Paeds · child-safety-and-social-paediatrics
Medical neglect and refusal of care
Also known as Medical neglect · Refusal of care · Treatment refusal · Parental refusal of medical treatment · Religious refusal of treatment · Vaccine refusal
Fellowship guide to medical neglect and refusal of care in children — the failure to seek, attend or comply with medically necessary treatment and the active parental refusal of recommended care on religious, ideological or personal grounds. Covers the Diekema harm-principle threshold for state intervention, the best-interests standard, the four classic refusal scenarios (vaccines, vitamin K, blood transfusion for Jehovah's Witness families, cancer chemotherapy), the mature-minor doctrine and contested adolescent refusals, a stepped engagement-to-escalation management plan that negotiates first and escalates to court orders when the harm threshold is met, and the regional legal frameworks across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old with newly diagnosed acute lymphoblastic leukaemia is brought by parents who have decided to treat the cancer with herbal remedies and dietary changes instead of chemotherapy. The first question an examiner wants you to hold is not "are these bad parents?" but "is this child at risk of significant harm from a failure to receive effective treatment, and if so, what is my duty?" Medical neglect and refusal of care together describe the spectrum of situations in which a child does not receive medically necessary treatment — whether through omission (neglect) or active rejection (refusal) — and the clinician must decide when to respect parental autonomy and when to override it. [2] [3]
The working definition of medical neglect is operational rather than legal: a caregiver who has the responsibility and capacity to do so fails to provide, seek, or follow through with medical care that the child needs, to a degree that causes or risks harming the child's health or development. Jenny, writing for the AAP Committee on Child Abuse and Neglect, framed medical neglect as a failure to meet a clear and documented medical need — missed appointments, non-compliance with essential medications, delay in seeking care for a deteriorating condition, and refusal of recommended treatment. What makes it neglect rather than circumstance is the adequacy of the caregiving response relative to the severity of the child's medical need. [2] [5]
Refusal of care deserves its own name because it presents as an active decision rather than passive omission. A parent who declines vaccines on ideological grounds, a Jehovah's Witness family who refuses blood products for their bleeding child, or a family who rejects chemotherapy for a curable cancer are each making a deliberate choice — and the clinician's task is to respect that choice up to the point where the child faces significant, imminent and preventable harm. The distinction between access barriers (poverty, transport, health literacy, system failure) and deliberate refusal matters enormously, because the first calls for support and advocacy while the second calls for negotiation and, if needed, legal intervention. [1] [3]
The broader neglect framework, the six-domain classification, and the multi-agency assessment live on the neglect-and-supervisory-neglect leaf. This page owns medical neglect and refusal of care as the clinical-ethics interface — the point where unmet medical need meets parental authority, the harm threshold, and the legal duty to act. [2] [5]
Classification
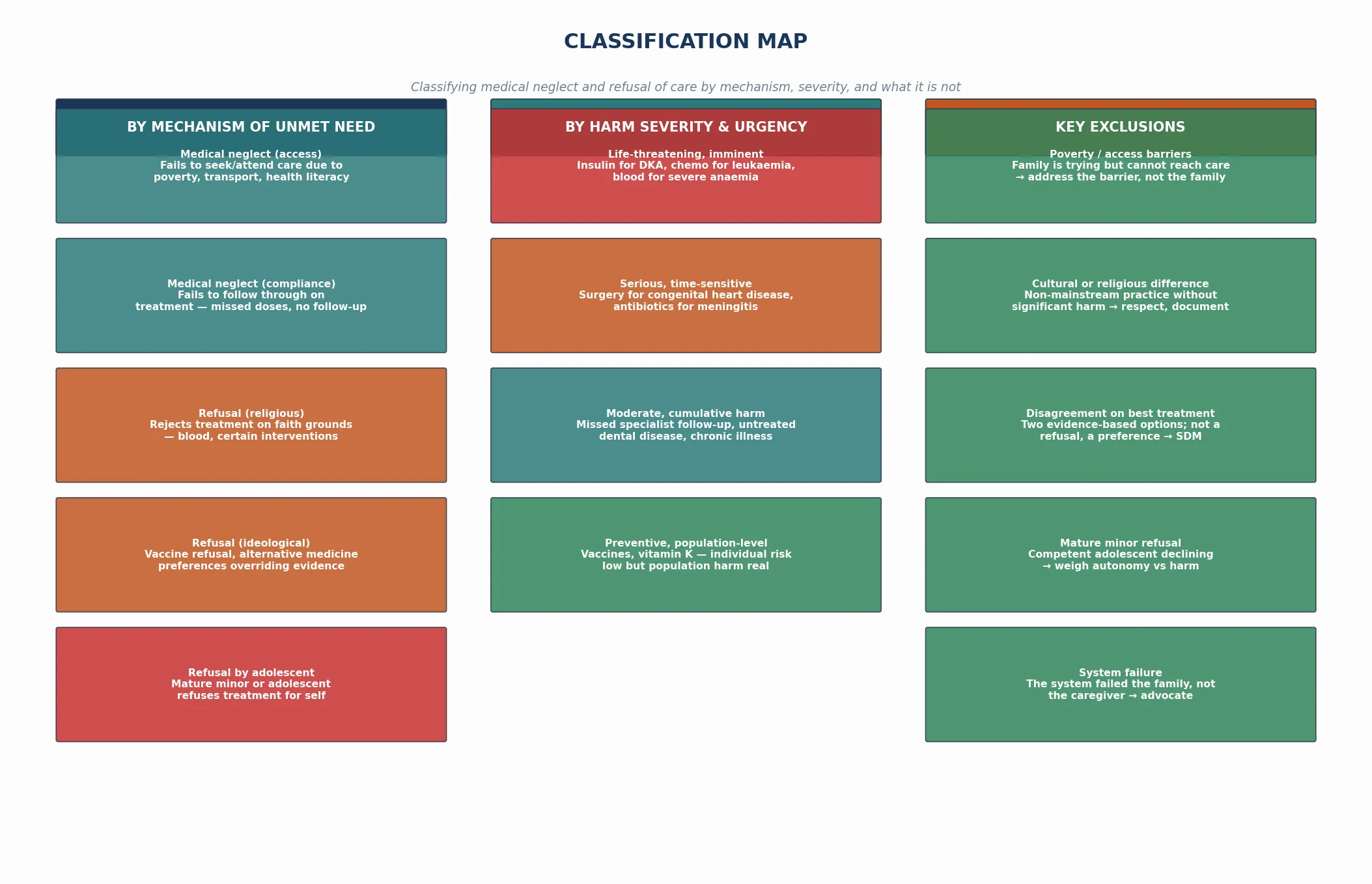
Sort every case of unmet medical need along three axes before you name the response: what is the mechanism of the unmet need, how severe and imminent is the potential harm, and what is the exclusion that changes the plan. The same missed appointment means something different in a family who cannot afford transport than in one who has decided the treatment is unnecessary. [3] [4]
By mechanism of unmet need
| Mechanism | What the caregiver does | Presenting clue |
|---|---|---|
| Medical neglect (access) | Cannot reach care — poverty, transport, health literacy, system failure | Late presentation, missed appointments, no GP engagement |
| Medical neglect (compliance) | Fails to follow through — missed doses, no follow-up, lost prescriptions | Deteriorating chronic disease, recurrent admissions |
| Refusal (religious) | Rejects treatment on faith grounds — blood products, certain interventions | Jehovah's Witness family, faith-healing communities |
| Refusal (ideological) | Rejects treatment on belief — vaccines, alternative medicine preferences | Vaccine refusal, vitamin K refusal, herbal treatment for cancer |
| Refusal by adolescent | Competent young person declines treatment for themselves | Mature minor refusing chemotherapy or blood products |
Medical neglect versus refusal of care — omission versus rejection
- Passive failure to seek, attend or comply with care
- Often driven by access barriers, overwhelm, or capacity limitation
- First response: support, advocacy, address the barrier
- Report when the threshold for significant harm is met
- Deliberate decision to reject recommended treatment
- Driven by religious belief, ideology, or personal conviction
- First response: negotiate, inform, shared decision-making
- Escalate to court order when the harm threshold is met
By harm severity and the exclusions
The severity of potential harm drives the urgency of the response. A child with diabetic ketoacidosis whose parents refuse insulin faces imminent, life-threatening, preventable harm — that is above the Diekema threshold, and the clinician acts without delay. A child whose parents refuse a routine vaccine faces a lower individual risk but a real population-level risk, and the response is negotiation, harm reduction, and follow-up rather than a court order. The exclusions examiners probe are poverty and access barriers, genuine cultural or religious difference that does not cause significant harm, disagreement between two evidence-based options, and the mature minor's own refusal — each of which changes the plan from legal escalation to respect and support. [1] [11]
[1] [3] [11]Epidemiology & Risk Factors
Medical neglect is one of the most common forms of neglect encountered in clinical practice, yet it is also one of the most inconsistently reported, because the line between access failure and deliberate omission is genuinely difficult to draw. Jenny, writing for the AAP Committee on Child Abuse and Neglect, identified medical neglect as a recurring pattern in which children present with worsening disease that appropriate and available treatment would have prevented — and the prevalence is driven by the same factors that drive neglect broadly. [2] [13]
What places a child at risk? Medical neglect clusters where caregiver capacity is overwhelmed: parental mental illness, substance use, intellectual disability, social isolation, and severe socioeconomic hardship. Ward and Baird emphasised that medical neglect is rarely a single event — it is a pattern of missed appointments, unfilled prescriptions, and delayed presentations that accumulates harm over time. Families with limited health literacy, language barriers, or transport difficulties are over-represented, and the risk is highest in children with chronic, complex conditions who depend on sustained engagement with the medical system. [4] [5]
Refusal of care has a different epidemiology. Vaccine refusal is concentrated in communities with specific ideological clusters, and Phadke and colleagues demonstrated that non-medical vaccine exemptions are associated with increased measles and pertussis outbreaks — the population harm is real even when the individual risk is low. Vitamin K refusal tracks alongside vaccine refusal, and Sahni showed that mothers who refuse vitamin K are far more likely to also refuse immunisation. Cancer treatment refusal is rare but devastating, and Caruso Brown's systematic review found that refusal is most common in families with strong alternative-medicine beliefs or who distrust the conventional system. [7] [8] [9]
Pathophysiology
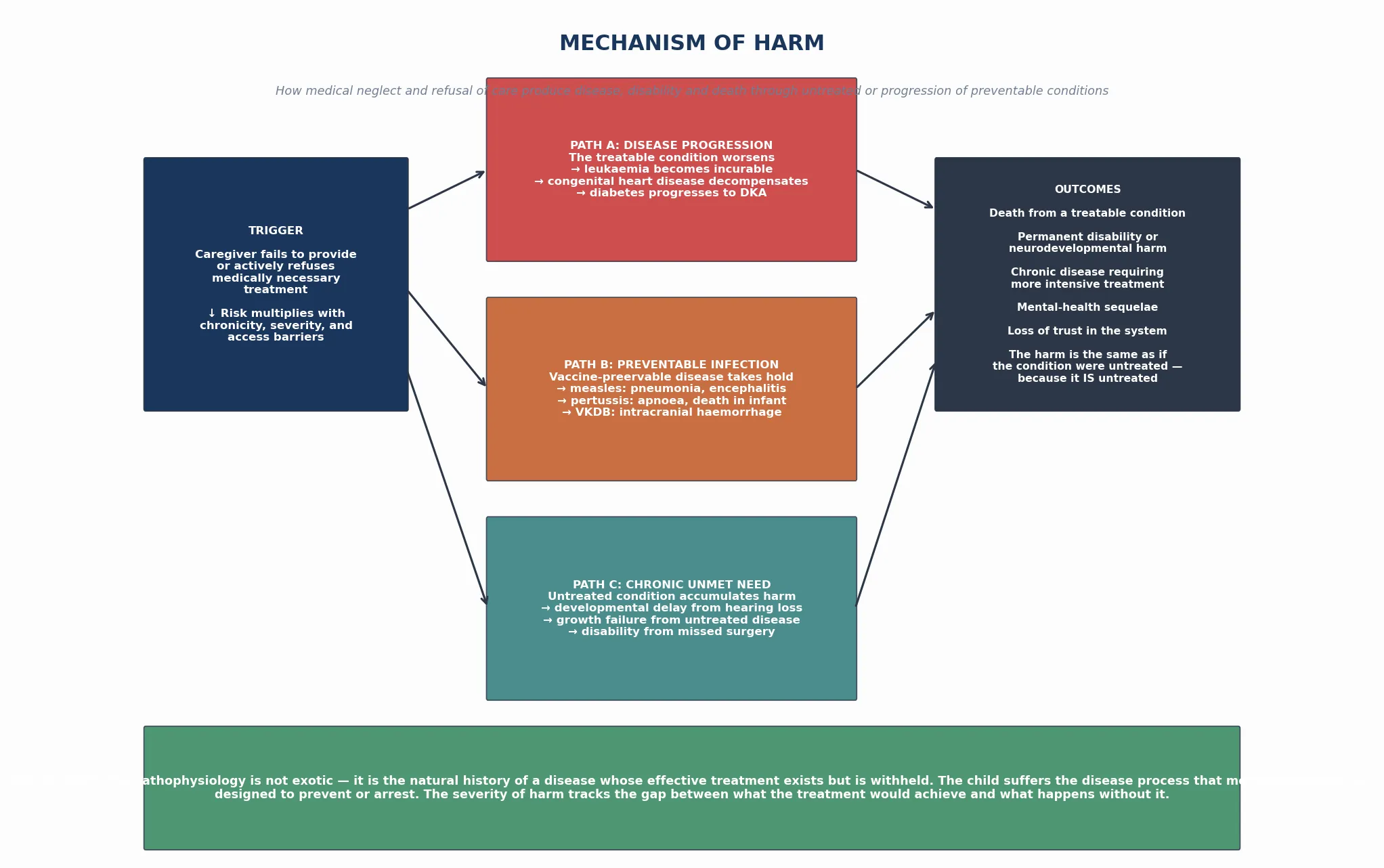
The harm in medical neglect and refusal of care is not exotic — it is the natural history of a disease whose effective treatment exists but is withheld. The child suffers the disease process that modern medicine was designed to prevent or arrest, and the severity of the harm tracks the gap between what the treatment would achieve and what happens without it. [2] [13]
The mechanisms track the scenario. When parents refuse insulin for a child with diabetes, the pathophysiology is straightforward diabetic ketoacidosis — dehydration, electrolyte derangement, cerebral oedema, and death — precisely as if the insulin had never been discovered. When parents refuse chemotherapy for a child with acute lymphoblastic leukaemia, the leukaemia progresses unchecked, and a disease with a ninety per cent cure rate becomes uniformly fatal. When parents refuse vaccines, the child is exposed to pathogens that herd immunity would otherwise prevent, and the disease — measles pneumonia, pertussis apnoea, haemophilus meningitis — runs its natural course. [7] [9]
The vitamin K refusal pathway deserves specific attention. Sahni demonstrated that infants whose parents refuse intramuscular vitamin K at birth are at risk of late vitamin K deficiency bleeding, which typically presents between two and twelve weeks as intracranial haemorrhage — a catastrophic, often fatal or neurologically devastating event that a single injection would have prevented. The mechanism is the same vitamin K dependent clotting factor deficiency that the prophylaxis was designed to address. [8]
The Jehovah's Witness blood-transfusion refusal operates through the pathophysiology of severe anaemia and coagulopathy. Conti and colleagues described how the refusal of blood products in a child with acute blood loss or severe chronic anaemia leads to tissue hypoxia, cardiovascular collapse, and death — and the threshold for overriding parental refusal is lower in a child than in an adult because the child cannot consent to the refusal on their own behalf. [6]
Clinical Presentation
Parents rarely lead with "I am refusing treatment for my child." They bring a child with a worsening condition, a missed appointment pattern, or a specific treatment decision — and the task is to identify the unmet medical need and assess its consequences. The presentation is as varied as the conditions themselves. [2] [4]
Medical neglect presents through the consequences of untreated or under-treated disease. A child with asthma who has recurrent admissions because the preventer is never collected. An infant with faltering growth because the feeding plan was never followed. A child with congenital heart disease who deteriorates because the surgical referral was missed. A child with epilepsy who has uncontrolled seizures because the anticonvulsant is given inconsistently. The unifying feature is a gap between what the child needs and what they are receiving. [4] [13]
Refusal of care presents at a decision point. A family at the newborn check who declines vitamin K. A family at the immunisation visit who declines the schedule. A family at the oncology consultation who declines chemotherapy. A Jehovah's Witness family at the surgical consent who decline blood products. In each case the refusal is explicit, documented, and the clinician's task is to assess harm, negotiate, and decide whether the threshold for intervention is met. [1] [3]
Differential Diagnosis
Build the differential in layers: the things that drive medical neglect, the things that mimic refusal, and the coexisting factors that complicate the picture. The single most examined distinction is deliberate refusal from access failure, and getting it wrong in either direction harms the child. [1] [4]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Missed appointments, late presentations | Access-based medical neglect | Deliberate refusal if treatment is actively rejected when offered |
| Cannot afford transport or medication | Socioeconomic barrier — not neglect | If income support resolves the gap, the problem was access |
| Family declines one vaccine, accepts others | Selective refusal — negotiate | Total refusal if all vaccines rejected |
| Family declines blood products on faith | Religious refusal — Jehovah's Witness | Assess if alternative blood-sparing strategies suffice |
| Adolescent declines cancer treatment | Mature minor — assess competence | If not competent, parental consent governs |
| Family prefers alternative to chemotherapy | Ideological refusal | Assess if harm is imminent and treatment is curative |
| No GP engagement, no immunisations | Pattern of medical neglect | Single system failure if all else adequate |
The two mirror-image errors examiners test are over-calling medical neglect in a family whose only problem is access — which stigmatises and fails to offer help — and under-calling it by attributing a chronic pattern of unmet need to a single difficult period. When the mechanism and the caregiving response tell different stories, return to the harm threshold: is the child suffering, or likely to suffer, significant harm from the unmet need, and what response does that harm demand? [2] [5]
Clinical & Bedside Assessment
Lead with a non-judgemental, information-gathering approach. A parent who feels accused will disengage, and you lose the child. The goal is to understand what drives the unmet need or refusal — whether it is a barrier, a belief, or a misunderstanding — and to document what you find. [1] [3]
Medical-neglect and refusal-informed assessment sequence
Establish rapport and explore the reason
Curious, non-blaming stance; ask what the family understands about the condition and treatment; explore barriers, beliefs, and fears without dismissing them.
Assess the medical need and the gap
What treatment is being withheld or refused? What is the condition, its natural history untreated, and the expected benefit of treatment?
Apply the harm threshold
Is the child at significant risk of serious harm? Is the harm imminent? Is the treatment likely to be effective? Is the burden proportionate? (Diekema)
Separate access barriers from refusal
Poverty, transport, health literacy, and system failure call for support; deliberate religious or ideological refusal calls for negotiation and possible escalation.
Assess caregiver capacity
Mental illness, substance use, intellectual disability, overwhelm — capacity frames the response and may shift from legal to supportive.
Document the refusal verbatim
Record the information given, the family's understanding, the specific treatment refused, the harm assessment, and the plan — the record is what defends the decision.
Formulate and decide the threshold
Negotiate versus escalate to court order; involve ethics and legal teams early; named lead and safety-net; never close the file on one conversation.
Assess the child clinically. Is there current harm from the unmet need? Is the condition stable or deteriorating? What is the trajectory without treatment? The clinical assessment grounds the harm assessment in observable fact rather than theoretical risk, and a deteriorating child is above the threshold for intervention regardless of the parent's stated reasons. [2] [13]
Assess the family's understanding of the condition, the treatment, and the consequences of refusal. A family that declines chemotherapy may hold misconceptions about survival rates, side effects, or alternatives that clear information could address. The duty to provide accurate, comprehensible information about the risks and benefits of the recommended treatment and the consequences of refusing it is foundational — without it, the refusal is not fully informed. [1] [12]
Investigations
Medical neglect and refusal of care are clinical and contextual assessments, not laboratory diagnoses. There is no blood test, scan, or biomarker that confirms the unmet need — the workup is targeted at the medical consequences of the gap in care. [2] [4]
Investigate the condition itself. If the child has a deteriorating chronic disease because the treatment is not being given, investigate the current state of the disease — a haemoglobin in a child whose transfusion is refused, a blood gas in a child whose insulin is withheld, a skeletal survey if the pattern raises broader safeguarding concern. The investigation is guided by the medical need, not by the neglect. [4] [13]
Document the pattern of unmet need through multi-source information-gathering. With appropriate consent — or under child-protection authority when consent is refused and the threshold is met — obtain the general-practice record, the hospital records, the prescription-dispensing records, the immunisation history, and any prior child-protection involvement. A pattern of missed appointments, unfilled prescriptions, and late presentations across multiple settings is what confirms chronic medical neglect over a single episode. [2] [5]
Management — Resuscitation
"Resuscitation" in the context of medical neglect and refusal of care means immediate medical stabilisation of any harm already caused, and the end of any present danger from the unmet need. If a child presents in diabetic ketoacidosis because insulin was refused, you treat the DKA now — and the legal and ethical negotiation about ongoing insulin runs in parallel, not instead of the treatment. [1] [2]
Make a same-day safety plan: treat the medical emergency, secure the treatment that the child needs, assess whether the family can safely supervise the child in the interim, and escalate to child protection or a court order if the refusal poses imminent harm. Recognise that no negotiation or ethics consultation can run while a child is acutely dying of a treatable condition — stabilisation is the first act. [2] [3]
Management — Definitive & Stepwise
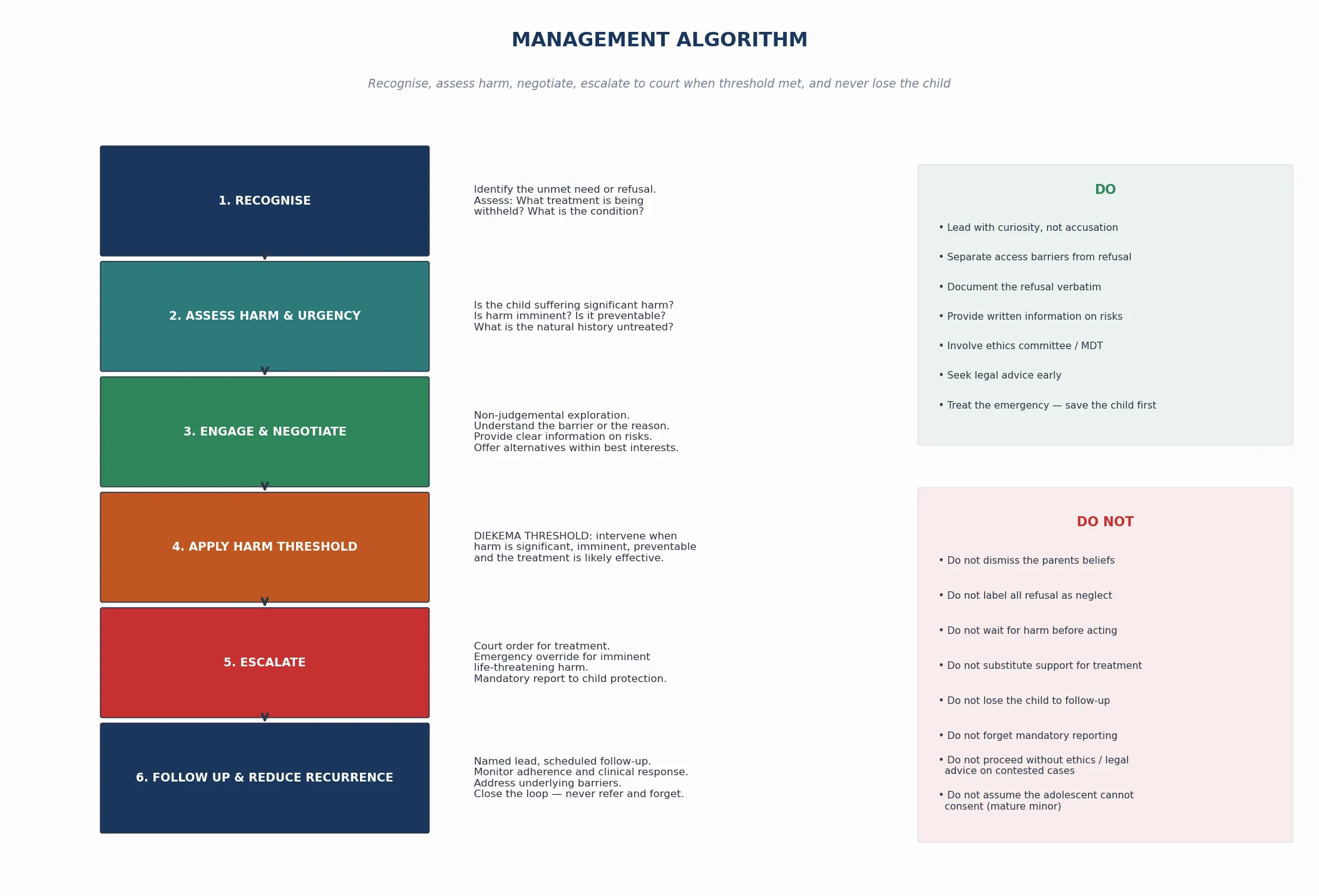
The management frame is stepped: recognise, assess harm, negotiate, apply the harm threshold, escalate to court or child protection when the threshold is met, and follow up to reduce recurrence. Negotiation and legal escalation are not opposites — the first is attempted before the second, and both serve the same goal of ensuring the child receives necessary treatment. [1] [12]
Step 1 — Recognise and assess harm
Identify the unmet need or refusal, assess the medical condition, and apply the Diekema harm threshold: is the child at significant risk of serious harm, is the harm imminent, is the treatment likely to be effective, and is the burden proportionate? The answer determines whether the plan is negotiation, support, or immediate escalation. [1] [11]
Step 2 — Engage and negotiate
Lead with a non-judgemental exploration of the family's reasons, provide clear and accurate information about the condition, the treatment, and the consequences of refusal, and offer alternatives that fall within the child's best interests where they exist. For Jehovah's Witness families, this means exploring blood-sparing surgical techniques, cell salvage, and erythropoietin. For vaccine-hesitant families, it means addressing specific concerns, offering a modified schedule if it meets minimum protection, and documenting the discussion. Most refusals are resolved through this step — the clinician who reaches straight for a court order without attempting negotiation has not met the standard. [1] [3]
Step 3 — Apply the harm threshold and escalate
When negotiation fails and the harm threshold is met, escalate. Seek a court order for treatment — the court acts in the child's best interests under parens patriae jurisdiction, and the order shifts the decision-making authority from the parent to the court. In an emergency, treat under the doctrine of necessity: if the child faces imminent death or serious harm and the treatment is life-saving, the clinician treats without parental consent and the court ratifies retrospectively. Make a mandatory child-protection report if the pattern of medical neglect meets the threshold for significant harm. [1] [2]
Step 4 — Follow up and reduce recurrence
Name the clinician who owns the plan, set the follow-up date, and document return precautions: deterioration, missed appointments, new refusal, or disclosure of harm. Medical neglect is chronic and recurrent, and a single court order or negotiation that resolves the immediate crisis does not close the file. Monitor adherence, the clinical response, and the family's ongoing engagement, and re-evaluate the threshold if risk resurfaces. [4] [5]
Specific Subtypes & Scenarios
Vaccine refusal. The most common refusal scenario in primary care. Phadke demonstrated the population-level harm of non-medical exemptions through increased measles and pertussis outbreaks, but the individual child's risk is often low in a well-immunised community. The response is negotiation: address specific concerns, provide clear information on risks and benefits, offer a catch-up schedule, document the refusal, and keep the door open at every visit. A court order is rarely sought for vaccine refusal alone, but the refusal must be documented and the child monitored for the consequences of the decision. [7]
Neonatal vitamin K refusal. Sahni showed that vitamin K refusal tracks alongside vaccine refusal and carries a real risk of late vitamin K deficiency bleeding — intracranial haemorrhage between two and twelve weeks of life. The response is clear information about the risk, harm reduction through oral vitamin K where the family will accept it (though oral regimens are less reliable), documentation, and vigilance for any bleeding presentation in the first months. [8]
Jehovah's Witness blood-transfusion refusal. Conti described the ethical and legal framework for refusing blood products on religious grounds. The clinician explores blood-sparing strategies, respects the family's faith up to the harm threshold, and seeks a court order when the child faces life-threatening anaemia or haemorrhage. Courts in ANZ, UK, US and Canada consistently override parental refusal of blood transfusion for children on the basis that the child's right to life outweighs the parents' religious freedom — the child cannot consent to their own martyrdom. [6]
Cancer treatment refusal. Caruso Brown's systematic review established that refusal of curative chemotherapy for childhood cancer is rare but devastating — a disease with a ninety per cent cure rate becomes uniformly fatal. The clinician negotiates intensively, involves the ethics committee, addresses fears about side effects and alternatives, and seeks a court order if the family persists in refusing treatment for a curable cancer. The threshold is met because the harm (death) is significant, imminent, and preventable. [9]
Mature minor refusal. Coleman and Rosoff established that competent adolescents may have the legal authority to consent to or refuse general medical treatment in many jurisdictions. Assess competence: does the young person understand the condition, the treatment, the consequences of refusal, and the alternatives? If competent, their refusal may carry weight — but courts have overridden even competent adolescent refusals of life-saving treatment, weighing the young person's developing autonomy against the gravity and irreversibility of the harm. [10]
Medical neglect in chronic disease. A child with a chronic condition — epilepsy, asthma, congenital heart disease — whose treatment is inconsistently given. The response addresses the access barriers and caregiver capacity, monitors adherence through objective measures (prescription dispensing, drug levels, clinic attendance), and escalates to child protection if the pattern causes significant harm despite support. [4] [13]
Faith-healing communities. Families who reject all conventional medicine on religious grounds present the starkest scenario — a child with appendicitis or pneumonia whose family relies on prayer. The threshold is met for any life-threatening condition with effective treatment, and the clinician seeks a court order immediately while documenting the family's beliefs and the medical need without dismissing the faith. [1] [2]
Complications & Pitfalls
- Assuming all refusal is medical neglect — a family that declines one vaccine but accepts the rest, or that prefers one evidence-based option over another, is not neglectful. [1]
- Waiting for the child to deteriorate before seeking a court order when the treatment window for a curative condition is closing. [9]
- Failing to document the refusal, the information given, and the harm assessment — the record is what defends the decision if it is later challenged. [2]
- Reaching straight for a court order without attempting negotiation — most refusals are resolved through respectful, informed conversation. [3]
- Treating access barriers as deliberate non-compliance — poverty and transport failure call for support, not legal intervention. [4]
- Assuming the adolescent cannot consent — a competent mature minor has authority over their own general medical treatment in many jurisdictions. [10]
- Losing the child to follow-up after a single negotiation — the file is never closed on one conversation, because patterns recur. [5]
Prognosis & Disposition
The prognosis of medical neglect and refusal of care is the prognosis of the underlying condition if it is treated versus if it is not. A child with acute lymphoblastic leukaemia who receives chemotherapy has a ninety per cent cure rate; a child who does not has zero. The gap between these outcomes is the measure of the harm, and it is what makes early intervention so critical. [9]
Recovery is possible when the treatment is provided and the engagement is sustained. Caruso Brown documented that most families who initially refuse cancer treatment will accept it after negotiation, ethics consultation, and time — which is why the clinician who attempts negotiation before escalation is practicing good medicine as well as good ethics. The prognosis improves when the barriers are addressed, the information is clear, and the family feels respected rather than coerced. [9] [12]
Disposition after successful negotiation: a documented plan of agreed treatment, named clinical lead, scheduled follow-up, and clear return precautions. [1] [3] Disposition when the threshold is met and negotiation fails: court order for treatment, child-protection report, and treatment under the order with the family supported throughout. [1] [2] Disposition for a pattern of medical neglect with access barriers: targeted support — transport, financial assistance, health-literacy education, care coordination — with monitoring and escalation if the pattern persists despite support. [4] [5]
Markers of a good outcome are the child receiving the treatment they need, the family engaging with the medical home, and no recurrence of the unmet need. The medical home carries the long view — sustained engagement, trust-building, and the addressing of barriers — because a single court order resolves the crisis but does not resolve the underlying drivers of the neglect or refusal. [4] [13]
Special Populations
Infants and young children are the most vulnerable because they cannot self-protect or articulate their unmet need, and the treatment window for many conditions is narrowest in early life. Assess vitamin K refusal, vaccine refusal, and delayed presentation closely in this group, because the consequences of unmet need are most severe when the child is smallest. [8] [13]
Adolescents occupy a unique position because they may have the legal authority to consent to or refuse their own treatment. Coleman and Rosoff established that competent mature minors can make general medical treatment decisions in many jurisdictions, but the threshold for overriding an adolescent's refusal of life-saving treatment is lower than for an adult — the developing autonomy, the irreversibility of the harm, and the presumption of future competence all weigh in favour of intervention. Assess competence carefully, document it, and involve ethics and legal teams when the stakes are high. [10]
Children with disability and chronic complex conditions are over-represented in medical neglect because they depend on sustained, intensive engagement with the medical system. A family that can meet the needs of a healthy child may be overwhelmed by the demands of a child with complex medical needs, and the response must address the caregiver-capacity gap alongside the medical need. Families with limited health literacy, language barriers, or migrant and refugee status need professional interpreters, culturally safe care, and targeted support that addresses the access barrier rather than labelling it as non-compliance. [4] [5]
Families living in socioeconomic hardship need a response that addresses the material determinants first — transport, financial assistance, prescription access — because a plan that ignores poverty cannot succeed. Indigenous families need non-stigmatising services that acknowledge intergenerational trauma and work with community-controlled organisations, because the history of child-protection intervention in Indigenous communities makes trust-building essential. [4]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [2]
- Diekema 2004 Theor Med Bioeth — the harm-principle threshold for state intervention when parents refuse treatment; the foundational four-condition test. [1]
- Jenny 2007 Pediatrics (AAP Committee on Child Abuse and Neglect) — the AAP policy on recognising and responding to medical neglect; the clinical approach and the criteria. [2]
- Boos and Fortin 2014 Pediatr Ann — the practical topic review of medical neglect in the broader context of child maltreatment. [3]
- Ward and Baird 2022 Paediatr Child Health — the working-with-families approach to medical neglect across clinical settings. [4]
- Salter and Hester 2023 Pediatrics — the consensus recommendations on paediatric decision-making that integrate the best-interests standard with the harm threshold. [12]
- Birchley 2016 J Med Ethics — the critical analysis of the harm principle and best interests in disputes about parental decision-making. [11]
In Australia, paediatricians are mandatory reporters in all states and territories; New Zealand has no mandatory reporting duty for health professionals (reporting is voluntary with good-faith protection). Medical neglect that meets the threshold for significant harm must be reported to the relevant child-protection authority. Court orders for medical treatment of a child are sought through the family court or the children's court under the parens patriae jurisdiction. The Family Court of Australia and the New Zealand High Court have consistently overridden parental refusal of blood transfusion for children of Jehovah's Witness families on the basis that the child's best interests — and right to life — outweigh parental religious freedom. The treating clinician should involve the hospital legal team and the child-protection unit early. [1] [2]
Controversies: where the line between access failure and deliberate neglect truly lies; the threshold for overriding a competent adolescent's refusal of life-saving treatment; whether religious exemptions for faith-healing should exist at all; how to balance parental authority with child autonomy in the mature-minor grey zone; and how to deliver evidence-based negotiation when services are stretched and the family is unreachable. [1] [11]
Exam Pearls
REFUSE
- Medical neglect is the failure to provide, seek or comply with medically necessary treatment; refusal of care is the active rejection of recommended treatment — the response to each is different. [2] [3]
- The Diekema harm-principle threshold is the central organising principle: significant, imminent, preventable harm with an effective, proportionate treatment. [1]
- Most refusals are resolved through respectful, informed negotiation — reaching straight for a court order without attempting it is a failure of practice. [3] [9]
- Courts in all four regions consistently override parental refusal of blood transfusion for children — the child cannot consent to their own death. [6]
- A competent mature minor may have legal authority over their own general medical treatment, but the threshold for overriding refusal of life-saving treatment is lower than for an adult. [10]
- Never close the file on a single conversation — the file is never closed until the child is receiving the treatment they need and the pattern is resolved. [4] [5]
References
- [1]Diekema DS Parental refusals of medical treatment: the harm principle as threshold for state intervention. Theor Med Bioeth, 2004.PMID 15637945
- [2]Jenny C, American Academy of Pediatrics Committee on Child Abuse and Neglect Recognizing and responding to medical neglect. Pediatrics, 2007.PMID 18055690
- [3]Boos SC, Fortin K Medical neglect. Pediatr Ann, 2014.PMID 25369577
- [4]Ward MGK, Baird B Medical neglect: Working with children, youth, and families. Paediatr Child Health, 2022.PMID 36200106
- [5]Dubowitz H Neglect in children. Pediatr Ann, 2013.PMID 23556521
- [6]Conti A, Capasso E, Casella C, et al. Blood transfusion in children: the refusal of Jehovah's Witness parents. Open Med (Wars), 2018.PMID 29666843
- [7]Phadke VK, Bednarczyk RA, Salmon DA, et al. Association between vaccine refusal and vaccine-preventable diseases in the United States: a review of measles and pertussis. JAMA, 2016.PMID 26978210
- [8]Sahni V, Lai FY, MacDonald SE Neonatal vitamin K refusal and nonimmunization. Pediatrics, 2014.PMID 25136042
- [9]Caruso Brown AE, Slutzky AR Refusal of treatment of childhood cancer: a systematic review. Pediatrics, 2017.PMID 29146622
- [10]Coleman DL, Rosoff PM The legal authority of mature minors to consent to general medical treatment. Pediatrics, 2013.PMID 23530175
- [11]Birchley G Harm is all you need? Best interests and disputes about parental decision-making. J Med Ethics, 2016.PMID 26401048
- [12]Salter EK, Hester DM, Vinarcsik L, et al. Pediatric decision making: consensus recommendations. Pediatrics, 2023.PMID 37555276
- [13]Jenny C, Metz JB Medical child abuse and medical neglect. Pediatr Rev, 2020.PMID 32005682