Paeds · child-safety-and-social-paediatrics
Physical abuse: bruising and sentinel injuries
Also known as Non-accidental bruising · Inflicted soft-tissue injury · TEN-4 FACES-L bruising rule · Sentinel injury recognition · Bruising in suspected child abuse
A fellowship-level, exam-exhaustive approach to inflicted bruising and sentinel injuries: the TEN-4 FACES-L decision rule, the significance of any bruise in a non-mobile infant, patterned and high-specificity injury, the differential (including bleeding disorders), skeletal survey and coagulopathy work-up, mandatory reporting and the safeguarding pathway across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Physical abuse is inflicted injury, and for the bedside clinician the first and most common evidence is the skin. Bruising is the most frequent manifestation of physical abuse and the most easily missed. The job of the clinician is not to convict a caregiver but to recognise when a pattern of bruising is improbable as an accident and must trigger a structured safeguarding response. [1] [4]
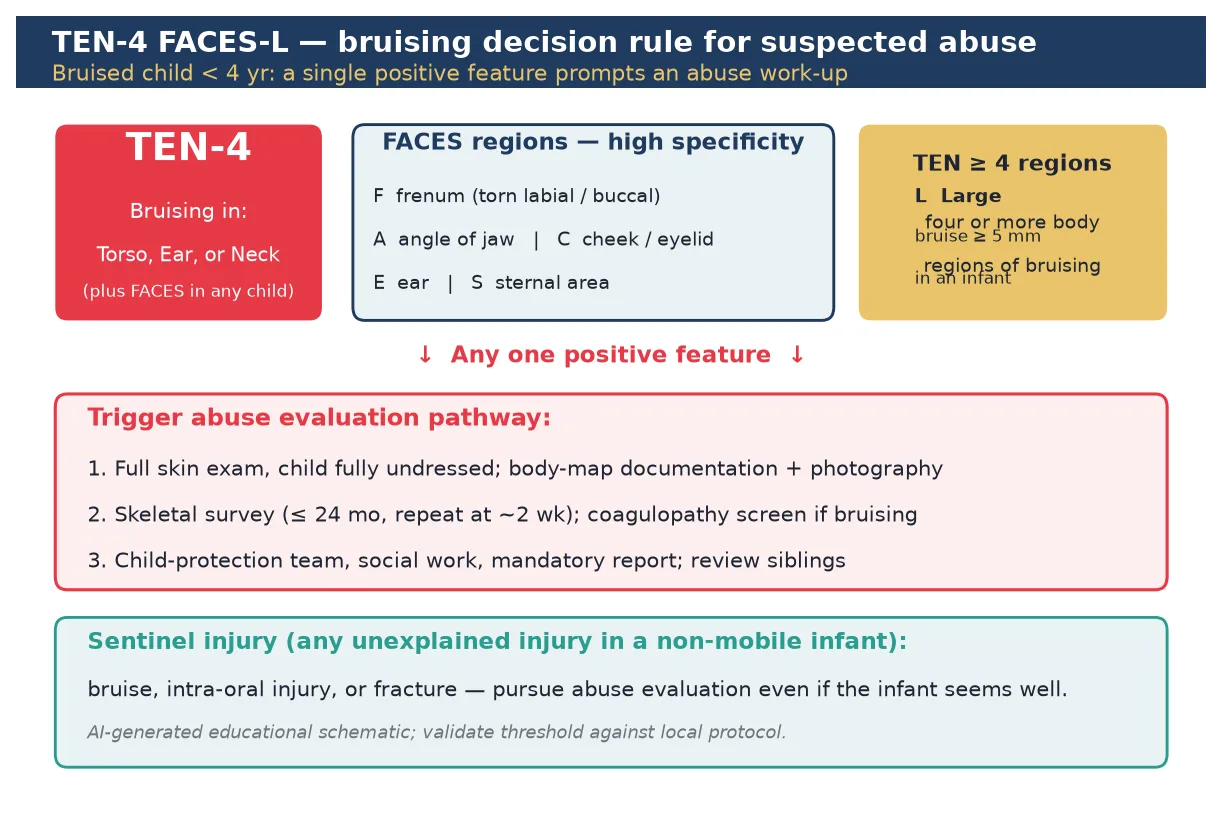
Two linked concepts anchor this page. The first is the discriminating bruise — a bruise whose location, number, shape or size raises the probability of inflicted injury high enough to mandate an evaluation. The TEN-4 FACES-L clinical decision rule operationalises that judgement. The second is the sentinel injury, defined as a minor injury seen in a pre-mobile infant that is poorly explained and that, on later review, is understood to have been inflicted. [2] [5]
The reason sentinel injuries matter is prevention. Infants who later present with abusive head trauma or major inflicted injury have often had a prior, smaller injury that a clinician saw and explained away. Recognising the sentinel injury and acting on it is one of the few points in child protection where a clinician can intervene before catastrophe. [2] [7]
This page owns recognition and the immediate safeguarding response for bruising and sentinel soft-tissue injury. It cross-links to dedicated pages on abusive head trauma, inflicted fractures, inflicted burns, intra-oral injury, and mandatory reporting. It does not duplicate those workups. [4]
Classification
Classify the child first by developmental mobility, because mobility is the single most important filter for whether a bruise can be accidental. A non-mobile infant is one who is not yet independently cruising — not rolling to a bruise, not crawling into furniture. A cruising or walking toddler collects bruises on bony prominences. A school-age child collects them on shins and knees. The same bruise that is trivial in a four-year-old is alarming in a four-month-old. [3] [4]
Classify the bruise next by whether it trips a rule component. TEN-4 FACES-L sorts bruising into positive features: torso, ear or neck location; any FACES site; four or more bruised body regions; and large size. Any single component in a child under four is a trigger. Patterned bruising — a hand-slap, ligature line, bite, or implement imprint — sits outside the rule because it is independently diagnostic of inflicted injury. [1] [5]
Classify the sentinel injury separately because it is a category defined by context, not by appearance. A sentinel injury is any apparently minor, inflicted injury in an infant who is not yet mobile — most often a bruise, an intra-oral injury, or a fracture discovered incidentally. Its importance lies in what it predicts, not in how severe it looks at the time. [2] [6]
Epidemiology & Risk Factors
Bruising is common in mobile children and rare in non-mobile infants. The landmark work on accidental bruising showed that bruising is uncommon in infants who are not yet cruising, and that the number of bruises rises with developmental stage and activity. That gradient is the empirical basis for treating any bruise in a non-mobile infant as abnormal. [3]
Sentinel injuries are the missed opportunities of child protection. In the cohort that defined the term, sentinel injuries were found in roughly a quarter of infants evaluated for abuse, yet many had been seen by a clinician before the abusive presentation without the injury being recognised or acted on. Bruises and intra-oral injuries were the most common sentinel types. [2]
Risk factors cluster at three levels. At the child level: young age (infancy), prematurity, disability, and being one of a multiple. At the caregiver level: young parental age, single caregiver, mental health or substance-use problems, intimate-partner violence, and a personal history of abuse. At the contextual level: socioeconomic stress, housing instability, social isolation, and prior child-protection contact. None of these factors is diagnostic on its own, but together they raise the prior probability of inflicted injury and should sharpen your threshold to evaluate. [4] [7]
Recurrence is the reason to act early. A child who has been injured once is at elevated risk of further and more severe injury. Studies of children who later present with abusive head trauma show that many had a prior sentinel injury documented in the medical record. The sentinel injury is therefore both a diagnostic clue and a prevention opportunity. [7] [2]
Pathophysiology
A bruise is extravasated blood in soft tissue after blunt force. The colour change that follows depends on depth, location, and the individual, which is why dating bruises by colour alone is unreliable and should not be done. Inflicted bruises differ from accidental ones chiefly in where and how the force was applied, not in their colour science. [4]
The discriminating regions exist because of anatomy and behaviour. The torso, ears, neck, cheeks, and angle of the jaw are soft areas that a mobile child rarely strikes in normal play, whereas the forehead, shins, knees, and elbows are bony prominences over which a mobile child habitually falls. A bruise on a soft, protected site implies a force that did not come from the child's own locomotion. [1] [5]
Patterned bruising preserves the shape of the inflicting object because capillaries rupture at the edges of impact while central vessels are compressed and spared — the classic negative imprint. A slap leaves finger marks; a grip leaves oval fingertip bruises; a ligature leaves a circumferential line; a bite leaves an arc of paired punctures. These marks are inflicted by definition because no accidental mechanism reproduces them. [4] [8]
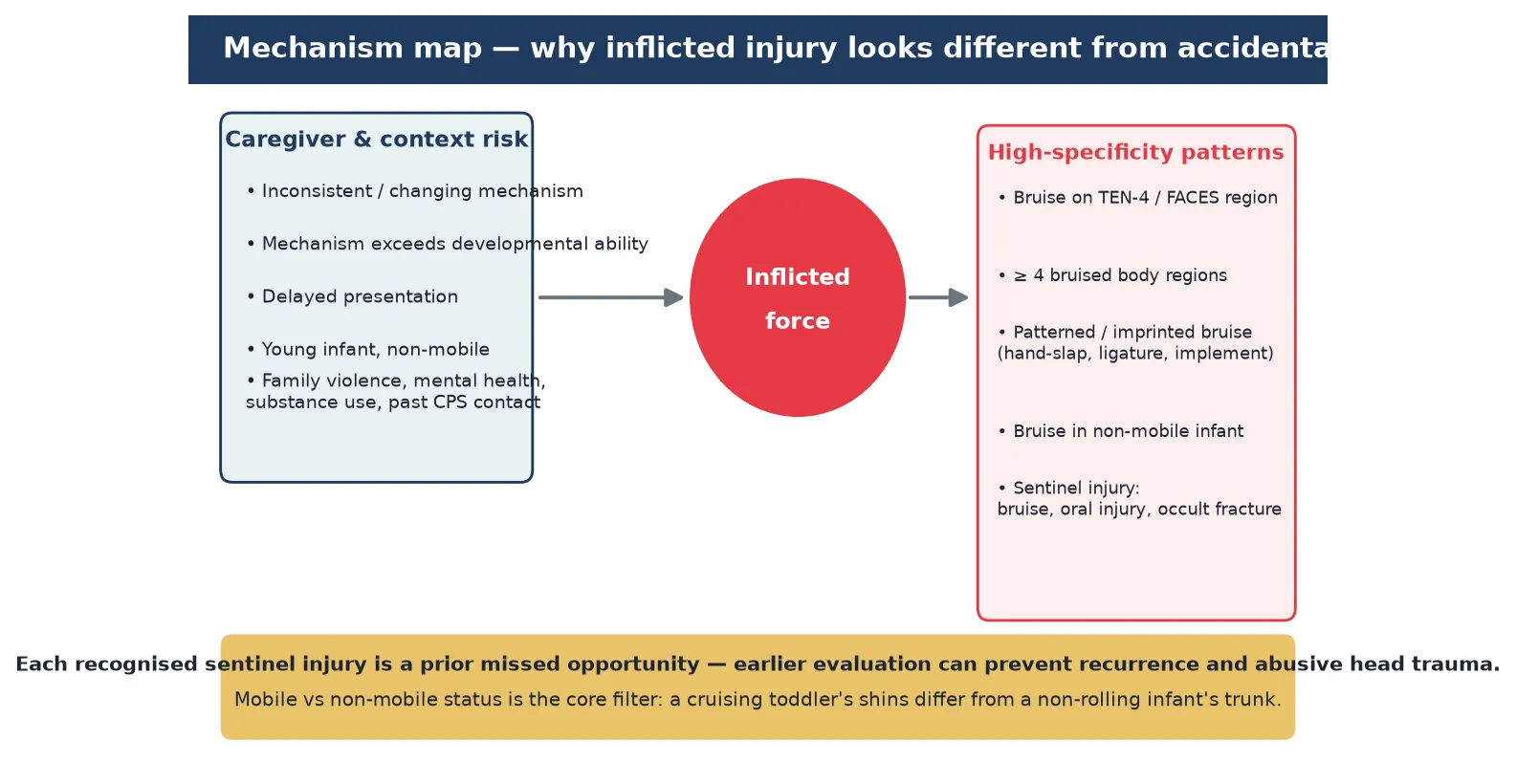
The sentinel injury pathway is the same mechanism seen earlier and smaller. An inflicted bruise or intra-oral injury in a non-mobile infant is the same act of force that, repeated or escalated, will later produce a fracture or a head injury. The biology does not change between the sentinel event and the catastrophic one — only the clinician's opportunity to intervene changes. [2] [7]
Clinical Presentation
A sentinel injury often presents incidentally. A parent brings an infant for a minor complaint — a feeding worry, a fever, a rash — and during the examination you notice a small bruise on the ear, a torn frenum, or a mark on the trunk. The injury is not the reason for the visit, and it is easy to attribute it to a sibling, a bouncy chair, or a wriggle. That ease of explanation is exactly the trap. [2] [6]
Bruising that should prompt an abuse evaluation includes bruises in any TEN-4 region, any FACES site, four or more bruised body regions, a large bruise, and any patterned mark. Palm bruising in infants is a specific, recognisable pattern that should prompt concern because no normal mechanism produces it. Bruises of apparently identical age across several sites also raise concern, as does bruising to the ears, neck, or cheeks. [1] [5] [8]
Intra-oral injuries deserve special attention because they are easily hidden. A torn upper labial frenum, a lacerated frenulum, or bruising of the lips or palate in a non-mobile infant is highly concerning. The systematic review of intra-oral injuries found that a torn frenum in a non-ambulatory infant is strongly associated with abuse and warrants evaluation. [9]
Visceral injury is rare but lethal when missed. Inflicted abdominal injury may present with subtle bruising of the abdominal wall, vomiting, or signs of shock, and can occur without external marks. The message for this page is that a child with bruising should be examined for the possibility of occult visceral as well as occult bony injury, and that abdominal bruising is never trivial. [10]
Differential Diagnosis
The most common alternative diagnosis to consider is a genuine bleeding disorder, because it can produce bruising that mimics abuse. Haemophilia, von Willebrand disease, immune thrombocytopenia, and rare inherited disorders such as Ehlers-Danlos syndrome all belong in the differential. The evaluation is not a choice between abuse and bleeding disorder — both can coexist, and a bleeding disorder does not protect a child from abuse. [4] [11]
Cultural practices can produce patterned marks that are not abuse. Coin rubbing (gua sha), cupping, and moxibustion leave linear, circular, or burnt marks that can alarm an unfamiliar clinician. Ask about the practice respectfully and document it; the marks of these practices are typically symmetric, on expected sites, and explained openly by the family. [4]
Accidental bruising remains the most common explanation for bruises in mobile children, and most bruises in mobile children are accidental. Mongolian blue spots (dermal melanocytosis) are birthmarks, not bruises, and are found on the sacrum, buttocks, and back in infants; they do not change colour over days and require no evaluation. The role of the rule is to identify the minority of bruises that are not accidental. [3] [4]
The trap to avoid is the premature anchor. A single plausible-sounding mechanism, a tidy family, or a normal platelet count does not cancel a high-specificity bruise pattern. Keep the differential open, run the rule, and let the pattern drive the evaluation rather than the first offered story. [1] [5]
Clinical & Bedside Assessment
Examine the child fully undressed. This is the single most important bedside action and the one most often skipped. A bruise on the back or ear will be missed while the child is dressed. Document every injury on a body map with measurements, colour, shape, and whether it is patterned. Use medical photography with a size reference. Record the developmental mobility of the child in the same note. [4]
Take the history of each injury separately and verbatim. Ask the caregiver to explain each mark, and record their exact words. Probe the mechanism: who was present, what was the child doing, on what surface, with what object. Then ask the developmental question: could a child at this stage of mobility produce that injury? A rolling two-month-old cannot strike their own ear; a cruising two-year-old can bang a shin. [2] [4]
Take a full psychosocial and safety history. Ask about parental mental health, substance use, intimate-partner violence, family stress, and prior child-protection involvement. Ask about the pregnancy and whether it was planned, about other children in the home, and about previous injuries. Do this with curiosity and without accusation; the goal is information, not confrontation. [4] [7]
Anatomy of a missed sentinel injury
- Week 0: Infant presents with a minor complaint; a small ear bruise is noted and attributed to the bouncy chair. [2]
- Week 2: Infant re-presents with a torn frenum; the sentinel injury is not linked to the earlier visit. [9]
- Week 6: Infant presents with abusive head trauma. Both earlier contacts are now recognised as missed sentinel injuries. [7]
Examine for occult injury as part of the bedside assessment. Look in the mouth for a torn frenum and oral bruising; palpate the abdomen for tenderness or guarding; examine the genitals if indicated; check the fontanelle and tone. The skin examination is the entry point, but the assessment extends to the systems that inflicted injury can damage silently. [9] [10]
Investigations
A skeletal survey is the core investigation for any child under two years with suspected physical abuse, and should be considered in older infants and toddlers depending on the clinical picture. The survey is a full set of dedicated radiographs, not a single babygram, and it should be repeated at about two weeks because occult fractures, especially rib and metaphyseal fractures, become visible as they heal. [4]
Coagulation testing is indicated when bruising is the presenting feature, and it should follow a structured panel rather than an isolated test. A reasonable screen includes full blood examination and platelet count, prothrombin time, activated partial thromboplastin time, fibrinogen, and a von Willebrand panel, with further testing guided by results. Critically, a normal coagulation screen does not exclude abuse, and the work-up should proceed in parallel with the safeguarding response rather than waiting on laboratory return. [4] [11]
Neuroimaging is indicated when there is any concern for abusive head trauma. An infant with bruising, especially facial or scalp bruising, warrants careful neurological assessment, and a low threshold for neuroimaging where any altered consciousness, seizures, vomiting, or an enlarging head circumference is present. Cross-link the abusive head trauma page for the full algorithm. [4] [7]
Consider additional tests by presentation: lipase or liver enzymes and abdominal imaging for possible visceral injury; toxicology if poisoning is suspected; and screening for occult injury in siblings and other young household contacts. Investigations are not a substitute for the safeguarding pathway — they run alongside it and inform the child-protection assessment. [10] [4]
Management — Resuscitation
Most bruising and sentinel injuries are not immediately life-threatening, but inflicted injury can hide a serious occult problem. Begin with ABCDE. A child who is shocked, has altered consciousness, ongoing seizure, respiratory distress, or signs of abusive head or abdominal trauma takes priority over documentation. [4]
If occult abdominal injury is suspected, resuscitate for potential blood loss, establish intravenous access, cross-match, and arrange urgent imaging. Inflicted abdominal injury carries a high mortality when missed because the external signs may be minimal. A tender or distended abdomen in a child with bruising is a surgical and safeguarding emergency at once. [10]
If there is any sign of abusive head trauma — altered consciousness, vomiting, seizures, apnoea, or an abnormal neurological examination — escalate immediately to senior paediatric and neurosurgical care. Do not attribute altered consciousness to a minor mechanism. Cross-link the abusive head trauma page for the resuscitation algorithm. [4] [7]
Ensure the child is in a safe place during and after resuscitation. The resuscitation bay is also a safeguarding space: maintain appropriate supervision, do not allow a suspected perpetrator to be alone with the child, and begin the child-protection referral in parallel with stabilisation. [4]
Management — Definitive & Stepwise
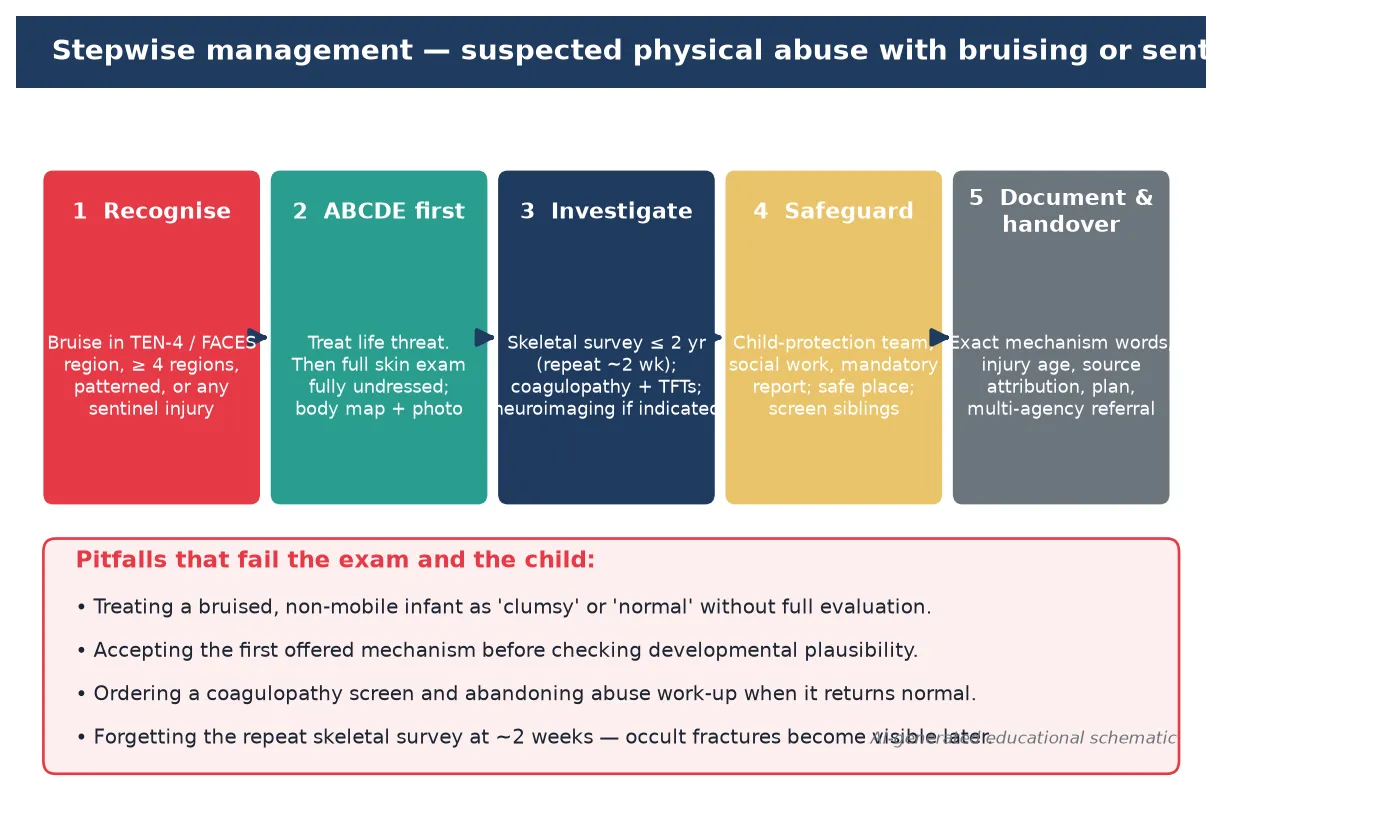
Once the child is stable, run a repeatable safeguarding algorithm. The steps below are the standard sequence; adapt timing to acuity but do not skip steps. [4] [2]
- Recognise the discriminating pattern or sentinel injury using TEN-4 FACES-L and developmental mobility.
- Examine fully undressed; document every injury on a body map with photography and measurements.
- Investigate with skeletal survey under two years (plus repeat at ~2 weeks), coagulopathy panel, and neuroimaging or abdominal imaging as indicated.
- Refer to the child-protection or social-work team and the designated doctor for child protection; arrange a place of safety if the child cannot go home.
- Report under your jurisdiction's mandatory reporting law; do not wait for certainty.
- Screen siblings and other young household contacts for occult injury.
- Document the mechanism verbatim, source attribution, your clinical reasoning, and the multi-agency plan. [4] [2] [7]
TEN-4 FACES-L
Place-of-safety decisions are made by the multi-agency team, not by a single clinician. The threshold for admission or alternative care is the assessed risk of further injury, not the severity of the current bruise. A sentinel injury may look minor, yet the risk of recurrence is real; err toward admitting the child for a place of safety while the assessment is completed. [2] [7]
Specific Subtypes & Scenarios
Bruise in a non-mobile infant. Any bruise in an infant not yet cruising is abnormal until proven otherwise. This is a single-trigger event: skeletal survey, coagulopathy panel, child-protection referral, and mandatory report. Do not accept a bouncy-chair or sibling explanation without evaluation. [3] [2]
Patterned bruising. A hand-slap, ligature line, bite mark, or implement imprint is inflicted by definition. Measure and photograph the pattern; a bite that breaks the skin or shows dental characteristics may need forensic dental review. Treat as a trigger for the full pathway. [4] [8]
Torn frenum in a pre-mobile infant. A torn upper labial frenum in a non-ambulatory infant is strongly associated with abuse and is a sentinel injury. Examine the mouth in every infant, arrange the full evaluation, and do not attribute it to a feeding spoon without assessment. [9]
The child with a bleeding disorder. A child with haemophilia or von Willebrand disease can be abused. A normal or abnormal coagulation result does not settle the question. Run the rule on the pattern, run the panel on the blood, and run the safeguarding pathway in parallel. [11] [4]
Palm bruising in an infant. Palm bruising in an infant is a recognisable pattern of abuse because no normal infant mechanism produces a bruise on the palm. Treat it as a high-specificity sign and pursue the evaluation. [8]
Sibling of an abused child. Siblings and other young household contacts of a child with confirmed or suspected abuse should be examined and screened for occult injury, including skeletal survey in those under two. Sentinel or occult injuries are commonly found in siblings. [4] [2]
Cultural practice marks. Coin rubbing, cupping, and moxibustion produce symmetric, openly explained marks on expected sites. Ask respectfully, document, and do not conflate with abuse — but do not let a claim of cultural practice override a genuine high-specificity pattern elsewhere. [4]
The well-looking sentinel-injury infant. An infant with a sentinel injury often looks well. The absence of systemic signs is expected and does not reduce the need for evaluation. The danger is precisely that the infant looks fine, so the injury is explained away and the next presentation is catastrophic. [2] [7]
Complications & Pitfalls
The leading pitfall is the explained-away sentinel injury. A minor bruise is attributed to a bouncy chair, a torn frenum to a spoon, a small mark to a sibling, and the child is discharged. When the same child later presents with abusive head trauma, the earlier contact is recognised as the missed opportunity. The remedy is a low threshold to evaluate any unexplained injury in a non-mobile infant. [2] [7]
The second pitfall is relying on bruise colour to date injuries. Colour change is too variable across individuals and sites to date a bruise reliably, and attempts to do so can mislead courts and clinicians. Document colour and location, but do not claim to date a bruise from its colour alone. [4]
The third pitfall is treating a normal coagulation screen as proof of abuse. A normal screen excludes some bleeding disorders but does not exclude rare ones and does not address the pattern. The work-up is parallel, not sequential, and the safeguarding response proceeds regardless. [11] [4]
The fourth pitfall is forgetting the repeat skeletal survey. Occult fractures, especially posterior rib and classic metaphyseal lesions, often only become visible as they heal. A single early survey will miss injuries that a repeat at about two weeks will show. [4]
The fifth pitfall is failing to screen siblings. Sentinel and occult injuries are found in siblings of abused children; omitting them leaves children in danger and weakens the assessment of the index child. [2] [4]
The sixth pitfall is corridor confrontation. Accusing a caregiver at the bedside endangers the child, destroys rapport, and has no investigative value. The clinician's role is to recognise, investigate, document, and refer; the multi-agency team conducts the investigation. [4]
Prognosis & Disposition
An infant with a recognised sentinel injury who receives a full evaluation and a place-of-safety plan has a materially better prognosis than one sent home. The point of early recognition is to interrupt the trajectory toward more severe injury. Children who are evaluated and protected after a sentinel injury avoid the recurrence that would otherwise have followed. [2] [7]
Disposition is a multi-agency decision. Admission for a place of safety is appropriate whenever the assessed risk of recurrence is non-trivial, regardless of how minor the current injury looks. The child may be discharged to a safe caregiver, to alternative care, or remain in hospital while the child-protection assessment and any legal orders are completed. [4]
Long-term, children who have been physically abused are at elevated risk of further abuse, developmental and mental-health sequelae, and family disruption. The follow-up plan should include developmental surveillance, mental-health support, and a clear re-presentation pathway. A single contact rarely ends the risk; continuity of care does. [4] [7]
Special Populations
Infants and non-mobile children are the highest-risk group for sentinel injury and carry the lowest threshold for evaluation. Preterm and low-birth-weight infants, and infants with disability or medical complexity, are over-represented among abused children and may be less able to signal discomfort, so a high index of suspicion is warranted. [2] [4]
Children with disability and neurodiversity are at increased risk of maltreatment and may communicate injury behaviourally. Accept alternative communication and carer expertise, and apply the same TEN-4 FACES-L logic without diluting the threshold because the child is disabled. [4]
Migrant, refugee, and asylum-seeking families may bring cultural practices that produce innocent marks and may face language barriers during assessment. Use a professional interpreter, ask about cultural practices respectfully, and do not let language discordance degrade the history of injury. [4]
Children in out-of-home care and youth-justice settings carry high background rates of maltreatment. Clarify legal decision-makers, expect fragmented history, and screen actively for both fresh and old injuries on presentation. [4]
Evidence, Guidelines & Regional Differences
The evidence base for discriminating bruising rests on three pillars. The first is the descriptive epidemiology of accidental bruising, which established that bruising is rare in non-mobile infants and rises with mobility. The second is the original discriminating-features work, which defined the TEN-4 components. The third is the multicentre validation of the rule, which confirmed high sensitivity for abuse in young children presenting with bruising and solidified the FACES-L additions. [3] [1] [5]
Sentinel-injury evidence comes from cohort studies of infants evaluated for abuse and from retrospective review of children with abusive head trauma, both of which show that prior minor injuries are common and often missed. These observational data are the basis for the prevention message that anchors this topic. [2] [7]
The bleeding-disorder differential is supported by recent work examining adherence to AAP recommendations on coagulation testing in suspected abuse, which informs how to run the panel in parallel with safeguarding. [11] [4]
Mandatory reporting of suspected child abuse applies in all Australian states and territories and in New Zealand, with the exact classes of reporter and grounds set by local statute. The Royal Australasian College of Physicians expects all paediatric trainees to recognise and act on suspected maltreatment. Use the RACP general paediatrics curriculum and your local child-protection unit for jurisdictional detail rather than a memorised universal rule. [4]
NICE guideline NG76 sets the UK approach to child abuse and neglect, and the RCPCH Child Protection Evidence series summarises the evidence on bruising. Mandatory reporting duties vary across the four nations; apply information-sharing duties and document clearly. MRCPCH stations reward recognition of high-specificity patterns and a structured safeguarding response. [4]
The AAP clinical report on the evaluation of suspected child physical abuse sets the US standard, including skeletal survey under two years, the repeat film, and coagulation testing. The ABP content outline and ACGME milestones treat recognition of child maltreatment as an entrustable skill. In Canada, the RCPSC Core EPA on recognising and managing suspected maltreatment frames the expectation. [4]
Exam Pearls
- Any bruise in a non-mobile infant is abnormal until proven otherwise. [3] [2]
- TEN-4 FACES-L: torso, ear, neck; FACES regions; four or more regions; large bruise. One positive feature triggers evaluation. [1] [5]
- A sentinel injury is a prior missed opportunity; act on it to prevent abusive head trauma. [2] [7]
- Patterned bruising is inflicted by definition — hand-slap, ligature, bite, implement. [4] [8]
- A torn frenum in a pre-mobile infant is a sentinel injury. [9]
- Do not date a bruise by its colour. [4]
- A normal coagulation screen does not close the case; run the panel in parallel with safeguarding. [11] [4]
- Always repeat the skeletal survey at about two weeks to catch occult rib and metaphyseal fractures. [4]
- Screen siblings and other young household contacts. [2]
- Examine every child fully undressed and document on a body map. [4]
- Record the caregiver's mechanism verbatim, then test it against developmental plausibility. [2]
- Do not confront a caregiver in the corridor; recognise, investigate, refer, and let the multi-agency team investigate. [4]
References
- [1]Pierce MC Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics, 2010.PMID 19969620
- [2]Sheets LK Sentinel injuries in infants evaluated for child physical abuse. Pediatrics, 2013.PMID 23478861
- [3]Sugar NF Bruises in infants and toddlers: those who don't cruise rarely bruise. Puget Sound Pediatric Research Network. Archives of pediatrics & adolescent medicine, 1999.PMID 10201724
- [4]Christian CW The evaluation of suspected child physical abuse. Pediatrics, 2015.PMID 25917988
- [5]Pierce MC Validation of a Clinical Decision Rule to Predict Abuse in Young Children Based on Bruising Characteristics. JAMA network open, 2021.PMID 33852003
- [6]Petska HW Sentinel injuries: subtle findings of physical abuse. Pediatric clinics of North America, 2014.PMID 25242706
- [7]Letson MM Prior opportunities to identify abuse in children with abusive head trauma. Child abuse & neglect, 2016.PMID 27680755
- [8]Ruiz-Maldonado TM Palm Bruising in Infants: A Recognizable Pattern of Abuse. The Journal of emergency medicine, 2021.PMID 33795168
- [9]Maguire S Diagnosing abuse: a systematic review of torn frenum and other intra-oral injuries. Archives of disease in childhood, 2007.PMID 17468129
- [10]Maguire SA A systematic review of abusive visceral injuries in childhood--their range and recognition. Child abuse & neglect, 2013.PMID 23306146
- [11]Hultman L Testing for bleeding disorders in child abuse: AAP recommendation adherence and testing results. Child abuse & neglect, 2025.PMID 40158474