Paeds · child-safety-and-social-paediatrics
Refugee, asylum-seeking and newly arrived children
Also known as Refugee child health · Asylum-seeking children · Newly arrived migrant children · Unaccompanied minors · Forcibly displaced children · Catch-up care for migrant children
A fellowship approach to health care for refugee, asylum-seeking and newly arrived children: classification of migration status and stage of journey; the heavy cumulative infectious-disease, immunisation, mental-health, nutrition, growth, developmental, dental and sensory burden and its forced-displacement toxic-stress mechanism; a trauma-informed, interpreter-mediated on-arrival health assessment; guardianship and consent authority and conditional confidentiality, especially for unaccompanied or separated children; stepwise catch-up screening and management; the harm of immigration detention; and advocacy across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A nine-year-old girl arrives in your clinic six weeks after her family fled a conflict zone. She has no immunisation record, speaks a language none of your nurses share, and her mother is anxious about what you will tell the caseworker. This is the everyday work of caring for refugee and newly arrived children, and the clinical skill it tests is delivering catch-up, trauma-aware medicine across language, culture and broken records. [1] [15]
A refugee child is one whose family has crossed an international border because of a well-founded fear of persecution, and who holds or is seeking formal protection. An asylum-seeking child has lodged a protection claim that is still pending, and a newly arrived migrant child has recently crossed a border under any migration pathway. The distinctions matter legally, but clinically the task is the same: treat the child in front of you. [1]
What makes this population clinically distinct is the accumulated adversity of forced displacement, layered on top of whatever brought the child across the border. Infectious disease, missing immunisation, mental-health difficulty, faltering growth and unmet dental and sensory need are all far more common than in community peers. Recognising that burden — and using a trained interpreter every time — is the core task. [3] [16]
The clinician's role is to be the stable, trusted medical home that catches the child up to their peers. You screen on arrival, you reconstruct the history, you coordinate the team around the family, and you plan for recovery and acculturation so that resettlement becomes a health intervention rather than another disruption. [1] [2]
Classification
Begin with the child in front of you, then classify their migration status and the stage of their journey, because the second tells you where the catch-up window sits and the first sets the legal context. [1]
Refugee
Convention-recognised
- Protection granted or resettled
- Often eligible for full health coverage
- Stability supports recovery
- Still needs the full catch-up bundle
Asylum-seeker
Claim pending
- Heightened uncertainty sustains arousal
- Coverage and access vary by jurisdiction
- Mental-health risk is high
- Detention risk is highest here
Newly arrived migrant
Recent cross-border
- Status and pathway vary widely
- Records may be fragmented or absent
- Catch-up immunisation often needed
- Apply the universal health-needs lens
Unaccompanied / separated
No parent or carer
- State or appointed guardian holds responsibility
- Attachment loss and isolation concentrate risk
- Guardianship governs consent
- Highest combined clinical and psychosocial need
The stage of the journey runs alongside the status and matters because it shifts the clinical task. A child may be pre-departure (still exposed to conflict and disrupted care), in transit (facing danger, exploitation and uncertainty), on arrival (the screening window when the hidden burden is meant to be found), or resettled (entering the medical home for recovery and acculturation). Before you treat, you must know where the child sits, because it tells you whether to screen, to stabilise, or to support recovery. [1] [15]
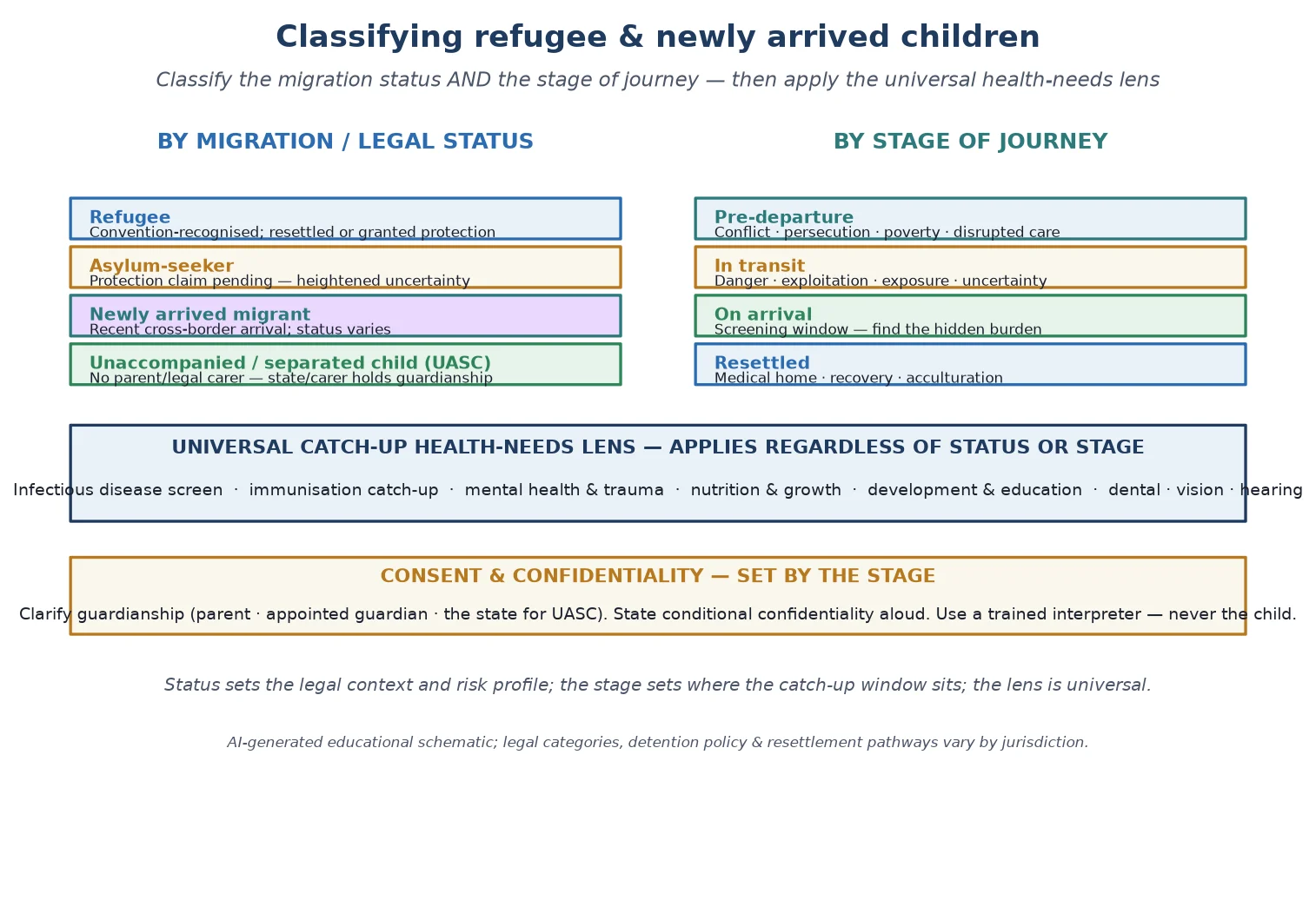
Whatever the status, the catch-up health-needs lens is universal. Every refugee or newly arrived child deserves a trauma-informed assessment, an infectious-disease and immunisation screen, attention to mental health, nutrition, growth, development and sensory health, and a clear statement of who can consent. The status changes the legal context and the risk profile; it does not change the bundle. [1] [4]
Epidemiology & Risk Factors
Forced displacement affects tens of millions of children worldwide, and Australia, New Zealand, the UK, the US and Canada all receive refugee and asylum-seeking children through resettlement and spontaneous arrival pathways. [1] [3]
The health burden is not a small upward shift; it is large across nearly every domain an examiner names. Infectious diseases such as tuberculosis, hepatitis B and C, intestinal parasites and malaria are markedly more prevalent than in the host community, reflecting exposure before and during the journey. [4] [5]
Nutrition and growth problems are over-represented. Iron-deficiency anaemia, vitamin D deficiency and rickets are common, and faltering growth reflects pre-arrival deprivation in younger children. Elevated blood lead is a particular concern in resettled refugee children and warrants routine screening. [7] [6]
Mental-health difficulty is the signature burden of this population. PTSD, depression and anxiety are several-fold more common than in host-community peers, with risk driven by cumulative trauma exposure and family separation, and protection conferred by family unity, stability, school engagement and social support. [2] [9]
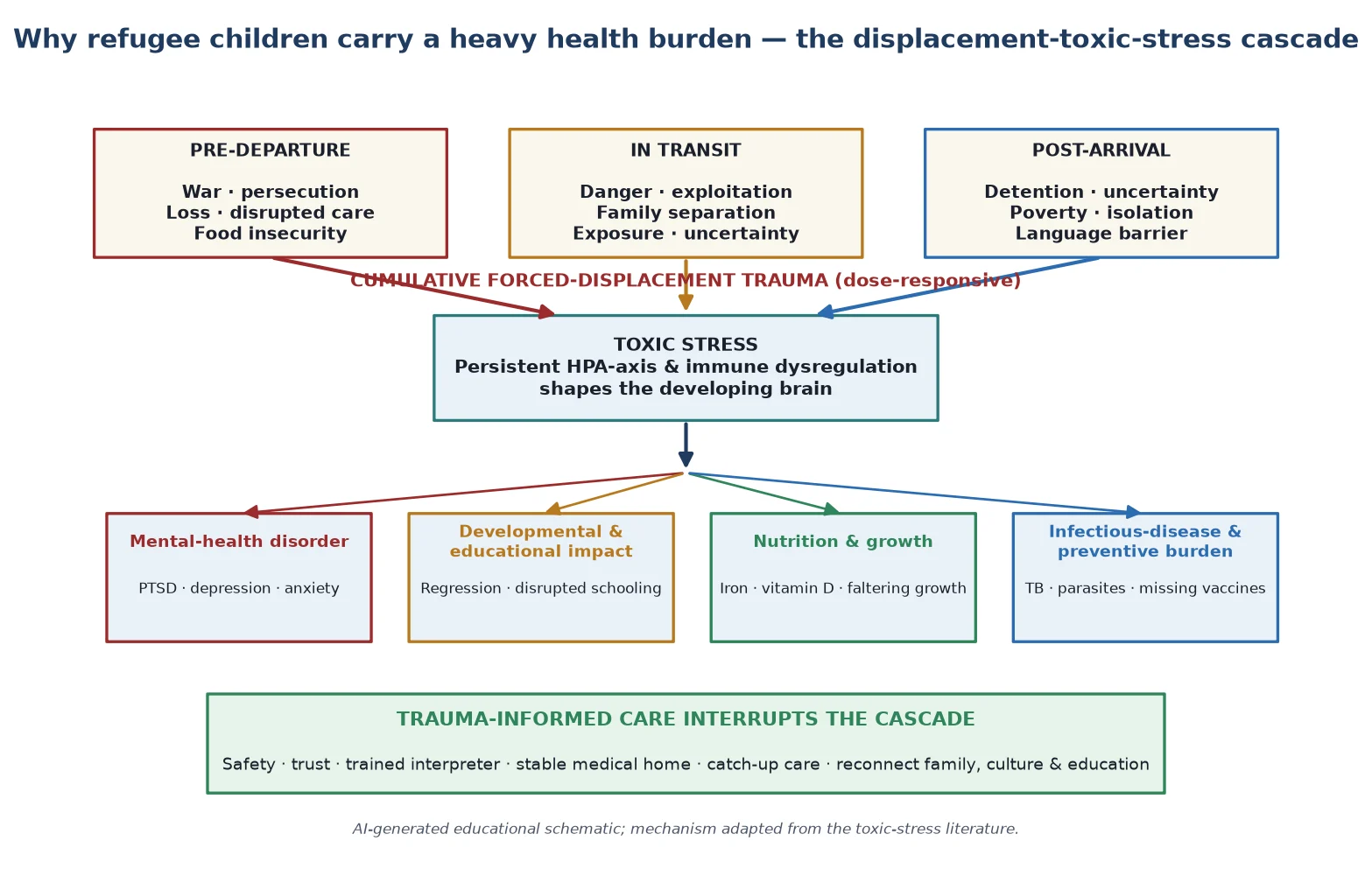
Adverse experiences are the engine of this burden, and the relationship is dose-responsive: more cumulative trauma exposure — across pre-departure conflict, transit danger and post-arrival uncertainty — produces more dysregulation. This is why stability itself is a health intervention. [2]
Subgroups carry the highest risk and are the ones an examiner will probe: unaccompanied minors, children held in immigration detention, those from intense conflict settings, infants and young children, and those with chronic disease or disability whose care has been disrupted. [9] [10]
Language barriers, low health literacy, poverty and fragmented records act as access barriers that worsen outcomes. A child whose history has to be retold at every service, through an ad-hoc interpreter, has been given several chances to fall through the gaps. [14] [15]
Pathophysiology
The clinical picture only makes sense once you see how forced displacement becomes biology. Pre-departure conflict, transit dangers and post-arrival uncertainty accumulate as cumulative trauma, and that trauma acts on a developing child through a toxic-stress mechanism. [2]
Toxic stress persistently activates and dysregulates the stress response — the HPA axis, immune signalling and neurodevelopment — so that the developing brain is shaped by chronic threat rather than by safety. The relationship is dose-responsive, which is why the youngest children, whose brains are most plastic, carry the deepest developmental risk. [2]
Family separation and the loss of a caregiving figure are their own mechanism of harm. An unaccompanied child has lost the attachment figure that buffers stress, and that loss shows up as hypervigilance, withdrawal, distrust or indiscriminate friendliness — behaviours that are adaptations to loss, not signs of a primary disorder. [9]
Acculturation stress operates as a distinct post-arrival mechanism on top of the original trauma. A resettled adolescent is navigating a new language, school, peer group and identity at the same time as recovering from displacement, and that load sustains arousal even when the child is now physically safe. [2]
Chronic uncertainty sustains the cascade. A pending asylum determination, the threat of detention, or housing instability keeps the stress response activated, so the child cannot settle into recovery even after arrival. [10]
Finally, language barriers and fragmented records compound the biological burden by delaying identification and treatment — a child's tuberculosis, anaemia or unmet immunisation simply goes unrecognised through the gaps in records and communication. [4] [14]
Clinical Presentation
A child may arrive in your orbit in two ways: acutely, in the days around arrival with a febrile illness or crisis, or routinely, for the scheduled on-arrival health assessment. The acute presentation is the emergency — fever in a child from a malaria-endemic region, dehydration, sepsis, severe malnutrition, or a mental-health crisis. The routine presentation is the planned visit at which the hidden burden is meant to be found. [1] [15]
Unrecognised trauma shows itself differently in a younger child than in an adolescent. Look for regression (loss of skills, sleep disturbance, feeding difficulty), withdrawal, somatic complaints and disrupted play in younger children, and intrusion, avoidance, hyperarousal, self-harm or substance use in older children. None of these is a diagnosis on its own; each is a signal to screen. [2] [13]
Developmental and educational difficulty presents differently across age. A young child may show global delay or disrupted play; a school-age child may present with learning difficulty and inattention that have been attributed to language rather than to unmet need; an adolescent may present with school refusal and disengagement. [3]
Nutrition problems present concretely. Faltering growth and fatigue suggest pre-arrival deprivation; pallor points to iron-deficiency anaemia; bowed legs or bone pain suggest rickets from vitamin D deficiency; and pica or developmental change should raise the possibility of lead exposure. [7] [6]
Mental-health difficulty often surfaces indirectly. A child who freezes when you raise your voice, who is hypervigilant in the waiting room, who complains of headaches and stomach aches repeatedly, or who has withdrawn from peers is telling you something about distress — and you should screen rather than reassure and move on. [13] [2]
At the on-arrival assessment you will often find the unmet burden made concrete: fragmented or absent immunisation, growth faltering, untreated dental caries, uncorrected vision or hearing deficits, and laboratory evidence of tuberculosis, parasites, anaemia, vitamin D deficiency or lead exposure. [3] [5] [11]
A child currently held in detention may present with deterioration — sleep disturbance, regression, withdrawal or worsening of chronic disease — driven by the environment rather than the original trauma, and that environmental cause is itself a clinical finding. [10]
Differential Diagnosis
The central diagnostic skill in this population is telling apart trauma-driven symptoms from those that signal a discrete disorder — and resisting the pull to label too quickly. Trauma symptoms of intrusion, avoidance, hyperarousance and dissociation overlap with primary anxiety and depressive disorders, and the two often genuinely co-occur. [2] [13]
Developmental delay caused by disrupted education and trauma must be distinguished from a specific neurodevelopmental disorder such as fetal alcohol spectrum disorder, intellectual developmental disorder or autism. The history matters: a single post-arrival assessment undercalls the child's potential, because delay driven by deprivation and disrupted schooling can improve with stability. [3]
Fever in a newly arrived child is the highest-stakes differential. You must hold malaria, typhoid, tuberculosis and other imported infections in the same frame as common childhood illness, and a child from a malaria-endemic region with fever is presumed to have malaria until proven otherwise. [4] [5]
Faltering growth must be read against the history of pre-arrival deprivation and catch-up needs. It may reflect deprivation that will recover with nutrition and stability, or it may signal organic disease — and you must investigate rather than assume. [3] [7]
Iron-deficiency anaemia is common and nutritional, but a child from a haemoglobinopathy-endemic region needs a haemoglobinopathy screen rather than an assumption that pallor is only iron deficiency. [4]
When a refugee child presents with a somatic complaint, you must hold two truths at once: physical illness is real and common in this group (and is often missed), and trauma also manifests somatically. Avoid diagnostic overshadowing — never assume a symptom is "just stress" until you have excluded organic disease. [3] [2]
Finally, acculturation stress in a recently resettled adolescent must be distinguished from a primary mental-health disorder. The distinguishing feature is the temporal link to the resettlement transition and the protective effect of family unity, peer connection and school engagement. [2]
Clinical & Bedside Assessment
Open every encounter with the trauma-informed principles an examiner will look for: safety, trust, choice, collaboration and strengths. Greet the child first, before the family; explain what the visit is for; let the child keep a comfort object and the family close; offer choice about the sequence of the examination; and pace the assessment so the child is not overwhelmed. [1] [2]
Before you assess or treat, clarify and document guardianship and consent authority. Who holds parental responsibility — parent, appointed guardian, or the state for an unaccompanied child — and, for an older adolescent, does the young person have capacity for the decision at hand under the mature-minor principle? Record the answer; it governs every intervention that follows. [1] [15]
[14] [1]State the conditional confidentiality frame aloud, in language the family can understand: what we talk about stays between us unless I am worried the child is not safe, someone else is being hurt, or the law tells me I must act. Be explicit about what a caseworker or immigration official will and will not receive, share the minimum necessary and lawful, and tell the family before you share anything that crosses a threshold. [1] [15]
Take a reconstructed history when records are fragmented: birth and perinatal history, developmental milestones, educational trajectory, immunisation where it can be found, and a trauma-informed psychosocial history adapted to the child's age and journey. Ask about pre-departure exposure, transit conditions, and current housing, family integrity and immigration status, always through the interpreter. [1] [3]
Examine trauma-informed. Explain what you will do before you do it, let the child say stop, leave underwear on, and prioritise the most important findings first. Measure growth and plot it; look for signs of neglect, dental caries, rickets, and uncorrected vision or hearing; and screen development against age expectations. [2] [3]
Screen for mental-health and trauma difficulty in a developmentally and culturally appropriate way. For younger children use structured parent-report measures; for older children add validated self-report screens for depression, anxiety, PTSD and suicidality, choosing instruments validated for displaced children where available. [13] [2]
Document to protect the child and inform the care team lawfully: record what was found, what was disclosed, who holds guardianship, what was shared and why, and the plan — in language that serves the child at the next service, not only this one. [1] [14]
Investigations
The standard sets a screening bundle for newly arrived children, and examiners expect you to reproduce it. An initial screening on arrival triages acute problems — acute-illness assessment, a mental-health and suicide screen, growth, vision and hearing, dental, and a brief developmental screen. [1] [4]
The comprehensive assessment completes the bundle: growth and puberty, vision and hearing, dental review, developmental and educational screen, mental-health and trauma assessment, sexual-health assessment where age-appropriate, immunisation reconstruction with catch-up, and targeted laboratory testing. [4] [15]
What the comprehensive screening bundle typically covers
The infectious-disease screen addresses the common hidden burdens: tuberculosis with an interferon-gamma release assay or tuberculin skin test, hepatitis B serology (with hepatitis C and HIV where indicated), syphilis serology, schistosomiasis and strongyloides serology where epidemiologically appropriate, stool for ova, cysts and parasites, and a malaria film in any febrile child or one from a malaria-endemic region. Add a full blood count, iron studies, vitamin D, lead level, and a haemoglobinopathy screen for children from endemic regions. Reconstruct the immunisation record from every available source and plan catch-up to the national schedule.
Which mental-health instruments you choose should match the child's age, language and culture. Validated screening and assessment tools for forcibly displaced children exist, and you should arrange formal trauma and developmental assessment whenever symptoms or delay are suspected. [13]
Immunisation reconstruction is a high-yield task. Overseas records are often incomplete, and predeparture vaccination does not always translate to documented protection, so verify and catch up to the national schedule rather than assuming immunity. [11] [4]
Growth, iron and vitamin D data should be interpreted against the history of deprivation and catch-up needs. Faltering growth may reflect pre-arrival deprivation or organic disease; iron and vitamin D deficiency are common, fixable targets; and an elevated lead level requires source identification and repeat testing. [7] [6] [3]
Management — Resuscitation
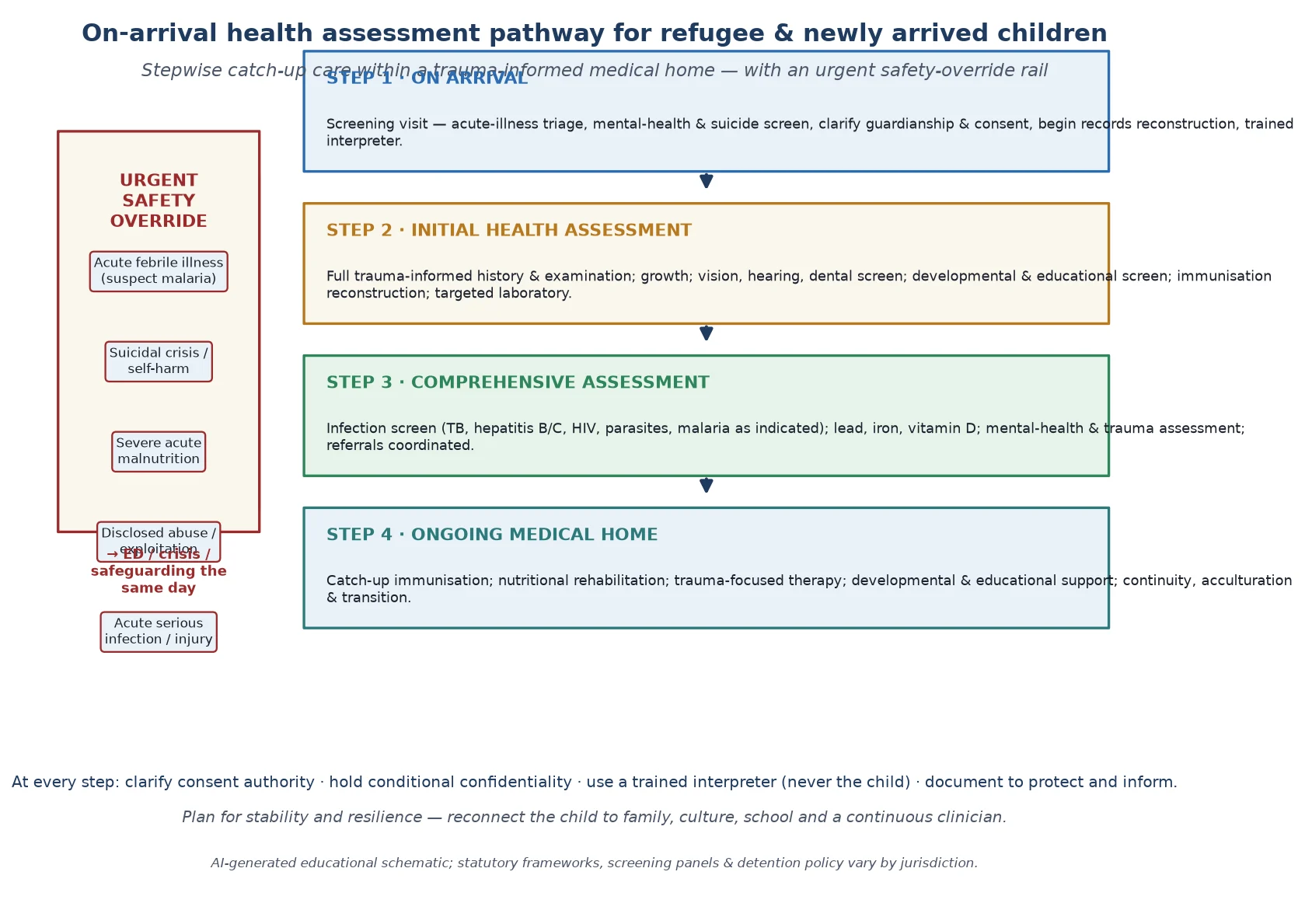
The "resuscitation" step in this topic is the immediate safety override: the things you cannot wait to address at a routine visit. A febrile child from a malaria-endemic region, severe malnutrition, dehydration, sepsis, an acute serious infection, an overdose, self-harm or active suicide risk all exit the routine pathway and trigger same-day ED or crisis activation. [1] [4]
Activate the pathway while preserving the therapeutic relationship. Tell the family what you are doing and why, involve crisis or safeguarding services as required, and stay engaged through the interpreter so the safety action does not read as abandonment. A family that has already lost so much is exquisitely alert to being "passed on." [2] [1]
When guardianship is unclear — most often for an unaccompanied child — and a time-critical decision is pending, act in the child's best interests while you clarify, but clarify and document as fast as you can. Life- or limb-threatening decisions never wait for paperwork, but everything else should follow the documented authority. [1] [15]
Stabilise and treat the acute problem — fever, infection, severe malnutrition or a mental-health crisis — and at the same time begin organising ongoing, language-appropriate care, because the child will leave your acute encounter into a family and a system that must be ready to continue. [4] [3]
A disclosure of abuse, exploitation or trafficking during the assessment is itself a resuscitation-level event: listen, do not interrogate, record the child's own words through the interpreter, and escalate to child-protection services and forensic assessment as the local pathway requires. Your job is to hear and protect, not to investigate. [1]
Management — Definitive & Stepwise
Definitive management is the stepwise on-arrival pathway, delivered through a trauma-informed, interpreter-mediated medical home. The timeline to reproduce is: initial screening on arrival, a structured initial health assessment, a comprehensive multidisciplinary assessment, and an ongoing medical home. [1] [15]
On-arrival health assessment pathway
On arrival
Screening visit — acute-illness triage, mental-health and suicide screen, clarify guardianship and consent, begin records reconstruction with a trained interpreter.
Initial health assessment
Full trauma-informed history and examination; growth; vision, hearing, dental screen; developmental and educational screen; immunisation reconstruction; targeted laboratory.
Comprehensive assessment
Infection screen (TB, hepatitis B/C, HIV, parasites, malaria as indicated); lead, iron, vitamin D; mental-health and trauma assessment; coordinated referrals.
Ongoing medical home
Catch-up immunisation; nutritional rehabilitation; trauma-focused therapy; developmental and educational support; continuity, acculturation and transition.
The written health care plan captures the assessment, the diagnoses, the medications, the immunisation status, the outstanding referrals and the follow-up — and it travels with the child. Specify who receives it so the next service inherits the work, not the void. [1] [14]
Deliver ongoing care as a medical home: the same clinicians, predictable visits, strengths-based reviews, and a single coordinator who holds the plan. Continuity is the treatment, because fragmented acute-only contact reproduces the instability that drove the burden. [1] [2]
Coordinate the multidisciplinary team deliberately — paediatrician, mental-health clinician, infectious-disease and refugee-health service, dental, education and early-intervention services, social work, and the interpreter — because no single clinician can meet the bundle. Name a coordinator and document the shared plan. [4] [15]
Manage mental-health and trauma difficulty with evidence-based, trauma-focused intervention first. Trauma-focused treatments show measurable effectiveness for refugee children with PTSD, so psychological therapy is the foundation; reserve psychotropic medication for defined indications under specialist oversight. [8] [2]
Catch up immunisation, rehabilitate nutrition with the family, and arrange dental, vision and hearing care early — these are concrete, fixable targets that change a child's trajectory and rebuild trust in the health system. [11] [7]
Support acculturation, educational engagement and family reunification, and name the strengths and resilience of the child and family explicitly. Many refugee families show extraordinary resilience, and a strengths-based frame is both clinically accurate and therapeutic. [1] [2]
Specific Subtypes & Scenarios
Infants and young children arriving with a family carry the highest nutritional, developmental and attachment stakes. Prioritise growth and nutrition, developmental screen, immunisation catch-up, and early-intervention referral, and reassess development after stability because a single snapshot undercalls potential. [3] [7]
The unaccompanied or separated child needs above all a clinician who clarifies guardianship, uses a trained interpreter, and does not underestimate the attachment loss. Guardianship governs consent, isolation concentrates the mental-health risk, and a named coordinator and trusted adult are therapeutic. [9] [1]
A child held in immigration detention presents a specific ethical and clinical challenge. Systematic-review and meta-analytic evidence shows that detention harms children's mental and physical health, so the clinician's role includes documentation, advocacy for community-based alternatives, and vigilant health surveillance. [10]
A child from a specific conflict setting — Afghan, Syrian, Sudanese, or others — may carry region-specific infectious-disease, nutrition and trauma considerations, so adapt the screen to the epidemiology of the country of origin and transit. [12] [5]
A child with chronic disease or disability who has had disrupted care needs an especially robust written care plan, medication reconciliation, and a named coordinator — because the cost of a fragmented handover is highest for the most medically fragile child. [3] [1]
An adolescent, including an unaccompanied youth, needs attention to mental health, sexual health and the transition to adult services, with confidential space appropriate to capacity and a plan that does not collapse when immigration status changes. [9] [2]
A child presenting acutely with imported malaria or febrile illness is a resuscitation-level scenario: suspect malaria in any febrile child from an endemic region, investigate and treat urgently, and screen for other imported infections once stable. [4] [5]
A child approaching a stable immigration outcome — granted protection, family reunification, or transition to adult services — needs the health plan locked in before the transition so that continuity, identity and the care plan travel with them. [1] [15]
Complications & Pitfalls
The most common and most easily preventable pitfall is using the child or an untrained family member as interpreter. It inverts family roles, exposes the child to distressing content, and corrupts the accuracy of the history, consent and disclosure. Professional interpreters are the standard, every time. [14] [1]
Fragmented records and care discontinuity cause direct harm: missed immunisation, duplicate or omitted testing, lapsed prescriptions, and a child whose history must be retold at every service. Prevent it by writing a health summary that travels with the child and by naming a coordinator. [3] [11]
Over-medicalising normal distress, or over-diagnosing trauma-driven behaviour as a primary disorder, is a well-described harm. Trauma-driven behaviour is first and foremost an adaptation to adversity, so offer evidence-based, trauma-focused intervention first and reserve psychotropics for defined indications. [8] [2]
[10]Diagnostic overshadowing is the mirror image: a physical illness, a sensory deficit or a developmental need is dismissed as "just stress" or "just the refugee background," and treatable disease is missed. Hold both truths — trauma is real, and so is organic disease — and investigate appropriately. [3] [6]
Failing to screen for imported infections, lead and vitamin D deficiency is a high-yield pitfall. Malaria, tuberculosis, parasites, elevated lead and rickets are common and fixable, and missing them at the on-arrival window delays treatment and prolongs harm. [4] [5]
Failure to clarify guardianship and consent authority creates legal and ethical risk, especially for unaccompanied children, where treating without knowing who holds responsibility is both unsafe and confused. Clarify and document before you act. [1] [15]
Finally, failure to plan for continuity and acculturation leaves a child isolated and disengaged from care. Resettlement without connection to family, school, culture and a continuous clinician squanders the recovery that stability could deliver. [2] [1]
Prognosis & Disposition
Prognosis here means the trajectory of safety, recovery, developmental catch-up, mental-health healing, educational engagement and stable relationships — and it is more modifiable than it looks. Stability, family unity, early mental-health support, school engagement and a continuous medical home all move the trajectory in the child's favour. [2] [1]
Routine disposition is a stable placement, a completed assessment bundle, a shared written care plan, and a child connected to the medical home with routine follow-up. [1]
Early-review disposition is a new disclosure, a placement or housing change, an incomplete assessment, a child still building trust, or an abnormal screening result awaiting confirmation — bring them back in days to weeks, not months. [15] [3]
Urgent disposition is active suicide risk, a febrile child from a malaria-endemic region, disclosed abuse or exploitation, acute psychosis, or medical instability — use ED, crisis or safeguarding pathways the same day. [4] [1]
Safety-net explicitly: who to call tonight, when to come back sooner, and how confidentiality will work with carer and caseworker after any override. Close the loop after mental-health, safeguarding, education or infectious-disease involvement. [1] [14]
Over time, early, trauma-informed, continuous medical-home care improves trajectory compared with fragmented acute-only contact — and the long-term outcomes for resettled refugee children, supported by family unity, education and stability, are far better than the burden at arrival would suggest. [2] [8]
Special Populations
Unaccompanied or separated children. Guardianship, attachment loss and isolation concentrate the risk here, so clarify the appointed guardian or state responsibility, use a trained interpreter, prioritise mental-health screening, and provide a trusted adult and a named coordinator. [9] [1]
Children held in or recently released from immigration detention. Document the health impact, provide vigilant surveillance, and advocate for community-based alternatives, because the evidence shows detention harms children. [10]
Indigenous or minority children within a migrant population. Cultural safety, respect for family and community decision-making, and acknowledgement of the intersection of racism and displacement are essential; racism is a health exposure. [1]
Children with disability, neurodiversity or complex chronic disease. Adapt communication and capacity assessment to ability, use supported decision-making, avoid diagnostic overshadowing, and provide an especially robust written care plan and coordinator. [3]
Infants and young children. Nutrition, attachment and development are most vulnerable here, so prioritise growth and nutrition, developmental screen, immunisation catch-up and early-intervention referral, and reassess after stability. [7] [3]
Adolescents, including unaccompanied youth. Attend to mental health, sexual health and the transition to adult services, with confidential space appropriate to capacity and a continuity plan robust to changes in immigration status. [9] [2]
Rural and remote children. Fragmented service access, interpreter scarcity and small-community dual relationships threaten confidentiality and continuity; create deliberate pathways including telehealth with a private space and remote interpreter access. [1]
Evidence, Guidelines & Regional Differences
The AAP standard. The American Academy of Pediatrics Council on Community Pediatrics clinical report — Linton and colleagues, 2019, "Providing Care for Children in Immigrant Families" — sets the current practice standard: a medical home, screening on arrival, catch-up preventive care, trauma-informed culturally effective care, and recognition that every child, regardless of immigration status, deserves care. [1]
The Canadian evidence-based guidelines. The Canadian Collaboration for Immigrant and Refugee Health guidelines — Pottie and colleagues, 2011 — anchor the screening bundle with evidence-based recommendations for tuberculosis, hepatitis, parasites, malaria, iron, vitamin D and mental health. [4]
The health burden, quantified. Baauw's 2019 systematic review and meta-analysis maps the health needs of refugee children identified on arrival, and the scoping review by Birhane in 2025 confirms the burden across infectious disease, nutrition, mental health and development. [3] [16]
Mental health — the Lancet series. Fazel's 2012 Lancet review establishes the elevated prevalence of mental-health disorder in refugee children resettled in high-income countries, names the cumulative-trauma mechanism, and identifies family unity, stability, school engagement and social support as the protective factors. [2]
Effective treatment. Velu's 2025 systematic review and meta-analysis shows that trauma-focused treatments are effective for refugee children with PTSD — the evidence base for offering trauma-focused therapy as first line. [8]
Sherif et al, 2026 — immigration detention of children
Systematic review and meta-analysis
Population: Children held in or exposed to immigration detention
Key finding
Immigration detention is associated with significant harm to children's mental and physical health, with effects persisting beyond release.
Practice change
Document the health impact, provide vigilant health surveillance, and advocate for community-based alternatives. Detention is never in a child's best interests.
Infectious disease and preventive gaps. Janda's 2020 study of unaccompanied refugee minors documents the yield of comprehensive infectious-disease screening, Joshua's 2013 Australian cohort shows the gaps in predeparture vaccination, and Pezzi's and Sheikh's work establishes elevated lead and vitamin D deficiency as routine screening targets. [5] [11] [6] [7]
Communication and assessment quality. Boylen's 2020 systematic review shows that professional interpreters improve outcomes for hospitalised migrant and refugee children, Verhagen's 2022 review catalogues validated mental-health screening tools for displaced children, and Alustiza's 2025 qualitative study captures the provider experience of initial asylum-seeker health assessments in Europe. [14] [13] [15]
ANZ: Australia operates offshore and onshore detention and community-based alternatives, with state-based refugee-health services and catch-up immunisation; New Zealand uses community-based reception. RCH Melbourne provides refugee-health clinical guidance. UK: the NHS offers initial health assessments for asylum seekers, with local-authority and Home Office pathways; the migrant health guide frames screening and access, and detained families are a recognised harm. US: the AAP immigrant-families clinical report sets the standard; refugee health screening follows CDC guidance, and Medicaid and state coverage frames access; lead and vitamin D screening are routine. Canada: the CCIRH evidence-based guidelines frame screening; provincial refugee-health programmes and the Interim Federal Health Program shape coverage; detention of children is opposed by paediatric bodies.
State the principle and check local law. Do not invent a universal detention policy, a universal screening panel, or a universal immigration pathway — they do not exist, and the local statute and immigration policy govern the operative detail. [1] [4]
Exam Pearls
- Open every answer with trauma-informed principles — safety, trust, choice, collaboration, strengths — then the screening bundle and the interpreter rule. [1] [2]
- Fever plus a malaria-endemic region is malaria until proven otherwise — name it early and treat it as an emergency. [4]
- Lead and vitamin D screening are routine, fixable targets; catch up immunisation to the national schedule. [6] [7] [11]
- Always use a trained interpreter — the single most examinable and most preventable pitfall. [14]
References
- [1]Linton JM, Green A, COUNCIL ON COMMUNITY PEDIATRICS Providing Care for Children in Immigrant Families. Pediatrics, 2019.PMID 31427460
- [2]Fazel M, Reed RV, Panter-Brick C, Stein A Mental health of displaced and refugee children resettled in high-income countries: risk and protective factors. Lancet, 2012.PMID 21835459
- [3]Baauw A, Kist-van Holthe J, Slattery B, et al Health needs of refugee children identified on arrival in reception countries: a systematic review and meta-analysis. BMJ Paediatrics Open, 2019.PMID 31646192
- [4]Pottie K, Greenaway C, Feightner J, et al Evidence-based clinical guidelines for immigrants and refugees. CMAJ, 2011.PMID 20530168
- [5]Janda A, Eder K, Fressle R, et al Comprehensive infectious disease screening in a cohort of unaccompanied refugee minors in Germany from 2016 to 2017: a cross-sectional study. PLoS Medicine, 2020.PMID 32231358
- [6]Pezzi C, Lee D, Kennedy L, et al Blood Lead Levels Among Resettled Refugee Children in Select US States, 2010-2014. Pediatrics, 2019.PMID 30996119
- [7]Sheikh M, Wang S, Pal A, MacIntyre CR, Wood N, Gunesekera H Vitamin D deficiency in refugee children from conflict zones. Journal of Immigrant and Minority Health, 2011.PMID 20198433
- [8]Velu ME, Kuiper RM, Schok M, et al Effectiveness of trauma-focused treatments for refugee children: a systematic review and meta-analyses. European Journal of Psychotraumatology, 2025.PMID 40387621
- [9]Daniel-Calveras A, Baldaqui N, Baeza I Mental health of unaccompanied refugee minors in Europe: a systematic review. Child Abuse & Neglect, 2022.PMID 36095862
- [10]Sherif B, Hocking DC, Asghari-Jafarabadi M, et al Immigration detention of children: a systematic review and meta-analysis of physical and mental health impacts. European Child & Adolescent Psychiatry, 2026.PMID 40864279
- [11]Joshua PR, Smith MM, Koh AS, et al Australian population cohort study of newly arrived refugee children: how effective is predeparture measles and rubella vaccination? Pediatric Infectious Disease Journal, 2013.PMID 22955722
- [12]Abuali M, Navarro I, Baisch M, et al Health Profile of Afghan Pediatric Refugees Resettled to Philadelphia in 2021-2022. Clinical Pediatrics, 2024.PMID 37905725
- [13]Verhagen IL, Noom MJ, Lindauer RJL, et al Mental health screening and assessment tools for forcibly displaced children: a systematic review. European Journal of Psychotraumatology, 2022.PMID 36212114
- [14]Boylen S, Cherian S, Gill FJ, et al Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI Evidence Synthesis, 2020.PMID 32813387
- [15]Alustiza M, Pach S, Yeung S, et al Initial health assessments of children and young people seeking asylum and refugees in Europe: insights from a qualitative study of health care providers. European Journal of Pediatrics, 2025.PMID 40936000
- [16]Birhane BM, Dawson A, Hayen A Health of refugee children upon arrival in high-income countries: a scoping review. Journal of Migration and Health, 2025.PMID 41328262