Paeds · child-safety-and-social-paediatrics
Prevention of child maltreatment and family support
Also known as Child maltreatment prevention · Preventing child abuse and neglect · Family support programmes · Strengthening families and protective factors · Upstream child protection
Fellowship topic on preventing child maltreatment and supporting families: the public-health frame of primary, secondary and tertiary prevention; the WHO INSPIRE seven strategies and the Strengthening Families protective factors; why prevention works biologically through the toxic-stress cascade and the buffering adult; risk and protective factors and the prevention paradox; the prevention opportunity at every child contact; the stepped universal-to-intensive pathway of evidence-based interventions (Nurse-Family Partnership, Triple P, school-based sexual-abuse prevention, economic strengthening); recurrence prevention after a sentinel injury or substantiated harm; Indigenous, rural, refugee, disability and socioeconomic-disadvantage prevention; what does not work and the controversies; and ANZ/UK/US/Canada policy structure.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
I.N.S.P.I.R.E. — the seven strategies WHO packages into one prevention framework
Overview & Definition
Picture a six-week-old baby at a routine immunisation visit. The mother is tired, the partner left last month, the rent rose again, and there is no food in the cupboard. There is no injury here, no disclosure, nothing to report. There is, however, a window — the kind of window that, used well, means the family never returns with a sentinel injury or a child-protection referral. Prevention of child maltreatment is the discipline of using that window. [7] [1]
Prevention is deliberate action to stop maltreatment before it occurs, to find and support families at risk early, and to reduce recurrence and long-term harm when maltreatment has already happened. The central insight is that maltreatment is common, mostly invisible to child-protection agencies, and shaped by modifiable factors — parental stress, social isolation, material hardship, and the absence of a buffering adult. Waiting to act until an injury appears is to act late. [7] [6]
The clinician's role is narrower than the government's but more intimate. A paediatrician sees almost every child in the first years of life through the well-child schedule, immunisations, and acute visits. Each contact is a prevention opportunity: to build on family strengths, to screen for stressors, to offer evidence-based support, and to escalate to protection only when a reasonable belief of current significant harm appears. [1] [3]
This page owns the prevention and family-support framework. It does not rebuild the recognition-to-response bundle, the mandatory-reporting thresholds, or the workup for each abuse subtype — those live in the linked leaves. Here the question is what the clinician does before harm, and after recurrence, to make harm less likely. [1] [2]
Classification
Sort prevention the way a public-health physician sorts it — by when you act relative to harm. Primary prevention reaches the whole population before maltreatment occurs: universal parenting support, school-based education, and the laws and economic policies that shape how families live. Secondary prevention targets families with identified risk factors and intervenes early, most often through structured home visiting from pregnancy or infancy. Tertiary prevention acts after maltreatment has happened, to prevent recurrence, reduce long-term harm, and restore the buffering relationship. [1] [1]
The World Health Organization packages the strongest evidence into seven complementary strategies, known by the acronym INSPIRE: implementation and enforcement of laws, norms and values, safe environments, parent and caregiver support, income and economic strengthening, response and support services, and education and life skills. These are not a menu of alternatives; they are meant to run together, because maltreatment has many drivers and no single strategy addresses them all. [1] [7]
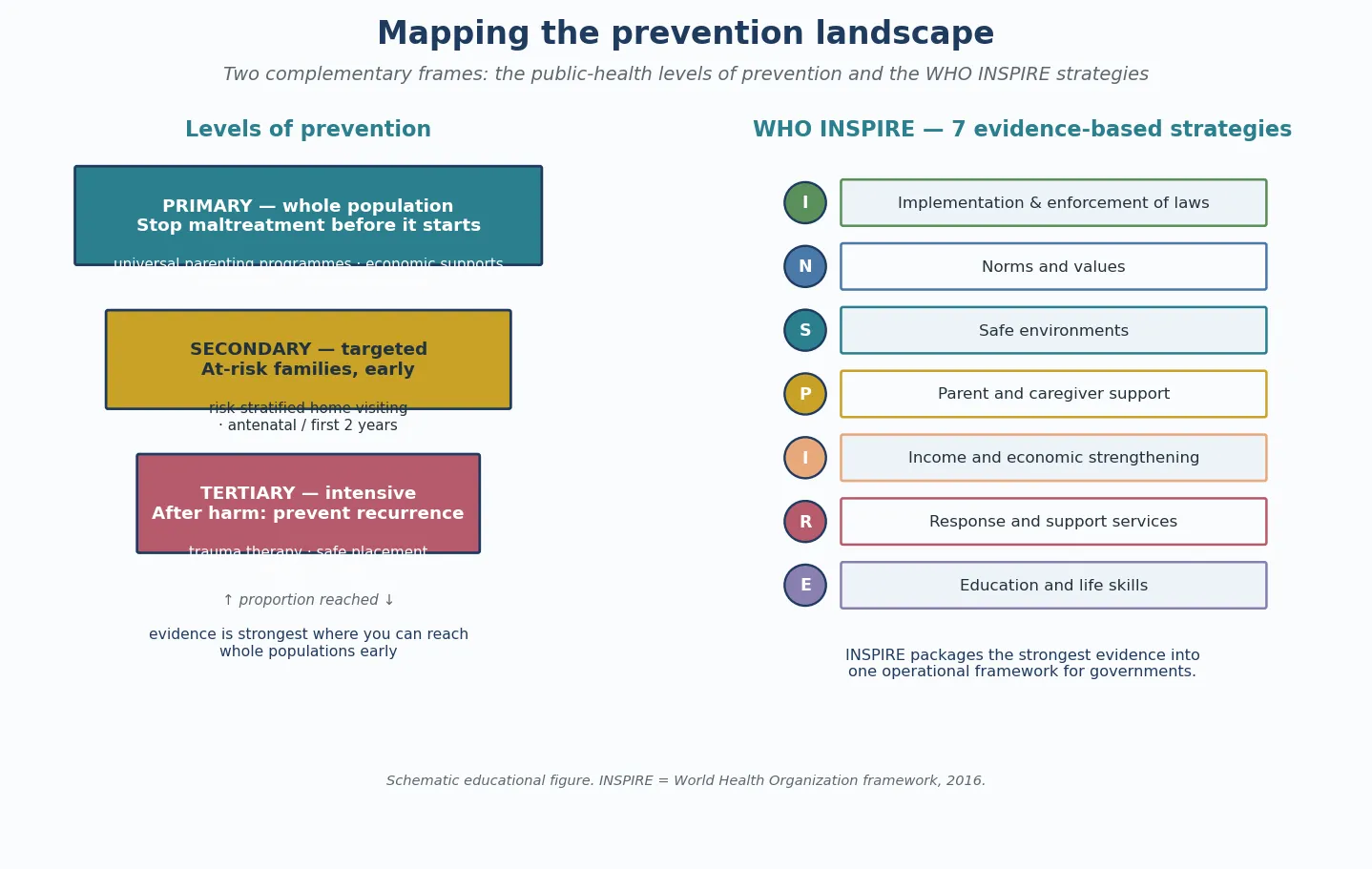
A second frame, used widely in family-support practice, sorts by the protective factors that prevention aims to build: parental resilience, social connections, concrete support in times of need, knowledge of parenting and child development, and the social-emotional competence of children. These five factors are the strengths-based counterpart to the risk-factor list, and a clinician can assess and reinforce them at any visit. [1] [9]
The deepest classification question is practical: which level of support does this family need? A family doing well needs universal support; a family under stress needs targeted help; a family in which harm has occurred needs intensive, coordinated input. The sections below build that stepped pathway. [1] [3]
Epidemiology & Risk Factors
How much maltreatment is there, and where does prevention reach? Two answers come back, and the gap between them is the central epidemiological fact for prevention. Official agency-substantiated rates — what child-protection systems record — markedly under-estimate true prevalence, because most maltreatment is never reported or substantiated. Self-report surveys of adults recalling childhood show that maltreatment is several-fold more common than agency data suggest. [7] [11]
The global burden is large. A WHO systematic review estimated that roughly one billion children aged two to seventeen years experienced past-year violence, and high-income-country data place physical abuse and neglect among the most common adverse exposures of childhood. National survey data show that exposure to violence, crime and abuse is widespread, and trends over the 2000s showed declines in several forms, coinciding with prevention and policy effort — though the burden remains far higher than agency data imply. [7] [11]
The prevention paradox follows directly. Because most maltreated children belong to the large group of families with modest risk, a strategy aimed only at high-risk families cannot by itself achieve large population reductions. Effective prevention combines a wide universal base — reaching the many — with a targeted layer for the fewer families with identified risk, and an intensive layer for the still fewer in whom harm has occurred. [3] [1]
The risk factors prevention targets are modifiable and cluster at three levels. Child factors include prematurity, infancy, chronic illness, disability, and behaviour that challenges caregivers. Parent and family factors include parental mental illness, substance use, intimate-partner violence, social isolation, a caregiver's own history of childhood adversity, and young or single parenthood. Community factors include poverty, housing and food insecurity, neighbourhood violence, and poor access to support. [7] [4]
None of these factors is diagnostic. Most families with risk factors never maltreat their child, and conflating disadvantage with risk is itself a harm. The factors mark where support should go, and they pair with protective factors — a stable adult, social connections, parental resilience, concrete material support, and community safety — that prevention is designed to build. [7] [9]
Pathophysiology
Why does prevention work — and why does a stable adult matter so much? The answer is the biology of toxic stress, and it is the mechanism that turns an epidemiological observation into a clinical rationale. Maltreatment harms a child not only through the acute injury but through a chronic, biological cascade that unfolds across the life course. [5] [4]
A child's stress response is healthy when it is brief and buffered. When a threat passes and a responsive adult comforts the child, the cortisol and adrenergic surge settles and the brain records a safely mastered challenge. Maltreatment removes the buffer: the threat comes from within the caregiving relationship, so the stress response stays activated for weeks, months and years. That sustained activation is toxic stress. It recalibrates the developing hypothalamic-pituitary-adrenal axis, dysregulates the immune system, and alters the architecture of the brain — especially the limbic and prefrontal circuits that govern emotion, attention and impulse. [5] [6]
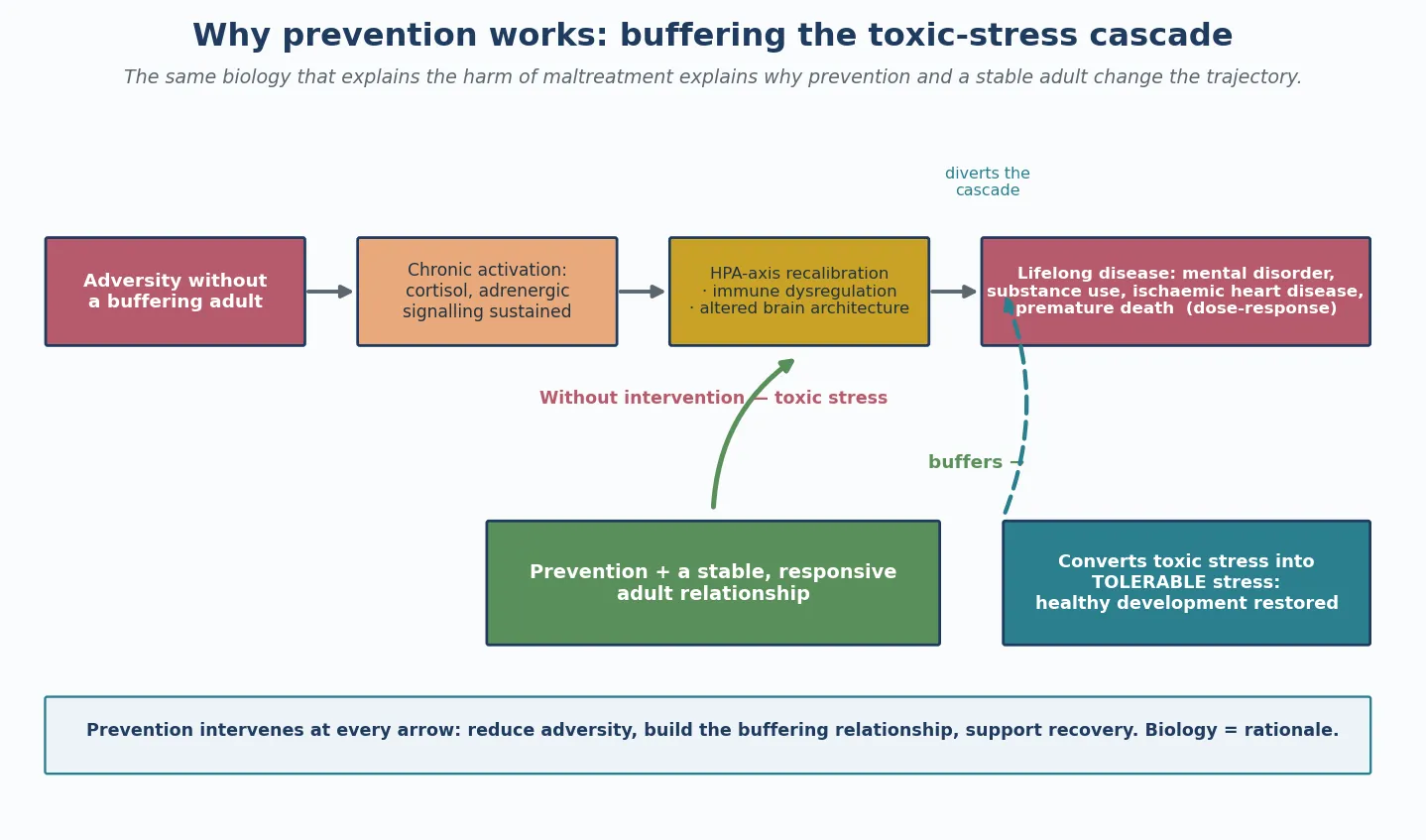
The same cascade produces the adult disease associations that make the evidence so consequential. A meta-analysis of the long-term health consequences of abuse and neglect found elevated risks of mental disorder, substance use, self-harm and physical disease. The Adverse Childhood Experiences study showed a graded relationship between the ACE score and the leading causes of adult death, including ischaemic heart disease. The relationship is dose-response: more cumulative adversity, more downstream disease. [6] [5]
The therapeutic implication is precise. A stable, responsive adult relationship converts toxic stress into tolerable stress, so the buffering adult is both the strongest risk factor for harm (when absent) and the strongest mechanism of recovery (when present). Prevention therefore aims to build, protect and restore that relationship — through universal parenting support, through targeted home visiting that strengthens the parent-infant relationship, and through trauma-focused therapy after harm. [5] [4]
Each level of prevention intervenes at a different arrow of the cascade. Primary prevention reduces the adversity a family faces (economic support, alcohol policy, safe environments). Secondary prevention builds the buffering relationship in at-risk families before harm occurs. Tertiary prevention restores regulation and prevents re-injury after harm. The biology of harm and the biology of recovery are the same biology. [5] [2]
Clinical Presentation
For a prevention topic, presentation is not an injury — it is a recognition that a family would benefit from support. The trigger is the contact itself, and the contact exists at every point the child is seen: antenatal and postnatal care, the well-child schedule, immunisation visits, school health, and acute presentations to the ward or emergency department. [1] [3]
The circumstances that signal a need for targeted (secondary) prevention are the modifiable risk factors above. A first pregnancy with disadvantage, parental mental illness or substance use, intimate-partner violence, financial strain, housing instability, social isolation, and a caregiver's own maltreatment history each raise the case for offering structured support rather than universal contact alone. These are not grounds for a report; they are grounds for a warm hand-off. [7] [8]
Child markers raise the intensity of prevention further. Prematurity, disability or chronic illness, faltering growth, a developmental concern, a sentinel injury, and being in or entering out-of-home care each indicate a child whose family needs more than the universal offer. These markers prompt a structured needs assessment and, where indicated, a referral to evidence-based support. [7] [1]
The absence of overt risk does not make prevention unnecessary. Because most maltreatment sits among the many modest-risk families, universal programmes — population-level parenting support, school-based education, and economic policy — reach the group where most harm actually occurs. A clinician who offers support only to obviously high-risk families misses the majority. [3] [1]
Differential Diagnosis
The "differential" for a prevention topic is the decision about which level of support a family needs, and it guards two errors: leaving a family unsupported, and over-surveilling a family on the basis of bias. The aim is to match the intensity of support to need, without stigma and without missing current harm. [1] [7]
First, separate a family who will benefit from universal prevention from one who needs targeted secondary support, and from one who needs intensive tertiary input. A family doing well receives the universal offer; a family with identified risk factors receives targeted support; a family in which harm has occurred receives coordinated, intensive input. The decision turns on the risk and protective factor assessment, not on a single screening score. [1] [3]
Second, separate a family under stress who needs support from a family where there is reasonable belief of significant harm. The first routes to family support; the second switches immediately to the recognition-to-response bundle and a report. Holding this boundary keeps the supportive stance safe — when current harm is suspected, safety overrides the supportive frame. [7] [1]
Third, separate the modifiable drivers, because each routes to a different intervention. Poverty, housing and food insecurity route to material support and social prescribing. Parental mental illness, substance use and intimate-partner violence route to clinical treatment and family-violence services. Confusing them — offering a parenting programme to a family without food — feels like blame and does not fix the cause. [1] [9]
Fourth, guard against the bias that turns prevention into surveillance. Socioeconomic disadvantage, Indigenous status and single parenthood are not themselves markers of maltreatment risk; conflating them causes harm, erodes trust, and drives inequity. Assess needs, not stereotypes, and use objective, validated assessment rather than impression. [7] [1]
Clinical & Bedside Assessment
The prevention assessment is trauma-informed, strengths-based, and framed as support rather than surveillance. At every contact, take a family history that asks about supports and stressors and protective factors — not only risk — and explain that the questions are there to help, not to judge. The stance itself determines whether the family returns. [1] [9]
Assess the five Strengthening Families protective factors explicitly: parental resilience, social connections, concrete support in times of need, knowledge of parenting and child development, and the social-emotional competence of the child. Their presence is as important as the absence of risk, because building them is what prevention does. A family with strong social connections and material stability is already partly protected. [1] [9]
Screen for the modifiable drivers of maltreatment using validated, locally approved instruments: parental depression, intimate-partner violence, substance use, and social needs such as food and housing insecurity. Apply these universally and without stigma, and have a warm hand-off pathway ready for every positive screen, because screening without a response damages trust and changes nothing. [7] [8]
Assess child growth, development and emotional state at routine visits, because faltering in these domains is often the first signal that a family needs more support. Coordinate with primary care, early-childhood services and education, so that the assessment is continuous rather than a snapshot that depends on a single clinician. [7] [1]
Investigations
There is no blood test or scan for prevention. The "workup" is a structured needs and risk assessment that decides the intensity of support a family should be offered, and it sits alongside a documented family-needs plan that records strengths, needs, agreed supports and a review date. [1] [8]
Use validated, locally approved screening instruments for parental depression, intimate-partner violence, substance use and social needs. Apply them universally and without stigma, and connect every positive screen to a defined response pathway — a named person or service the family can reach. Screening that does not lead to support damages trust and wastes the opportunity. [7] [9]
Use routine developmental and psychosocial surveillance as the ongoing monitor. Growth, development, behaviour and school engagement tell you whether the support a family receives is enough, or whether prevention needs to escalate. A child whose growth or development falters despite support prompts a reassessment of the whole plan. [7] [1]
Do not use the ACE score as an individual diagnostic or triage test. Its value is epidemiological — it established the dose-response between cumulative adversity and adult disease — and at the bedside a numerical score risks labelling and stigma without changing what you offer. Ask about adversity to understand and support; do not score it. [5] [4]
Management — Resuscitation
The prevention stance is supportive — until it surfaces a reasonable belief of current significant harm, at which point safety overrides the supportive frame. If a contact raises concern that a child is being harmed now, switch immediately to the recognition-to-response bundle: stabilise, examine, document, and report. Prevention never asks you to wait when there is current danger. [7] [1]
Address acute parental crisis that threatens the child today. Active suicidal ideation, acute intimate-partner violence, acute intoxication, or an unsafe home need crisis services and a safety net before the family leaves. Link the caregiver to mental-health, family-violence or addiction services, and arrange follow-up that is real, not token. [7] [2]
Meet concrete material need that is driving crisis today. Food, formula, safe sleeping equipment and housing are both risk factors and immediate harms, and a family without them cannot be expected to engage with a parenting programme. Social work and local support services can meet the need the same day in many cases. [1] [1]
Engage the non-offending or primary caregiver as the central partner, because the buffering-adult mechanism runs through them. Document the prevention encounter — the risk and protective assessment, the supports offered, and the follow-up plan — so continuity is not lost between clinicians and services, and so the next contact begins where this one ended. [2] [12]
Management — Definitive & Stepwise
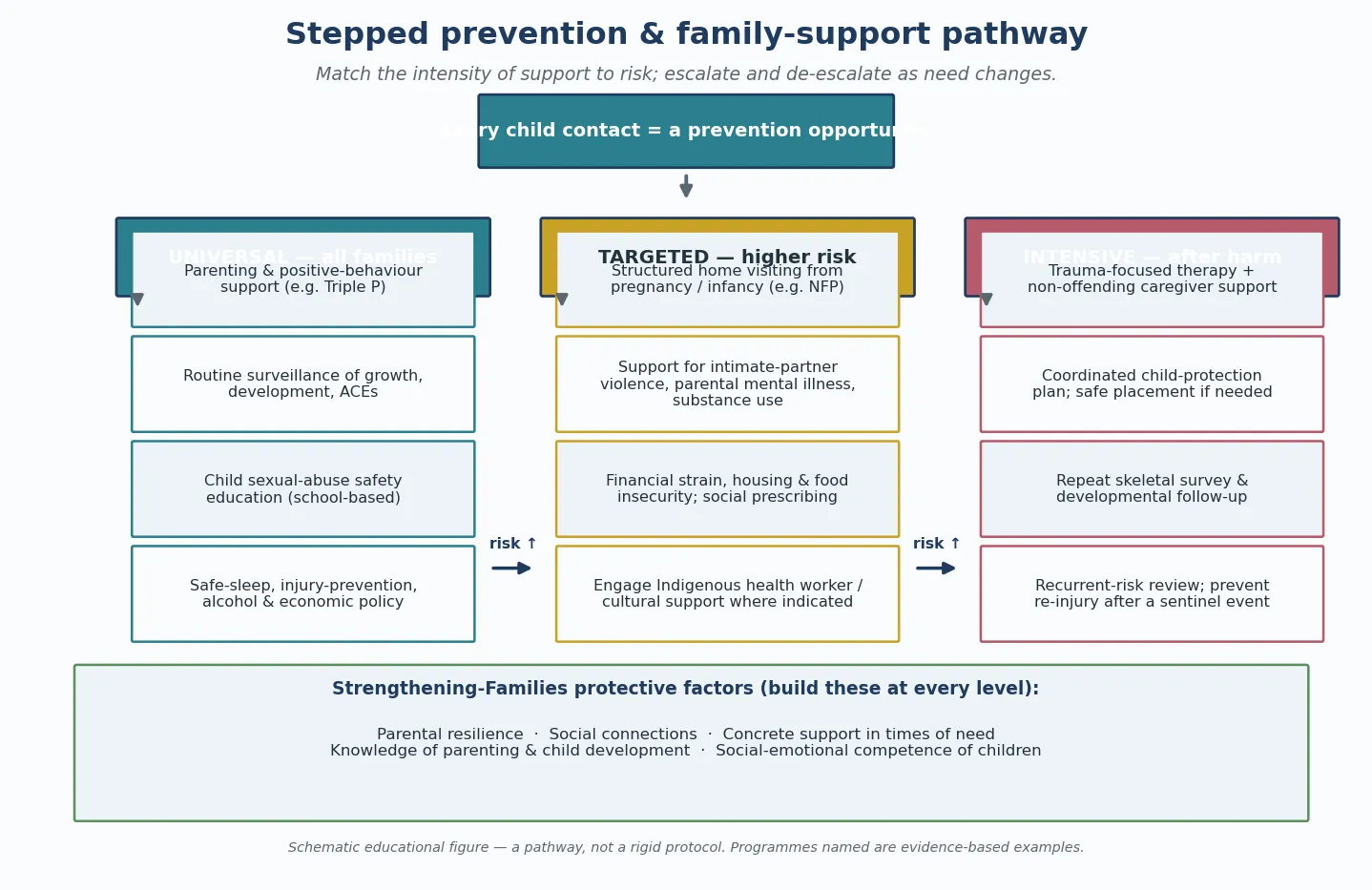
Definitive prevention is a stepped pathway matched to risk, with universal support for all families, targeted support for at-risk families, and intensive support after harm. Escalate and de-escalate as need changes, and couple every level with the response services that catch the families prevention does not reach. [1] [1]
The stepped prevention pathway
Universal: offer evidence-based parenting and positive-behaviour support at population scale — the Triple P population trial reduced substantiated maltreatment and out-of-home entries when delivered at scale.
Universal: deliver school-based child sexual abuse prevention education — a Cochrane review found it improves children's knowledge and self-protective skills without increasing anxiety.
Universal: address structural drivers through income and economic strengthening, housing and food support, and alcohol and safe-environment policy.
Targeted: offer structured home visiting from pregnancy or infancy for at-risk families — the Nurse-Family Partnership showed long-term reductions in verified maltreatment and child injuries.
Targeted: treat parental mental illness, substance use and intimate-partner violence, and meet concrete material need, because these are the modifiable drivers.
Intensive: after harm, deliver trauma-focused therapy, support the non-offending caregiver, build a written safety plan, and arrange fixed follow-up and recurrence-prevention review.
At the universal level, the strongest population evidence comes from the Triple P system. In a population-based trial, delivering Triple P at a county-wide scale was associated with reductions in substantiated maltreatment and out-of-home-care entries, compared with counties without it. The point is reach: a programme that works only in a clinic reaches few families, while one delivered at scale shifts the whole curve. [3] [9]
A meta-analysis of parent-training components shows what makes parenting programmes work: teaching positive parent-child interaction, giving parents opportunities to practise the skills with their child, and teaching consistent discipline including time-out. Programmes that include these components have larger effects, and that detail is what an examiner rewards. [9] [1]
At the targeted level, the best-evidenced model is the Nurse-Family Partnership: structured nurse home visiting beginning in pregnancy for first-time mothers in circumstances of disadvantage. In a fifteen-year follow-up of the original randomised trial, families who received the programme had fewer verified maltreatment reports and fewer child injuries than controls, alongside long-term maternal life-course benefit. [2] [12]
A meta-analysis of home-visiting components confirms the principle: outcomes are better when programmes are well-specified, delivered as designed, and sustained through the period of highest risk. Home visiting is not a generic service; it is a programme with a model, a dose, and a measured effect. [8] [2]
School-based child sexual abuse prevention education is delivered as a universal education-and-life-skills intervention. A Cochrane review found that such programmes improve children's knowledge of sexual abuse and their self-protection skills, and do not increase anxiety — a frequent concern of parents and schools. The effect is on knowledge and disclosure skills, and the programme is part of a wider safeguarding system rather than a stand-alone shield. [10] [1]
Income and economic strengthening addresses the structural drivers that sit upstream of individual behaviour. Financial supports, housing and food security, and alcohol policy change the conditions in which parenting happens, and they pair with parent-support and response services to form a complete prevention package. Offering a parenting programme to a family without food does not fix the cause. [1] [1]
At the intensive level, after a sentinel injury or substantiated harm, tertiary prevention prevents recurrence — which may otherwise be fatal. Deliver trauma-focused therapy for the child and support for the non-offending caregiver, build a written safety plan specifying who the child lives with and the supervision arrangements, arrange supervised contact where needed, and set a fixed follow-up and recurrence-prevention review date. [7] [12]
Specific Subtypes & Scenarios
A first-time mother in disadvantage, seen antenatally. This is the classic indication for structured nurse home visiting. The Nurse-Family Partnership begins in pregnancy and continues through the child's second year, and its long-term randomised-trial evidence — reduced verified maltreatment, fewer child injuries, and maternal life-course benefit — makes it the best-evidenced targeted home-visiting model. Offer it early; the programme's effect depends on starting in pregnancy. [2] [12]
A population offered parenting support at scale. The Triple P population trial showed that delivering a parenting programme across a whole population reduced substantiated maltreatment and out-of-home-care entries. The examiner-rewarded point is reach: the same programme that helps an individual family in a clinic reduces harm at population scale when delivered widely. [3] [9]
Children receiving school-based sexual abuse prevention education. A Cochrane review found these programmes improve children's knowledge and self-protection skills without raising anxiety. They are a universal education-and-life-skills intervention, part of a wider system that includes disclosure pathways and trained responders. [10] [1]
After a sentinel injury or substantiated harm (tertiary prevention). Re-injury after a sentinel event may be fatal, so recurrence prevention is not optional. Deliver trauma-focused therapy, support the non-offending caregiver, build a written safety plan, arrange supervised contact where needed, set a fixed follow-up date, and complete a repeat skeletal survey where indicated. The plan is shared and continuous. [7] [12]
A child in or entering out-of-home care. Every contact is a prevention opportunity. Children in care carry high baseline adversity and cumulative placement risk, so screen actively for unmet health and developmental need, coordinate health assessments across placements, and treat each contact as a chance to strengthen the buffering relationship. [7] [1]
An Indigenous child (Aboriginal and Torres Strait Islander, Maori). Prevention must be culturally safe, community-led, and grounded in addressing structural determinants and historical context. Engage Indigenous health workers and family, hold the same objective, evidence-based standards, and do not conflate disadvantage with risk. Imposed, non-cultural prevention re-creates the harm it aims to prevent. [7] [1]
Complications & Pitfalls
Over-surveillance driven by bias is the most common harm a prevention stance causes. Treating poverty, Indigenous status or single parenthood as evidence of maltreatment risk erodes trust, drives families away from services, and produces inequity. Assess needs, not stereotypes, and use objective, validated assessment rather than impression. [7] [1]
Using the ACE score as an individual diagnostic or triage test is a frequent and avoidable error. The ACE score is a population risk marker that established the dose-response between adversity and adult disease; it is not a screening investigation, and applying it that way labels children without changing management. Ask about adversity to understand and support, not to score. [5] [4]
Relying on popular but unproven programmes diverts resources from effective ones. Stand-alone, scare-based or purely didactic interventions often lack evidence, and some widely used approaches have not been shown to reduce maltreatment. Prefer the well-specified, well-evidenced models — home visiting delivered as designed, parenting programmes with the effective components, school-based education with a Cochrane-supported curriculum. [1] [9]
Eroding trust by framing prevention as surveillance defeats the purpose. A supportive, strengths-based, voluntary stance engages families; a punitive, mandatory-only stance drives them away from exactly the services that would help. The clinician's language, tone and framing at the first contact often determine whether the family returns. [1] [7]
The false dichotomy of "family support versus child protection" traps clinicians into choosing one frame. Prevention and protection are a continuum, and the clinician moves between them depending on whether there is reasonable belief of current significant harm. The supportive stance does not suspend the duty to report; the duty to report does not suspend the supportive stance. [7] [1]
Failing to address structural drivers is the upstream version of the same error. Offering a parenting programme to a family without food or housing does not fix the cause and can feel like blame. Pair the clinical intervention with material and social support, because the modifiable drivers of maltreatment sit upstream of individual behaviour. [1] [1]
Prognosis & Disposition
Well-implemented prevention changes outcomes at population scale. The Nurse-Family Partnership randomised trials showed long-term reductions in verified maltreatment and child injuries over fifteen-year follow-up, and the Triple P population trial reduced substantiated maltreatment and out-of-home entries when delivered at scale. These are not clinic-level effects; they are population shifts. [2] [3]
Recurrence is common when a child returns to an unchanged environment, and re-injury after a sentinel event may be fatal — which is why tertiary prevention is not optional. A written safety plan, supervised contact, fixed follow-up and recurrence-prevention review reduce the risk of the second, more serious event. [7] [12]
The protective factor with the strongest evidence is a stable, responsive adult relationship, so disposition and support aim to build and protect it. Where the child cannot remain safely at home, placement with kin or a foster family preserves the relational buffer better than an institutional setting, and trauma-focused therapy supports recovery in both the child and the non-offending caregiver. [5] [6]
Disposition is a continuum rather than a single decision: ongoing universal support in the medical home, targeted family-support referral (home visiting, social work, financial and parenting programmes), and intensive coordinated support after harm. The clinician's job is to place the family on the right step of the pathway and to revisit it as need changes. [1] [3]
The safety-net is explicit: a written prevention plan, engagement of primary care, early-childhood services and education, a clear re-contact pathway for the family, and continuity that does not depend on a single clinician. Deterioration is caught early when the family knows how to return and the system remembers them between visits. [7] [8]
Special Populations
In Australia and Aotearoa New Zealand, prevention is delivered through a mix of the well-child medical home, universal parenting support, and targeted home visiting, with specific attention to Aboriginal and Torres Strait Islander and Maori children through community-led, culturally safe programmes. The RACP holds paediatricians to a role in prevention and advocacy, and the statutory child-protection systems run alongside — not instead of — family-support services. The buffering-adult principle is expressed in policy through early-years investment and family-violence response. [7]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children require culturally safe, community-led prevention that addresses structural determinants and historical context. Engage Indigenous health workers and family, apply the same objective, evidence-based standards, and do not conflate disadvantage with risk. Prevention imposed without cultural grounding re-creates the harm it aims to prevent. [7] [1]
Rural and remote children are reached through outreach, telehealth, school health and visiting services, because distance and workforce shortage limit access to face-to-face support. The prevention plan for a remote family accounts for what is actually available locally, and telehealth extends the reach of home visiting and parenting support. [7] [1]
Refugee, asylum-seeking and migrant children carry high baseline adversity and settlement stress. Screen actively for past and ongoing adversity and unmet health need, address language through trained interpreters (never a child), and connect the family to settlement and community supports. [7] [1]
Children with disability or chronic illness have a higher baseline prevalence of maltreatment, are often non-verbal, and may show only behavioural change or sleep disturbance as the signal of stress. Hold a higher index of prevention support, adapt communication to the child, and do not attribute distress to the disability. [7] [1]
Adolescent parents and families in socioeconomic disadvantage benefit from antenatal-onset home visiting and concrete material support, because material and social stress is the modifiable driver of recurrence. Children in out-of-home care are treated at every contact as a prevention opportunity, with coordinated health, developmental and mental-health assessment across placements. [2] [7]
Evidence, Guidelines & Regional Differences
The causal chain from maltreatment to adult disease now rests on large meta-analytic evidence, and it is the biological and epidemiological rationale for prevention. The ACE study established a graded relationship between the ACE score and the leading adult causes of death, including ischaemic heart disease. A meta-analysis of the long-term health consequences of abuse and neglect confirmed elevated risks of mental disorder, substance use, self-harm and physical disease in a dose-response pattern. [5] [6]
Nurse-Family Partnership — 15-year follow-up
Population: First-time mothers in disadvantage randomised to nurse home visiting from pregnancy through age 2, versus comparison services.
Key finding
At 15-year follow-up, the programme group had fewer verified child maltreatment reports and fewer child injuries than controls, alongside lower maternal welfare dependence and fewer subsequent pregnancies.
Practice change
Structured, antenatal-onset nurse home visiting is the best-evidenced targeted prevention for at-risk first-time families.
The prevention-intervention evidence base is set out in the Lancet series. The MacMillan review of interventions to prevent child maltreatment and associated impairment distinguishes what is supported (home visiting delivered as designed, parenting programmes with effective components) from what is not, and it grounds the stepped pathway. The burden and consequences papers establish why prevention is worth the investment. [1] [7]
The Triple P population trial is the cornerstone of the universal parenting-support case. Delivering the system at county-wide scale was associated with reduced substantiated maltreatment and out-of-home entries compared with control counties — a population-level effect, not merely a clinic effect. Parenting-programme component meta-analyses identify the active ingredients: teaching positive interaction, practising with the child, and consistent discipline including time-out. [3] [9]
School-based child sexual abuse prevention education is supported by a Cochrane review showing improved knowledge and self-protection skills without increased anxiety. The effect is on knowledge and disclosure; the programme is part of a wider safeguarding system. The home-visiting component meta-analysis reinforces that outcomes depend on programmes being well-specified, delivered as designed, and sustained through the highest-risk period. [10] [8]
The WHO INSPIRE framework packages the seven evidence-based strategies into one operational structure for governments, and the WHO global status report tracks country progress. These set the global policy frame against which regional practice is compared. [1] [7]
The regional policy structure is consistent in principle and varies in detail. In ANZ, the RACP holds paediatricians to a role in prevention and advocacy, and the well-child medical home is the platform. In the UK, the RCPCH and the statutory "Working Together" framework set the safeguarding and prevention standard, and health visitors deliver much of the home-visiting layer. In the US, the AAP and CDC promote prevention, home visiting is supported through federal programmes, and Bright Futures frames the well-child platform. In Canada, the RCPSC holds a health-advocate competency, and provinces deliver prevention through public health and child welfare. In every region the principle is the same: prevent before harm, support at-risk families, and act on current danger. [7] [1]
The controversies are real. Which programmes scale and sustain in real-world conditions; the balance between voluntary family support and statutory child protection; the misuse of the ACE score as a screening test; the risk of bias in over-surveillance; and the evidence gap for prevention in low- and middle-income settings all remain active. The defence against each is the same: evidence-based programmes delivered as designed, a strengths-based non-stigmatising stance, and a clear boundary between support and protection. [1] [7]
Exam Pearls
- Prevention is primary (whole population, before harm), secondary (targeted at-risk families, early), and tertiary (after harm, to prevent recurrence) — frame it as a public-health enterprise. [1]
- WHO INSPIRE = Implementation/enforcement of laws, Norms and values, Safe environments, Parent and caregiver support, Income and economic strengthening, Response and support services, Education and life skills. [1]
- The Nurse-Family Partnership 15-year follow-up showed reduced verified maltreatment and child injuries — the best-evidenced targeted home-visiting model. [2]
- Triple P at population scale reduced substantiated maltreatment and out-of-home entries — population-level parenting support works. [3]
- The single most protective factor — and the biological mechanism of prevention — is a stable, responsive adult relationship. [5]
- Do not use the ACE score as an individual diagnostic or triage test; it is a population risk marker. [5] [4]
- School-based child sexual abuse prevention education improves knowledge and self-protection skills without increasing anxiety (Cochrane). [10]
- Over-surveillance of poverty or Indigenous status is harmful and inequitable — the false dichotomy is "family support versus child protection." [7]
References
- [1]MacMillan HL; Thomas BH; Jamieson E; et al Interventions to prevent child maltreatment and associated impairment. Lancet, 2009.PMID 19056113
- [2]Olds DL; Eckenrode J; Henderson CR Jr; et al Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial. JAMA, 1997.PMID 9272895
- [3]Prinz RJ; Sanders MR; Shapiro CJ; Whitaker DJ; Lutzker JR Population-based prevention of child maltreatment: the U.S. Triple P system population trial. Prevention Science, 2009.PMID 19160053
- [4]Hughes K; Bellis MA; Hardcastle KA; et al The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health, 2017.PMID 29253477
- [5]Felitti VJ; Anda RF; Nordenberg D; et al Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 1998.PMID 9635069
- [6]Norman RE; Byambaa M; De R; Butchart A; Scott J; Vos T The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine, 2012.PMID 23209385
- [7]Gilbert R; Widom CS; Browne K; Fergusson D; Webb E; Janson S Burden and consequences of child maltreatment in high-income countries. Lancet, 2009.PMID 19056114
- [8]Filene JH; Gaughan DM; Nir T Components associated with home visiting program outcomes: a meta-analysis. Pediatrics, 2013.PMID 24187111
- [9]Kaminski JW; Valle LA; Filene JH; Boyle CL A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 2008.PMID 18205039
- [10]Walsh K; Zwi K; Woolfenden S; Shlonsky A School-based education programmes for the prevention of child sexual abuse. Cochrane Database of Systematic Reviews, 2015.PMID 25876919
- [11]Finkelhor D; Turner HA; Ormrod R; Hamby SL Trends in children's exposure to violence, 2003 to 2011. JAMA Pediatrics, 2014.PMID 24781431
- [12]Eckenrode J; Campa MI; Morris PA; et al The Prevention of Child Maltreatment Through the Nurse Family Partnership Program: Mediating Effects in a Long-Term Follow-up Study. Child Maltreatment, 2017.PMID 28032513