE, Hyman DH Maltreatment of children with disabilities. Pediatrics, 2021.PMID 33875536
- [16]Morrison SE, Bruce C, Wilson S Children's disclosure of sexual abuse: a systematic review of qualitative research exploring barriers and facilitators. Journal of Child Sexual Abuse, 2018.PMID 29488844