Paeds · child-safety-and-social-paediatrics
Psychological and emotional abuse
Also known as Emotional abuse in children · Psychological maltreatment of children · Emotional neglect in childhood · Psychological abuse and neglect · Coercive control of a child by a caregiver · Non-physical child maltreatment · Witnessing intimate-partner violence as a form of child abuse
A fellowship approach to psychological and emotional abuse of children: a sustained pattern of caregiver behaviour — spurning, terrorizing, isolating, exploiting, denying responsiveness, or mental-health neglect — that conveys the child is worthless, unloved, endangered, or valued only in meeting another's needs. Recognise that it leaves no mark yet is as harmful as physical or sexual abuse, assess the pattern and its developmental impact, exclude or find concurrent maltreatment, and act through a stepped, trauma-informed, jurisdiction-specific safeguarding pathway across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-year-old is brought to your clinic for bedwetting and "behaviour problems." Her mother describes her, in front of her, as "evil, stupid, a waste of space," and tells you she locks her in her room for hours "to teach her a lesson." The child sits frozen, eyes on her mother, silent. There is no mark on her body, no fracture, no burn — and yet what you are witnessing is child abuse. This is psychological and emotional abuse, the most prevalent and the most invisible form of maltreatment, and it is your business. [2] [12]
The definition that holds across guidelines is Glaser's conceptual framework: emotional abuse, or psychological maltreatment, is a repeated pattern of caregiver behaviour — or an extreme single act — that conveys to the child that they are worthless, unloved, endangered, or of value only in meeting another person's needs. Three features make a behaviour abusive rather than merely poor parenting: it is a pattern sustained over time, it comes from a person in a caregiving relationship with the child, and it causes, or is likely to cause, harm to the child's health or development. The American Academy of Pediatrics restates this in operational terms a clinician can apply at the bedside. [2] [4]
The decisive idea, and the one examiners test, is that the absence of a physical injury does not mean the absence of harm. Emotional abuse operates through the same biological pathways as every other maltreatment — the toxic-stress cascade — and the outcome is mediated by the same factor that is missing in the first place: a safe, stable, nurturing relationship. Shonkoff's developmental-science framework turns the old idea that "words don't hurt" on its head: a hostile, unpredictable, rejecting caregiver environment is an active biological force on the developing brain. [5] [3]
That gives you the clinician's task. You are not waiting for a specialist to confirm the diagnosis. You are looking for the pattern in the relationship, weighing its impact on the child, checking for concurrent maltreatment, and reporting within your jurisdiction — because the longer the exposure, the worse the outcome, and because a safe adult, found early, can change the trajectory. [12] [5]
Classification
Classify psychological maltreatment by the direction of the caregiver behaviour and by the type of behaviour. The direction splits cleanly into emotional abuse — acts of commission, things done to the child — and emotional neglect — acts of omission, things the child needs and is not given. Both live on one continuum of psychological maltreatment, and a single child almost always experiences a mixture of the two. [2] [4]
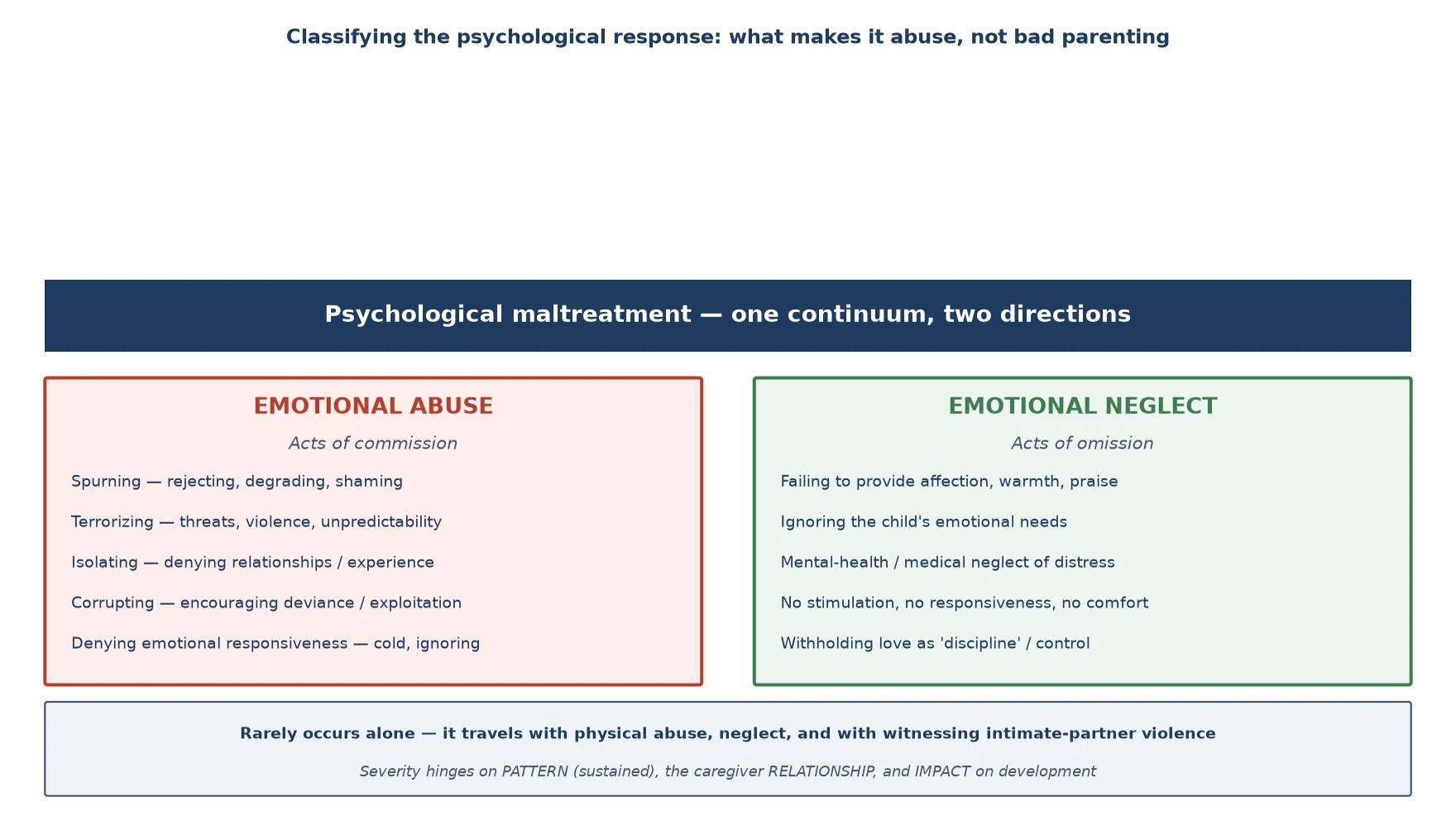
The behavioural categories Glaser and the APSAC framework describe are what you elicit in the history, not abstract labels. Spurning is rejecting, degrading, shaming, ridiculing or humiliating the child. Terrorizing is threatening violence, abandonment or harm, or placing the child in unpredictable danger. Isolating is denying the child normal relationships, experiences or freedom. Exploiting or corrupting is encouraging deviance, criminality or sexualisation, or using the child to meet the adult's needs. Denying emotional responsiveness is being cold, ignoring the child, or failing to provide affection and comfort. Mental-health, medical and educational neglect is failing to obtain care the child needs for a psychological, developmental or medical problem. [2] [4]
Emotional abuse
Acts of commission
- Spurning — rejecting, degrading, shaming
- Terrorizing — threats, violence, unpredictability
- Isolating — denying relationships or experience
- Corrupting — exploiting the child's needs
- Denying responsiveness — cold, ignoring
Emotional neglect
Acts of omission
- No affection, warmth or praise
- Ignoring the child's emotional needs
- Mental-health or medical neglect
- No stimulation or responsiveness
- Withholding love as control
Witnessing IPV
A recognised form
- Exposure to intimate-partner violence
- Coercive control in the home
- Now classified as a form of abuse
- Carries its own ACE burden
- Ask directly — it is common
The discriminator
Pattern + impact
- Sustained over time, not a one-off
- Comes from a caregiver relationship
- Likely to harm development
- Mix of abuse and neglect
- Almost never occurs alone
One category you must always ask about is witnessing intimate-partner violence. The contemporary safeguarding consensus, and the ACE evidence, treats a child's exposure to coercive control and violence between adults in the home as a form of psychological maltreatment in its own right — it terrorizes, it corrupts, and it denies a safe environment. Asking "is there conflict or violence in the home?" is a screening question, not an intrusion, because it carries its own dose of harm and changes the safety plan. [6] [9]
The question that separates abuse from "bad parenting" is never "is the parent harsh?" — it is "does this pattern cause, or is it likely to cause, harm to the child's health or development?" A single shouted insult on a hard day is not abuse; a daily climate of contempt, threat, or cold indifference is. Cultural practice and harsh discipline are not exempt — when the pattern meets the harm threshold, the duty to act is the same. [2] [12]
Epidemiology & Risk Factors
Psychological maltreatment is the most common form of child abuse and the most under-recognised. Stoltenborgh and colleagues' meta-analytic work shows that neglect — of which emotional neglect is a major component — is highly prevalent across populations, and emotional abuse itself is reliably underestimated precisely because it leaves no mark and is not captured by injury surveillance. The hidden nature of the harm is the epidemiological fact that shapes your practice: you will see this in every clinic, and most of it will not have been reported. [11] [2]
The Adverse Childhood Experiences study provides the dose-response backbone. Felitti and colleagues showed, in a large adult cohort, that the number of categories of childhood adversity — which include emotional, physical and sexual abuse, household substance use, mental illness, incarceration and intimate-partner violence — predicts, in a graded fashion, the leading causes of adult morbidity and mortality. Hughes and colleagues' meta-analysis extended this: multiple ACEs roughly multiply the risk of mental illness, substance use, violence victimisation and perpetration, and physical disease across the life course. [1] [6]
Hughes — Lancet Public Health meta-analysis (2017)
Population: Adults reporting adverse childhood experiences across 37 studies internationally
Key finding
A strong dose-response: compared with no ACEs, those with four or more had markedly higher odds of mental illness, substance use, interpersonal violence, and physical disease across the life course.
Risk factors cluster in the caregiving environment, and Sidebotham's ALSPAC cohort study maps them. The strongest and most actionable are caregiver mental illness, problematic alcohol or drug use, intimate-partner violence, a parental history of their own childhood abuse, family stress and socioeconomic disadvantage, and social isolation. Child factors raise risk too: a child with a disability, developmental difference, or difficult temperament, or one whose needs are harder to meet, is at elevated risk — and is simultaneously less able to disclose. Each is a screening question, not a footnote. [9] [12]
The protective factors are the mirror image, and they are also the treatment: a safe, stable, nurturing adult; parental insight and willingness to engage; access to support services; and a connected school or community. A child exposed to a hostile caregiver who also has a reliable, warm grandparent, teacher or mentor may weather the harm far better — the clearest proof that outcome is mediated by the presence of a buffering relationship, not determined by the exposure. [5] [10]
Pathophysiology
There is no lesion of emotional abuse on a blood test. The mechanism is the toxic-stress cascade: a sustained, unpredictable threat, delivered by the very person who should buffer it, activates the child's stress-response system without the safety net that would make the stress tolerable. Shonkoff's framework distinguishes three stress responses — positive, tolerable, and toxic — and emotional abuse is the archetype of the toxic form, because the source of threat and the source of safety are the same person. [5] [3]
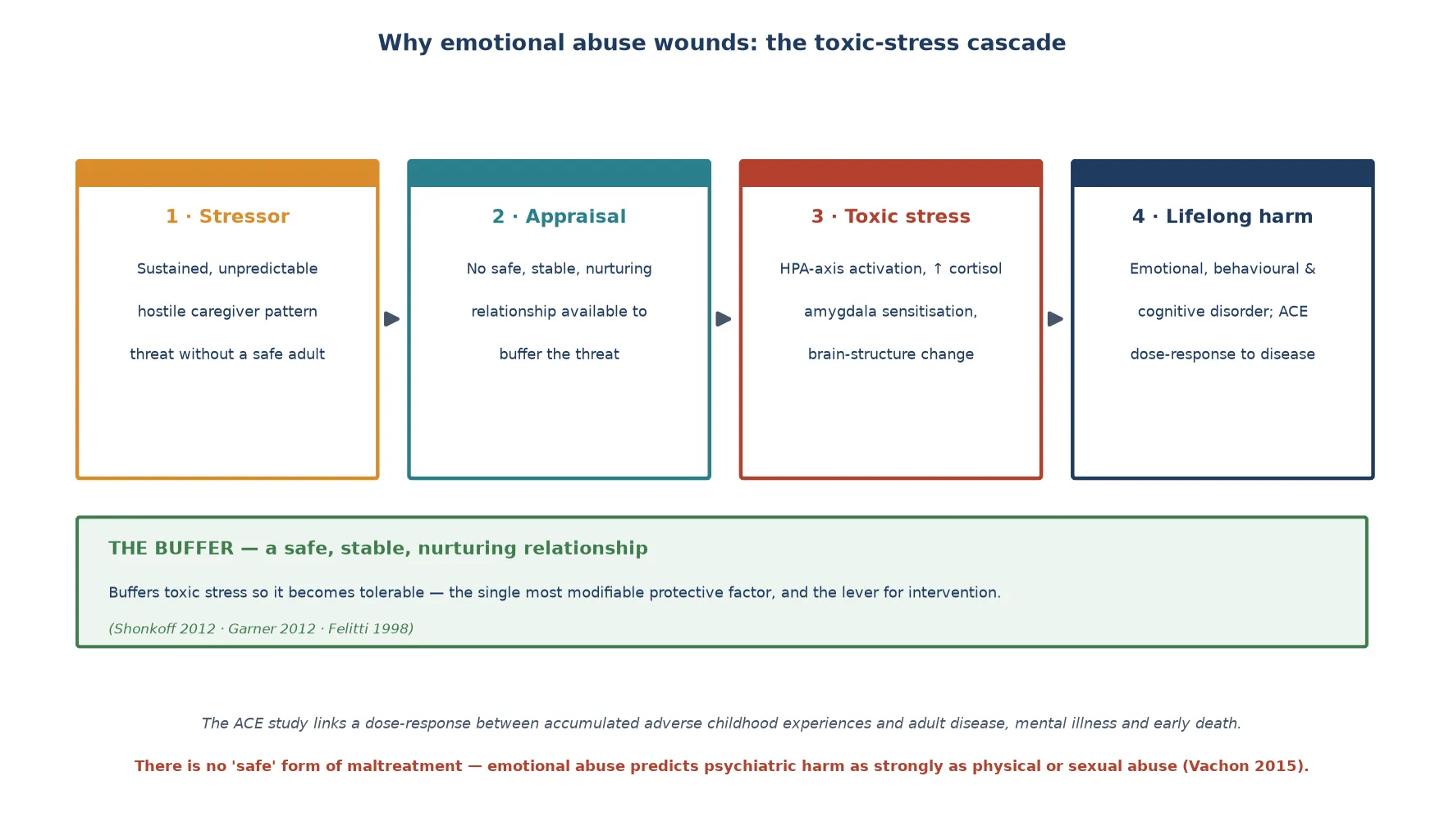
The cascade runs in four stages. The stressor is the hostile, rejecting, terrifying or emotionally absent caregiver environment. The appraisal stage fails because no safe, stable, nurturing relationship is available to buffer the threat — the very buffer a child needs is the source of danger. Toxic stress follows: chronic activation of the hypothalamic–pituitary–adrenal axis, sustained cortisol exposure, sensitisation of the amygdala, and measurable change in brain structures central to learning, memory and emotional regulation. The outcome is the dose-response curve the ACE study describes — mental illness, substance use, physical disease, and early death. [5] [1]
How toxic stress runs — and where you break it
Sustained, hostile caregiver pattern = a threat with no safe adult
No buffer → the stress system stays activated (chronic cortisol)
HPA-axis change, amygdala sensitisation, brain-structure alteration
Expressed as emotional, behavioural and cognitive disorder
ACE dose-response → mental illness, substance use, chronic disease
Break it at ANY node: remove the threat, supply the buffer, treat the harm
Glaser's review of the neuroscience grounds the clinical claim: child abuse and neglect, including the emotional forms, change the developing brain. The regions involved — those mediating threat detection, emotional regulation, attachment and executive function — are exactly the ones that present clinically as the child's behavioural and learning problems. This is why a "difficult" child living in a hostile caregiving environment is showing you a brain under sustained threat, not a character flaw. [3]
The most important evidence for your threshold to act is Vachon and colleagues' analysis: when different forms of maltreatment are disentangled, emotional maltreatment predicts psychiatric and behavioural harm as strongly as physical or sexual abuse. There is no "safe" form of child abuse. The clinician who waits for a bruise before acting on a hostile, terrorizing caregiving environment is waiting past the point of harm. [8] [7]
Clinical Presentation
Emotional abuse rarely presents as "abuse." It arrives disguised as the child's symptoms — the bedwetting, the aggression, the school refusal, the failure to thrive, the self-harm — or as a caregiver's behaviour that stops you in the room. Your task is to recognise the disguise and ask what the caregiving environment is doing to this child. [2] [12]
In the infant and preschool child, the signs are developmental and relational. Watch for failure to thrive without organic cause, developmental delay, regression, a frozen watchfulness, indiscriminate or absent attachment, and a child who flinches, avoids eye contact, or is excessively compliant. The caregiver may appear cold, hostile, or indifferent, may blame the child for everything, or may be so preoccupied with their own distress that the child is invisible. [3] [5]
In the school-age child and adolescent, the presentation broadens into emotional, behavioural and educational domains. Low self-esteem, anxiety, depression, anger and aggression, social withdrawal, self-harm and suicidal ideation, disordered eating, substance use, running away, and educational failure or school refusal are all flags — and each one should prompt a question about what is happening at home. None is pathognomonic; all become suspect when the caregiving environment is hostile, chaotic, or absent. [7] [12]
The caregiver behaviour itself is a clinical sign. A parent who, in your presence, belittles, threatens, terrorizes, scapegoats or coldly ignores the child; who uses the child to meet their own emotional needs; who gives a history that does not fit the child; or who refuses to engage with the child's distress, is showing you the abuse in real time. Document it factually — what was said and done, by whom, in front of whom — because your contemporaneous note may be the clearest evidence. [4] [12]
The family context completes the picture. Caregiver mental illness, substance use, intimate-partner violence, a parent's own history of abuse, poverty, housing instability and social isolation are not background noise — they are the engine of the pattern. A family under unrelenting strain with no support is the setting in which emotional abuse takes root and persists, which is why assessing the family system is part of assessing the child. [9] [10]
Differential Diagnosis
The central discrimination is between harm attributable to a caregiver pattern and symptoms arising from a primary child disorder. A child can have both — and often does — but the question that triggers a safeguarding response is whether the caregiving environment is causing, worsening, or failing to protect the child from harm. The history from the child and from collateral informants, not any single test, makes the call. [12] [4]
The hardest overlap is with primary neurodevelopmental and psychiatric disorders. ADHD, autism, an anxiety disorder, a depressive disorder, an attachment disorder and a learning difficulty can all produce the withdrawal, aggression, regression or school failure that emotional abuse produces. Resolve it by assessing the caregiving environment directly: a child whose symptoms resolve when they are safe, or whose caregiver is hostile and rejecting, points to maltreatment as a cause or contributor, not merely a comorbidity. [12] [8]
Distinguish failure to thrive and developmental delay from organic disease — but do so without dismissing the possibility that the cause is emotional neglect or a hostile environment. The discipline is to investigate the medical differential fully while assessing the caregiving relationship in parallel, because treating only the organic cause in an emotionally neglected child leaves the active harm untreated. [3] [11]
Separate cultural practice and harsh discipline from abuse by the harm standard, not by cultural labelling. Reasonable, culturally normative child-rearing that does not endanger the child's health or development is not abuse; a pattern that terrorizes, degrades, isolates or denies responsiveness, whatever its cultural framing, meets the threshold. When unsure, consult your local safeguarding team rather than defaulting to inaction. [2] [4]
Finally, recognise fabricated or induced illness as an overlap pattern. A caregiver who describes, exaggerates or induces symptoms that serve the adult's needs — attention, control, the sick role — is psychologically maltreating the child even when the medical workup is negative. The clue is a child whose reported symptoms do not fit the examination, whose caregiver resists recovery, and whose care is fragmented across multiple services. [12] [4]
Clinical & Bedside Assessment
Begin with the child alone, wherever developmentally possible, using open questions and then specific ones. Ask directly about what happens at home when things go wrong, how the child is treated, whether anyone frightens or hurts them, and whether they feel loved. Direct, calm questioning is safe and high-yield; do not rehearse leading questions or promise blanket secrecy you cannot keep. Tell the child what you will do next. [4] [12]
Anchor the history in the caregiving environment. Ask who lives in the home, who cares for the child, and about caregiver mental health, substance use, intimate-partner violence, a parental history of abuse, and the family's supports and stressors. These are the risk factors the ALSPAC cohort identified, and they are the modifiable engine of the pattern — ask each one, and document the answers. [9] [10]
The emotional-abuse history — what you must ask
Take collateral history deliberately. Teachers, early-childhood educators, general practitioners and any child-protection or welfare services hold pieces of the pattern you will not see in one visit. With appropriate consent, or through your jurisdiction's information-sharing provisions, seek their observations — a child who is frozen, fearful or regressed at school, or a family known to services, materially changes your assessment. [9] [4]
Observe the child–caregiver interaction and document it factually. Note the child's affect, watchfulness, flinching, compliance, and whether they seek or avoid the caregiver; note the caregiver's warmth, hostility, blame, responsiveness and use of the child. Examination is directed at the developmental and growth picture and at finding or excluding signs of concurrent physical abuse or neglect — a pattern of injury or self-harm, untreated medical needs, or signs of sexual abuse. The absence of physical signs does not exclude emotional abuse; their presence escalates the response. [3] [4]
Investigations
There is no biological test for emotional abuse, and none is needed to make the diagnosis — which rests on the pattern of caregiver behaviour and its developmental impact. Over-investigating a child to "prove" emotional abuse is harmful and unnecessary. The investigative task is targeted, not exhaustive. [2] [4]
The first investigative question is always "is there concurrent physical or sexual abuse or neglect?" If the history, examination or pattern raises that possibility, investigate accordingly — a skeletal survey, neuroimaging, blood tests for failure to thrive, or a forensic sexual-assault examination by a trained clinician, as the picture demands. Emotional abuse is the entry point; the concurrent injury may be the immediate danger. [4] [12]
Use standardised screens to quantify the impact and track it over time, not to make the diagnosis. The Strengths and Difficulties Questionnaire maps broad emotional and behavioural problems; age-appropriate mood and anxiety screens quantify depressive and anxious symptoms; and direct, repeated questioning about self-harm and suicidal ideation is mandatory, because emotional abuse raises suicide risk. Screening is repeated at every meaningful contact, not done once. [7] [6]
Arrange specialist and multidisciplinary assessment where the picture is complex — developmental assessment for a child with delay or regression, child and adolescent mental-health assessment where a disorder is suspected, and referral to a child-protection or safeguarding team for the forensic and safety components you do not own alone. Your role is to recognise, report, and coordinate, not to single-handedly prove the case. [12] [4]
Management — Resuscitation
The immediate priority is safety, and it has two limbs. The first is the child's immediate physical and psychological safety: is there concurrent physical or sexual abuse, or neglect, that places the child in danger right now? Is the child suicidal, or at risk of serious self-harm? The second is the legal and protective response your jurisdiction requires. [4] [12]
[4] [7]If the child discloses suicidal ideation or intent, treat it as the emergency it is regardless of the abuse: assess ideation, intent, plan and access to means; build a safety plan; arrange same-day urgent mental-health assessment; do not leave the child alone; and involve carers within the bounds of safety. Emotional abuse is a risk factor for suicide, and disclosed ideation overrides every other clinical priority. [7] [12]
If there is immediate danger from concurrent physical or sexual abuse, or a child too unsafe to return home, escalate at once to your local child-protection authority, the police where relevant, and your hospital safeguarding team. Do not attempt to manage an acute safety crisis alone — your job is to recognise, secure the child, report, and hand the forensic and placement decisions to the system built for them. [4] [9]
If the situation is serious but not immediately dangerous, the immediate action is to report within your jurisdiction's framework and begin the documented safeguarding pathway. Know your local law: in Australia and New Zealand, mandatory reporting obligations vary by state and territory but generally require reporting of suspected child abuse; in the UK the paediatrician shares information with children's social care; in the US and Canada, reporting to child protective services is mandated. Reporting is not an accusation; it is a request for assessment. [4] [12]
Management — Definitive & Stepwise
The definitive response is a three-tier, trauma-informed safeguarding pathway — recognise and report, protect, and then repair. The tiers are not alternatives; a single child may need all three at once, and the paediatrician's job is to coordinate the plan, not to deliver every component. [5] [10]
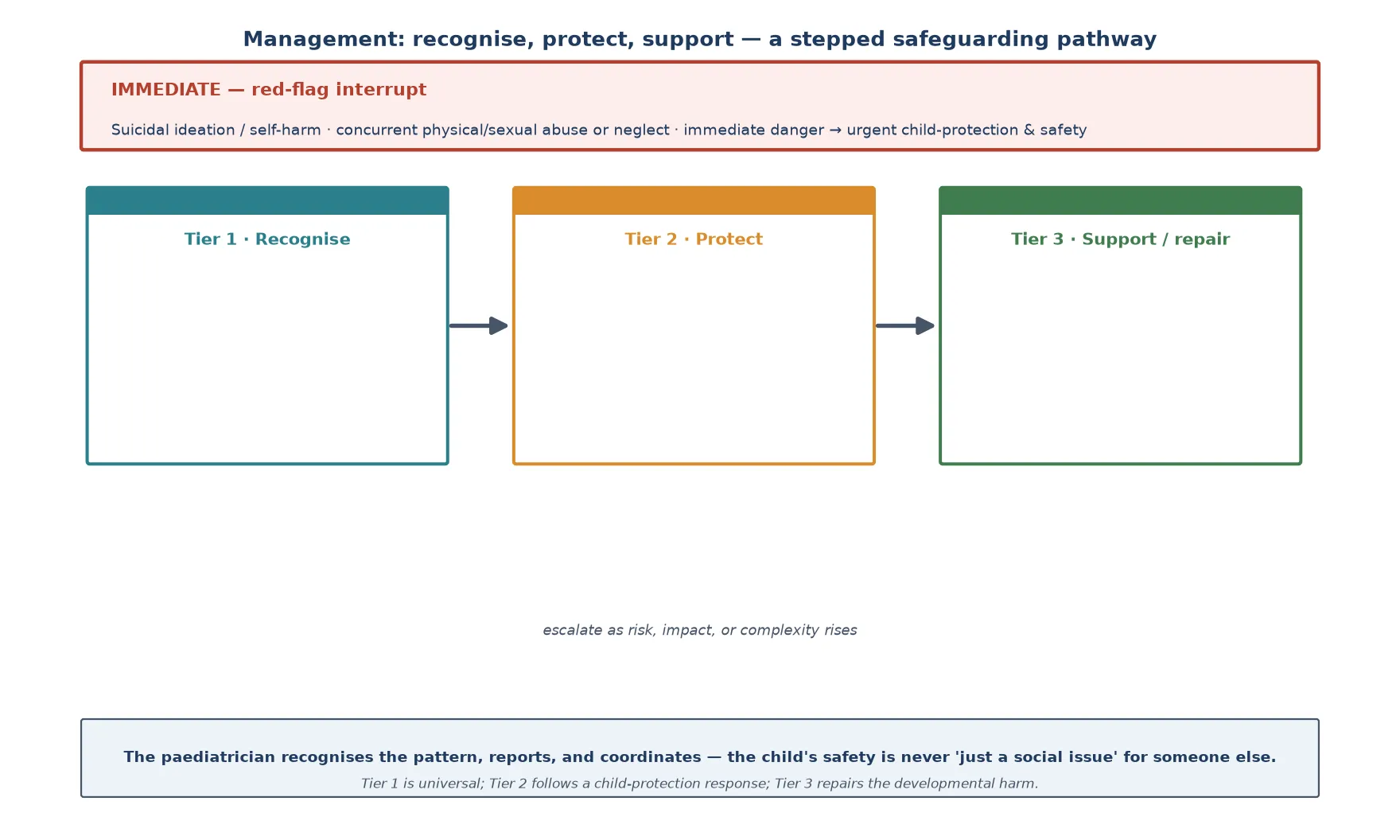
Tier 1 — Recognise and report. This is every clinician's job at every contact. Ask about the caregiving environment, observe the interaction, take collateral history, document factually, name emotional abuse as a concern, and report within your jurisdiction. Psychoeducation — that words and a hostile climate cause real, biological harm — applies to the family, to schools, and to colleagues who still think "no bruise, no problem." [4] [5]
Tier 2 — Protect. This follows a child-protection response: referral to child-protection services and a strategy discussion, a safety plan that reduces the child's contact with the source of harm, stabilisation of the placement (which may mean kinship or out-of-home care), and direct work on the caregiving environment — treating caregiver mental illness, substance use and intimate-partner violence, and building family supports. The aim is to stop the exposure and supply the buffer. [10] [9]
Tier 3 — Support and repair. This is the long arc. Evidence-based parenting programs help willing caregivers change the pattern; trauma-focused therapy helps the child process the harm and rebuild regulation and relationships; child and adolescent mental-health services treat the disorders the abuse produced — depression, anxiety, post-traumatic stress, self-harm; and sustained relational and school support rebuilds the developmental trajectory. The repair is relational because the wound was relational. [12] [3]
Building the plan — and who owns each step
Recognise + document the pattern; report per jurisdiction (paediatrician)
Strategy discussion + safety plan (child-protection team)
Stabilise placement; treat caregiver factors (social care + adult services)
Parenting program for the caregiver; trauma-focused therapy for the child
CAMHS for disorder / self-harm; treat depression, anxiety, PTSD
Sustained school + relational support; the paediatrician coordinates
Throughout, apply a trauma-informed stance. Tell the child they are believed and not to blame; give them control over pace and information wherever safely possible; avoid re-traumatising assessments; share information on a need-to-know basis; and recognise that the family in front of you may carry its own history of abuse. Trauma-informed care is not soft — it is the set of conditions under which disclosure, engagement and recovery become possible. [5] [12]
Specific Subtypes & Scenarios
Witnessing intimate-partner violence is the subtype most often missed and most clearly now classed as psychological maltreatment. A child exposed to coercive control, threats or violence between adults in the home is terrorized, denied a safe environment, and carries an independent ACE burden. Ask directly about conflict and violence in the home, integrate the answer into your safety plan, and coordinate with adult and family-violence services — protecting the protective parent often protects the child. [6] [9]
Terrorizing — threats of violence, abandonment or extreme unpredictability — produces a child who is hypervigilant, anxious and dysregulated. Isolating, which denies the child normal relationships and experience, is a feature of children kept from school, peers and health care; suspect it in a child who is "invisible" to services. Exploiting and corrupting — using the child to meet adult needs, or exposing them to criminality or inappropriate sexualisation — overlaps with sexual abuse and with youth-justice presentations. [2] [4]
Fabricated or induced illness sits at the boundary of emotional and physical abuse. A caregiver who fabricates, exaggerates or induces illness serves their own needs at the expense of the child's, exposes the child to harmful investigation and treatment, and psychologically distorts the child's sense of their own body. The clue is poor fit between reported and observed findings, a caregiver who resists recovery, and fragmented care across services. Recognise, protect, and escalate to a specialist child-protection team. [12] [4]
The adolescent presents with self-harm, substance use, school refusal, disordered eating, depression, or running away, and may resist disclosure because loyalty to the caregiver and fear of removal compete with the need for help. Build trust, ask directly about suicidality, and remember that emotional abuse in adolescence is still abuse — the threshold to act is the same. The institutional setting — residential care, youth justice, boarding — carries its own patterns of isolation and corrupting influence and demands the same vigilance. [7] [12]
Complications & Pitfalls
The complications of emotional abuse are the lifelong consequences the ACE study maps: mental illness, substance use, self-harm and suicide, interpersonal violence, chronic physical disease, and early death, all rising with the ACE dose. Emotional abuse is not the mildest form — it carries harm comparable to physical and sexual abuse, and the child who experiences several forms suffers most. [1] [8]
The commonest pitfall is dismissing the picture as "just bad parenting" or "a cultural difference" and doing nothing. The harm standard, not the label, decides the duty. The second is waiting for a physical injury before acting — by the time one appears, the child has often been harmed for years. The third is missing concurrent maltreatment: emotional abuse is the entry point, and the physical, sexual or neglectful abuse travelling with it may be the immediate danger. [2] [4]
Diagnostic overshadowing cuts the other way: a disabled or neurodivergent child whose distress, regression or behaviour change is attributed to "the disability" rather than to an abusive caregiving environment is a child whose maltreatment is being missed. The safeguard is the same discipline used elsewhere — every new symptom in a vulnerable child gets the full differential, including abuse. [12] [9]
The procedural pitfalls are just as costly: failing to report when the threshold is met, promising the child absolute secrecy you cannot keep, conducting a leading or repeated interview that contaminates disclosure, or attempting to manage a safety crisis alone. Know your jurisdiction, document contemporaneously, share information appropriately, and hand forensic and placement decisions to the system built for them. [4] [12]
Prognosis & Disposition
Outcome is mediated, not determined — the same principle that governs the whole field of developmental adversity. The duration, severity and pervasiveness of the exposure set the baseline risk, but the presence of a safe, stable, nurturing adult, the speed of removal from the source of harm, and the quality of the repair all shift the trajectory. A child removed early into a stable, caring placement, given trauma-focused support, can recover substantially. [5] [10]
The prognosis worsens with longer exposure, multiple forms of maltreatment, untreated caregiver illness, and absence of any buffering relationship. It improves with early recognition, a stable placement, treatment of the child's disorders, and sustained relational and educational support. This is why your early action — recognising and reporting — genuinely changes the outcome, even though you will rarely see the full arc yourself. [1] [3]
Disposition follows the tiered pathway. The child at immediate risk is admitted or placed for safety; the child with a treatable mental-health disorder is referred to CAMHS; the child whose caregiver will engage goes into a parenting program with support; and the child who is safe but recovering needs sustained primary-care, school and community follow-up. The paediatrician's role does not end at the report — it runs through coordination and long-term support. [12] [4]
Special Populations
Children with disability and neurodivergent children are at elevated risk of every form of maltreatment, including emotional abuse, and are simultaneously less able to disclose and more often subject to diagnostic overshadowing. Adapt your assessment to their communication, use observation and informant report, and apply the same harm standard — a hostile, rejecting or neglectful caregiving environment is abuse regardless of the child's baseline. [9] [12]
Indigenous children, and migrant, refugee and asylum-seeking families, may face the cumulative risk of intergenerational trauma, racism, separation, language barriers and reduced access to services, layered on top of the caregiving stressors that drive abuse. Respond with cultural safety, trained interpreters (never family members for safeguarding disclosure), and an awareness that reporting obligations apply equally while the supporting response must be culturally informed. [6] [10]
Children in out-of-home care and in youth-justice settings carry the highest ACE loads in the population, and the abuse that brought them there is often ongoing in its developmental effects. Their emotional and behavioural presentations are maltreatment sequelae until proven otherwise, and they need trauma-informed, consistency-focused care rather than punishment. Adolescents who self-harm, use substances, or refuse school are a high-risk group in whom emotional abuse must be actively excluded. [1] [7]
Socioeconomically disadvantaged families face the structural stressors — poverty, housing instability, food insecurity, social isolation — that fuel the caregiving patterns behind emotional abuse. Recognising the structural drivers is not a reason to lower the threshold for action; it is a reason to combine the safeguarding response with material and social support, because a family supported out of crisis can, with the right help, become safe. [9] [10]
Evidence, Guidelines & Regional Differences
The developmental-science consensus — Shonkoff and Garner's AAP policy statements on toxic stress — anchors the contemporary understanding that emotional abuse is biologically harmful, not merely unpleasant. The APSAC framework and the AAP's clinical report on psychological maltreatment operationalise recognition and response for the clinician, and DeJong and colleagues' recent review addresses the practical challenges of recognising emotional abuse in clinical settings. [5] [4] [12]
[4] [12]The regional difference that matters most at the bedside is the threshold and mechanism of reporting. The duty to report reasonable suspicion is near-universal across ANZ, the UK, the US and Canada; what varies is who must report, which forms of maltreatment are mandated, and which agency receives the report. Learn your local threshold and pathway before you need them — the worst time to learn your jurisdiction's law is during a disclosure. [4]
Controversies remain in how best to measure the prevalence of emotional abuse, how to distinguish cultural practice from harm, and how to balance the protective response against the harms of unnecessary removal. The evidence is clearest on two points examiners reward: emotional abuse is common, hidden, and biologically harmful; and a safe, stable, nurturing relationship is both the missing factor and the most powerful treatment. [2] [5]
Exam Pearls
[2] [4] [8]References
- [1]Felitti VJ; Anda RF; Nordenberg D; Williamson DF; et al Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 1998.PMID 9635069
- [2]Glaser D Emotional abuse and neglect (psychological maltreatment): a conceptual framework. Child Abuse & Neglect, 2002.PMID 12201163
- [3]Glaser D Child abuse and neglect and the brain--a review. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 2000.PMID 10763678
- [4]Hibbard R; Barlow J; Macmillan H; Committee on Child Abuse and Neglect; et al Psychological maltreatment. Pediatrics, 2012.PMID 22848125
- [5]Shonkoff JP; Garner AS; Committee on Psychosocial Aspects of Child and Family Health; et al The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 2012.PMID 22201156
- [6]Hughes K; Bellis MA; Hardcastle KA; Sethi D; et al The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. The Lancet Public Health, 2017.PMID 29253477
- [7]Norman RE; Byambaa M; De R; Butchart A; et al The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine, 2012.PMID 23209385
- [8]Vachon DD; Krueger RF; Rogosch FA; Cicchetti D Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry, 2015.PMID 26465073
- [9]Sidebotham P; Heron J; ALSPAC Study Team Child maltreatment in the "children of the nineties": a cohort study of risk factors. Child Abuse & Neglect, 2006.PMID 16701895
- [10]Garner AS; Shonkoff JP; Committee on Psychosocial Aspects of Child and Family Health; et al Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [11]Stoltenborgh M; Bakermans-Kranenburg MJ; van Ijzendoorn MH The neglect of child neglect: a meta-analytic review of the prevalence of neglect. Social Psychiatry and Psychiatric Epidemiology, 2013.PMID 22797133
- [12]DeJong M; Wilkinson S; Apostu C; Glaser D Emotional abuse and neglect in a clinical setting: challenges for mental health professionals. BJPsych Bulletin, 2022.PMID 34544522