Paeds · child-safety-and-social-paediatrics
Poverty, food insecurity and social prescribing
Also known as Childhood poverty · Material hardship and child health · Food insecurity in children · Social determinants of health screening · Social prescribing and community referral · Health equity and the paediatric medical home
A fellowship approach to poverty and food insecurity as the most prevalent risk to child health: how material hardship, food insecurity and housing instability become biology through a toxic-stress cascade; how to screen every family with validated tools (the two-item Hunger Vital Sign and social-needs instruments); how to co-design and deliver a social prescription that connects a family to food, income, housing and welfare support; and how to advocate at the bedside and the policy level — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-year-old girl is brought to your clinic for school-entry immunisation. Her mother has lost her casual job, the family has been evicted, and the child has missed three months of school. She is quiet, her growth has fallen across centiles, and her mother asks quietly whether you know anywhere that gives food. This is the everyday work of social paediatrics, and the clinical skill it tests is whether you treat poverty as a clinical problem you can act on, rather than a background fact you file away. [2] [1]
Poverty is not simply low income; it is the inability to meet the material needs that keep a child housed, fed, warm, safe and able to participate. In paediatrics we frame it as material hardship — the lived experience of going without food, stable housing, heating, or health care because the household cannot afford them — because that is the exposure that becomes biology. [2] [11]
Food insecurity is the limited or uncertain availability of nutritionally adequate and safe food, or the limited or uncertain ability to acquire food in socially acceptable ways. It runs from marginal anxiety about running out, through reduced diet quality, to very low food security where intake is disrupted and children go hungry. It is measured, not guessed, with a validated two-item screen. [3] [5]
Social prescribing is the structured pathway by which a clinician identifies a family's unmet social needs and connects them to community resources — food programs, income and welfare rights support, housing and utility assistance, and community activities — often through a link worker who bridges the clinic and the community. It is the operational tool that turns screening into action. [17] [16]
What makes this topic clinically distinct is that the exposure is modifiable. Unlike many diagnoses in paediatrics, poverty and food insecurity are conditions you can change with a referral, a prescription for food, or an advocacy action — and the evidence that doing so improves child health and development is now strong. [9] [12]
The clinician's role is to be the family's advocate within a medical home that screens routinely, responds proportionately, and closes the loop. You screen because hardship is common and invisible; you act because inaction is itself a harm; and you advocate because the dose of adversity a child carries is a matter of policy, not just of parenting. [2] [13]
Classification
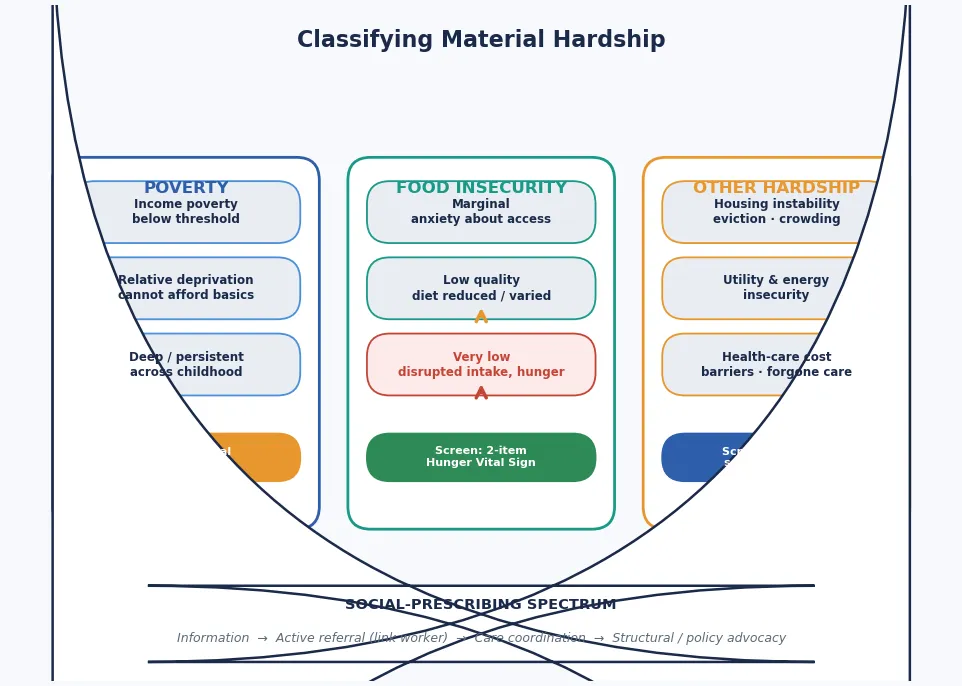
Begin with the family in front of you, then classify what kind of hardship they face and how severe it is, because severity drives the urgency and the intervention. [11]
Income poverty
Household below threshold
- Measured against local income lines (relative or absolute)
- Necessary but not sufficient — captures income, not lived experience
- Deep or persistent poverty across childhood carries the worst outcomes
- Often coexists with but does not equal material hardship
Food insecurity
Uncertain access to food
- Marginal — anxiety about running out, no reduction in intake
- Low — reduced diet quality, variety, or portions
- Very low — disrupted eating patterns, child hunger
- Screen with the validated two-item Hunger Vital Sign
Housing instability
Shelter insecurity
- Crowding, multiple moves, or falling behind on rent
- Eviction and homelessness are acute crises with measurable child harm
- Linked to developmental delay and behavioural difficulty
- Ask explicitly — families rarely volunteer it
Energy & utility insecurity
Inability to heat or power the home
- Thermal stress, food spoilage, and interrupted device use
- Linked to respiratory and mental-health difficulty
- Often captured in composite social-needs tools
- Eligible for targeted welfare and utility assistance
The severity gradient matters at the bedside because it tells you how urgently to act. Marginal food insecurity predicts poorer health even before intake falls, which is why screening picks up families who would not otherwise be identified. Very low food security, eviction, and homelessness are acute, and they join the resuscitation track alongside organic disease. [5] [18]
Whatever the domain, the screening lens is universal. Every family is asked, at every well-child contact, because hardship is common, fluctuating, and often invisible — and because the harm begins before a child looks undernourished. Routine, destigmatised screening is the standard of care. [10] [2]
Epidemiology & Risk Factors
Poverty and food insecurity are common across all four jurisdictions an examiner will expect you to know. Roughly one in six to one in five children lives in income poverty across Australia, New Zealand, the UK, the US and Canada, and food insecurity affects a substantial minority of households with children — with rates that rise sharply in times of economic shock, inflation, and housing crisis. [2] [13]
Young children are over-represented among those living in poverty, which makes the developmental stakes especially high. The brain and stress-response systems are most plastic in exactly the years these children are most exposed to material deprivation, so the biological cost concentrates in the first years of life. [1] [6]
The health burden is not a modest upward shift; it is large across nearly every domain an examiner names. Food insecurity in children under four is associated with poorer health, developmental risk, and increased hospitalisation, and school-age food-insecure children show deficits in academic performance, weight gain, and social skills. [5] [4]
Housing instability is its own epidemic with measurable child harm. Families with very young children who experience eviction show increased household hardship, food insecurity, and child and caregiver health problems — so housing is a clinical vital sign, not a social footnote. [18] [14]
The relationship between material hardship and outcome is dose-responsive. Each increment of deprivation — each move, each missed meal, each period of cold or crowding — adds to the cumulative adversity that shapes the developing brain and stress response. This is why screening and intervening early matters: you are reducing the dose. [1] [7]
Subgroups carry the highest cumulative risk and are the ones an examiner will probe: families with young children, single-parent households, Indigenous and minority families, migrant and refugee families, rural and remote families, and those already in contact with child protection or mental-health services. [2] [13]
The most powerful epidemiological finding for an exam is that the burden is reversible. When families receive income supplements, children show improved long-term functioning in adulthood — evidence that poverty is a treatable condition, not an immutable fact. [15] [13]
Pathophysiology
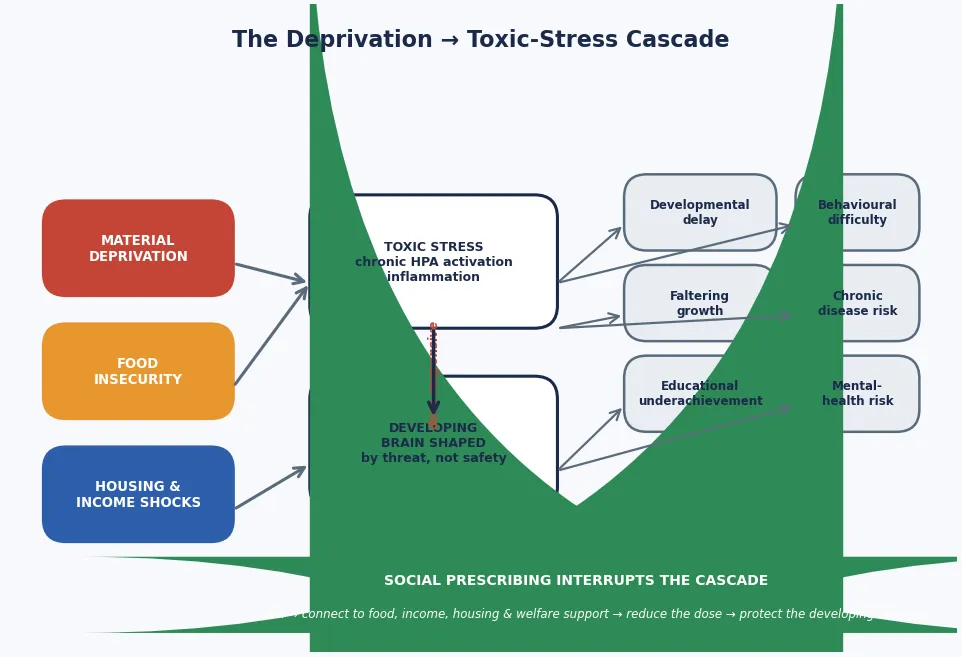
The clinical picture only makes sense once you see how material deprivation becomes biology. Poverty, food insecurity and housing instability accumulate as adverse childhood experiences, and those experiences act on a developing child through a toxic-stress mechanism. [7] [1]
Toxic stress persistently activates and dysregulates the stress response — the HPA axis, immune signalling and neurodevelopment — so that the developing brain is shaped by chronic threat rather than by safety. The relationship is dose-responsive: more cumulative deprivation produces more dysregulation, which is why the youngest children, whose brains are most plastic, carry the deepest developmental risk. [6] [7]
Food insecurity is not merely "less food." Chronic inadequate nutrition during the period of most rapid brain growth impairs neurodevelopment directly, and the household anxiety, disrupted routines, and trade-offs between food and other essentials create chronic psychological stress that feeds the same toxic-stress pathway. [5] [4]
Housing instability adds a distinct mechanism of harm beyond income. Each eviction, each move, and each period of crowding severs the routines, sleep, schooling and relationships that a child depends on — and the resulting allostatic load tracks into measurable health and developmental deficit. [18] [14]
Material deprivation also changes how a family experiences the clinical encounter. A parent who cannot afford transport, who fears judgement, or who is choosing between food and a prescription may delay presenting, ration medication, or withhold the truth of their hardship — so non-attendance, partial adherence, and late presentation are clinical data about deprivation, not character flaws. [2] [11]
The pathophysiology also explains why the intervention works: by reducing the dose of adversity, social prescribing changes the biology. Income support, food security, and stable housing reduce HPA activation and improve developmental outcomes — the toxic-stress cascade is interruptible. [15] [12]
Clinical Presentation
A family experiencing material hardship may present in two ways: acutely, with a crisis such as eviction, faltering growth, or an untreated acute illness, or routinely, at a well-child visit where the hardship is meant to be found by screening. The acute presentation is the emergency; the routine presentation is where the invisible burden is uncovered. [2] [5]
Food insecurity shows itself differently at different ages. An infant may present with faltering growth, an unsettled feeding pattern, or iron-deficiency anaemia; a preschooler may have behavioural dysregulation, frequent infections, or poor sleep; and a school-age child may show declining academic performance, social withdrawal, or recurrent abdominal pain. None of these is diagnostic on its own; each is a signal to screen. [4] [5]
Developmental and educational difficulty often presents as the first visible harm of poverty. A child who has fallen behind on milestones, who is struggling at school, or whose behaviour has been labelled "naughty" rather than understood as a response to material stress is the everyday face of deprivation-driven delay. [6] [12]
Behavioural and mental-health difficulty is common and bidirectional. Food-insecure children show higher rates of anxiety, irritability and behavioural difficulty, and the household stress that accompanies hardship drives parental mental-health problems that further shape child outcomes. The mechanism is the same toxic-stress cascade, not a separate problem. [7] [1]
Housing instability presents clinically as a pattern rather than a single event: missed appointments because of a move, repeated acute presentations from different addresses, sleep disruption from crowding, and a child whose health and schooling regress after each relocation. The pattern is the diagnosis. [18] [14]
A family may disclose hardship only indirectly. A parent who asks whether you know a food charity, who delays filling a prescription, who misses appointments because transport is unaffordable, or whose child comes to clinic hungry is telling you about material deprivation — and you should name it, screen for it, and act on it. [2] [11]
At the well-child visit you will often find the unmet burden made concrete: growth that has fallen across centiles, iron-deficiency anaemia, dental caries, incomplete immunisation, and developmental delay that no one has yet named — each of which is a clinical signal pointing back to the social determinant. [5] [12]
Differential Diagnosis
The central diagnostic skill is telling apart the harm caused by material deprivation from organic disease — and resisting the pull to assume a symptom is "just social." Faltering growth may reflect food insecurity, but it may also be organic, and the two coexist; you must investigate both. [5] [12]
Developmental delay driven by poverty and chronic stress must be distinguished from a specific neurodevelopmental disorder. Deprivation, inadequate nutrition, and a chaotic environment can each produce delay that improves when the material conditions improve — so a single assessment in the middle of a housing crisis undercalls the child's potential. [6] [1]
Behavioural difficulty and inattention driven by food insecurity and household stress overlap with anxiety disorders and ADHD, and the two are genuinely co-occurring. The useful question is not "trauma or ADHD?" but "what does this child need, in what order, for the true picture to emerge once the material conditions stabilise?" [7] [4]
When a child from a materially deprived household presents with a somatic complaint, hold two truths at once: organic disease is real and common (and is often missed because of the assumption it is "just social"), and toxic stress also manifests somatically. Avoid diagnostic overshadowing — never assume a symptom is social until you have excluded disease. [2] [1]
Iron-deficiency anaemia in a young child may be dietary — the classic consequence of poor-quality, food-insecure diets — but it may also reflect occult blood loss or malabsorption, so you investigate while you also screen for and address the food insecurity. [5] [12]
Frequent infections or delayed recovery may reflect the immune dysregulation of chronic stress and inadequate nutrition, but they may also signal an underlying immunodeficiency — so you assess on the merits and do not shortcut the workup. [7] [6]
Finally, a disclosure of neglect arising from, or compounded by, material deprivation shifts the frame from differential diagnosis to safeguarding. Material hardship is not neglect, but severe, persistent unmet need that harms a child may require child-protection involvement — and the decision is clinical and legal, made with the family and the local authority. [2] [14]
Clinical & Bedside Assessment
Open every encounter with a trauma-informed, destigmatising frame: greet the family, explain why you ask about hardship routinely (because you ask everyone), and make clear that the answers change the plan, not the respect you show. Ask about material hardship as you would ask about smoking or sleep — matter-of-factly, at every visit. [2] [11]
Before you screen, build the encounter that makes an honest answer possible. Offer privacy, use a trained interpreter where needed (never the child), and frame screening as universal — "we ask all families these questions because they matter for children's health" — which reduces stigma and improves disclosure. [10] [8]
[3] [10]Screen the broader social determinants with a validated instrument — tools such as the WE CARE, PRAPARE, or a locally validated social-needs questionnaire cover food, housing, income, utilities, transport, education, and interpersonal safety. A systematic review confirms that screening is feasible, acceptable, and identifies need that would otherwise be missed. [8] [9]
Take a full clinical history alongside the social screen, because the two inform each other: growth trajectory, feeding and dietary history, developmental milestones, school engagement, sleep, and any recent change in the household's circumstances. Plot growth and look for the centile crossing that flags faltering growth. [5] [12]
Examine thoroughly — growth, nutrition status, signs of micronutrient deficiency, dental caries, and any developmental finding — because organic disease and material deprivation coexist, and you must not shortcut the clinical assessment on the assumption that the cause is social. [2] [1]
Document the social findings in the clinical record with the same rigour you apply to organic findings: which domains of hardship are present, the severity, the family's priorities, and the referrals made. The social history is clinical data, and it travels with the child. [11] [10]
Investigations
The "investigation" step in this topic combines the clinical workup with the social-needs assessment, because both are needed to act safely. Measure growth and plot it; check a full blood count and iron studies where dietary inadequacy or faltering growth is present; and arrange lead testing where housing age or environmental exposure is plausible. [5] [12]
What the clinical and social assessment bundle typically covers
The clinical bundle addresses the common organic consequences of material deprivation: growth measurement and centile plotting, a full blood count and iron studies for anaemia, a developmental screen against age expectations, vision and hearing, and dental review. The social bundle uses the two-item Hunger Vital Sign plus a validated multi-domain social-needs instrument covering food, housing, income, utilities, transport and safety. Together they tell you both what the deprivation is doing and what the family needs.
Which screening instruments you choose should match the family and the setting. The Hunger Vital Sign is the minimum food-insecurity screen; a broader tool such as WE CARE or PRAPARE captures the wider social-needs landscape; and a structured developmental screen (such as the Ages and Stages Questionnaire or Parents' Evaluation of Developmental Status) should be added whenever delay is suspected, because deprivation-driven delay is eminently modifiable. [9] [8]
Iron studies matter disproportionately in this population. Food-insecure children are at elevated risk of iron-deficiency anaemia from poor-quality diets, and anaemia itself impairs development — so check, treat, and address the dietary cause simultaneously. [5] [12]
Growth data should be interpreted against the history of deprivation. Faltering growth may reflect food insecurity, organic disease, or both; rapid weight recovery after income or food support may reflect correction of deprivation — but the obesity risk that accompanies some food-insecure dietary patterns (energy-dense, nutrient-poor food) is also real, so you monitor the trajectory in both directions. [4] [5]
Management — Resuscitation
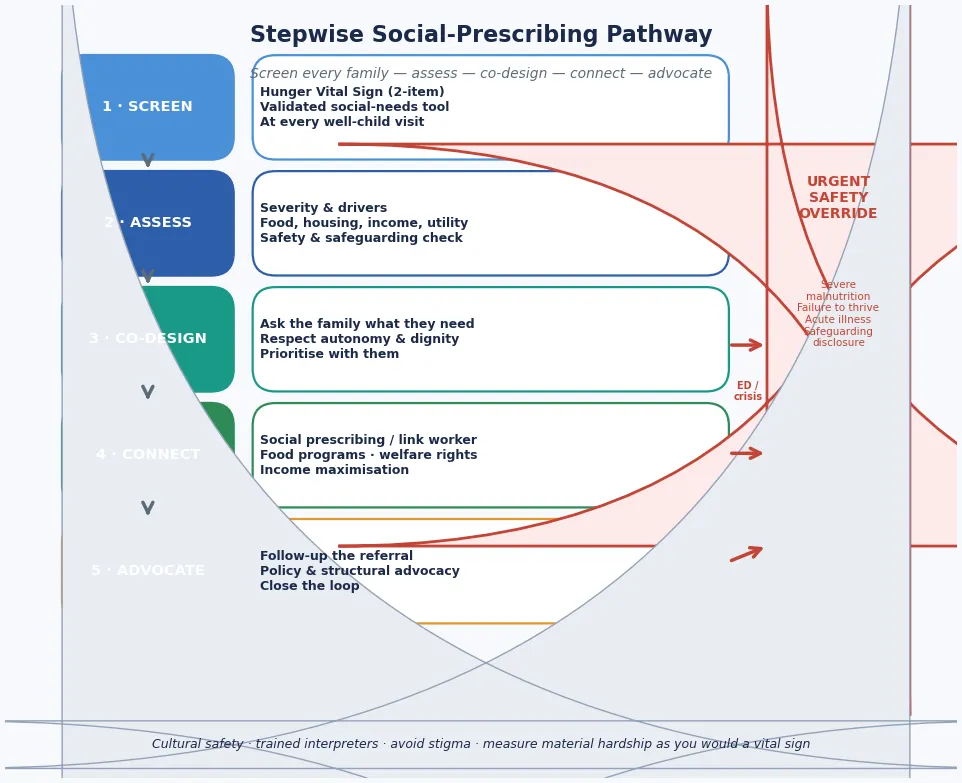
The "resuscitation" step in this topic is the immediate safety override: the things you cannot wait a routine referral to address. Severe malnutrition or failure to thrive, an acute serious illness layered on untreated hardship, a safeguarding disclosure, or a family in acute eviction or homelessness all exit the routine pathway and trigger same-day clinical, social-work, or crisis activation. [2] [5]
Treat the acute clinical problem first — severe anaemia, acute infection, dehydration, or failure to thrive — while you begin organising the social response, because the child will leave your encounter into a household that must be ready to continue. Do not attribute an acute presentation to poverty alone until you have excluded and treated organic disease. [1] [2]
For a family in acute housing crisis, activate social work and welfare referral the same day. Eviction and homelessness in families with very young children carry measurable and immediate harm, and the clinical team's advocacy can trigger emergency housing, welfare payments, or legal support that changes the trajectory within hours. [18] [14]
A safeguarding concern arising from, or compounded by, material deprivation requires the standard child-protection response: document, share the minimum necessary and lawful with child-protection services, and treat under best interests. Material hardship is not neglect, but severe unmet need that endangers a child crosses into safeguarding territory. [2] [13]
When a parent presents in mental-health crisis, intimate-partner violence, or substance use that destabilises the household, treat the crisis and involve the appropriate adult and family services — because the parent's capacity is part of the child's safety, and family-level support is part of paediatric care. [7] [2]
Management — Definitive & Stepwise
Definitive management is the social-prescribing pathway: screen, assess, co-design, connect, and follow up — delivered through the medical home and, where available, a dedicated link worker. The five-step model is the framework an examiner expects you to reproduce. [11] [17]
The five-step social-prescribing pathway
1 · Screen
Ask every family — Hunger Vital Sign plus a validated multi-domain social-needs tool — at every well-child visit.
2 · Assess
Clarify the severity and drivers of each domain (food, housing, income, utility, safety); check for organic consequences and safeguarding concerns.
3 · Co-design
Ask the family what they need and what they will accept; respect autonomy and dignity; prioritise with them, not for them.
4 · Connect
Social prescribing — active referral to food programs, welfare rights and income maximisation, housing and utility support, and community resources, often via a link worker.
5 · Follow up & advocate
Check the referral worked, measure whether hardship resolved, close the loop, and advocate at the policy level for the structural causes.
The evidence that this pathway works is now strong. A cluster randomised controlled trial of addressing social determinants at well-child visits showed reduced unmet social needs, and a systematic review of social-prescribing evidence supports its feasibility and acceptability across populations including children and families. [9] [17]
Deliver the pathway through a medical home: the same clinicians, routine screening at every visit, a named coordinator, and a warm handover to community resources. A link worker — where the model exists — bridges the clinic and the community, taking the referral, meeting the family, and following through, so that a positive screen does not become a dead-end referral. [16] [11]
The concrete, fixable targets are powerful. Food programs and produce prescriptions address food insecurity directly; income maximisation through welfare-rights support lifts household resources; housing and utility assistance stabilises the home; and medical-legal partnerships resolve the legal problems (eviction, benefit denial) that drive material hardship. Each is a treatment, not a referral to nowhere. [11] [14]
Address the organic consequences in parallel: treat iron-deficiency anaemia, support catch-up growth and nutrition, arrange developmental and educational support, and complete immunisation catch-up — because the clinical and social plans reinforce each other. [5] [12]
Advocate at the policy level as part of the management plan. Income supplements improve long-term child functioning, child health insurance improves access and outcomes, and structural interventions on housing, food policy, and income support are the most powerful levers a paediatrician can pull — through professional bodies, public statements, and local systems advocacy. [15] [13]
Specific Subtypes & Scenarios
Infants and toddlers in food-insecure households are the highest-stakes subgroup because brain growth is most rapid and most vulnerable. Prioritise growth measurement and centile plotting, feeding and dietary assessment, iron studies, developmental screen, and early connection to food and income support; reassess after the material conditions improve, because deprivation-driven faltering recovers when the dose is reduced. [5] [1]
School-age children with food insecurity present with a recognisable cluster: declining academic performance, social-skills deficits, behavioural difficulty, and weight-pattern disruption. A landmark cohort study established that food insecurity affects academic performance, weight gain, and social skills in school children, so address the food insecurity alongside the educational and developmental support. [4] [12]
A family facing eviction or homelessness needs same-day advocacy. Eviction in families with very young children is associated with increased hardship, food insecurity, and child and caregiver health problems — so activate social work, welfare, and legal support, and use medical-legal partnership where it exists to prevent or delay the eviction. [18] [14]
Children with chronic illness or disability in materially deprived households carry compounded risk: the cost of managing a chronic condition deepens poverty, and poverty worsens the condition. Social prescribing for children with neurodisability and their families is feasible and valued, so build the social-needs assessment into the chronic-disease plan from the outset. [16] [12]
An Indigenous or minority family requires culturally safe care: respect for family and community, acknowledgement of the structural and historical drivers of inequity, and locally appropriate services including Aboriginal community-controlled organisations where available. Racism is itself a health exposure, and culturally unsafe screening compounds harm. [2] [13]
A migrant, refugee or asylum-seeking family brings layered material, language, and legal precarity on top of food and housing insecurity. Use trained interpreters, screen for the social determinants with cultural adaptation, address missed preventive care, and connect to settlement and welfare services. [2] [10]
A rural or remote family faces fragmented service access, transport costs, and digital-exclusion barriers to social prescribing. Create deliberate pathways including telehealth-delivered screening and referral, and advocate for the rural services that make the pathway real. [2] [13]
Complications & Pitfalls
The most common pitfall is failing to screen at all, on the assumption that the family "would tell you" if they were struggling. They will not, reliably, because hardship carries shame and because the parent may not connect the child's symptom to the household's finances. Universal, routine screening is the standard, and it catches the families who would otherwise be missed. [10] [8]
Screening without action is the second pitfall. Asking about hardship and then doing nothing is worse than not asking, because it raises a need and then abandons it. Only screen if you have — or can build — the referral pathway to respond, and document what you offered. [9] [11]
Diagnostic overshadowing — attributing a child's symptoms to "just poverty" and missing organic disease — is a well-described harm. Faltering growth, behavioural difficulty, and somatic complaints in a materially deprived child may be driven by deprivation, but they may also be organic, and you must investigate both. [1] [5]
[2] [12]Stigmatising the family — through judgemental language, a punitive tone, or a frame that implies the hardship is the parent's fault — breaches trust and suppresses future disclosure. Screen routinely and matter-of-factly, use neutral language, and treat the family as partners in solving a structural problem. [2] [11]
Failing to follow up the referral is the final common pitfall. A positive screen that leads to a referral no one checks is a dead end; close the loop by asking, at the next visit, whether the family connected with the resource and whether the hardship resolved, and measure whether your pathway works. [9] [17]
Prognosis & Disposition
Prognosis here means the trajectory of health, development, and household stability — and it is more modifiable than it looks. Early identification, active social prescribing, and structural advocacy all move the trajectory in the child's favour, and the evidence for reversibility is the most encouraging part of this topic. [15] [12]
Routine disposition is a screened family with an active social prescription, a connected community resource, and a planned follow-up to confirm the hardship was addressed. The child returns to routine well-child care with the social determinant treated alongside the clinical plan. [11] [2]
Early-review disposition is a newly positive screen, a family in transition (job loss, housing move), or a child whose growth or development is faltering — bring them back in weeks, not months, to confirm the referral worked and the trajectory is correcting. [5] [12]
Urgent disposition is severe malnutrition or failure to thrive, an acute serious illness, acute eviction or homelessness, or a safeguarding concern — use ED, social-work, crisis-housing, or child-protection pathways the same day. [18] [2]
Safety-net explicitly: who to call tonight, where the family can get food or emergency housing today, and when to come back sooner. Close the loop after welfare, food-program, housing, or safeguarding involvement. [11] [14]
Over time, income supplements and structural interventions improve long-term functioning — children whose families received income supplements show better adult outcomes — which is the evidence that poverty is treatable and that the paediatrician's role extends from the screen to the policy. [15] [13]
Special Populations
Indigenous children (Aboriginal, Torres Strait Islander, Māori, First Nations). Over-represented among children in poverty, a legacy rooted in colonisation and systemic disadvantage; cultural safety, respect for family and community, and locally appropriate services (including Aboriginal community-controlled organisations) are essential. Racism is a health exposure. [2] [13]
Migrant, refugee and asylum-seeking children. Layered material, language and legal precarity; use trained interpreters, screen with cultural adaptation, address missed preventive care, and connect to settlement and welfare services. [2] [10]
Children with chronic illness, disability or neurodiversity. Compounded risk through the cost of managing a chronic condition; build the social-needs assessment into the chronic-disease plan, and use social prescribing to connect families to support. [16] [12]
Infants and toddlers. The developmental and nutritional stakes are highest here, so prioritise growth, feeding and dietary assessment, iron studies, developmental screen, and early connection to food and income support. [5] [1]
Children in out-of-home care. Already carrying the burden of adversity, these children are disproportionately affected by material hardship; coordinate the social-needs screen with the care plan and consent authority. [2] [11]
Rural and remote families. Fragmented service access, transport costs, and digital exclusion threaten the social-prescribing pathway; create deliberate telehealth-delivered pathways and advocate for rural services. [2] [13]
Evidence, Guidelines & Regional Differences
Poverty as the most prevalent paediatric risk. Schickedanz, Dreyer and Halfon's 2015 review frames childhood poverty as the most prevalent risk to child health, and Dreyer's 2023 review on achieving child health equity sets the policy solutions — together they anchor the fellowship-level answer. [2] [13]
The developing brain. Luby's 2015 study — "Poverty's Most Insidious Damage: The Developing Brain" — demonstrates that poverty shapes the brain, and Hackman and Farah's 2009 review establishes the neuroscientific basis linking socioeconomic status to the developing brain. Shonkoff's 2012 report on the lifelong effects of early adversity and toxic stress provides the mechanism. [1] [6] [7]
Food insecurity, quantified. The Children's HealthWatch group established the two-item Hunger Vital Sign (Hager, 2010), the relationship between food insecurity and health and development in children under four (Drennen, 2019), and the effects on school children's academic performance, weight gain and social skills (Jyoti, 2005) — the evidence base for universal food-insecurity screening. [3] [5] [4]
Screening and social prescribing evidence. Sokol's 2019 systematic review confirms screening for social determinants is feasible and acceptable. Garg's 2015 cluster RCT shows that addressing social determinants at well-child visits reduces unmet social needs, and his 2019 survey describes how US paediatricians screen and refer. His 2021 review with colleagues lays out the clinical approaches to reducing material hardship. [8] [9] [10] [11]
Copeland et al, 2022 — long-term outcomes of childhood family income supplements
Longitudinal analysis of a natural experiment
Population: Children whose families received income supplements (casino payments) versus those who did not
Key finding
Family income supplements during childhood were associated with improved adult functioning, supporting the conclusion that poverty is modifiable and that income intervention changes long-term developmental and mental-health trajectories.
Practice change
Treat material hardship as a modifiable risk factor; advocate for income-support and anti-poverty policies as part of paediatric care.
Housing and eviction. Green, Bovell-Ammon and Sandel's 2021 review frames housing and neighbourhoods as root causes of child poverty, and Cutts and colleagues' 2022 study shows that eviction in families with very young children is associated with increased hardship, food insecurity and health problems — the evidence for treating housing instability as a clinical vital sign. [14] [18]
Social prescribing for children. Bickerdike's 2017 systematic review established the evidence base for social prescribing broadly, and Gordon and colleagues' 2023 systematic review examined social prescribing for children and young people with neurodisability initiated in a hospital setting, demonstrating feasibility and family acceptability. [17] [16]
ANZ: each state and territory governs income support, housing, and welfare services; Aboriginal community-controlled services and cultural-safety requirements apply. RCH Melbourne provides clinical guidance on the social determinants of child health. UK: NICE guidance on social prescribing and community-based support frames the link-worker model; NHS England's universal personalised care programme embeds social prescribing in primary care. The Marmot review frames child health inequalities. US: the AAP guidance on poverty and child health sets the standard for screening; Medicaid, SNAP, and WIC frame food and health-care support, and medical-legal partnerships address the legal drivers of material hardship. Canada: provincial social-assistance and child-benefit programmes frame income support; Indigenous child and family services and Jordan's Principle apply for First Nations, Inuit and Métis children.
State the principle and check local pathways. Do not invent a universal income line, a universal food-assistance programme name, or a universal link-worker model — they vary by jurisdiction, and the local welfare, housing and community-service architecture governs what you can actually connect a family to. [2] [11]
Exam Pearls
[2] [1] [11]- Open every answer with poverty as the most prevalent paediatric risk and the dose-response toxic-stress mechanism, then the five-step social-prescribing pathway. [2] [1]
- Always screen every family routinely — the Hunger Vital Sign and a validated social-needs tool — because hardship is common, fluctuating, and invisible. [3] [10]
- Name the high-prevalence harms: faltering growth, iron-deficiency anaemia, developmental delay, behavioural difficulty, and educational underachievement. [5] [4]
- Social prescribing is the operational tool — screen, assess, co-design, connect, follow up — and a link worker bridges the clinic and the community. [11] [17]
- Avoid diagnostic overshadowing — never assume a sign is "just social" until you have excluded and treated organic disease. [1] [2]
- The burden is reversible: income supplements improve long-term functioning, which is why advocacy is part of the plan. [15] [13]
References
- [1]Luby JL Poverty's Most Insidious Damage: The Developing Brain JAMA Pediatrics, 2015.PMID 26191940
- [2]Schickedanz A, Dreyer BP, Halfon N Childhood Poverty: Understanding and Preventing the Adverse Impacts of a Most-Prevalent Risk to Pediatric Health and Well-Being Pediatric Clinics of North America, 2015.PMID 26318943
- [3]Hager ER, Quigg AM, Black MM, Coleman SM, Heeren T, Rose-Jacobs R, Cook JT, de Cuba SA, Casey PH, Chilton M, Sites EW, Cutts DB, Meyers AF, Frank DA Development and Validity of a 2-Item Screen to Identify Families at Risk for Food Insecurity Pediatrics, 2010.PMID 20595453
- [4]Jyoti DF, Frongillo EA, Jones SJ Food Insecurity Affects School Children's Academic Performance, Weight Gain, and Social Skills Journal of Nutrition, 2005.PMID 16317128
- [5]Drennen CR, Coleman SM, Ettinger de Cuba S, Frank DA, Chilton M, Cook JT, Cutts DB, Heeren T, Casey PH, Black MM Food Insecurity, Health, and Development in Children Under Age Four Years Pediatrics, 2019.PMID 31501233
- [6]Hackman DA, Farah MJ Socioeconomic Status and the Developing Brain Trends in Cognitive Sciences, 2009.PMID 19135405
- [7]Shonkoff JP, Garner AS, Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, Section on Developmental and Behavioral Pediatrics The Lifelong Effects of Early Childhood Adversity and Toxic Stress Pediatrics, 2012.PMID 22201156
- [8]Sokol R, Austin A, Chandler C, Byrum E, Bousquette J, Lancaster C, Shah S, Nakitsas B, Noppert G, Mendoza JA Screening Children for Social Determinants of Health: A Systematic Review Pediatrics, 2019.PMID 31548335
- [9]Garg A, Toy S, Tripodis Y, Silverstein M, Freeman E Addressing Social Determinants of Health at Well Child Care Visits: A Cluster RCT Pediatrics, 2015.PMID 25560448
- [10]Garg A, Cull W, Olson L, Boyd AF, Federico SG, Dreyer B, Racine AD Screening and Referral for Low-Income Families' Social Determinants of Health by US Pediatricians Academic Pediatrics, 2019.PMID 31129128
- [11]Garg A, Brochier A, Messmer E, Fiori KP Clinical Approaches to Reducing Material Hardship Due to Poverty: Social Risks/Needs Identification and Interventions Academic Pediatrics, 2021.PMID 34740423
- [12]Gross RS, Messito MJ, Klass P, Canfield CF, Yin HS, Morris PA Integrating Health Care Strategies to Prevent Poverty-Related Disparities in Development and Growth: Addressing Core Outcomes of Early Childhood Academic Pediatrics, 2021.PMID 34740424
- [13]Dreyer BP Achieving Child Health Equity: Policy Solutions Pediatric Clinics of North America, 2023.PMID 37422319
- [14]Green KA, Bovell-Ammon A, Sandel M Housing and Neighborhoods as Root Causes of Child Poverty Academic Pediatrics, 2021.PMID 34740428
- [15]Copeland WE, Tong G, Gaydosh L, Hill SN, Godwin J, Shanahan L, Costello EJ Long-term Outcomes of Childhood Family Income Supplements on Adult Functioning JAMA Pediatrics, 2022.PMID 35994270
- [16]Gordon K, Gordon L, Basu AP Social Prescribing for Children and Young People with Neurodisability and Their Families Initiated in a Hospital Setting: A Systematic Review BMJ Open, 2023.PMID 38135327
- [17]Bickerdike L, Booth A, Wilson PM, Farley K, Wright K Social Prescribing: Less Rhetoric and More Reality. A Systematic Review of the Evidence BMJ Open, 2017.PMID 28389486
- [18]Cutts DB, Ettinger de Cuba S, Bovell-Ammon A, Wellington C, Coleman SM, Frank DA, Sandel M, Heeren T, Chilton M, Hessler K, Meyers A, Casey P Eviction and Household Health and Hardships in Families With Very Young Children Pediatrics, 2022.PMID 36120757