Paeds · child-safety-and-social-paediatrics
Trauma-informed examination and forensic documentation
Also known as Trauma-informed forensic medical examination · Forensic documentation in child maltreatment · Child protection medical examination · Medico-legal examination of the child · Trauma-informed paediatric assessment
A fellowship approach to performing a trauma-informed medical examination of a child who may have been maltreated and to documenting the findings so the record is contemporaneous, objective and court-admissible: setting the tempo and the environment, running a single trained forensic interview, conducting the consented and chaperoned examination, capturing photo-documentation, maintaining chain of custody, separating fact from opinion, and handing the whole bundle to the safeguarding and reporting systems that act on it.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old boy is brought to the emergency department at midnight by a foster carer after he disclosed being hit. The triage nurse asks you what happens next. Your job at that moment is not to decide whether abuse occurred. Your job is to run a safe, staged assessment that protects the child, preserves any time-limited evidence, treats what can be treated, and produces a record that the child-protection and police systems can act on — all without making the child tell their story more times than is strictly necessary. [1] [5]
Trauma-informed examination is the application of trauma-informed care to the medical encounter with a child who may have been maltreated. The Substance Abuse and Mental Health Services Administration frames trauma-informed care around six principles — safety, trustworthiness and transparency, peer support, collaboration and mutuality, empowerment and choice, and awareness of cultural, historical and gender issues — and each one has a concrete operational meaning at the bedside. Safety means a quiet, private room and a calm, predictable examiner. Choice means telling the child they can stop the examination at any time. Transparency means explaining what you will do before you do it. [1] [2]
Forensic documentation is the second product of that encounter, and it is what separates a clinical visit from a medico-legal examination. The record must be contemporaneous, objective, and structured so that a court can read what was observed, what the child said in their own words, and what the clinician inferred — each clearly distinguished. A note written from memory hours later, or an opinion blended into a factual description, collapses under cross-examination and can cost a child their protection. [6] [7]
The single most important clinical rule is that re-traumatisation is itself a harm, and avoiding it is part of the treatment. A child who is examined repeatedly, questioned suggestively, or rushed through an unexplained procedure is not merely distressed in the moment — the encounter encodes as a further traumatic memory, fragments their recall, and worsens their long-term outcomes. Minimising the number of times the child must tell their story is therefore a clinical objective, not a courtesy. [1] [3]
Classification
The first decision in any forensic examination is the tempo: is this an acute presentation inside the forensic evidence window, or a non-acute disclosure that is elective and unhurried? Everything downstream — the setting, the urgency, whether a forensic kit is taken, how the team is mobilised — flows from that single call. [5]
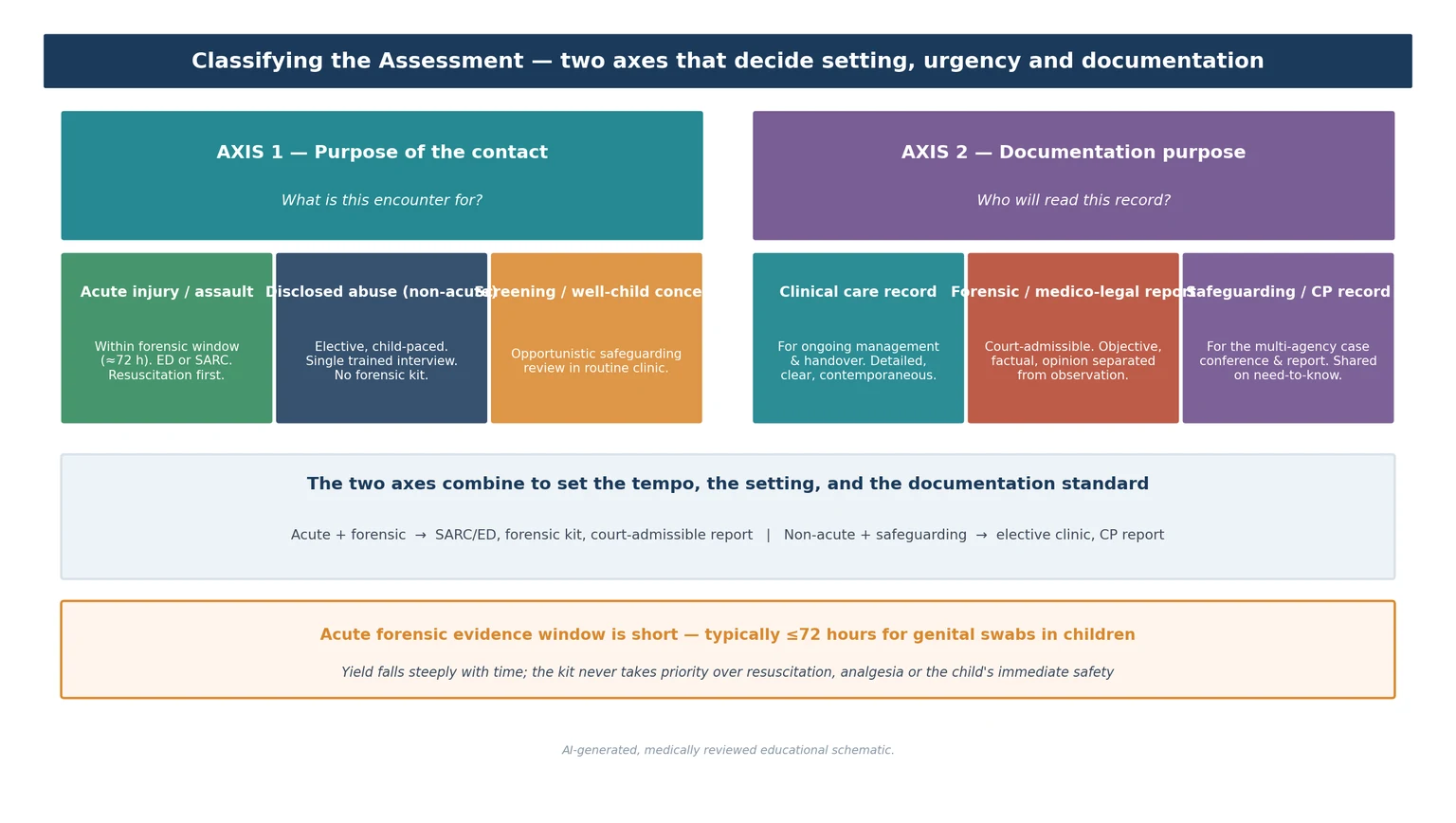
The second useful axis is the purpose of the documentation. A clinical care record guides ongoing management and handover. A forensic medico-legal report is written for a court and must be objective, factual, and must separate opinion from observation. A safeguarding record feeds the multi-agency case conference and is shared on a need-to-know basis. The three overlap but demand different disciplines, and confusing them is how clinicians write notes that help no one. [6] [7]
Acute (<72 h)
Time-critical
- Forensic evidence kit while the window is open
- Resuscitation and analgesia take priority over the kit
- STI baseline and post-exposure prophylaxis as indicated
- Dedicated SARC or child-protection setting
- Court-admissible report issued within the deadline
Non-acute
Elective
- Most referrals — disclosure is usually delayed
- Unhurried, child-paced examination
- Forensic kit rarely useful
- Focus on history, photo-documentation, STI testing
- Safeguarding record and therapy planning central
Screening concern
Opportunistic
- Built into a routine clinic or foster-care health check
- Create the conditions for disclosure, do not hunt for injury
- Examine for sentinel injuries and neglect
- Document concerns and refer onward
- Never dismiss a tentative disclosure as 'just a hint'
A third axis the examiner may press is the type of maltreatment suspected: physical abuse with cutaneous or skeletal injury, sexual abuse requiring anogenital examination, neglect or supervisory failure, or emotional and psychological abuse. Each carries its own examination focus, its own set of findings to document, and its own differential to exclude. The shared spine is the trauma-informed approach and the documentation standard, which is why this topic sits across all of them. [5]
Epidemiology & Risk Factors
Child maltreatment is common, and the children who experience it are over-represented in every paediatric setting. A minority of abused children ever reach a dedicated child-protection service, which is why the general paediatrician, the emergency clinician, and the community nurse are the de facto front line. The scale of the problem is the reason every clinician who sees children must be competent in the trauma-informed examination, not only the subspecialist. [1] [3]
Trauma exposure of any kind — not only maltreatment — is itself a risk factor for poor engagement with healthcare, for fragmented recall during a stressful examination, and for the emotional dysregulation that can make a child appear uncooperative or indifferent. Recognising that a frozen, mute, or apparently indifferent child is displaying a threat response, rather than refusing to engage, is the clinical skill that lets you adjust the encounter rather than abandon it. [4]
Risk of a poor forensic outcome clusters in predictable places. Children examined by clinicians without child-protection training, children who are interviewed multiple times by different agencies, children whose accompanying adult is the suspected perpetrator and is not separated, and cases where documentation is delayed or opinion is conflated with fact — these are the cases where the medical evidence fails to protect. Forensic medical results influence law-enforcement action most when the examination is timely, the documentation is meticulous, and the chain of custody is intact. [7]
Pathophysiology
Understanding the neurobiology of trauma is what turns a well-meaning examination into a trauma-informed one, because it explains why a frightened child freezes, fragments their account, and disengages — and why a calm, explained, paced encounter recovers both their cooperation and their memory. [1] [4]
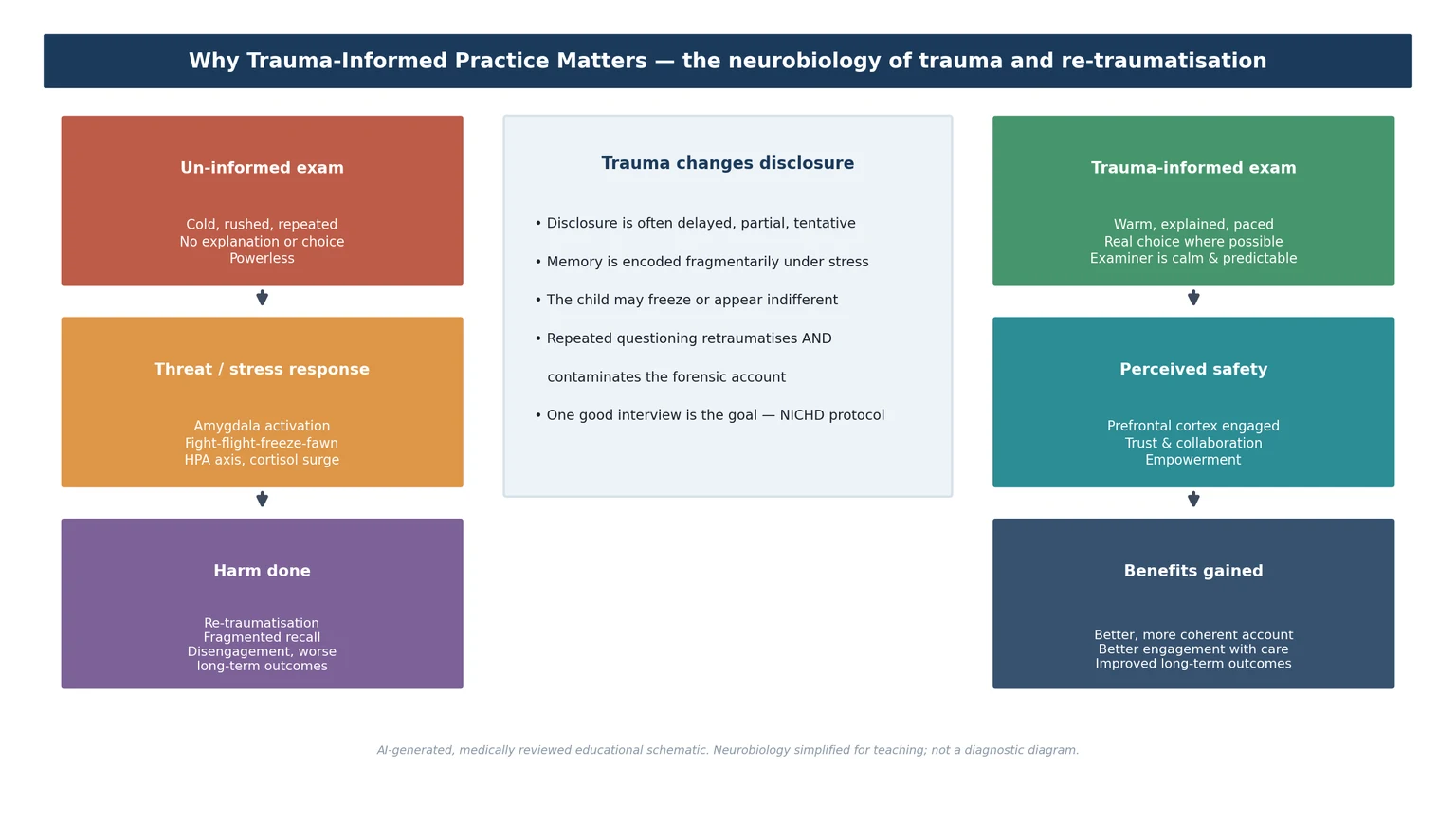
Under acute threat the amygdala drives the familiar fight, flight, freeze, fawn cascade and the hypothalamic-pituitary-adrenal axis releases a cortisol surge. The prefrontal cortex — the seat of deliberate, verbal, organised recall — is suppressed in favour of survival. This is why a frightened child cannot give a tidy chronological history, why they may freeze or appear indifferent, and why pushing harder does not yield more information. It yields less, and it encodes the encounter as a further trauma. [4]
A trauma-informed encounter works because it restores enough perceived safety for the prefrontal cortex to come back online. A calm, predictable examiner, an explanation of what will happen, a genuine offer of choice, and permission to stop all reduce the threat signal. The child becomes able to think, to speak, and to cooperate — and the account they give is more complete and more accurate. The same principle is why repeated questioning both retraumatises and contaminates the evidence: each suggestive prompt overwrites the original memory. [1] [6]
Answer
A child who goes still, silent and apparently compliant during an examination is not "fine with it". Freezing is a threat response, and apparent compliance under dissociation is one of the most dangerous things to misread, because the clinician proceeds while the child is being harmed. Slowing down, naming what you see ("you've gone very quiet — we can stop if you need to"), and giving a real exit restores agency and is the correct response. [1] [4]
Clinical Presentation
Children who need a forensic examination arrive in three ways, and the arrival shapes the assessment. The first is an acute presentation — a child brought in within hours of an assault or an inflicted injury, often distressed, sometimes injured, and inside the forensic evidence window. The second is a non-acute disclosure — a child who tells someone days, weeks or months later, referred electively for assessment. The third is a concern raised by a professional — a teacher, a foster carer, a health visitor — without a clear disclosure, where the task is to create the conditions for a disclosure rather than to hunt for an injury. [5] [11]
The presentation of trauma itself is the one examiners most often mishandle. A maltreated child may be hypervigilant, flattened, dissociated, or developmentally regressed. They may flinch at approach, avoid eye contact, or become selectively mute. None of these are signs that the child is "difficult" or "unreliable"; they are signs of a nervous system primed by threat. Reading them correctly — and adjusting the pace and the approach accordingly — is the clinical skill this topic is built around. [1] [4]
Acute presentation
Inside the window
- Distressed, sometimes injured, within ≈72 hours
- Resuscitation and analgesia first
- Forensic kit, STI bundle, safety plan in sequence
- Court-admissible report required
Non-acute disclosure
Elective
- Disclosure delayed by days, weeks or years
- Child may be calm or flattened
- Unhurried, child-paced examination
- Photo-documentation and STI testing over kit
Professional concern
No disclosure yet
- Teacher, carer or health visitor worried
- Build rapport; do not force a disclosure
- Examine for sentinel injuries and neglect
- Document concerns; refer to trained interviewer
The accompanying adult is part of the presentation, and reading them is part of the assessment. A carer who is supportive and appropriately distressed is different from one who is controlling, who answers for the child, who refuses to leave, or who is vaguely hostile. A controlling adult who will not be separated from the child may be the perpetrator, and the refusal to allow privacy is itself a red flag that must change how the encounter is run. [5]
Differential Diagnosis
In a forensic examination the "differential" is less a list of diseases and more a disciplined separation of inflicted from accidental, and of normal variant from pathological finding. The wrong label is catastrophic in either direction — missing abuse endangers a child, and over-calling a benign variant or an accidental injury destroys a family. [5] [11]
Accidental injury
History fits
- Clear, consistent mechanism (straddle, fall)
- Injury distribution matches the mechanism
- Pattern of bruising on bony prominences
- Documented, timely presentation
Inflicted injury
Concerning pattern
- Bruising in non-mobile infants
- Patterned marks, bites, grip marks
- Injury distribution not explained by the history
- Inconsistent or evolving history
Normal variant
Do not over-call
- Mongolian spots, striae, benign rashes
- Midline posterior hymenal notch
- Urethral prolapse, vestibular band
- Resolve the mimic before labelling abuse
Medical mimic
Bleeding / skin
- Coagulopathy, immune thrombocytopenia
- Lichen sclerosus, atopic dermatitis
- Staphylococcal scalded skin
- Culture-confirmed infection before STI label
Two principles resolve most of the differential. First, the history must fit the finding: a straddle mechanism that explains a labial contusion is reassuring, while the same finding with no plausible mechanism is not. Second, the location and pattern discriminate: inflicted cutaneous injury appears in unexpected places (bruises on the ears, neck, torso, or in a non-mobile infant), while accidental injury clusters on bony prominences consistent with a fall. The forensic documentation must record both the finding and the offered explanation, and must record them separately from the clinician's opinion. [5]
The most dangerous error is to document a finding as "consistent with abuse" when it is non-specific. Most cutaneous and anogenital findings in confirmed abuse are normal or non-specific, which is why the disciplined separation of observation, offered history, and clinical opinion is what protects both the child and the integrity of the record. [5] [7]
Clinical & Bedside Assessment
The assessment is trauma-informed and child-paced from the moment the child arrives, and it follows a fixed order that every fellowship candidate must be able to recite under pressure. The setting is quiet, private and child-friendly. The examiner is competent and supported by a chaperone. The child is told what will happen and given genuine choices where they exist. Every effort is made to minimise the number of times the child must tell their story, because each repeat is both a re-traumatisation and a contamination of the account. [1] [5]
The trauma-informed forensic examination, in order
Safety first — resuscitate, analgesia, separate the child from the suspected perpetrator
Prepare the environment, team and consent before the child enters the room
State the limits of confidentiality honestly, including mandatory reporting
Single forensic interview by a trained interviewer (NICHD protocol) — the clinician listens
General examination: growth, skin, sentinel injuries, signs of neglect
Focused examination only if indicated, child-paced, top-to-toe, with permission at each step
Colposcopy with photo-documentation, with explicit and separate consent for the images
Contemporaneous documentation: verbatim history, observed findings on body diagrams, opinion separate
Forensic samples with a continuous chain of custody if within the window
Safety planning, mandatory report, and disposition before the child leaves
The forensic interview is the heart of the assessment, and the clinician's role in it is deliberately constrained. A trained interviewer uses a structured protocol — the National Institute of Child Health and Human Development Investigative Interview Protocol is the best-evidenced — that opens with rapport-building and open-ended narrative and only later, if at all, moves to focused questions, deliberately avoiding leading or suggestive prompts. The medical clinician should not re-interview the child about the detail of the abuse. One good interview is the goal, because repeated and suggestive questioning both contaminates the evidence and distresses the child. [6]
The physical examination is technique-dependent and must be done by a competent examiner. For a cutaneous examination the child is examined top-to-toe with every surface inspected and every injury documented on a body diagram with a scale. For an anogenital examination the standard position is supine frog-leg with labial separation then traction, adding the knee-chest position when the hymen is not adequately seen. Colposcopy provides magnification and the means to capture images for peer review. The child is told what will happen, given permission to stop, and never held down. [5] [11]
In Australia and Aotearoa New Zealand, forensic examinations are performed by clinicians with child-protection training, often through a dedicated Sexual Assault Referral Centre, a paediatric forensic medical service, or a child-protection unit, with remote peer review where local expertise is limited. Mandatory reporting of a reasonable belief of child abuse applies to all registered medical practitioners, and the threshold is belief, not proof. [5]
Investigations
Investigations in a forensic examination serve three purposes: to address acute medical needs, to detect infection or injury, and to preserve evidence. They are chosen by the timing of the alleged contact, the type of maltreatment suspected, and the child's developmental stage — never sent as a blanket panel. Blood-borne virus testing and repeat serology are timed to incubation and seroconversion windows. [5] [7]
Forensic kit
Only if within window
- Collected when the alleged contact is within the forensic window (typically ≤72 h)
- Swabs for semen, sperm, DNA; clothing, debris, foreign hair
- Strict, continuous chain of custody; consent for the kit and for storage
- Never delays resuscitation, analgesia or immediate safety
Photo-documentation
Always, with consent
- Colposcopy or high-resolution camera with a scale and colour reference
- Explicit, separate consent for the images and their storage
- Images labelled, stored securely, available for peer review
- Defends the documented finding in court
Targeted medical tests
By presentation
- STI testing by age, timing and site
- Bloods for coagulopathy if bruising is unexplained
- Skeletal survey and neuroimaging in suspected physical abuse of infants
- Pregnancy test in any post-menarchal adolescent
Photo-documentation deserves its own discipline because it is the part of the record most often mishandled. Every image must be taken with explicit and separately documented consent, must include a scale and a colour reference, must be labelled with the child's identifier and the date and time, and must be stored securely with restricted access. Images exist for peer review and for the court; they are a clinical and a forensic tool at once, and the consent conversation that precedes them must make that clear to the child and carer. [10]
The chain of custody is the unbroken, documented record of who held each forensic sample, from the moment it was collected to the moment it reached the laboratory. A single gap — an unlabelled swab, a sample left unattended, a transfer without a signature — is enough for the evidence to be excluded before it reaches court. The clinician who collects the sample owns the first link in that chain, and documenting it contemporaneously is non-negotiable. [7] [10]
Management — Resuscitation
Resuscitation comes before the forensic window, every time. An injured child is assessed and stabilised along the standard airway-breathing-circulation-disability-exposure pathway before any thought is given to the kit, the interview, or the documentation. The forensic kit is a time-limited element of the encounter; it is never the goal, and it never takes priority over a compromised airway, a tense abdomen, or a child in pain. [5]
The immediate priorities are haemodynamic stability, analgesia, and control of any active bleeding. A child with an acute inflicted injury — a deep laceration, a visceral injury, a burn — is managed exactly as any injured child is managed, with the added discipline that the team must preserve evidence and maintain the chain of custody while doing so. Clothing is bagged, not discarded; wounds are documented before they are dressed where possible; and the treating team communicates with the child-protection and forensic services in parallel. [5]
[5]Separating the child from the suspected perpetrator is a resuscitation-level safety priority. The child cannot give a free and accurate account in the presence of the person who harmed them, and the accompanying adult who refuses to leave may be that person. Establishing who has accompanied the child, who holds parental responsibility, and whether the child can be spoken to alone is part of the first minutes of the encounter, not an afterthought. [5]
Management — Definitive & Stepwise
Once the child is safe and stable, the definitive work proceeds in three phases — before the child, with the child, and after the child — each with its own discipline. The phases exist so that nothing is forgotten and nothing is contaminated, and so that the clinician can hand a complete, court-ready bundle to the safeguarding system. [1] [6]
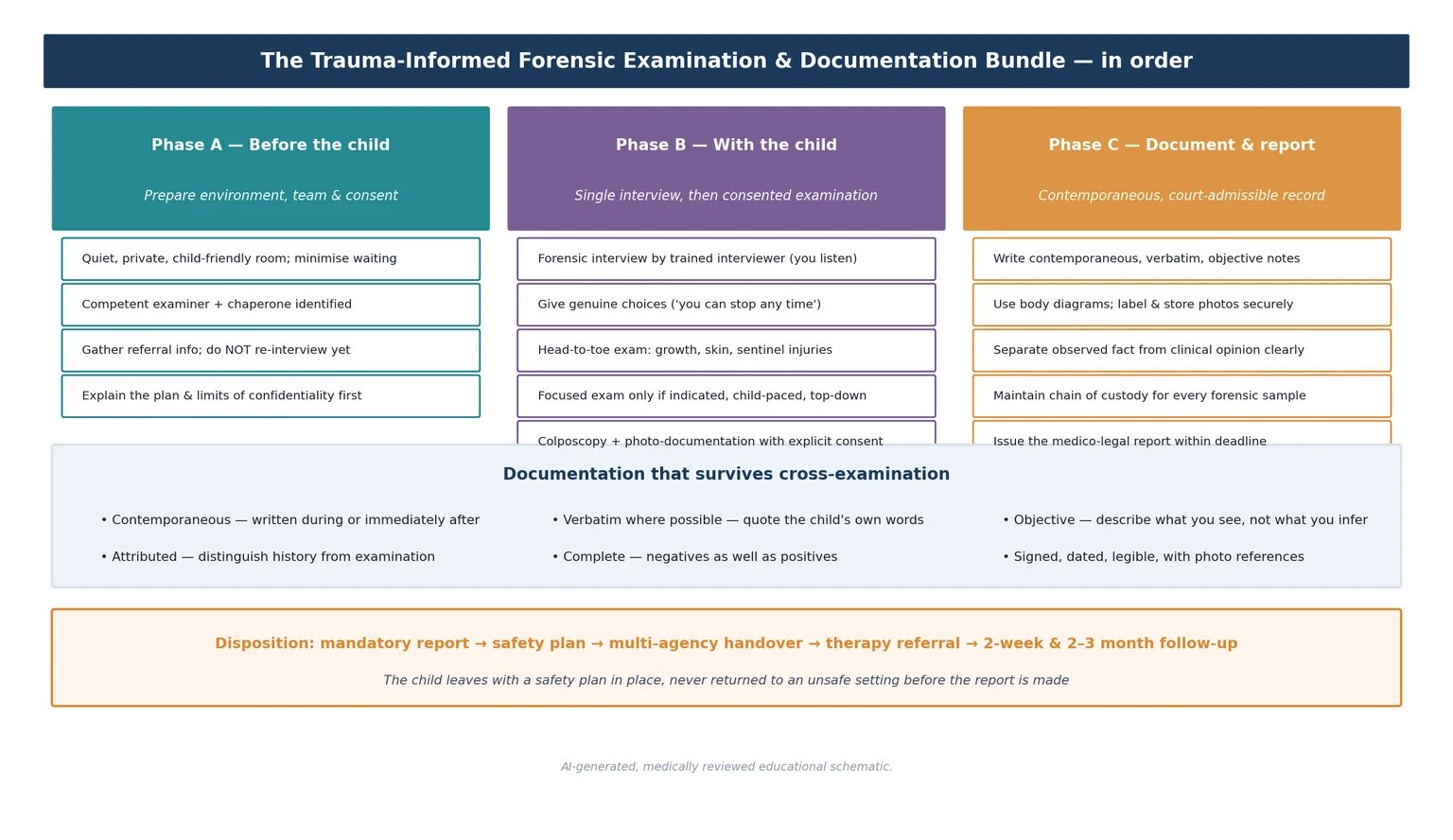
Phase A — before the child. Prepare the environment so that the child enters a calm, private, child-friendly space rather than a busy emergency bay. Identify the competent examiner and the chaperone. Gather the referral information from the agency, the school, or the carer — without re-interviewing the child — so that the clinician understands the allegation before meeting the child. Explain the plan and the limits of confidentiality to the child and carer before any history is taken, so that nobody is misled about what will be shared. [1]
Phase B — with the child. Run the single trained forensic interview, in which the clinician listens and documents rather than re-questions. Then conduct the consented examination: a general top-to-toe assessment of growth, skin, and signs of other maltreatment, followed by a focused examination only if indicated and only at the child's pace, with permission sought at each step. Use colposcopy with photo-documentation, having obtained explicit and separate consent for the images. Throughout, the child is told what is happening, given genuine choices where they exist, and allowed to stop. [5] [10]
Phase C — documentation and reporting. Write the contemporaneous record: the verbatim history in the child's own words, the observed findings on labelled body diagrams, the photo-documentation references, and the clinical opinion — each clearly distinguished. Maintain the chain of custody for every forensic sample. Issue the medico-legal report within the local deadline. Close with psychological first aid, the mandatory child-protection report, an agreed safety plan, a therapy referral, and a follow-up appointment. [6] [7]
What separates a court-admissible record from one that collapses
Specific Subtypes & Scenarios
The discipline of the trauma-informed forensic examination is constant, but the focus shifts with the subtype of maltreatment and the setting. The fellowship candidate must be able to adapt the spine to each scenario without losing the documentation standard. [5]
Acute sexual assault within the window. An adolescent presents within hours of an assault. The tempo is acute, the setting is a SARC or child-protection unit, and the bundle is time-limited: the forensic kit while the window is open, baseline specimens followed by post-exposure prophylaxis, emergency contraception if post-menarchal, HIV post-exposure prophylaxis risk assessment, and hepatitis B cover. Documentation is contemporaneous and court-admissible throughout, and the young person is the primary decision-maker wherever they are competent. [5] [7]
Non-acute disclosure in a young child. A prepubertal child discloses weeks or months later. There is no forensic window and no kit. The encounter is unhurried and child-paced, the single trained interview carries the diagnosis, and the examination is usually normal — which never excludes abuse. Photo-documentation and STI testing are the principal investigations, and the safeguarding record and therapy referral are the principal outputs. [5] [11]
Physical abuse with cutaneous injury. A child presents with bruising or patterned marks. The examination maps every injury on a body diagram with a scale, screens for sentinel injuries and signs of neglect, and excludes a bleeding diathesis where indicated. A skeletal survey and neuroimaging are considered in infants. The documentation must record the finding, the offered mechanism, and the clinician's opinion separately, because the gap between them is often what the court weighs. [5]
The non-verbal or disabled child. A child who cannot give a history is examined for the findings that speak for them: sentinel injuries, failure to thrive, signs of neglect, and anogenital findings. The examination is modified to the child's communication needs, with familiar carers present, communication aids, and a longer, more flexible encounter. The threshold for concern is lower, and the documentation must record the modifications made. [1] [5]
Complications & Pitfalls
The complications of a poor forensic examination fall on the child and on the case. Re-traumatisation through repeated examination and suggestive questioning is a direct harm to the child and a contamination of the evidence. A record written from memory, or an opinion stated as fact, collapses under cross-examination and can fail to protect the child in court. A break in the chain of custody excludes the evidence before it is weighed. [1] [7]
Re-traumatisation
Harm to the child
- Repeated examinations by different clinicians
- Suggestive or leading questioning
- Forcing an examination on a frozen child
- Encoding the encounter as a further trauma
Documentation failure
Harm to the case
- Notes reconstructed from memory
- Opinion blended into observed fact
- No body diagram, no scale, no photos
- Late, illegible, or altered record
Chain of custody
Evidence excluded
- Unlabelled or unattended samples
- Transfer without a signature
- Gap between collection and laboratory
- One gap excludes the whole sample
Confidentiality errors
Trust destroyed
- Promising secrecy that reporting cannot honour
- Disclosing findings to a suspected perpetrator
- Sharing beyond the need-to-know circle
- Failing to state the limits up front
The most common pitfall is the false-negative trap in reverse: using a normal examination to reassure a family that "nothing happened". A normal examination never excludes abuse, and documenting it as if it does is both clinically wrong and dangerous. The second is the over-call: labelling a non-specific or benign finding as diagnostic, which can destroy a family and undermine the clinician's credibility for the cases that matter. The disciplined separation of observation and opinion is what holds the line between the two. [5]
Confidentiality errors are a pitfall of their own. Promising a child or family that "no one else will know" is a promise mandatory reporting cannot keep, and making it destroys the trust the encounter depends on. The correct practice is to state the limits of confidentiality — including the duty to report — before the interview, framed as the clinician's job to keep the child safe rather than as a betrayal. [5]
Prognosis & Disposition
The prognosis of a maltreated child is shaped less by the single event than by what happens after it — whether they are believed, supported, removed from harm, and given timely therapy. The general paediatrician often owns the longitudinal relationship that follows the acute encounter, and the quality of the documentation at the index assessment determines whether that relationship is protected by a functioning safeguarding plan. [1] [4]
Long-term, trauma exposure is associated with post-traumatic stress, depression, suicidality, revictimisation, and a burden of adult physical disease. These outcomes are not fixed; timely, trauma-informed care, belief, and access to trauma-focused therapy modify them, which is why the disposition is never "examination done" but always "safety plan, report, therapy, and follow-up". [3] [4]
Disposition means the child leaves with a safety plan in place, a mandatory report filed, and a follow-up arranged — never returned to an unsafe setting before the report is made. The medico-legal report is issued within the local deadline, the multi-agency strategy discussion is scheduled, and the therapy referral is made. The general paediatrician who owns the follow-up is often the clinician who first examined the child, which is why the quality of the index record matters long after the encounter ends. [5]
Special Populations
Certain children face a higher risk of maltreatment, a harder examination, and a greater chance of being missed — and the trauma-informed approach must be adapted to each of them. The fellowship candidate must be able to describe the modification, not just name the group. [1]
Children with disability, especially those who are non-verbal or intellectually impaired, face substantially higher risk and disclose with greater difficulty. The examination is modified to their communication needs — familiar carers present, augmentative communication, a longer and more flexible encounter, and a willingness to examine opportunistically at a familiar clinic. The threshold for concern is lower, and the documentation must record the modifications made and the reasons for them. [1] [5]
Children in out-of-home care, young people in youth-justice settings, and refugee or migrant children carry elevated risk and often present with the accumulated burden of prior trauma. Indigenous children in settler-colonial contexts carry the additional weight of intergenerational trauma and systemic mistrust, and the trauma-informed principle of cultural, historical and gender awareness is not a platitude here but a clinical necessity — engaging cultural support, avoiding assumptions, and building trust over time. [1]
Adolescents carry their own consent, confidentiality, and decision-making dimensions. A mature minor can consent to examination, testing, and contraception, and the consultation is conducted with them as the primary decision-maker wherever they are competent. The limits of confidentiality are stated up front, and the encounter holds their autonomy alongside their safety. [5] [9]
Children in intensive or acute-care settings are a special case because the environment is intrinsically threatening. Applying trauma-informed principles in the paediatric intensive care unit — explanatory language, family presence where possible, minimisation of avoidable procedures, and attention to the sensory environment — is an emerging discipline, and the same principles that govern the forensic examination apply to the child recovering from any severe illness or injury. [12]
Evidence, Guidelines & Regional Differences
The operational evidence base for this topic draws on three streams: the trauma-informed care framework, the forensic-interview and examination literature, and the regional child-protection guidelines. The clinician must know which source governs which decision. [1] [5]
The trauma-informed care framework is anchored by the SAMHSA concept paper and the American Academy of Pediatrics clinical report, which translate the principles into paediatric practice. A 2024 systematic review of reviews found that trauma-informed care implementation in health settings shows promise for engagement and experience outcomes, though the evidence for hard clinical endpoints is still maturing — a candour the clinician should be able to reproduce when asked. [1] [3]
The forensic-interview literature is dominated by the National Institute of Child Health and Human Development Investigative Interview Protocol, whose body of research demonstrates that a structured, open-ended protocol improves the quality and informativeness of children's accounts. The examination literature is anchored by the Adams consensus guidance for anogenital findings and the broader child-protection examination texts. [5] [6]
Australia and Aotearoa New Zealand operate mandatory reporting of a reasonable belief of child abuse for all registered medical practitioners, with state and national child-protection legislation setting the thresholds and the reporting pathways. Forensic examinations are performed by trained clinicians through Sexual Assault Referral Centres, paediatric forensic medical services, or child-protection units, with remote peer review in rural and remote regions. [5]
The controversies are real and the candidate should name them. Who should examine the child, and how far should a generalist go before a subspecialist takes over? When is a forensic kit useful beyond the conventional window? How should photo-documentation consent be handled in very young children, and who owns the images? The answers vary by region and by service model, and the disciplined candidate states the local answer and the reasoning behind it rather than reciting a universal rule. [5] [10]
Exam Pearls
The single highest-yield sentence in this topic is this: a trauma-informed forensic examination is one procedure with two products — the child's safety, and a contemporaneous, court-admissible record — and the standard of both is set in the first five minutes of the encounter. Hold that, hold the six SAMHSA principles, and hold the order of the bundle, and the rest follows. [1] [5]
References
- [1]Forkey H, Szilagyi M, Kelly ET, Duffee J Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [2]Marsac ML, Kassam-Adams N, Hildenbrand AK, Nicholls E, Winston FK, Leff SS Implementing a Trauma-Informed Approach in Pediatric Health Care Networks. JAMA Pediatrics, 2016.PMID 26571032
- [3]Goldstein E, Chokshi B, Melendez-Torres GJ, Rios A, Jelley M, Lewis-O'Connor A Effectiveness of Trauma-Informed Care Implementation in Health Care Settings: Systematic Review of Reviews and Realist Synthesis. The Permanente Journal, 2024.PMID 38444328
- [4]Keeshin BR, Bryant BJ, Gargaro ER Emotional Dysregulation: A Trauma-Informed Approach. Child and Adolescent Psychiatric Clinics of North America, 2021.PMID 33743945
- [5]Adams JA, Kellogg ND, Farst KJ, Harper NS, Palusci VJ, Frasier LD Updated Guidelines for the Medical Assessment and Care of Children Who May Have Been Sexually Abused. Journal of Pediatric and Adolescent Gynecology, 2016.PMID 26220352
- [6]Lamb ME, Orbach Y, Hershkowitz I, Esplin PW, Horowitz D A structured forensic interview protocol improves the quality and informativeness of investigative interviews with children: a review of research using the NICHD Investigative Interview Protocol. Child Abuse & Neglect, 2007.PMID 18023872
- [7]Cross TP, Schmitt T Forensic medical results and law enforcement actions following sexual assault: A comparison of child, adolescent and adult cases. Child Abuse & Neglect, 2019.PMID 31075572
- [8]Feldman KW, Jenkins C, Laney T, Seidel K Toward instituting a chaperone policy in outpatient pediatric clinics. Child Abuse & Neglect, 2009.PMID 19818498
- [9]Berhane A, Hackell JM, Wallace S Use of Chaperones for the Pediatric and Adolescent Encounter: Policy Statement. Pediatrics, 2025.PMID 40383537
- [10]Brennan PA The medical and ethical aspects of photography in the sexual assault examination: why does it offend? Journal of Clinical Forensic Medicine, 2006.PMID 16571379
- [11]Lahoti SL, McClain N, Girardet R, McNeese M, Cheung K Evaluating the child for sexual abuse. American Family Physician, 2001.PMID 11261865
- [12]Demers LA, Wright NM, Kopstick AJ, Niehaus CE, Hall TA, Williams CN Is Pediatric Intensive Care Trauma-Informed? A Review of Principles and Evidence. Children (Basel), 2022.PMID 36291511