Paeds · child-safety-and-social-paediatrics
Neglect and supervisory neglect
Also known as Child neglect · Supervisory neglect · Physical neglect · Emotional neglect · Medical neglect · Educational neglect
Fellowship guide to child neglect and supervisory neglect across the physical, emotional, medical, educational, supervisory and nutritional domains: neglect as an act of omission rather than commission, the most common yet under-recognised form of maltreatment, the developmental and lifelong consequences of chronic unmet need, the supervision-and-injury evidence of Saluja and Morrongiello, a non-judgemental multi-agency assessment that separates neglect from poverty, a stepped plan pairing family support with mandatory reporting when thresholds are met, and a closed-loop reduce-recurrence disposition across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A three-year-old presents to the emergency department with a scald, and the story does not fit the burn. The first question an examiner wants you to hold is not "was the child hit?" but "was the child watched?" — because the commonest maltreatment a general paediatrician meets is not an act of harm but an absence of care. Neglect is the failure to provide, protect and supervise, and it is both the most prevalent and the most under-recognised form of child maltreatment. [1] [2]
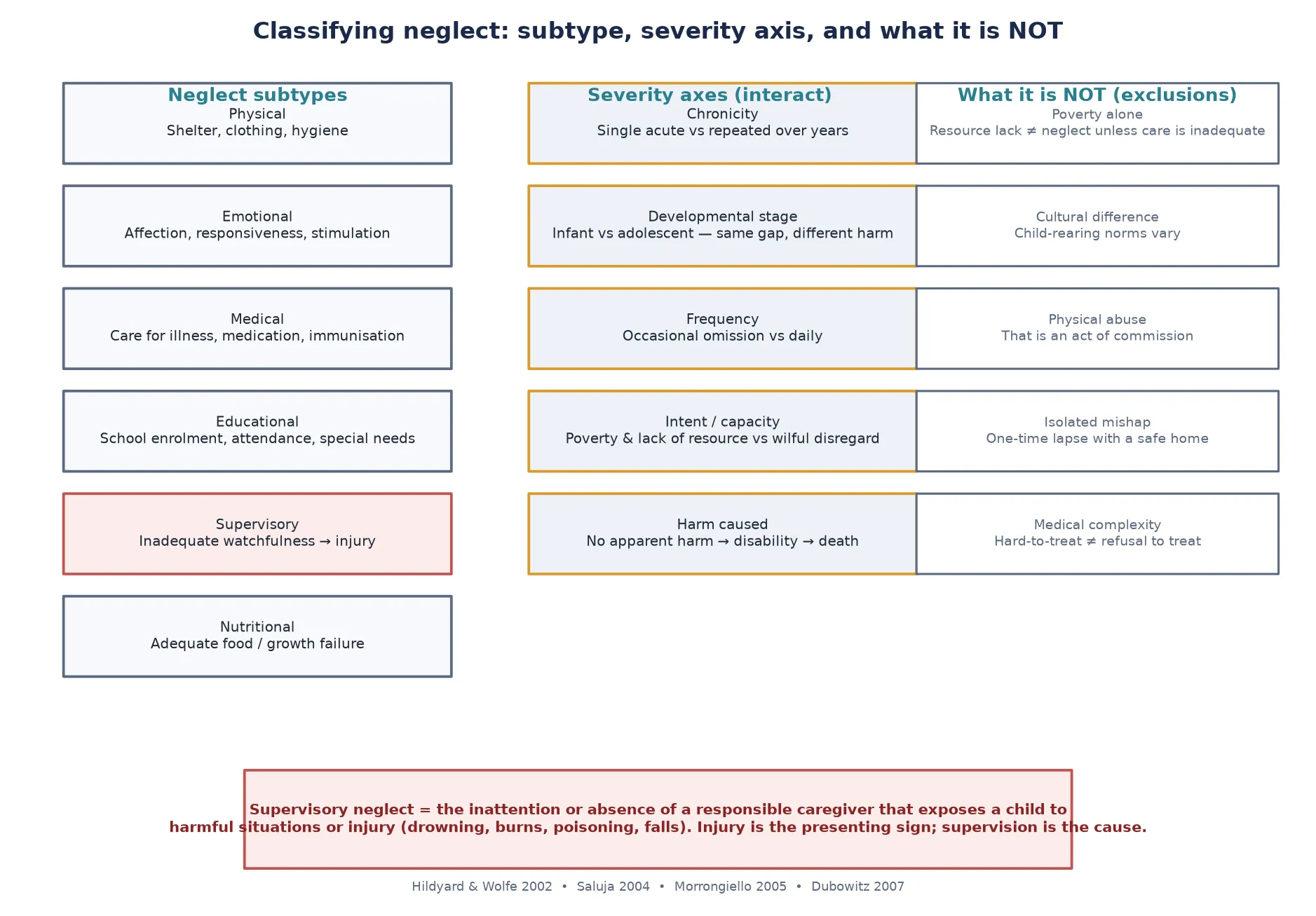
The working definition is operational rather than legal: a child is neglected when a caregiver, who has the means and responsibility to do so, persistently fails to meet basic needs to a degree that harms or risks harming the child's health, development or dignity. The harm may be physical, emotional, developmental, educational, or — in supervisory neglect — an injury or death that adequate supervision would have prevented. What makes it neglect rather than misfortune is the chronicity and the adequacy of the caregiving response, not the family's income. [1] [6]
Supervisory neglect deserves its own name because it presents through injury rather than deprivation. Saluja and colleagues defined the role of supervision in child injury risk around three components — attention, proximity and continuity — and showed that measurement is genuinely hard, because supervision is dynamic and context-dependent. When a toddler drowns, is poisoned, or sustains a bath scald, the mechanism is usually a lapse in one of those three, and the paediatrician's task is to decide whether the lapse reflects an isolated mishap in a safe home or a pattern of inadequate watchfulness. [7] [8]
Deep technique for non-accidental physical injury lives on the physical-abuse leaf, faltering growth on its own leaf, and out-of-home-care assessment on a separate leaf. This page owns neglect across its six domains — physical, emotional, medical, educational, supervisory and nutritional — with supervisory neglect as the distinctive, injury-presenting focus. [1] [2]
Classification
Sort every neglected child along three axes before you name the plan: which need is unmet, how severe and chronic the failure is, and what it is not. The same dirty, underweight child means something different in a family with no resources who is doing everything possible than in a family with means who is not engaging. [1] [6]
By domain of unmet need
| Domain | What the caregiver fails to do | Presenting clue |
|---|---|---|
| Physical | Provide adequate shelter, clothing, hygiene | Inadequate clothing for weather, infestations, untreated skin disease |
| Emotional | Provide affection, responsiveness, stimulation | Withdrawn, vacant, indiscriminate, or dysregulated child |
| Medical | Seek and adhere to care for treatable illness | Late-presenting severe asthma, untreated dental caries, missed immunisations |
| Educational | Enrol and ensure school attendance, meet special needs | Chronic non-attendance, unmet learning difficulty |
| Supervisory | Provide adequate watchfulness against harm | Drowning, scald, poisoning, fall, unsafe exposure |
| Nutritional | Provide adequate food | Faltering growth, micronutrient deficiency |
Neglect versus abuse — the commission / omission divide
- Failure to provide, protect, watch, respond
- Most common form of maltreatment
- Presents through deprivation or an inadequately-supervised injury
- Severity tracks chronicity and developmental stage
- An act that harms — physical, sexual, emotional
- Often an identifiable event or pattern of events
- Presents through injury or disclosure
- Cross-link the physical-abuse leaf for mechanism
By severity and the exclusions
Severity is not a single number. It is the product of chronicity, the child's developmental stage, the frequency of omission, the caregiver's intent and capacity, and the harm already caused. A single inadequate night is not neglect in a home that is otherwise safe and responsive; the same omission repeated daily across infancy is severe neglect. The exclusions examiners probe are poverty alone, cultural difference in child-rearing, an isolated mishap, and genuine medical complexity — each of which changes the response from child protection to family support. [1] [6]
[1] [6] [7]Epidemiology & Risk Factors
Neglect is the most common substantiated form of child maltreatment across high-income countries, yet it is also the most under-reported, because there is no single dramatic event to disclose. Gilbert and colleagues, in the Lancet series on child maltreatment, established that the burden of neglect is substantial and its consequences rival those of abuse. Stoltenborgh's meta-analysis — pointedly titled "The neglect of child neglect" — confirmed that self-report studies yield far higher prevalence than official-substantiation figures, revealing how much is missed. [5] [11]
What places a child at risk? Neglect clusters where caregiver capacity is overwhelmed: parental mental illness, substance use, intellectual disability, intimate-partner violence, social isolation, and severe socioeconomic hardship. Kobulsky framed neglect as a global challenge in which structural deprivation, family capacity and child vulnerability interact, not a private failing of one parent. The younger the child and the longer the exposure, the greater the harm — which is why infants and toddlers carry the heaviest burden and the worst outcomes. [2] [3]
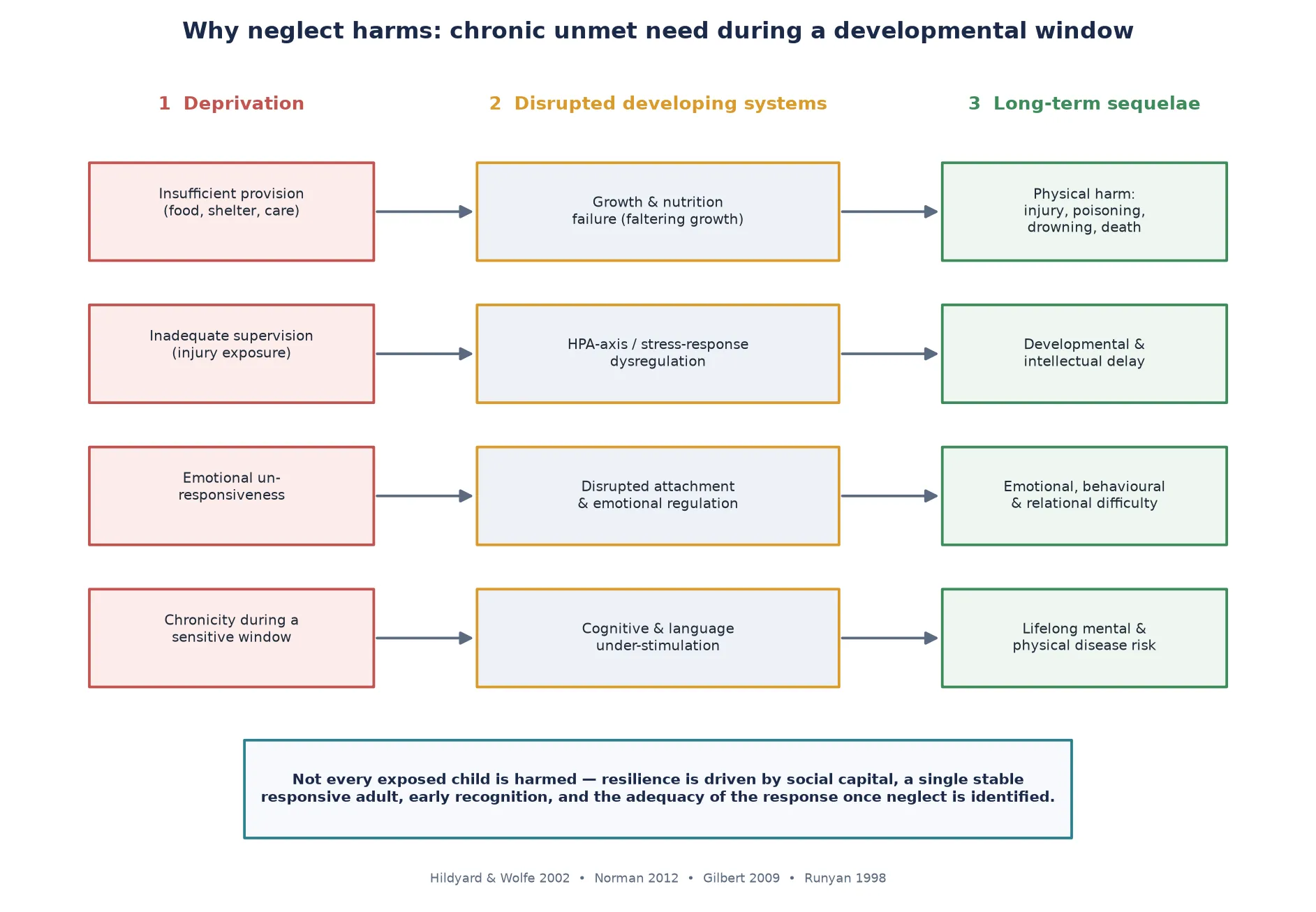
Protective forces point the other way. Runyan's work showed that children can prosper in unfavourable environments when social capital — community ties, a stable and responsive adult, and accessible services — buffers the adversity. A single committed grandparent, a functioning school, and a responsive medical home each reduce the chance that deprivation crosses into harm. This is the evidence base for treating neglect with support as much as with protection. [13]
Pathophysiology
Neglect harms through chronic unmet need during a developmental window, not through a single injurious event. Picture the institutionally-deprived or chaotically-parented infant whose distress rarely meets a responsive face, whose hunger is unpredictably answered, and whose explorations go unsupervised. Each unmet need is small; their accumulation is the pathogen. [6] [12]
The mechanisms track the domain. Nutritional and physical neglect produce faltering growth and micronutrient deficiency through straightforward energy and nutrient deficit. Emotional neglect and unresponsiveness disrupt attachment formation and emotional regulation, leaving a child watchful, withdrawn, or indiscriminately sociable. Under-stimulation during the sensitive windows for language and cognition yields measurable developmental and intellectual delay. Supervisory neglect operates differently — it exposes the child to hazards, and the injury or death is the direct mechanism of harm. [6] [7]
The neuroscience of early deprivation is consistent across these pathways. Chronic unmet need activates the stress response repeatedly during a window when the HPA axis, attachment and regulatory systems are being calibrated, and the developing brain adapts to an unreliable world. Norman's systematic review and meta-analysis linked child neglect to long-term mental and physical disease, placing neglect alongside abuse as a driver of lifelong morbidity. The hopeful corollary is that the same plasticity that makes early neglect damaging makes a corrective, responsive environment therapeutic. [6] [12]
Clinical Presentation
Parents rarely lead with "I am neglecting my child." They bring a child with an injury, a faltering weight, chronic school absence, untreated dental caries, or a behavioural concern — and the pattern across domains is what you must assemble. Neglect is almost always multi-domain by the time it reaches a clinician. [1] [6]
Physical neglect shows as inadequate clothing for the weather, poor hygiene, untreated infestations, and recurring minor illness. Emotional neglect shows as a child who is withdrawn or vacant, who does not seek comfort, or who is indiscriminately sociable with strangers. Medical neglect shows as late presentation of treatable disease, missed immunisations, and untreated dental caries. Educational neglect shows as chronic non-attendance and unmet learning need. Nutritional neglect shows as faltering growth and micronutrient deficiency. Supervisory neglect shows as the injury — a drowning near-miss, a bath scald, a poisoning, a fall from an unguarded height. [1] [7]
The developmental and contextual variants matter. Infants and toddlers present through growth and developmental failure because they cannot self-protect; school-age children present through non-attendance, hunger, or behavioural change; adolescents may present through risk-taking layered on years of unmet need. Always gather the school's, the general practitioner's, and any social-worker's view, because multi-agency information is how you separate a cross-setting pattern from a single difficult period in an otherwise adequate home. [2] [6]
Differential Diagnosis
Build the differential in layers: the things neglect is not, the things that mimic its signs, and the coexisting maltreatment that travels with it. The single most examined distinction is neglect versus poverty, and getting it wrong in either direction harms the child. [1] [6]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Poverty alone | Resource lack despite adequate caregiving effort | The child is clean, clothed within means, and engaged; respond with material support, not child protection |
| Cultural difference | Child-rearing norms that vary by culture | The child is thriving within the family's cultural frame; assess function, not conformity |
| Medical complexity | Hard-to-treat illness in an engaged family | The family is seeking and adhering to care; the difficulty is the disease |
| Faltering growth from organic disease | Underlying GI, endocrine, cardiac, genetic cause | The family is responsive and the child improves with disease-specific treatment |
| Isolated mishap | Single lapse in an otherwise safe, supervised home | No prior injuries, safe environment, engaged caregiver |
| Coexisting physical or sexual abuse | Injury pattern or disclosure suggesting commission | Assess for abuse on its own leaf and run both pathways |
The two mirror-image errors examiners love are over-calling neglect in a family whose only problem is poverty — which stigmatises and fails to offer help — and under-calling neglect by attributing a chronic, multi-domain pattern to "cultural difference" or "a difficult patch." When the function and the caregiving response tell different stories, return to the chronicity and the adequacy of care, and gather multi-agency information before settling. [1] [6]
Clinical & Bedside Assessment
Lead with a non-judgemental, multi-agency history. A parent who feels accused will disengage, and you lose the child. Neglect is almost never the story a single visit tells; it is the story that emerges when clinic, school, general practice, and child-protection records are brought together. [1] [2]
Neglect-informed assessment sequence
Engage and establish rapport
Curious, non-blaming stance; explore the family's strengths and stressors; reassure that the goal is help, not punishment.
Map the domains of unmet need
Physical, emotional, medical, educational, supervisory, nutritional — ask concretely about housing, food, supervision, school, healthcare, affection.
Assess severity and chronicity
How long, how often, across how many settings; the child's developmental stage; the harm already caused and the risk of further harm.
Examine the child
Growth, hygiene, dental, skin, untreated illness, signs of abuse; developmental assessment; the injury in supervisory presentations.
Gather multi-agency information
With consent where possible — school, GP, immunisations, child-protection history; this is how you separate pattern from episode.
Assess caregiver capacity
Mental illness, substance use, intellectual disability, intimate-partner violence, social isolation, overwhelm — capacity frames the response.
Formulate and decide the threshold
Support versus mandatory report; named lead; safety-net and follow-up; never close the file on a single visit.
Examine the child head to toe. Plot growth and look for faltering; note dental caries, poor hygiene, untreated skin disease, and signs of coexisting abuse. In a supervisory presentation, characterise the injury and judge whether the mechanism and the supervision story fit the child's developmental stage. Assess development directly, because neglect and developmental delay coexist and each changes the plan. [6] [7]
Assess caregiver capacity kindly but directly. An overwhelmed parent with untreated depression, substance use, or intimate-partner violence cannot meet the child's needs alone, and your plan must match real life. Distinguish capacity-limitation from wilful disregard, because the first calls for family support and the second for child protection — though both may coexist, and both may require reporting when the threshold is met. [2] [13]
Investigations
Neglect is a clinical and contextual diagnosis, not a laboratory one. There is no blood test, scan, or biomarker that confirms neglect, and the commonest investigation error is the shotgun panel ordered for a "failing" child when the real need is a careful history and a growth chart. [1] [6]
Investigate when the story points somewhere. Plot and investigate faltering growth to exclude organic disease. Arrange dental review for untreated caries. When a supervisory injury is the presentation, image and work up the injury on the physical-abuse pathway if the mechanism or pattern raises concern for non-accidental injury. Screen for the consequences of chronic neglect — iron deficiency, recurrent infection, developmental delay — and treat each on its own merits. [6] [7]
Multi-agency information-gathering is the most important "investigation" you do. With appropriate consent — or under child-protection authority when consent is refused and the threshold is met — obtain school-attendance and educational records, the general-practice record, immunisation history, and any prior child-protection involvement. Discordant accounts between home and school are themselves data, and a pattern across settings is what confirms chronic neglect over a single episode. [2] [13]
Management — Resuscitation
"Resuscitation" in neglect means immediate safety, medical stabilisation, and the end of any present danger — not a drug, and not a single therapy session. [1] [7]
Make a same-day safety plan: who supervises the child now, where they stay, who to call, and where to go. Treat injury and illness first; secure food, shelter and supervision; and address any immediate threat. Recognise that no medication resuscitates neglect — safety, stability and the meeting of basic needs are the resuscitation. [1] [2]
Management — Definitive & Stepwise
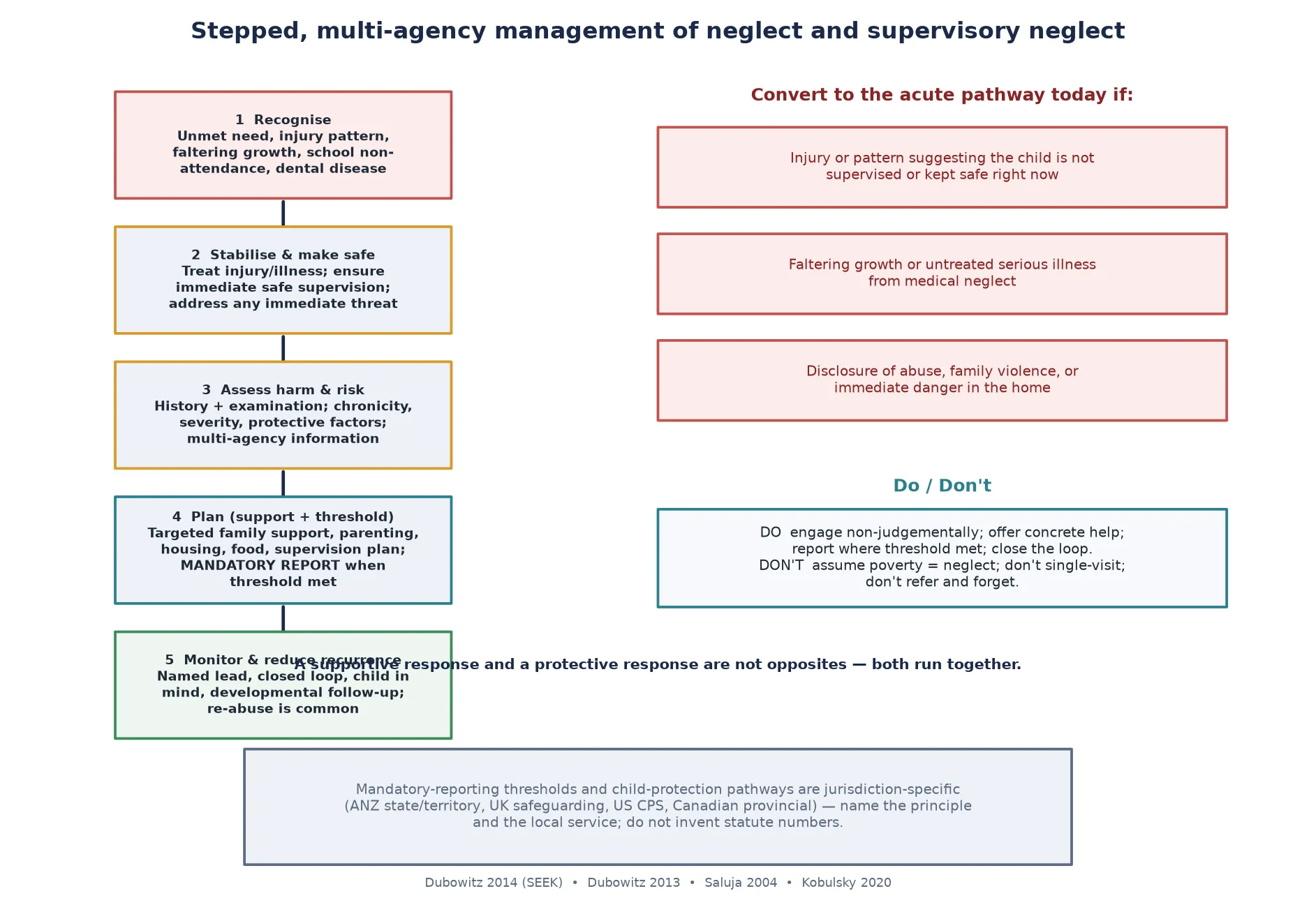
Stepped, multi-agency care is the frame, and the order matters: recognise, stabilise and make safe, assess harm and risk, plan with support and threshold, then monitor and reduce recurrence. A supportive response and a protective response run together at every step. [1] [4]
Step 1 — Recognise and stabilise
Identify the neglect across domains, treat any injury or illness, and ensure immediate safe supervision. End any present danger before any longer-term work begins, because no family-support programme can take hold while a child is acutely unsafe. [1] [7]
Step 2 — Assess harm and risk
Take the multi-agency history, examine the child, and judge both the harm already caused and the risk of further harm. Chronicity, severity, the child's developmental stage, caregiver capacity, and protective factors each shape the plan. A formulation that names the domains, the chronicity, and the threshold decision is what guides the next step. [2] [6]
Step 3 — Plan: support plus threshold
Deliver a plan that pairs concrete family support with child-protection reporting when the threshold is met. Support means targeted help matched to the domain: parenting programmes, material assistance for food and housing, mental-health and substance-use treatment for the caregiver, a supervision and home-safety plan, school engagement, and a medical home for the child's health needs. The Safe Environment for Every Kid (SEEK) model, developed by Dubowitz, is the named evidence-based primary-care approach that addresses psychosocial risk factors to prevent neglect. When the threshold for mandatory reporting is met — serious harm, ongoing danger, or failure of a supportive response — report to child protection; do not substitute support for protection where protection is required. [1] [4]
Step 4 — Monitor and reduce recurrence
Name the clinician who owns the plan, set the follow-up date, and document return precautions: new injury, escalating need, placement breakdown, or disclosure of abuse. Neglect is chronic and recurrent, and re-abuse is common, so a single intervention that closes the file fails the child. Monitor growth, development, school engagement, and the caregiving response, adjust the support, and re-evaluate the threshold if risk resurfaces. Close the loop with child protection, the school, and the general practitioner. [2] [13]
Specific Subtypes & Scenarios
Supervisory neglect (the injury-presenting subtype). Characterise the injury and judge whether the supervision story fits the child's developmental stage; Saluja's attention–proximity–continuity framework and Morrongiello's supervision research frame the assessment. A second injury, an unsafe home, or an overwhelmed caregiver converts the plan to child protection. [7] [8]
Medical neglect. Late presentation of treatable illness, missed immunisations, or untreated dental caries; distinguish a family that is struggling to access care from one that is refusing care, and address the access barrier while ensuring the child receives treatment. [1] [2]
Educational neglect. Chronic non-attendance and unmet learning need; engage the school and educational welfare, and screen for the unmet special need that the non-attendance masks. [1] [6]
Emotional neglect. Withdrawn, vacant, indiscriminate, or dysregulated child; pair the neglect response with relationship-based intervention, and cross-link the attachment-disorders leaf for the disordered-social-relatedness picture. [6]
Nutritional neglect. Faltering growth and micronutrient deficiency; investigate organic causes, then frame the nutritional rehabilitation and the caregiving response together on the faltering-growth leaf. [6]
Child of a parent with mental illness or substance use. Caregiver-capacity support is part of the child's plan; an untreated parent cannot meet the child's needs alone, and family-support services must run alongside child monitoring. [2] [13]
Child already in out-of-home care. Assess for accumulated neglect-related morbidity — developmental delay, untreated illness, growth failure — and deliver a health assessment that catches up what was missed; cross-link the out-of-home-care leaf. [6]
Adolescent with long-standing neglect. Layer risk-taking, mental-health, and substance-use assessment onto the neglect plan; deliver integrated care that addresses both the historical deprivation and the current risk. [6] [12]
Refugee, asylum-seeking and culturally diverse child. Use culturally safe assessment, professional interpreters, and material support; distinguish genuine neglect from the deprivation of displacement, which calls for settlement help rather than child protection. [3] [13]
Complications & Pitfalls
- Assuming poverty equals neglect, and stigmatising a family whose only problem is material hardship. [1]
- Attributing a chronic multi-domain pattern to "cultural difference" or "a difficult patch," and under-calling neglect. [1] [6]
- Missing the supervisory-neglect mechanism behind a "routine" injury such as a bath scald or near-drowning. [7] [8]
- Closing the file on a single home visit without support, follow-up, or a named lead. [2]
- Referring to child protection or family services and forgetting — re-abuse is common. [5] [13]
- Substituting support for protection where the threshold for mandatory reporting is clearly met. [1]
- Running only the physical-abuse workup and missing the chronic deprivation across the other domains. [6]
- Ignoring caregiver capacity — mental illness, substance use, intellectual disability, family violence — and expecting a plan to work without treating the parent. [2] [13]
- Failing to gather multi-agency information, so a cross-setting pattern is read as a single episode. [1] [2]
Prognosis & Disposition
Neglect is chronic and its consequences are developmental and lifelong. Norman's systematic review and meta-analysis linked neglect to long-term mental and physical disease, and Hildyard and Wolfe established the developmental issues and outcomes that track chronic unmet need. The younger the child and the longer the exposure, the worse the prognosis — which is exactly why early recognition and a sustained response matter. [6] [12]
Recovery is possible when care becomes adequate, stable and responsive. The same developmental plasticity that makes early neglect damaging makes a corrective environment therapeutic, and Runyan showed that social capital lets children prosper even in unfavourable environments. The mechanisms of recovery are a stable and responsive adult, the meeting of basic needs, and a sustained multi-agency response — not a single intervention. [12] [13]
Disposition after safety confirmed: a stepped, multi-agency plan of targeted family support with a named clinical lead, scheduled follow-up, developmental monitoring, and a clear threshold for re-reporting. [1] [4] Disposition when risk or a safeguarding concern surfaces: the acute child-protection pathway, crisis supports, and stability before any routine family-support work. [1] [7] Disposition for an adolescent with long-standing neglect plus risk-taking: integrated mental-health and substance-use care layered onto the neglect plan. [6] [12]
Markers of response are improving growth, hygiene and school engagement, fewer injuries, better developmental trajectory, and a caregiving response that is adequate without external compulsion. The medical home carries the long view — interim support, safety planning, and school liaison — because neglect is measured in years, not visits. [4] [13]
Special Populations
Infants and toddlers carry the heaviest burden and the worst outcomes, because they cannot self-protect and their developmental windows are most sensitive; assess growth, development and supervision closely in this group. Children with disability and neurodiversity may disclose less, depend more on the caregiver, and present with overlapping behavioural signs — adapt the assessment and avoid attributing all difficulty to the disability. [6] [13]
Children in out-of-home care carry accumulated neglect-related morbidity and need a comprehensive health assessment that catches up what was missed; cross-link the out-of-home-care leaf. Refugee, asylum-seeking and culturally and linguistically diverse families need culturally safe assessment, professional interpreters, and material support that distinguishes the deprivation of displacement from genuine neglect. Indigenous families need non-stigmatising services that acknowledge intergenerational trauma, racism, and the structural drivers of disadvantage, and that work with community-controlled organisations. [3] [13]
Rural and remote families should be offered telehealth-delivered support and supervision planning rather than told to wait. Families living in socioeconomic hardship need a response that addresses the material determinants first, because a plan that ignores food, housing and income cannot succeed. Children of parents with mental illness, substance use or intellectual disability need caregiver-capacity treatment built into the child's plan from the outset. [2] [4]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [6]
- Dubowitz 2013 Pediatr Ann — the operational definition and clinical approach to neglect in children; the foundational overview. [1]
- Dubowitz & Bennett 2007 Lancet — physical abuse and neglect of children; the burden and the clinical response. [2]
- Hildyard & Wolfe 2002 Child Abuse Negl — the developmental issues and outcomes of child neglect; the developmental-mechanism anchor. [6]
- Saluja et al. 2004 Inj Control Saf Promot — the role of supervision in child injury risk; the conceptual framework for supervisory neglect around attention, proximity and continuity. [7]
- Morrongiello 2005 J Pediatr Psychol — caregiver supervision and child-injury risk: defining and measuring supervision; the supervision-research foundation. [8]
- Morrongiello & House 2004 Inj Prev — measuring parent attributes and supervision behaviours relevant to child injury risk. [9]
- Gilbert et al. 2009 Lancet — burden and consequences of child maltreatment in high-income countries; neglect rivals abuse in harm. [5]
- Stoltenborgh et al. 2013 Soc Psychiatry — "The neglect of child neglect": self-report prevalence far exceeds official figures. [11]
- Norman et al. 2012 PLoS Med — long-term health consequences of neglect, a systematic review and meta-analysis. [12]
- Afifi et al. 2012 Pediatrics — harsh physical punishment and mental disorders; the overlap with harsh and neglectful parenting. [10]
- Kobulsky et al. 2020 Child Abuse Negl — neglect as a global challenge; structural and family drivers. [3]
- Dubowitz 2014 Pediatr Ann — the SEEK model: a primary-care approach to preventing neglect by addressing psychosocial risk. [4]
- Runyan et al. 1998 Pediatrics — children who prosper in unfavourable environments through social capital; the resilience evidence. [13]
Child neglect and supervisory neglect are managed through state and territory child-protection systems with jurisdiction-specific mandatory-reporting legislation. Paediatricians are mandatory reporters in every Australian state and territory (New Zealand has no mandatory reporting duty for health professionals — reporting is voluntary with good-faith protection); the threshold is a reasonable belief that a child has suffered or is at risk of significant harm. Aboriginal Community Controlled Health Services and culturally safe pathways are central for Aboriginal and Torres Strait Islander and Māori children, acknowledging intergenerational trauma and the over-representation of Indigenous children in care. Family-support services, parenting programmes, and the SEEK-style primary-care approach underpin prevention. [1] [4]
Controversies: where the line between poverty and neglect truly lies; the reliability of supervision measurement; the balance between support and protection in marginal cases; how to reduce recurrence in a chronic condition; and how to deliver evidence-based family support when services are stretched and access is thin in rural and remote regions. [3] [7]
Exam Pearls
NEGLECT
- Neglect is the most common and most under-recognised form of maltreatment — self-report far exceeds official figures. [5] [11]
- Supervisory neglect presents through injury — a scald, near-drowning, poisoning or fall — frame supervision around attention, proximity and continuity. [7] [8]
- Separate neglect from poverty using the adequacy of the caregiving response and chronicity, not income alone. [1] [6]
- The SEEK model is the named primary-care approach to preventing neglect by addressing psychosocial risk. [4]
- Recovery tracks the adequacy and stability of the corrective environment — social capital buffers adversity. [12] [13]
- Never refer and forget — re-abuse is common, so a named lead, scheduled follow-up, and a clear re-report threshold close the loop. [1] [2]
References
- [1]Dubowitz H Neglect in children. Pediatr Ann, 2013.PMID 23556521
- [2]Dubowitz H, Bennett S Physical abuse and neglect of children. Lancet, 2007.PMID 17544770
- [3]Kobulsky JM, Dubowitz H, Xu Y The global challenge of the neglect of children. Child Abuse Negl, 2020.PMID 31831190
- [4]Dubowitz H The Safe Environment for Every Kid model: promotion of children's health, development, and safety, and prevention of child neglect. Pediatr Ann, 2014.PMID 25369580
- [5]Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, Janson S Burden and consequences of child maltreatment in high-income countries. Lancet, 2009.PMID 19056114
- [6]Hildyard KL, Wolfe DA Child neglect: developmental issues and outcomes. Child Abuse Negl, 2002.PMID 12201162
- [7]Saluja G, Brenner R, Morrongiello BA, Haynie D, Rivera M, Cheng TL The role of supervision in child injury risk: definition, conceptual and measurement issues. Inj Control Saf Promot, 2004.PMID 14977501
- [8]Morrongiello BA Caregiver supervision and child-injury risk: I. Issues in defining and measuring supervision; II. Findings and directions for future research. J Pediatr Psychol, 2005.PMID 16166243
- [9]Morrongiello BA, House K Measuring parent attributes and supervision behaviors relevant to child injury risk: examining the usefulness of questionnaire measures. Inj Prev, 2004.PMID 15066978
- [10]Afifi TO, Mota NP, Dasiewicz P, MacMillan HL, Sareen J Physical punishment and mental disorders: results from a nationally representative US sample. Pediatrics, 2012.PMID 22753561
- [11]Stoltenborgh M, Bakermans-Kranenburg MJ, van Ijzendoorn MH The neglect of child neglect: a meta-analytic review of the prevalence of neglect. Soc Psychiatry Psychiatr Epidemiol, 2013.PMID 22797133
- [12]Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med, 2012.PMID 23209385
- [13]Runyan DK, Hunter WM, Socolar RR, Amaya-Jackson L, English D, Landsverk J Children who prosper in unfavorable environments: the relationship to social capital. Pediatrics, 1998.PMID 9417144