Paeds · child-safety-and-social-paediatrics
Poisoning as maltreatment
Also known as Non-accidental poisoning · Fabricated or induced illness · Munchausen syndrome by proxy · Medical child abuse · Pediatric condition falsification · Covert poisoning
Fellowship guide to poisoning as a form of child maltreatment — the deliberate administration or withholding of a substance by a caregiver to harm or fabricate illness in a child. Covers non-accidental poisoning and the induced-illness subtype (Munchausen syndrome by proxy / fabricated or induced illness), Rosenberg's defining triad, the common inducing agents (salt, insulin, sedatives, emetics), the bizarre recurrent toxidrome that resolves only on separation, the toxicology and covert-surveillance workup, and a stepped plan that treats the poisoning, secures the child, confirms the diagnosis, and triggers mandatory child-protection action across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A two-year-old keeps being admitted with unexplained drowsiness and seizures that no metabolic, infectious or neurological workup can explain, that happen only at home, and that stop the moment she is on the ward. The question an examiner wants you to hold is not "what rare disease is this?" but "who is producing it?" — because poisoning as maltreatment is a fabrication, not a misfortune. A caregiver is deliberately giving a substance, or withholding one, to harm the child or to manufacture the very illness you are being asked to diagnose. [1] [5]
The working definition is operational and rests on the caregiver's behaviour, not on a single laboratory value. Induced illness exists when a parent or carer fabricates, induces or exaggerates symptoms — by lying about the history, falsifying samples, contaminating lines, or actually administering a substance — in a child who is, in consequence, presented as more ill than they are and subjected to unnecessary investigation and treatment. The harm has two layers: the direct toxic effect of the agent, and the iatrogenic harm of the investigations, surgeries and treatments that follow from a false picture. [6] [10]
Two subtypes overlap in practice but are worth naming separately. Non-accidental poisoning is the deliberate administration of a toxic substance — salt, insulin, sedatives, emetics — with the intent to harm. Fabricated or induced illness, once called Munchausen syndrome by proxy and now medical child abuse or pediatric condition falsification, is the broader pattern in which the caregiver produces symptoms to live the medical role through the child. Poisoning is the induced, most dangerous edge of that spectrum. [2] [5]
Deep technique on inflicted physical injury lives on the abusive-head-trauma and physical-abuse leaves, neglect on its own leaf, and mandatory reporting on the protection-frameworks leaf. This page owns poisoning as maltreatment — non-accidental poisoning and the induced-illiness subtype — with the toxidrome, the workup, the separation test, and the safeguarding conversion as the focus. [6] [9]
Classification
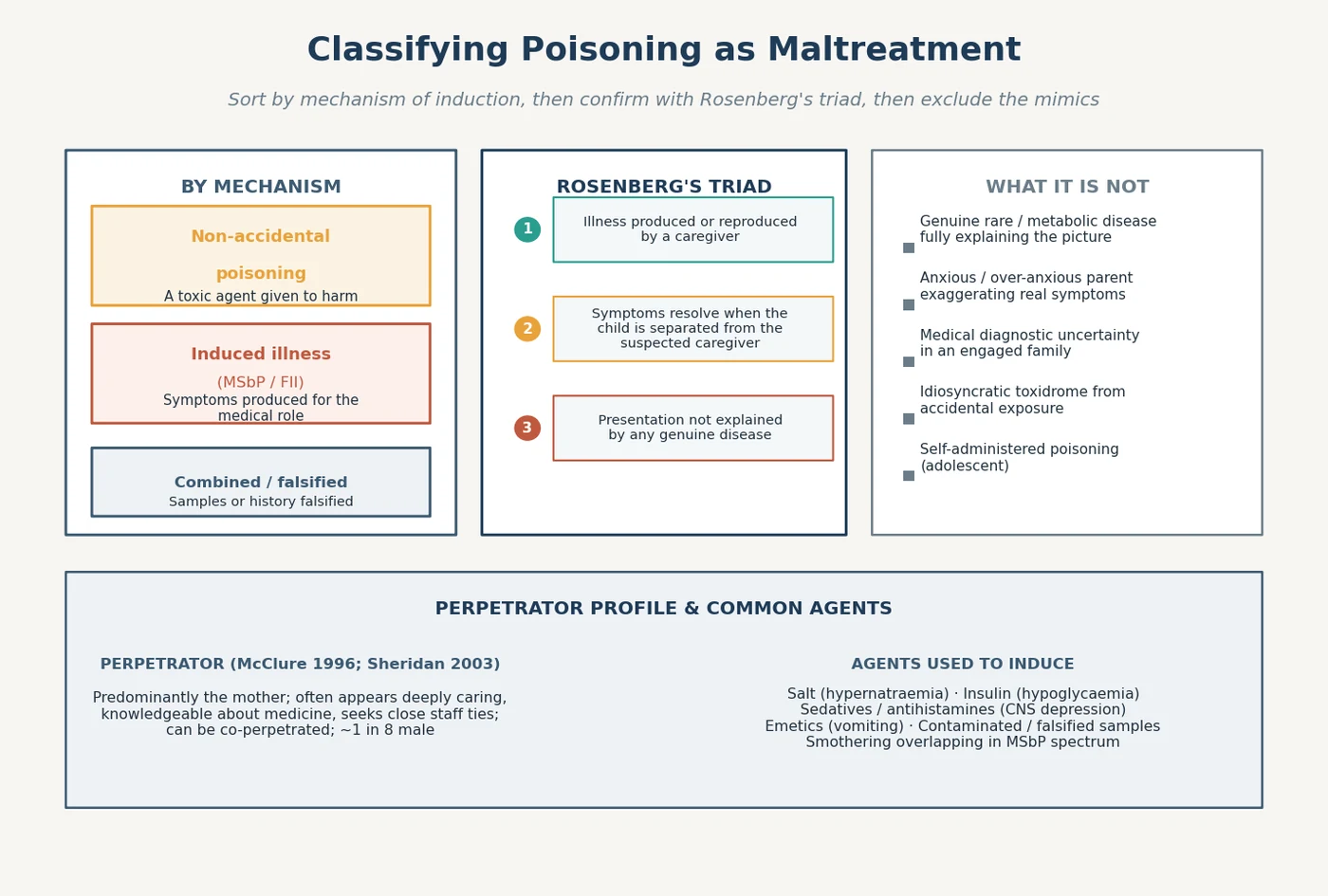
Sort every suspected case along two lines before you name the plan: how the illness is being produced, and whether the picture fits Rosenberg's triad or is one of the mimics. The same drowsy child means something different in a family with a rare metabolic disease who are engaged and consistent than in a family whose story keeps changing. [1] [10]
By mechanism of induction
Non-accidental poisoning
Induced illness (MSbP / FII)
Combined / falsified
The agent tells you the toxidrome to expect and the test to send. Salt drives hypernatraemia with seizures and brain injury; insulin or oral hypoglycaemics drive recurrent hypoglycaemia; sedatives, antihistamines and opioids drive central-nervous-system and respiratory depression; emetics, laxatives and diuretics drive dehydration and electrolyte chaos; and contaminated or falsified samples drive the team down a false investigative path. [3] [11]
By Rosenberg's triad and by exclusion
The triad — caregiver-produced, separation-resolving, disease-unexplained — sorts the genuine case from the mimic. The exclusions matter as much as the inclusions: a genuine rare or metabolic disease that fully explains the picture, an anxious parent exaggerating real symptoms, ordinary diagnostic uncertainty in an engaged family, an idiosyncratic or accidental toxidrome, and self-administered poisoning in an adolescent. Each exclusion changes the response, and none is made safely without the multi-agency information that distinguishes a pattern from an event. [1] [10]
Epidemiology & Risk Factors
Induced illness is rare but devastating, and the rarity is part of the danger: because most paediatricians see it seldom, the diagnosis is delayed and the child accrues harm while it is worked up as a metabolic or neurological mystery. McClure and colleagues captured the epidemiology of Munchausen syndrome by proxy alongside non-accidental poisoning and non-accidental suffocation in UK surveillance data, and the shared finding was that these are uncommon events with disproportionate mortality and recurrence. [2]
The perpetrator profile is consistent across the literature and is itself a clue rather than a stereotype. The caregiver is most often the biological mother, who appears deeply attentive, knowledgeable about the illness, and eager to forge close ties with staff; she may welcome invasive investigation and resist discharge. A minority of perpetrators are male, and co-perpetration occurs. Sheridan's updated review of several hundred cases held these features steady across decades and settings, and they frame why the diagnosis is so often missed — the family does not look neglectful. [5] [12]
Risk aggregates where caregiver capacity and child vulnerability meet. A perpetrator with a background of somatising, self-harm, personality difficulty or unresolved trauma; a young, pre-verbal or disabled child who cannot disclose; a family already known to child protection; and a clinical setting that trusts the articulate parent over the silent child all raise the risk that induction is both possible and undetected. Structural disadvantage is not the driver here as it is in neglect — the driver is the perpetrator's behaviour — but social isolation and medical sophistication raise the barrier to detection. [6] [9]
Pathophysiology
Harm in poisoning as maltreatment is the direct toxic or pharmacological effect of the administered agent, and that is why the toxidrome is the centrepiece of the bedside picture. Salt drives water out of brain cells and produces hypernatraemic seizures and brain injury; insulin drives glucose into cells and produces recurrent hypoglycaemic seizures and coma; sedatives and antihistamines depress the central nervous system and the respiratory drive; emetics and laxatives dehydrate and derange electrolytes. The child looks acutely, genuinely, dangerously ill — because they are. [3] [11]
Layered on the toxic effect is the iatrogenic harm, and an examiner will credit you for naming it. The false picture drives invasive investigation, repeated procedures, surgery, long admissions and powerful treatments that would never be given if the induction were known. The child is harmed twice: once by the poison, and again by the medicine applied to a lie. The induction succeeds precisely because the produced symptoms are real and the resulting encounters are clinically plausible. [6] [7]
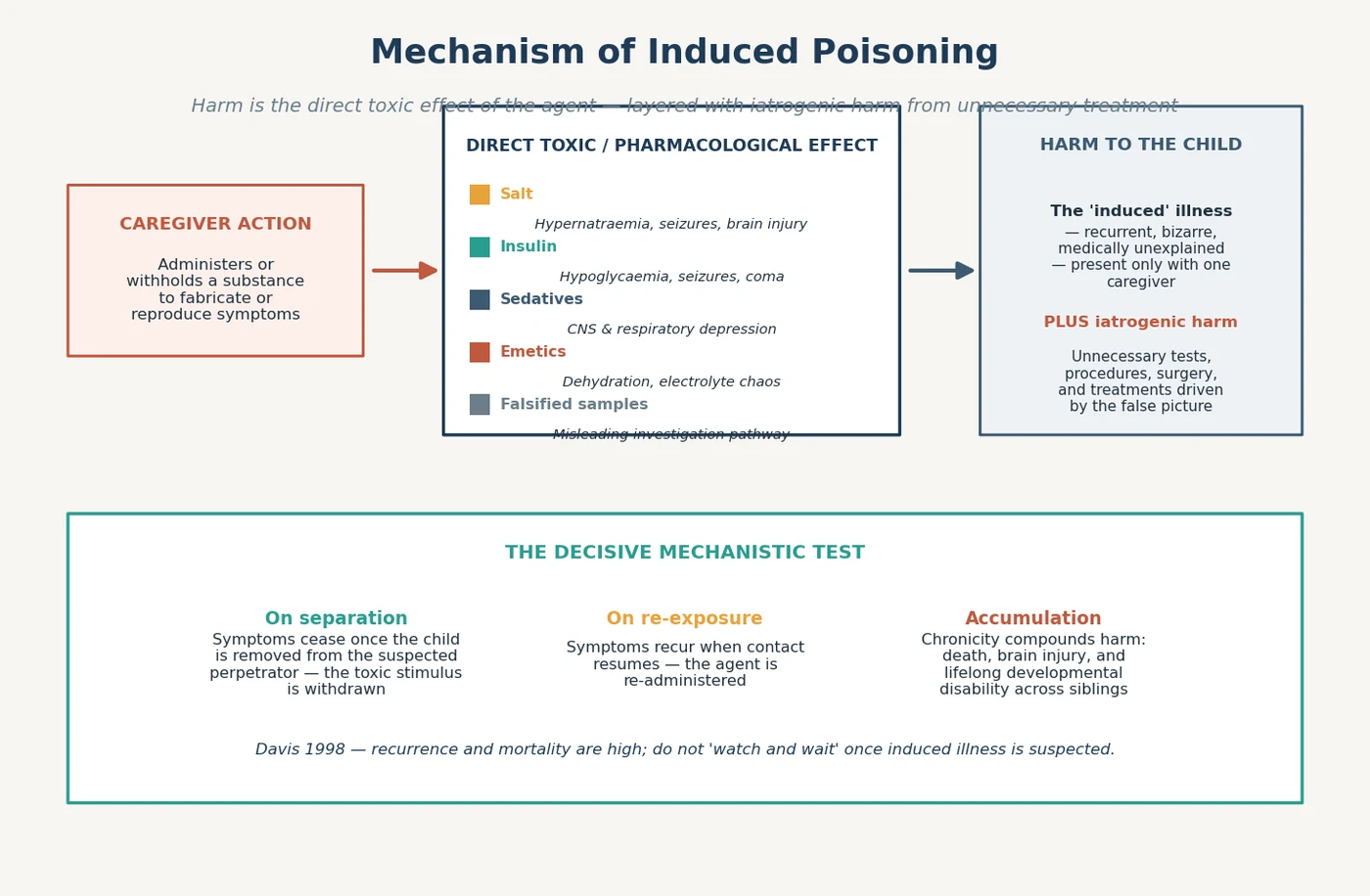
The neuroscience of separation holds the diagnosis and is the mechanistic test a candidate must defend. Withdraw the suspected perpetrator and the toxic stimulus is withdrawn, so the illness resolves; restore contact and the agent is re-administered, so the illness recurs. The same plasticity that makes chronic induction damaging means a child removed early can recover, which is why watching and waiting fails the child — the harm accumulates across admissions and across siblings. [4] [7]
Clinical Presentation
The presentation is a toxidrome that does not fit any disease and that follows the suspected caregiver rather than the child. Recurrent, bizarre, medically unexplained symptoms — unexplained drowsiness, seizures, apnoea, vomiting, hypoglycaemia or hypernatraemia — that occur only at home or only in one person's presence, that remit on admission, and that recur on discharge, are the signature. [1] [5]
Examine the inconsistencies as carefully as you examine the child. The reported history does not match the observed clinical course; the symptoms do not fit the physiology; the caregiver reports dramatic events that staff never witness; the child improves the instant the suspected caregiver leaves the bedside; and new symptoms appear when the caregiver returns. A list of these inconsistencies, kept prospectively in the chart, is often the first concrete evidence that induction is occurring. [6] [10]
[3] [9]The presentation differs by agent and by age. An infant or pre-verbal toddler presents with apnoea, seizures or collapse that the parent reports but staff never corroborate; a school-age child may describe symptoms to staff that contradict the parent's account, or may themselves be terrified of going home; an adolescent may self-poison, which must be separated from induction. Across ages, the unifying feature is that the illness is chronic, recurrent and inexplicable until the caregiver's behaviour is considered. [7] [8]
Differential Diagnosis
The differential is the reason induced illness is missed: every toxidrome and every unexplained recurrent illness has a long list of organic causes, and the clinician defaults to the rare disease rather than the deception. Your task is to hold both possibilities at once — investigate the organic cause thoroughly, and hold the safeguarding suspicion in parallel — because pursuing only one is the classic error. [6] [7]
INDUCE — the differential you must actively exclude
The two mirror-image errors define the failure mode. Over-calling induction in a child with a genuine rare disease subjects a sick child and an innocent family to a safeguarding process and delays the true diagnosis; under-calling induction in a child whose bizarre recurrent illness is being manufactured leaves them to be poisoned again. The discriminating move is never a single test — it is the multi-agency pattern: the chart, the school, the general practitioner, prior admissions, and the sibling history, assembled by the safeguarding team. [1] [8]
Clinical & Bedside Assessment
Take a meticulous, contemporaneous history and document the inconsistencies as they arise, because the chronology is the evidence. Record who gave what history, what was observed by staff, when symptoms occurred relative to the caregiver's presence, and any prior unexplained episodes in this child or siblings. Use a curious, non-confrontational stance with the family — the goal of the early encounter is to keep the child safe and the family engaged, not to extract a confession. [6] [7]
Examine the child fully and serially. Map the toxidrome, look for signs of repeated medical intervention — healed cannula sites, old surgical scars, patches of alopecia — and examine for coexisting inflicted injury that points to a broader pattern of abuse. Assess development and growth, which often falter across a long induction history, and note the child's demeanour: some induced children are strikingly attached to the perpetrating caregiver and numb to painful procedures. [5] [9]
Gather multi-agency information early and with the safeguarding team. Contact the general practitioner, the treating specialists, the hospital records from other centres, the school or early-learning service, and child protection, and ask specifically about siblings. Induction is almost never the story a single encounter tells; it is the story that emerges when a chronology across settings and clinicians is assembled — which is why the named safeguarding lead, not a lone registrar, owns this assessment. [4] [8]
Investigations
Investigate the toxidrome as genuine poisoning, and sample before you treat the picture away. Send blood and urine for a comprehensive toxicology screen, with specific assays guided by the suspected agent — a paired insulin and C-peptide for suspected exogenous insulin, a glucose and sodium for suspected salt or hypoglycaemic induction, and save residual serum and urine frozen, because the agent may only become clear later. Hair sampling extends the window backwards for chronic exposure, and contaminated samples should be re-drawn from a fresh, witnessed site. [3] [11]
Run the organic workup in parallel so that the exclusion of genuine disease is documented, not assumed. Metabolic, endocrine, neurological and infectious testing proceeds alongside the toxicology, because the safeguarding threshold and the clinical diagnosis both require you to show that no disease explains the picture. The workup is not a reason to delay protecting the child — if the suspicion is strong, secure the child first and complete the confirmation under a safeguarding plan. [6] [7]
The separation-and-confirmation sequence
Covert video surveillance is a confirmation tool, not a fishing expedition, and it belongs to the multi-agency strategy, not to a curious clinician. Used judiciously in a minority of cases where the suspicion is high but the evidence is incomplete, it has captured the act of induction and prevented further harm; used improperly it is unethical and legally hazardous. Decide whether it is indicated with the safeguarding team, the hospital legal service, and the police, and document the decision. [5] [7]
Management — Resuscitation
Treat the toxidreme first, because the child is genuinely, acutely ill from the agent. Stabilise the airway, breathing and circulation, control seizures, correct dangerous metabolic derangement, and sample for toxicology before the treatments that will mask the picture. The resuscitation is real paediatric emergency medicine — the safeguarding dimension runs alongside it, never instead of it. [3] [9]
Once the child is stabilised, secure them. The single most dangerous action at this stage is to discharge the child to the suspected perpetrator while the diagnosis is unresolved, because the agent will be re-administered. Admit the child, do not allow unsupervised access by the suspected caregiver without a safeguarding plan, and involve the named safeguarding lead and the duty social worker the same day. Separation is both the protective move and the diagnostic confirmation. [4] [6]
Management — Definitive & Stepwise
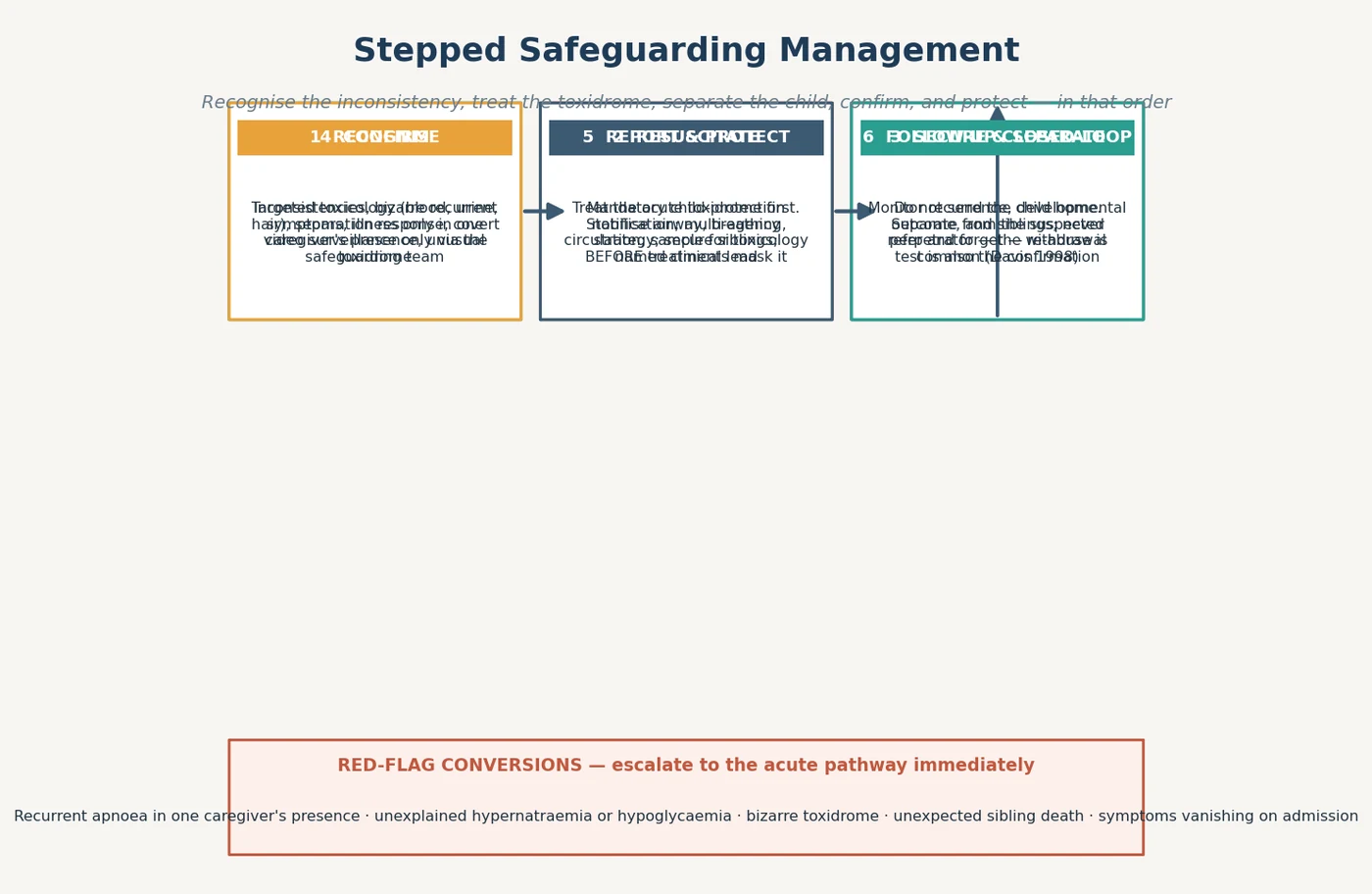
The definitive plan is a stepped, multi-agency safeguarding pathway that proceeds from recognition to closed-loop follow-up, and it is owned by the safeguarding team rather than by a lone clinician. Each step protects the child while the evidence is gathered; none substitutes for the next. [6] [8]
Step 1 — Recognise
Hold the safeguarding suspicion in parallel with the organic differential, document the inconsistencies prospectively, and escalate to the named safeguarding lead early. The recognition is the rate-limiting step: most cases are delayed because induction is never considered, so the discipline is to ask "who is producing this?" whenever a bizarre recurrent toxidrome presents. [6] [10]
Step 2 — Resuscitate and sample
Treat the acute poisoning and draw the toxicology before you mask the picture, as above. The samples gathered in the first hours of an acute presentation are often the only objective evidence of the agent, and they cannot be retrieved later. [3] [11]
Step 3 — Secure and separate
Admit the child, do not send them home, and separate them from the suspected perpetrator under a documented safeguarding plan. Observe the response to separation, which confirms the diagnosis when the toxidrome resolves without the caregiver present — and which protects the child from re-exposure while confirmation proceeds. [1] [4]
Step 4 — Confirm
Complete the targeted toxicology, the separation-response observation, and, where indicated within the legal framework, covert video surveillance coordinated by the safeguarding team. Document the exclusion of genuine disease so that the diagnosis rests on both the positive evidence of induction and the negative evidence of no organic cause. [5] [7]
Step 5 — Report and protect
Make the mandatory child-protection notification, convene the multi-agency strategy meeting, and secure the siblings, who carry the same recurrence risk. The paediatrician's role is recognition, stabilisation, evidence-gathering, reporting and coordination — not forensic investigation or statutory casework, which belong to child protection and the police. [2] [8]
Specific Subtypes & Scenarios
Salt poisoning is the named, examinable archetype, codified by Meadow, in which a caregiver administers salt to produce severe hypernatraemia with seizures and brain injury. The clues are recurrent unexplained hypernatraemia, polyuria from salt-induced diabetes insipidus, and resolution on separation; the confirmation is paired serum and urine osmolality and sodium with the separation response, sampled before fluid correction obscures the picture. [3]
Insulin or hypoglycaemic induction produces recurrent, severe, otherwise-unexplained hypoglycaemia, and the discriminating test is a paired insulin and C-peptide during a hypoglycaemic episode — high insulin with suppressed C-peptide points to exogenous administration rather than an insulinoma. Suspect it whenever a child has recurrent hypoglycaemic seizures that follow a caregiver's presence and resolve on admission. [6] [11]
Sedative or antihistamine induction, as illustrated by case reports such as alimemazine poisoning, presents as recurrent drowsiness or respiratory depression without an identified cause. The toxicology screen identifies the agent, the chronology links it to the caregiver, and the separation test confirms it. [11]
Complications & Pitfalls
[4] [6]Mortality and recurrence are high, and that is why watching and waiting fails. Davis and colleagues showed that children subjected to Munchausen syndrome by proxy, non-accidental poisoning and non-accidental suffocation carry a substantial risk of further abuse, and that risk extends to siblings — some of whom die. Once induced illness is suspected, the burden of proof shifts, and the safe default is to secure the child and the siblings while confirmation proceeds. [4] [5]
The pitfalls are procedural as much as clinical. Confronting or accusing the suspected caregiver before the child is safe and the strategy agreed destroys the separation opportunity and endangers the child. Discharging home to the suspected perpetrator, neglecting the siblings, pursuing only the organic differential and never the safeguarding suspicion, and relying on a single clinician rather than the multi-agency team are the failures that recur in case reviews. [7] [8]
Prognosis & Disposition
The prognosis is guarded and is determined by how early the induction is recognised and stopped. Children removed early from the toxic stimulus can recover, but chronic induction leaves death, brain injury, developmental disability and severe attachment disturbance, and the harm extends across siblings. A disposition that treats induction as a one-off event, rather than a chronic recurrent pattern, fails the child. [4] [5]
Disposition is a closed-loop, multi-agency plan with a named clinical lead. The child is placed safely — at home only with the non-perpetrating caregiver under a protection plan, or in out-of-home care where the risk demands it — the siblings are assessed and protected, the developmental and mental-health sequelae are addressed, and the follow-up monitors for recurrence. Re-abuse is common, so the file is never closed on a single intervention. [8] [12]
Special Populations
Children with disability or complex medical needs are over-represented among victims, because their genuine medical complexity both provides cover for the induction and makes disclosure impossible. A child with a real chronic illness can also be induced — the presence of disease does not exclude maltreatment, and the two may coexist in the same child, which raises the detection barrier further. Assess function and chronology, not the headline diagnosis. [9] [12]
Siblings must be assessed in every case, because the recurrence risk extends to them and the mortality is real. A sibling death, near-miss, or unexplained chronic illness in the family is both a red flag and a reason to widen the protection plan immediately, before further harm occurs. [2] [4]
Children in out-of-home care may carry a history of prior induction that complicates their presenting picture, and culturally and linguistically diverse families require careful interpreter-mediated assessment so that communication difficulty is not mistaken for deception, nor deception hidden behind it. The safeguarding principles are identical across populations; what changes is the care taken to gather the chronology fairly. [8] [9]
Evidence, Guidelines & Regional Differences
[7] [8]The evidence base is case-series and surveillance-driven rather than trial-based, because induced illness is rare and cannot ethically be studied by randomisation. The high-quality evidence comes from the UK and international surveillance studies of McClure and Meadow, the large case reviews of Rosenberg and Sheridan, and the consensus guidance of the RCPCH and the AAP. Reproduce the defining principles and named evidence — Rosenberg's triad, Meadow's salt-poisoning criteria, the McClure epidemiology, the Sheridan series, the Bass and Glaser management framework — without inventing incidence figures or agent-specific mortality. [1] [5]
The regional difference that matters is the reporting and surveillance pathway, not the clinical recognition. The triad, the toxidrome, the separation test and the multi-agency principle travel intact across ANZ, the UK, the US and Canada; what changes is the statute that triggers the notification, the service that owns covert surveillance, and the threshold for emergency removal. Name the principle and your local child-protection service, and do not invent jurisdiction-specific statute clauses. [6] [8]
Exam Pearls
ROSENBAUM — hold the whole case
The discriminating candidate does four things the others miss. They hold the safeguarding suspicion in parallel with the organic differential rather than choosing one. They sample for toxicology before the picture is masked. They secure and separate the child rather than discharging to the suspected perpetrator. And they own the multi-agency strategy with a named lead and a closed-loop follow-up that protects the siblings — because induced illness is chronic, recurrent and lethal, and watching and waiting is not a plan. [6] [8]
References
- [1]Rosenberg DA Web of deceit: a literature review of Munchausen syndrome by proxy Child Abuse Negl, 1987.PMID 3322516
- [2]McClure RJ, Davis PM, Meadow SR, Sibert JR Epidemiology of Munchausen syndrome by proxy, non-accidental poisoning, and non-accidental suffocation Arch Dis Child, 1996.PMID 8813872
- [3]Meadow R Non-accidental salt poisoning Arch Dis Child, 1993.PMID 8503665
- [4]Davis P, McClure RJ, Rolfe K, Chessman N, Pearson S, Sibert JR Procedures, placement, and risks of further abuse after Munchausen syndrome by proxy, non-accidental poisoning, and non-accidental suffocation Arch Dis Child, 1998.PMID 9613350
- [5]Sheridan MS The deceit continues: an updated literature review of Munchausen Syndrome by Proxy Child Abuse Negl, 2003.PMID 12686328
- [6]Bass C, Glaser D Early recognition and management of fabricated or induced illness in children Lancet, 2014.PMID 24612863
- [7]Glaser D, Davis P For debate: Forty years of fabricated or induced illness (FII): where next for paediatricians? Paper 2: Management of perplexing presentations including FII Arch Dis Child, 2019.PMID 29618483
- [8]Tully J, Hopkins O, Smith A, Williams K Fabricated or induced illness in children: A guide for Australian health-care practitioners J Paediatr Child Health, 2021.PMID 34310788
- [9]Hobbs CJ, Bilo RA Nonaccidental trauma: clinical aspects and epidemiology of child abuse Pediatr Radiol, 2009.PMID 19198825
- [10]Meadow R What is, and what is not, 'Munchausen syndrome by proxy'? Arch Dis Child, 1995.PMID 7618944
- [11]Gomila I, Lopez-Corominas V, Pellegrini M, Quesada L, Miravet E, Pichini S Alimemazine poisoning as evidence of Munchausen syndrome by proxy: A pediatric case report Forensic Sci Int, 2016.PMID 27567044
- [12]Focardi M, Guerini M, Defraia B, Nanni L, Grifoni R, Castellini G Medical Child Abuse: A Retrospective Analysis from a Tertiary Pediatric Hospital's Childhood and Adolescent Abuse Group Children (Basel), 2025.PMID 41300691