Paeds · child-safety-and-social-paediatrics
Sexually transmitted infections and child sexual abuse
Also known as Child sexual abuse evaluation · STI as a marker of sexual abuse · Prepubertal STI interpretation · Forensic sexual abuse examination · Sexual assault STI prophylaxis in children · Anogenital examination in suspected abuse
A fellowship approach to sexually transmitted infections (STIs) in the context of child sexual abuse: a trauma-informed, forensic-aware evaluation in which an STI is read as a graded marker of sexual contact rather than a routine infection, with age- and pathogen-specific interpretation of NAAT results, targeted forensic sample collection within the evidence window, STI and HIV post-exposure prophylaxis, mandated reporting across jurisdictions, and multidisciplinary safety planning for ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old presents with vaginal discharge. A swab returns gonorrhoea. The easy, dangerous move is to treat the infection and move on. The fellowship move is to recognise that gonococcal infection at a non-conjunctival site in a prepubertal child is a strong marker of sexual contact, and that the laboratory result is the start of a safeguarding process, not its conclusion. [1] [7]
Child sexual abuse is the involvement of a child in sexual activity that they cannot consent to, do not fully comprehend, or are developmentally unready for, including contact and non-contact acts. Sexually transmitted infections in children must therefore be read along two axes: they are clinical infections to diagnose and treat, and they are forensic signals whose strength as evidence of sexual contact depends on the pathogen, the child's age, and the exclusion of non-sexual transmission. [1] [2]
The central shift in thinking for this topic is that a positive STI test is never an isolated laboratory event in a child. A swab result has to be interpreted against perinatal acquisition (which can persist for years), autoinoculation and fomite transmission, known blood-borne exposure, and the child's disclosure and examination findings before it carries medico-legal weight. [7] [8]
Core sequence of an abuse-and-STI evaluation
Safety first
Confirm the child is safe now; address acute injury, bleeding or suicidality before any planned examination.
Trauma-informed history
Child-led disclosure; never interrogate. Capture perinatal, immunisation, menstrual and pregnancy context.
Targeted examination
General plus anogenital exam in a trained setting, with consent, chaperone and photo-documentation.
Risk-stratified testing
STI testing by age, risk and site; forensic samples if within the evidence window.
Prophylaxis and safety
STI/HIV prophylaxis, emergency contraception, mandated report and multidisciplinary follow-up.
Classification
Classify the clinical question first, then classify each organism by how strongly it points to sexual contact. The first split is between an acute presentation (recent assault, active bleeding or injury, a disclosure within the forensic window) and a non-acute presentation (disclosed days to weeks later, or detected through an incidental STI test), because that split decides whether forensic samples are still worth collecting. [9] [10]
The most useful second frame is pathogen strength — grading each STI as a strong, probable or low-specificity indicator of sexual contact. Gonococcal infection beyond the neonatal period, acquired syphilis, Trichomonas vaginalis in a prepubertal or premenarchal child, and HIV with no credible non-sexual route are strong indicators that trigger a child-protection response. Anogenital warts from HPV in an older child and HSV-2 are probable indicators that demand investigation and exclusion of other routes. Hepatitis B and C, and HPV in infancy, are lower-specificity findings that must be read with the full context. [1] [8]
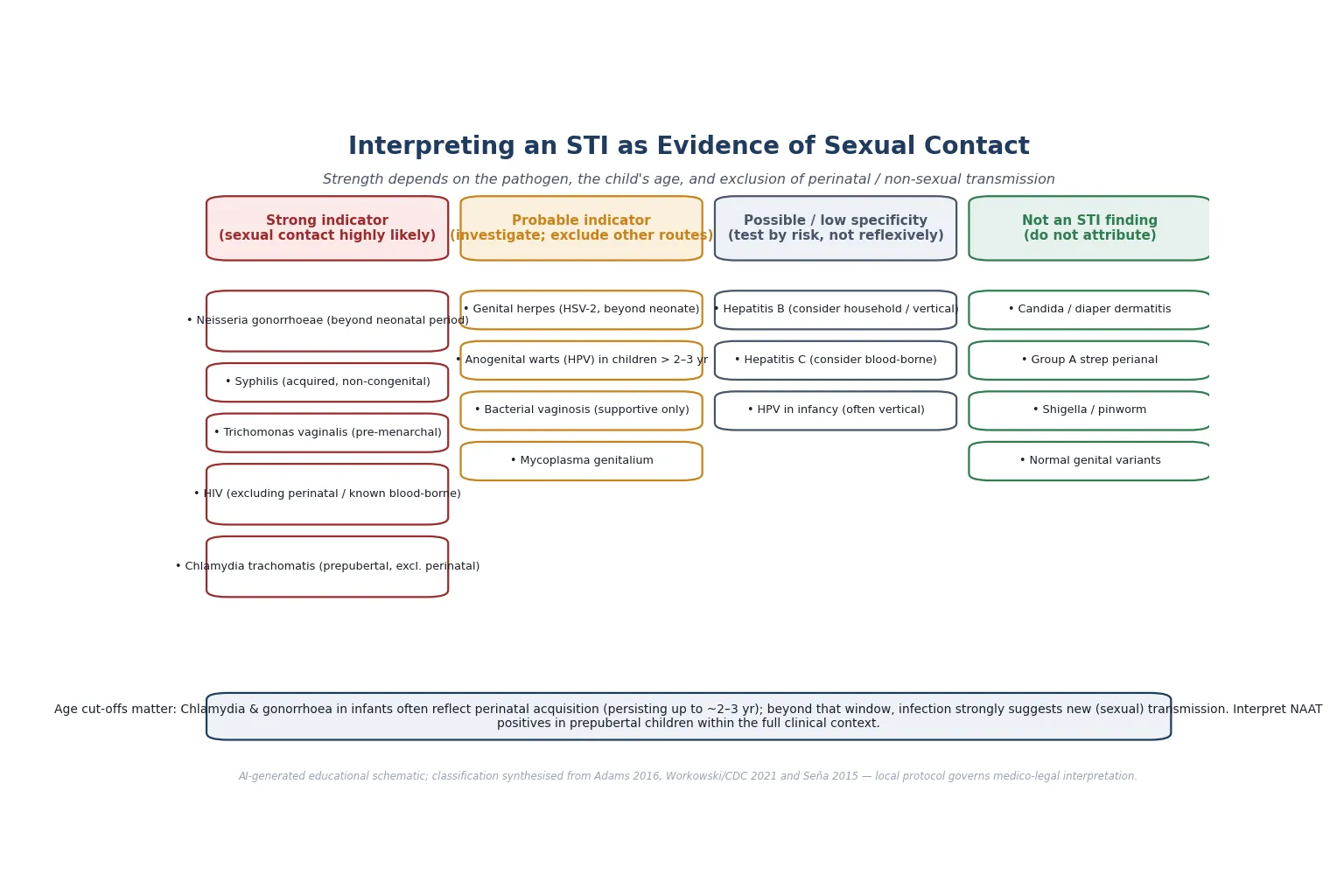
Read the figure like this: the same pathogen changes meaning with the child's age. Chlamydia in a one-year-old may be perinatal; the same organism in a six-year-old is a very different signal. [7]
Acute presentation
Forensic window open
- Recent disclosure or assault
- Active bleeding or injury
- Collect forensic samples early
- PEP timing is critical
Non-acute presentation
Window closed
- Disclosed days to weeks later
- Incidental STI finding
- Examination still valuable
- History and testing drive the case
Incidental STI result
Start of safeguarding
- Positive test prompts the question
- Grade the pathogen
- Exclude non-sexual routes
- Report per local law
Epidemiology & Risk Factors
Sexual violence against children is a global burden. A 2023 Global Burden of Disease analysis estimated the population health loss attributable to sexual violence against children across 204 countries and territories, confirming that this is among the most common and under-reported forms of maltreatment worldwide. [14]
Most abused children disclose late, partially, or not at all. Delayed, incomplete and retracted disclosure is the rule rather than the exception, which is why the absence of a clear story must never be used to dismiss a concerning finding or a positive test. [2] [8]
Risk amplifiers cluster around dependency and isolation: a perpetrator who is a caregiver or has unsupervised access; disability or communication difficulty that limits the child's ability to report; out-of-home care and youth-justice histories with fragmented records; social isolation and socioeconomic disadvantage; and prior maltreatment or domestic and family violence in the home. [2] [12]
The prevalence of STIs in children evaluated for suspected abuse is low overall, but rises sharply when there is a history of penetration, genital injury, or a perpetrator known to be infected. This is why testing is targeted by risk and disclosure detail rather than applied to every evaluated child. [5] [8]
Pathophysiology
A workable mechanism model explains why a positive test in a child has to be interpreted rather than taken at face value. The same organism can reach a child by several routes, and the route decides how seriously the result points to abuse. [7] [8]
Perinatal acquisition is the route clinicians forget most often. Chlamydia trachomatis, Neisseria gonorrhoeae, herpes simplex virus, human papillomavirus, HIV and syphilis can all be acquired at birth from an infected mother, and chlamydia in particular can persist in the nasopharynx and vagina for two to three years. A positive chlamydia NAAT in a toddler therefore requires careful thought about perinatal exposure before it is labelled sexual. [7]
Non-sexual transmission is uncommon but real. Autoinoculation, fomite and skin-to-skin spread can explain some anogenital warts, and household transmission is a recognised route for hepatitis B. These routes must be actively excluded rather than assumed away. [13]
Sexual contact is the route that child-protection investigation exists to assess. When the pathogen, the child's age and the clinical context all align, sexual transmission becomes the most plausible explanation, and the test result moves from a clinical infection into graded forensic evidence. [1] [5]
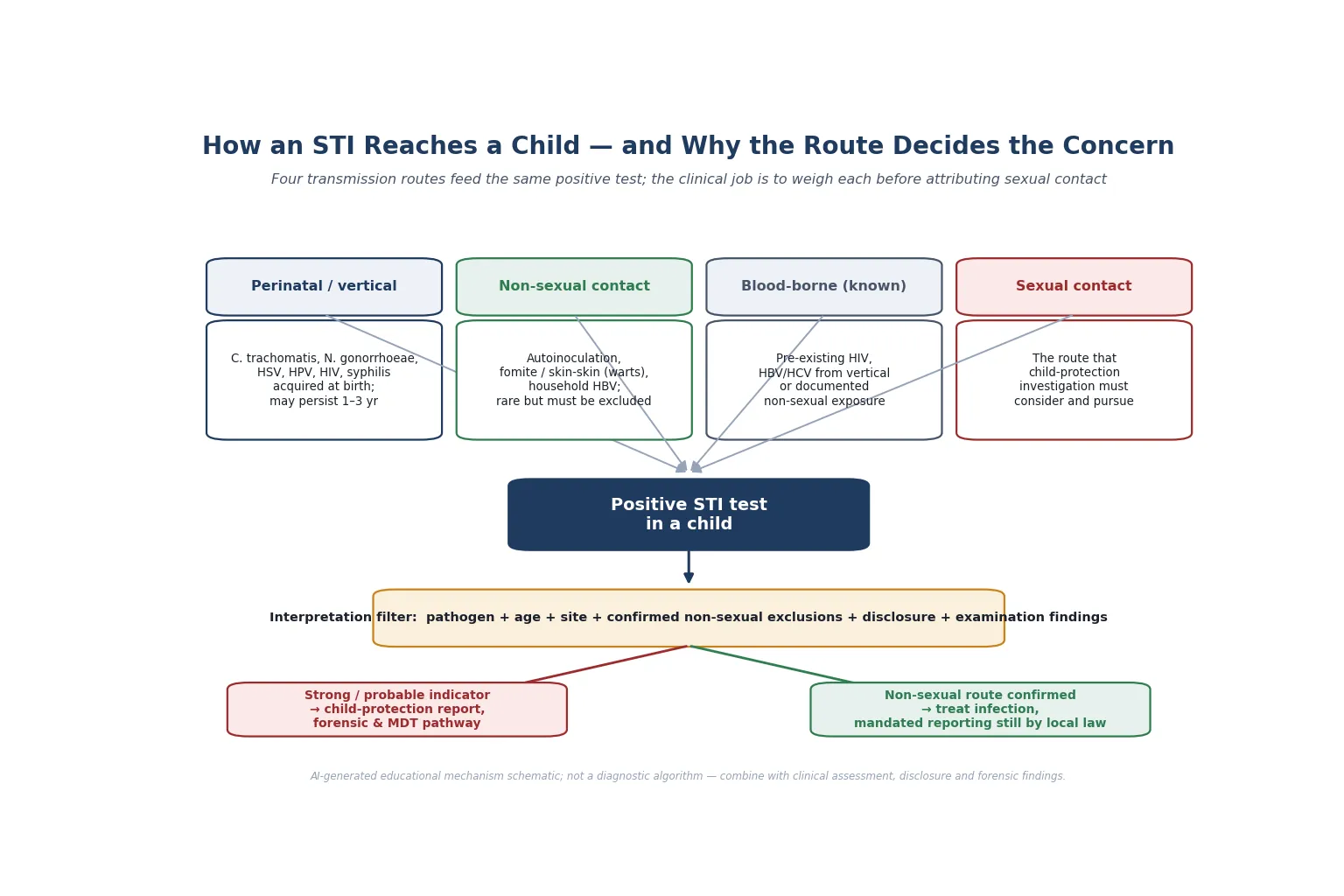
Read the figure like this: the filter in the middle is where your clinical reasoning lives. You cannot read a number off a laboratory form and jump to a conclusion; you must run every positive through the filter. [1]
Clinical Presentation
A child may present through several doors, and the clinician's job is to recognise each one. The most direct is a disclosure of contact, made to a parent, teacher or health worker, that triggers an assessment. The most insidious is an incidental STI finding on a swab taken for discharge, a positive urine NAAT, or a wart noticed at a routine visit. [2] [8]
Symptoms that should prompt questioning include unexplained vaginal or urethral discharge, dysuria, anogenital pain or bleeding, recurrent urinary tract infection, and behavioural change such as sexualised behaviour that is age-inappropriate or persistent. The AAP clinical report on sexual behaviours in children distinguishes normative, common behaviours from those that are concerning and warrant evaluation. [3]
Red-flag presentations are acute anogenital bleeding or injury, a disclosure of penetration, an assault within the forensic window, ongoing access to the child by the alleged perpetrator, and suicidality or acute dissociation at disclosure. Any of these shifts the encounter from a routine assessment to an urgent forensic and safeguarding response. [9] [10]
Differential Diagnosis
In this topic the differential is really a question of attribution: which non-sexual explanation could account for the finding, and has it been properly excluded? [8] [13]
| What it looks like | What else it could be | Must exclude |
|---|---|---|
| Vaginal discharge | Normal physiological secretion, candidiasis, foreign body, shigella, pinworm | STI on NAAT, ongoing access risk |
| Anogenital warts | Vertical HPV transmission (infancy), autoinoculation, lichenoid variants | Abuse when onset in older child, per Awasthi 2021 [13] |
| Genital ulcers | Aphthae, Crohn disease, Stevens-Johnson, trauma | HSV typing, syphilis serology |
| Perianal redness | Candida, group A strep perianal dermatitis, eczema, poor hygiene | STI testing by risk, not reflexively |
| Urethral/vaginal NAAT positive | Perinatal chlamydia persisting (under ~3 yr) | Maternal and perinatal history [7] |
Separate an infection problem (which organism, which site, which treatment) from a safety problem (who has access, is the child at ongoing risk) from a forensic problem (is evidence being preserved). They coexist and each needs its own plan. [5]
Clinical & Bedside Assessment
1. Triage safety and set the trauma-informed frame
Confirm the child is safe right now. If there is acute bleeding, injury or suicidality, stabilise first and escalate to urgent forensic and child-protection pathways. Explain what will happen at the child's pace, obtain consent (and assent where the child can give it), and offer a chaperone for every sensitive examination. [1] [10]
2. Take a trauma-informed history
Let the child disclose in their own words. Do not interrogate, lead or press for detail — forensic interviewing belongs to trained child-protection interviewers. Capture the perinatal and maternal history, immunisation status, any bleeding disorder, menstrual and pregnancy status for post-menarchal adolescents, and the timeframe of any alleged contact, because this drives the forensic window. [2] [10]
3. Perform a targeted examination in a trained setting
A general examination precedes a focused anogenital examination, performed by a clinician with paediatric forensic training using a colposcope where available. Findings are documented and, with consent, photographed, and interpreted against established normal variants and accidental injury patterns. Most substantiated abuse shows a normal or non-specific examination, so the examination is one data source among several. [1] [15]
4. Choose STI testing by age, risk and site
Order NAATs at the sites that match the history and the child's developmental stage, and add serology (syphilis, HIV, hepatitis) where the risk profile warrants it. Interpret any positive NAAT in a prepubertal child through the perinatal-acquisition and non-sexual-route lens before drawing conclusions. [7] [4]
5. Document with forensic discipline
Record consent, examination findings, photographs and sample chain of custody contemporaneously. Medico-legal notes may be read in court years later, so factual, non-leading, time-stamped documentation protects both the child and the integrity of any subsequent investigation. [1] [15]
Investigations
Testing is targeted, never reflexive. The decision to test rests on the child's age, the nature of the alleged contact, the presence of symptoms or injury, and the known infection status of the alleged perpetrator. [5] [8]
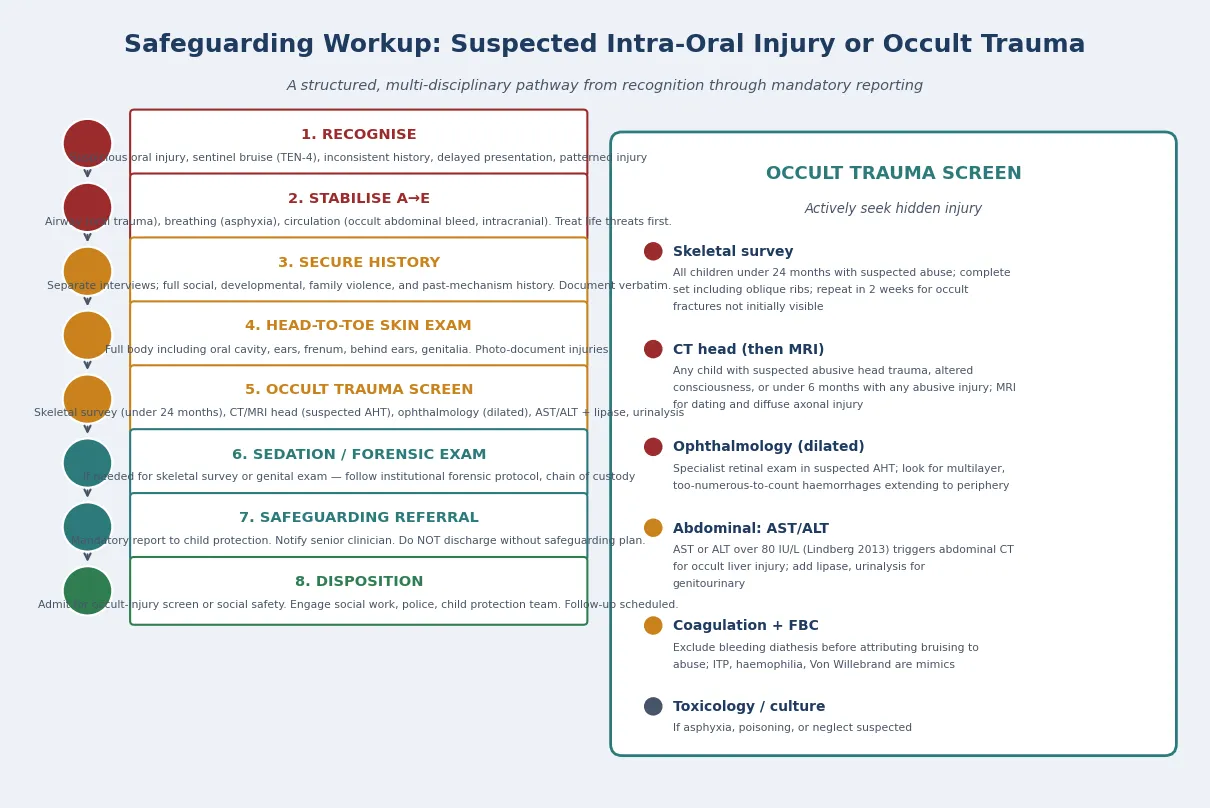
Often indicated are NAATs for Chlamydia trachomatis and Neisseria gonorrhoeae from the sites that match the history (vaginal, urine, rectal, pharyngeal as appropriate), with culture confirmation considered when a NAAT is positive in a prepubertal child, because culture has historically carried more medico-legal weight. Syphilis, HIV and hepatitis serology are added by risk. A pregnancy test is offered to post-menarchal adolescents. [4] [7]
Forensic samples are collected when the child presents within the evidence window after an acute assault. Christian and colleagues showed that forensic evidence yield in prepubertal victims is heavily concentrated in the first hours after assault, and more recent work supports DNA recovery beyond 24 hours in selected cases — but the window is short, so the decision to collect is time-critical. [9] [11]
Low-value patterns to avoid are reflexive full STI panels on every evaluated child, repeating NAATs without indication, relying on a single non-validated test, and delaying safety to wait for results. Cultures and serologies take days; safeguarding decisions cannot. [4] [5]
Management — Resuscitation
A suspected-abuse assessment can become a medical or psychological emergency at the point of disclosure. Recognise the pivot and act before returning to the planned evaluation. [1] [10]
- Stabilise physiology if there is acute anogenital injury, uncontrolled bleeding, acute suicidality or self-harm, or haemodynamic compromise. [9]
- Preserve forensic evidence: advise against washing, bathing or changing clothing, retain any clothing and collect samples within the evidence window, with chain of custody. [9] [11]
- Secure immediate safety: do not discharge the child to the care of the alleged perpetrator; involve child protection, social work and, where indicated, police and crisis mental-health services. [2] [1]
- Address immediate infection and pregnancy risk: begin STI prophylaxis, assess HIV post-exposure prophylaxis against source status and timing, offer emergency contraception to post-menarchal adolescents, and update hepatitis B vaccination where indicated. [4] [6]
Management — Definitive & Stepwise
Read the figure like this: the red bar is an interrupt, not a decoration. Any red-flag feature exits the routine pathway into an urgent forensic and safety response. [10]
Stepwise pathway
- Triage and safety, then consent and a trauma-informed pace. [1]
- History that is child-led, with perinatal, immunisation, menstrual and pregnancy context. [2]
- Targeted examination in a trained setting with photo-documentation. [1]
- Risk-stratified testing by age, risk and site; forensic samples if within window. [7] [9]
- Prophylaxis and treatment: STI prophylaxis, HIV PEP by risk and timing, emergency contraception, hepatitis B cover. [4] [6]
- Safety, mandated report and follow-up: child-protection notification, multidisciplinary care, psychosocial support and re-test intervals. [2] [12]
STI prophylaxis & HIV PEP after sexual assault/abuse — principle only
Dose
Refer to your current jurisdictional guideline and product information for the regimen, timing window and weight-based dosing
Re-testing and follow-up
Schedule repeat serology and re-testing at the intervals your local protocol sets, because infections acquired near the time of assault may be in the window period at first test. Coordinate with child-protection, mental-health and primary-care services so the child is not lost between them. [4] [5]
Specific Subtypes & Scenarios
Prepubertal child with gonococcal infection. This is a strong marker of sexual contact once perinatal acquisition is excluded, and it triggers a child-protection report and a full evaluation regardless of the presence or absence of disclosure. [1] [7]
Anogenital warts in a young child. Awasthi and colleagues found a substantial association between anogenital warts in children beyond infancy and child sexual abuse, but vertical transmission remains a credible explanation in the first years of life. Each case is assessed individually with the full context. [13]
Acute assault within the forensic window. Move quickly to preserve evidence, collect forensic samples early, and assess HIV PEP and STI prophylaxis against source status and timing. The first hours after assault carry the highest forensic yield. [9] [11]
Adolescent disclosure of assault. Add pregnancy prevention (emergency contraception and ongoing contraception options), confidentiality framed within safety limits, and trauma-informed mental-health follow-up. [4] [5]
Child with disability or communication difficulty. Use accessible communication, longer appointments, a trusted support person, and a high index of suspicion, because disclosure is harder and diagnostic overshadowing is a recognised risk. Capacity and consent are assessed properly, never assumed. [2]
Out-of-home care and youth-justice settings. Assume fragmented records, repeated exposures and complex consent. Reconstruct the history actively and clarify legal consent and carer authority for the placement context. [2] [12]
Complications & Pitfalls
- Treating an STI in a child as a routine infection and never considering sexual contact. [1]
- Interpreting a prepubertal chlamydia or gonorrhoea NAAT without weighing perinatal acquisition. [7]
- Missing the forensic window by deferring sample collection for administrative reasons. [9] [11]
- Concluding abuse from a single low-specificity finding (hepatitis, infantile HPV). [13]
- Over-relying on a normal examination to exclude abuse, when most substantiated cases are non-specific. [1] [2]
- Failing to make a mandated report because the disclosure was delayed or retracted. [2]
- Not offering HIV PEP or emergency contraception because of clinician discomfort or delay. [6] [4]
- Discharging a child into the care of the alleged perpetrator because the test is pending. [1]
- Promising the child absolute secrecy, which the mandatory-reporting duty will then break. [2]
- Losing the child to follow-up between child-protection, mental-health and primary care. [12]
Prognosis & Disposition
Prognosis here spans infection outcome, immediate safety, and long-term psychological health. Most STIs are treatable, but the enduring harm of child sexual abuse is psychological and developmental. [12]
An umbrella review by Hailes and colleagues confirmed strong associations between childhood sexual abuse and a range of long-term mental-health outcomes, which is why every confirmed or strongly suspected case needs trauma-informed psychological follow-up, not only infection management. [12]
Routine disposition is a completed evaluation, treatment started, child-protection notification made, and follow-up booked. Early-review disposition is for new symptoms, positive results needing treatment, prophylaxis side-effects, or psychological distress. Urgent disposition is acute injury, suicidality, ongoing danger, or a strong-marker STI with no safeguarding plan — escalate and do not discharge. [1] [2]
Close the loop with child-protection, mental-health and primary-care services, and name the next concrete contact so the child and family are not lost between them. [12]
Special Populations
Indigenous children and families. Deliver culturally safe care, address racism and intergenerational trauma as health exposures, connect to community-controlled services, and respect that disclosure and safety sit within kinship and cultural context. [2]
Migrant and refugee children. Use professional interpreters (never family members) for sensitive content, apply trauma-informed pacing, and be alert to different legal frameworks and to experiences of violence in transit. [2]
Out-of-home care and youth justice. Assume fragmented records and higher risk, reconstruct history actively, and clarify legal consent and carer authority for the placement context. [12]
Children with disability and neurodiversity. Use accessible materials and communication, assess capacity properly, offer a trusted support person, and maintain a high index of suspicion — diagnostic overshadowing can mask both disclosure and need. [2]
Socioeconomic disadvantage and rural/remote children. Address transport, cost and access barriers, and use telehealth linkages to specialist forensic services where local expertise is limited, while preserving privacy and continuity. [2]
Evidence, Guidelines & Regional Differences
Consensus medical-assessment guidelines. The Adams-led updated guidelines for the medical assessment and care of children who may have been sexually abused remain the operational backbone for examination, documentation and interpretation, building on the earlier 2007 guideline set. [1] [15]
AAP clinical reports. The AAP Committee on Child Abuse and Neglect clinical report on the evaluation of sexual abuse in children, and its companion on the evaluation of sexual behaviours in children, frame the paediatric approach across disclosure, examination and behavioural interpretation. [2] [3]
STI treatment and prophylaxis. The CDC Sexually Transmitted Infections Treatment Guidelines govern organism-specific therapy and the sexual-assault prophylaxis approach, while Seña and colleagues provide a comprehensive review of sexual assault and STIs across adults, adolescents and children. [4] [5]
HIV post-exposure prophylaxis. Girardet and colleagues describe the use and practical challenges of HIV PEP in children and adolescents presenting after reported sexual assault, informing risk-and-timing decisions. [6]
NAAT interpretation. Hammerschlag's review of nucleic acid amplification tests in investigating child sexual abuse underpins the age- and route-aware interpretation of NAAT positives in prepubertal children, complementing Bechtel's overview of sexual abuse and STIs. [7] [8]
Forensic evidence and timing. Christian and colleagues established that forensic evidence yield in prepubertal victims concentrates in the early hours after assault, with the timing-of-examination review framing how medical examination fits the broader investigation. Hornor and colleagues extend this by demonstrating DNA recovery benefit beyond 24 hours in selected cases. [9] [10] [11]
Anogenital warts. The systematic review and meta-analysis by Awasthi and colleagues quantifies the relationship between anogenital warts and child sexual abuse, calibrating how this finding should be weighed. [13]
Long-term outcomes and burden. Hailes and colleagues' umbrella review of long-term outcomes of childhood sexual abuse, and the GBD 2023 analysis of the global burden of sexual violence against children, ground the prognosis and public-health framing of the topic. [12] [14]
ANZ: state and territory mandatory-reporting laws govern the duty to report; specialist child-protection and forensic medical services (often through children's hospital networks and RCH-linked pathways) conduct evaluations; RCH clinical guidelines support STI and prophylaxis decisions. UK: NICE NG76 frames recognition, assessment and management of child abuse and neglect; multi-agency safeguarding under local safeguarding partnerships; RCPCH guidance on child protection medical examinations and Gillick/Fraser competence for adolescent consent. US: CDC STI Treatment Guidelines and the AAP clinical reports drive evaluation and prophylaxis; state-specific mandatory-reporting statutes; sexual assault nurse examiner (SANE) and child-abuse paediatrician pathways for forensic examination. Canada: provincial child-protection legislation and CPS/RCPSC-aligned child-abuse paediatrics pathways; regional sexual-assault treatment centre protocols govern prophylaxis and HIV PEP.
Exam Pearls
- Open every answer with safety first — acute injury, suicidality and ongoing perpetrator access take precedence over routine assessment. [1] [9]
- Read an STI as graded evidence: gonorrhoea, syphilis, Trichomonas and HIV are strong indicators once non-sexual routes are excluded. [1] [7]
- Perinatal acquisition of chlamydia can persist for years — never interpret a prepubertal NAAT without this context. [7]
- A normal examination does not exclude abuse; most substantiated cases are non-specific. [1] [2]
- Disclosure is often delayed, partial or retracted — its absence never overrides a concerning finding or a strong-marker STI. [2]
- The forensic window is short: preserve evidence and collect early, even though DNA may recover beyond 24 hours. [9] [11]
- Offer HIV PEP and emergency contraception by risk and timing; do not let clinician discomfort cause delay. [6] [4]
- Make the mandated report your jurisdiction requires — never promise the child absolute secrecy. [2]
- Photograph and document against normal variants with consent and chain of custody; your notes may be read in court. [1] [15]
- Confirm anogenital warts against the Awasthi meta-analysis: associated with abuse beyond infancy but vertical in the early years. [13]
SAFEGUARD framework
References
- [1]Adams JA, Kellogg ND, Farst KJ, Harper NS, Palusci VJ, Frasier LD Updated Guidelines for the Medical Assessment and Care of Children Who May Have Been Sexually Abused. J Pediatr Adolesc Gynecol, 2016.PMID 26220352
- [2]Kellogg N, American Academy of Pediatrics Committee on Child Abuse and Neglect The evaluation of sexual abuse in children. Pediatrics, 2005.PMID 16061610
- [3]Kellogg ND, Committee on Child Abuse and Neglect, American Academy of Pediatrics Clinical report--the evaluation of sexual behaviors in children. Pediatrics, 2009.PMID 19720674
- [4]Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep, 2021.PMID 34292926
- [5]Sena AC, Hsu KK, Kellogg N, Girardet R, Christian CW, Linden J Sexual Assault and Sexually Transmitted Infections in Adults, Adolescents, and Children. Clin Infect Dis, 2015.PMID 26602623
- [6]Girardet RG, Lemme S, Biason TA, Bolton K, Lahoti S HIV post-exposure prophylaxis in children and adolescents presenting for reported sexual assault. Child Abuse Negl, 2009.PMID 19324415
- [7]Hammerschlag MR Use of nucleic acid amplification tests in investigating child sexual abuse. Sex Transm Infect, 2001.PMID 11402219
- [8]Bechtel K Sexual abuse and sexually transmitted infections in children and adolescents. Curr Opin Pediatr, 2010.PMID 19952927
- [9]Christian CW, Lavelle JM, De Jong AR, Loiselle J, Brenner L, Joffe M Forensic evidence findings in prepubertal victims of sexual assault. Pediatrics, 2000.PMID 10878156
- [10]Christian CW Timing of the medical examination. J Child Sex Abus, 2011.PMID 21970643
- [11]Hornor G, Benzinger E, Doughty K, Hollar J, Wolf K Pediatric Forensic Analysis: The Benefits of DNA Collection Beyond 24 Hours. J Forensic Nurs, 2022.PMID 35149664
- [12]Hailes HP, Yu R, Danese A, Fazel S Long-term outcomes of childhood sexual abuse: an umbrella review. Lancet Psychiatry, 2019.PMID 31519507
- [13]Awasthi S, Ornelas J, Armstrong A, Johnson JA, Eisen DB Anogenital warts and relationship to child sexual abuse: Systematic review and meta-analysis. Pediatr Dermatol, 2021.PMID 34060139
- [14]GBD 2023 Intimate Partner Violence and Sexual Violence against Children Collaborators Disease burden attributable to intimate partner violence against females and sexual violence against children in 204 countries and territories, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet, 2026.PMID 41386261
- [15]Adams JA, Kaplan RA, Starling SP, Mehta NH, Finkel MA, Botash AS Guidelines for medical care of children who may have been sexually abused. J Pediatr Adolesc Gynecol, 2007.PMID 17561184