Paeds · child-safety-and-social-paediatrics
Youth justice and detained young people
Also known as Health of young people in detention · Juvenile justice health · Incarcerated adolescent health · Youth offending and health · Young offenders and developmental vulnerability · Detained youth and equivalence of care
Fellowship-level guide to the health of justice-involved and detained young people: the concentration of neurodisability, mental illness, trauma and substance use behind the gate; the equivalence-of-care principle; the entry-screening pathway; safeguarding, consent and confidentiality in custody; the post-release mortality spike; and the paediatrician's advocacy role across the community-to-detention-to-release arc.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a fifteen-year-old remanded in custody overnight for an alleged assault. Before the first hour passes he has disclosed suicidal thoughts, and you are the doctor called to see him. Your job is not to assess his guilt, and it is not to manage the security problem. It is to deliver the same standard of care he would receive in your emergency department, recognise the layers of vulnerability he carries, and act on the acute risk. [1] [16]
Justice-involved youth are young people whose lives have intersected with the youth justice system — from police diversion and community supervision through to sentenced or remand detention. Detention is the most restrictive end of that pathway, but most health needs are shared across the whole spectrum. The paediatric encounter matters wherever the young person sits on it. [1]
The load-bearing principle is equivalence of care: health services for young people in detention must be equivalent in standard, range and quality to those available in the community. Stated in the United Nations Havana Rules and adopted by national bodies, it means the young person does not forfeit the right to evidence-based, timely, confidential health care because a court has ordered their detention. [16]
The second principle is that detention is a screening window. Many of these young people have had erratic contact with health services, and detention is a rare moment of structure where unrecognised illness, disability and risk can be identified and addressed. Used well, it narrows rather than widens the health-equity gap. [10] [16]
Classification
Think of this group by what they carry, not by what they did. The useful clinical taxonomy sorts justice-involved young people by the dominant unmet health need, because that is what drives the assessment, the care plan and the handoff. [1] [16]
The five domains overlap heavily. A single young person may have post-traumatic stress disorder, fetal alcohol spectrum disorder, a traumatic brain injury, polysubstance use and untreated dental caries — and still need a pregnancy test. Expect the overlap, and screen broadly rather than narrowly. [1] [3]
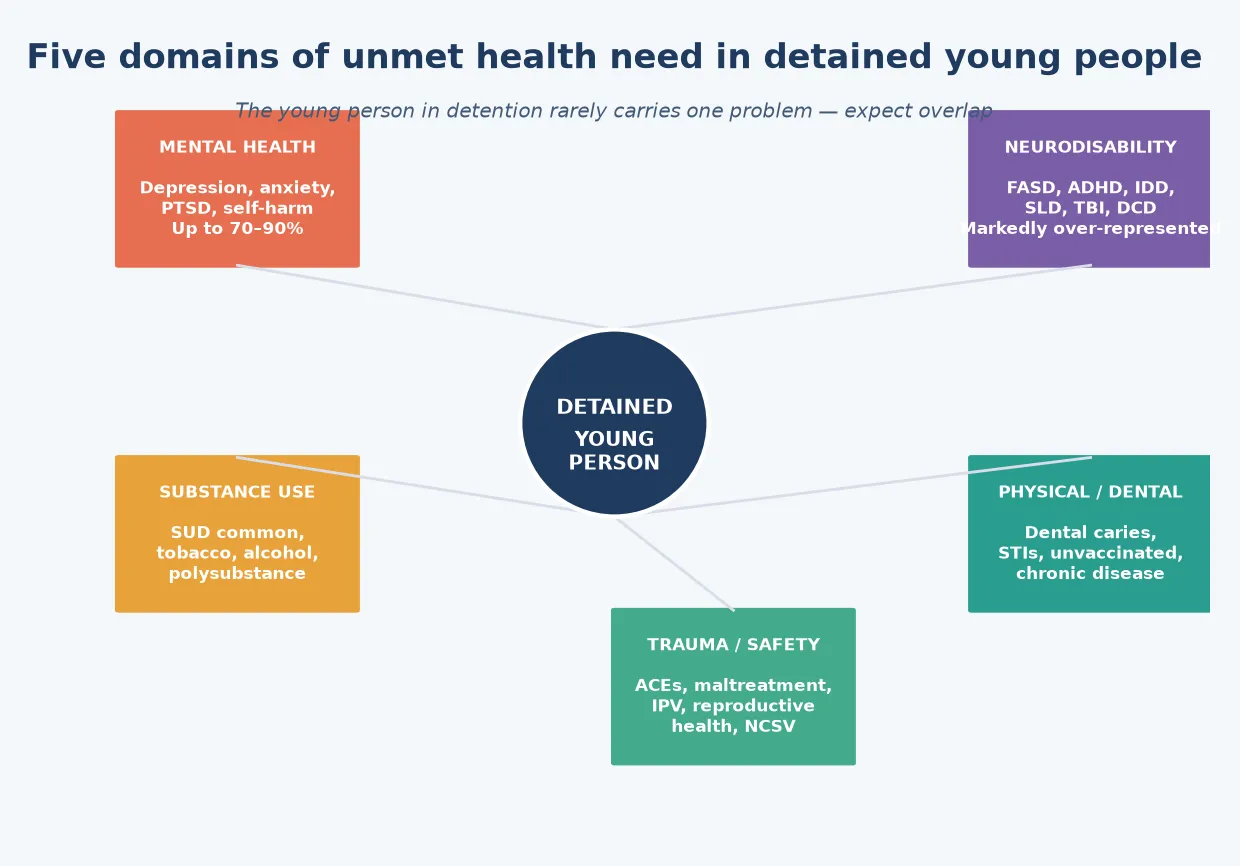
Dominant health domain — what to screen, what to expect
Epidemiology & Risk Factors
Justice-involved young people are few in absolute number but carry a disproportionate burden of illness. Globally, detention rates vary, but the health profile is remarkably consistent across high-income settings: a small, highly vulnerable group in whom adversity, disability and disease are concentrated. [1]
Borschmann and colleagues' global scoping review of adolescent detention health found that mental disorders, substance use and neurodisability occur at rates many multiples of community peers. The same review stressed that detention itself can expose young people to further harm — isolation, separation from family, and interruption of education and treatment. [1]
The mental-health burden is stark. Vincent and colleagues' MAYSI-2 national meta-analysis showed that the majority of young people entering juvenile justice facilities screen positive for clinically significant mental-health symptoms, with girls and some racial groups showing particular elevations. McBride's 2024 editorial framed the situation as a national state of emergency in children's mental health, with the justice system acting as a de facto mental-health service of last resort. [8] [9]
Neurodevelopmental disability is the hidden epidemic of youth justice. Billstedt and colleagues found that neurodevelopmental disorders — autism, ADHD, intellectual disability and communication disorders — overlapped extensively in young violent offenders, far above population rates. Kippin and colleagues showed that language disorder and fetal alcohol spectrum disorder are common among young people sentenced to detention, and frequently go unrecognised. [3] [12]
Bower and colleagues' Western Australian study is a landmark: more than one in three young people sentenced to detention met criteria for fetal alcohol spectrum disorder, a prevalence that dwarfs community estimates and reframes much "behavioural" non-compliance as unrecognised brain-based disability. [2]
Traumatic brain injury is another silent contributor. Moore, Indig and Haysom showed that TBI is common among incarcerated young people and clusters with mental illness, substance use and offending — a neurobiological load that impairs impulse control, attention and verbal processing, and that is rarely assessed in custody. [13]
Adverse childhood experiences are the upstream driver. Yohros' systematic review and meta-analysis confirmed that ACE exposure is associated with higher juvenile recidivism, and Moore and colleagues documented that childhood maltreatment and post-traumatic stress disorder are markedly elevated among incarcerated young offenders. The pathway runs from adversity to neurodisability to justice contact. [4] [14]
Indigenous overrepresentation is a defining feature of youth justice in Australia and New Zealand, and it reflects structural drivers, not individual pathology. Doolan and colleagues' birth-cohort study showed that child abuse and neglect partly explain the overrepresentation of Aboriginal and Torres Strait Islander young people in detention — pointing to prevention and early support, not criminalisation, as the leverage point. [6]
Pathophysiology
There is no single disease here — there is a causal pathway in which adversity becomes neurodisability, neurodisability becomes impaired self-regulation, and impaired self-regulation becomes justice contact. Understanding the pathway tells you where to intervene. [1] [3]
Early adversity — maltreatment, household dysfunction, poverty, housing instability and school exclusion — shapes brain development in ways that compromise executive function, emotional regulation and language. These are exactly the capacities a young person needs to navigate authority, follow instructions and desist from impulsive behaviour. [4] [14]
When neurodisability is added — fetal alcohol spectrum disorder, ADHD, intellectual disability, communication disorder, traumatic brain injury — the gap between the young person's capacity and the demands of the justice system widens. A young person who cannot process verbal instructions, who cannot regulate impulse, and who cannot read the social cues of a detention setting is set up to fail. [2] [12] [13]
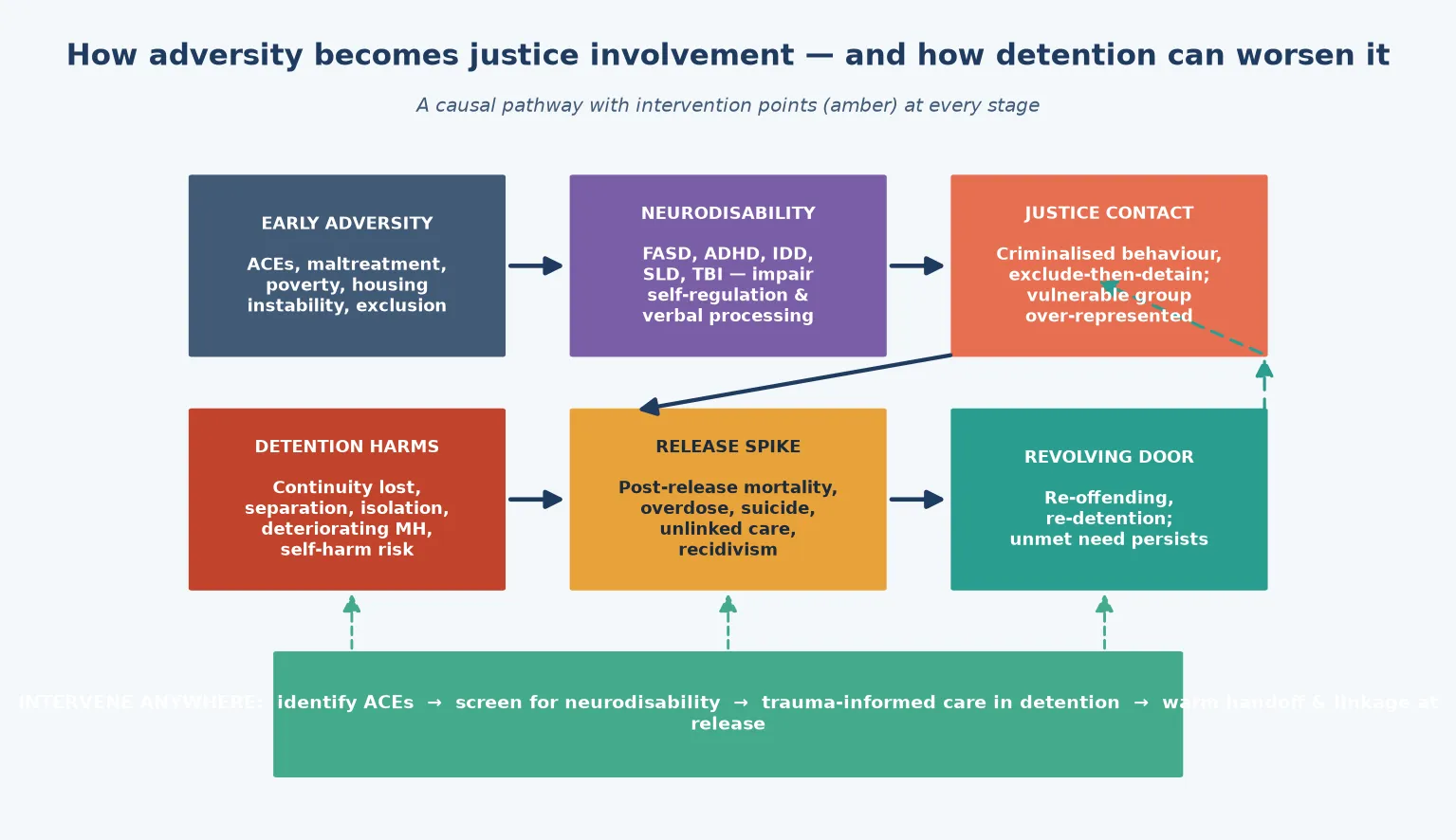
Detention itself can become a pathophysiological insult. Separation from family, disruption of schooling and treatment, exposure to isolation practices, and the deterioration of mental health in custody can convert a vulnerable young person into a sicker one. Balogun and colleagues asked whether juvenile detention impacts health, and found evidence that detention is associated with worse health outcomes, complicating any claim that custody is rehabilitative by default. [7]
Self-harm and suicidality are the acute end of the pathway. Borschmann and colleagues showed that self-harm is markedly elevated in young offenders, and Casiano and colleagues' population-based study confirmed a high prevalence with strong links to mental illness and trauma. The first days of custody are the highest-risk window, which is why entry screening for suicide risk is non-negotiable. [5] [11]
The post-release spike closes the loop. Borschmann and colleagues' individual-participant-data meta-analysis of over 1.4 million people found that the weeks immediately after release from incarceration carry a markedly elevated risk of death — suicide, overdose and injury dominate. Unmet need does not dissolve when the gate opens; it intensifies, and a young person without a linked clinician is at the mercy of it. [17]
Clinical Presentation
A young person entering detention rarely presents with a single complaint. They arrive through a reception process that may surface an acute problem — intoxication, injury, suicidal ideation — or may reveal nothing until a structured assessment finds the layers beneath. [1] [16]
The acute presentation dominates the first 24–72 hours. Intoxication or withdrawal from alcohol, cannabis or other substances can mimic behavioural disturbance. A disclosed or undisclosed injury from the precipitating event needs assessment. Acute suicidality, self-harm or psychotic symptoms require immediate risk management. These are the presentations that cannot wait for the routine screen. [5] [11]
The mental-health presentation is pervasive. Low mood, anxiety, irritability and sleep disturbance are near-universal, and post-traumatic stress symptoms — hypervigilance, flashbacks, emotional numbness — are common given the trauma load. Anger and non-compliance may be the visible tip, but they frequently sit on top of untreated mental illness and unrecognised neurodisability. [8] [14]
The neurodisability presentation is the one most often missed. A young person who appears oppositional may have a language disorder they cannot articulate, an attention disorder that makes structured settings unbearable, or fetal alcohol spectrum disorder that has gone unrecognised since childhood. Distinguish capacity from compliance: "won't" and "can't" look identical from across the room, but they need completely different responses. [2] [12]
The substance-use presentation ranges from acute intoxication and withdrawal to entrenched dependence. Tobacco use is near-universal; alcohol, cannabis and polysubstance use are common. Withdrawal can present with irritability, anxiety, sleep disturbance and autonomic signs, and it is easily mistaken for behavioural disturbance in a high-stress environment. [1] [13]
The physical and reproductive presentation includes dental pain, untreated chronic disease, visual and hearing problems, skin infection, and — particularly in young women — pregnancy, sexually transmitted infection and reproductive-health needs. Barnert and colleagues' systematic review showed that reproductive health needs among recently incarcerated youth are common and frequently unmet during reentry. [15]
The trauma presentation may surface as hypervigilance, distrust of authority, emotional withdrawal or reactive aggression. A young person who has been maltreated or exposed to family violence may experience the controlled, authoritative environment of detention as a re-traumatising setting, and procedures that feel routine to staff — searches, isolation, physical restraint — can trigger trauma responses. [4] [14]
Differential Diagnosis
When you encounter a detained young person, the first task is to distinguish behaviour from illness. What looks like defiance may be untreated mental illness, withdrawal, neurodisability or a trauma response. Reframe the presentation before you label it. [1] [14]
Distinguish substance withdrawal from behavioural disturbance. Irritability, anxiety, sleep disruption and autonomic signs in the first days of custody may reflect withdrawal rather than non-compliance, and the treatment is medical, not disciplinary. A substance-use screen and a withdrawal-risk assessment at entry separate the two. [13]
Separate capacity from wilful non-compliance. A young person who does not follow instructions may have a language disorder, intellectual disability, hearing loss or attention disorder that genuinely prevents understanding or execution. A brief cognitive and language screen, performed without judgement, distinguishes "can't" from "won't". [2] [12]
Differentiate trauma-driven reactivity from conduct disorder or antisocial behaviour. Hypervigilance, startle and reactive aggression in a young person with a maltreatment history may represent post-traumatic reactivity rather than primary conduct disturbance. The distinction changes the management — trauma-informed de-escalation and treatment, not punishment. [4] [14]
Distinguish mood and anxiety disorders from normal adolescent distress or situational upset. Detention is inherently stressful, and some distress is expected. Persistent low mood, anhedonia, panic, hopelessness and suicidal ideation that persist beyond the acute adjustment period, or that carry features of severity, point to a treatable disorder. [8] [9]
Telling apart psychotic symptoms from intoxication, dissociation or trauma-related phenomena can be difficult in custody. Acute hallucinations or delusional thinking need urgent assessment to exclude a primary psychotic disorder, substance-induced psychosis, or a trauma-related dissociative state. When uncertain, treat it as urgent and consult mental health. [1]
Clinical & Bedside Assessment
The entry health assessment is the centrepiece of detention medicine, and it must be structured, trauma-informed and broad. Treat it as the moment that captures what the community missed, and do it properly. [10] [16]
Secure immediate safety first. In the first 24–72 hours, assess suicide and self-harm risk explicitly, screen for intoxication and withdrawal, and identify any undisclosed injury or acute medical need. A young person at acute risk needs observation, a safety plan and, where indicated, constant supervision until the risk is clarified. [5] [11]
Take a trauma-informed history. Explain who you are, what you will do with the information, and the limits of confidentiality. Use open questions, pace the interview for trauma, and avoid interrogating about the offence — that is not your role. Ask about mental health, substance use, past head injury, developmental and educational history, and experiences of maltreatment or violence, but follow the young person's lead on pace and depth. [1] [14]
Screen systematically. Use a validated mental-health screening tool — the Massachusetts Youth Screening Instrument (MAYSI-2) is the most widely used — to flag symptoms requiring fuller assessment. Add a substance-use screen, a cognitive and language flag, and a reproductive and sexual-health screen where relevant. Document the screens and their results. [8] [16]
Examine thoroughly. Measure height and weight, examine for signs of injury, infection or chronic disease, check vision and hearing, and inspect the mouth for dental disease. A young person may not have seen a dentist or optometrist in years, and detention is the chance to catch it. [1] [10]
Assess capacity and consent carefully. Assume a literacy and language barrier until you have evidence to the contrary. Check that the young person understands what is being offered, the alternatives, and the consequences of refusing, and document the assessment of capacity under the mature-minor framework applicable in your jurisdiction. [12] [16]
Investigations
Investigations in detention follow the clinical questions the screen raises, not a blanket protocol. The goal is to bring the standard of assessment up to community equivalence, not to run tests the community would not run. [16]
Mental-health assessment drives most investigation. A positive MAYSI-2 screen, or clinical concern, warrants a structured mental-health assessment — ideally by a clinician with adolescent and forensic expertise — to clarify the diagnosis, assess risk, and guide treatment. Casiano and colleagues confirmed that mental illness is the strongest correlate of self-harm in juvenile detention, so risk assessment is central. [8] [11]
Neurodevelopmental assessment is warranted when the screen flags cognitive, language or behavioural concerns. Formal cognitive and language assessment, and evaluation for fetal alcohol spectrum disorder, attention-deficit/hyperactivity disorder and autistic traits, can transform a young person's trajectory — a recognised disability opens access to support, adaptation and, where relevant, diversion. [2] [12]
Substance-use assessment clarifies dependence and withdrawal risk, and identifies young people who would benefit from treatment. Screening tools and a structured history are the starting point, with referral to adolescent substance-use services where dependence is identified. [1] [13]
Physical-health investigation targets the findings of the examination. Dental review, vision and hearing testing, sexually transmitted infection screening, and vaccination catch-up address the common gaps. Chronic disease — asthma, epilepsy, diabetes — needs the same work-up and management plan it would receive in the community. [10] [15]
Investigations that are not helpful include blanket neuroimaging without clinical indication, routine drug testing used punitively rather than clinically, and any test ordered to serve a security rather than a health purpose. Every investigation should answer a clinical question and serve the young person's care. [16]
Management — Resuscitation
The resuscitation phase is about the acute risks that threaten life or limb in the first hours and days of custody. Identify them, act on them, and document what you did. [5] [16]
Suicide and self-harm risk is the dominant acute threat. A young person who discloses suicidal ideation, who has a recent history of self-harm, or who is intoxicated, isolated or in acute crisis needs a clear, documented risk-management plan — observation level, removal of means, supportive contact, and urgent mental-health assessment. Do not rely on observation alone; treat it as a clinical emergency. [5] [11]
Intoxication and withdrawal need medical management. Assess the substance, the timeframe, the severity and the comorbidity, and monitor for deterioration. Alcohol and benzodiazepine withdrawal can be life-threatening; opioid withdrawal is miserable and drives self-discharge or self-harm risk. Treat withdrawal symptomatically and escalate to hospital care if severity exceeds the facility's capacity. [13]
Acute medical and surgical emergencies — injuries, seizures, diabetic emergencies, acute psychosis with risk — are managed as they would be in any setting, with transfer to an acute hospital when the facility cannot provide the required level of care. Equivalence of care means the young person reaches the same standard regardless of their custodial status. [7] [16]
Allocate roles so that clinical care and the custodial process run in parallel rather than in conflict. Your job is to advocate for the medical priority, communicate clearly with custodial staff about what the young person needs, and document the clinical reasoning. When clinical and security agendas collide, the health need comes first. [16]
Management — Definitive & Stepwise
Once the acute risks are managed, the definitive phase builds a comprehensive care plan that matches community equivalence and sets up continuity through release. This is where detention becomes a health-improving intervention rather than a holding operation. [10] [16]
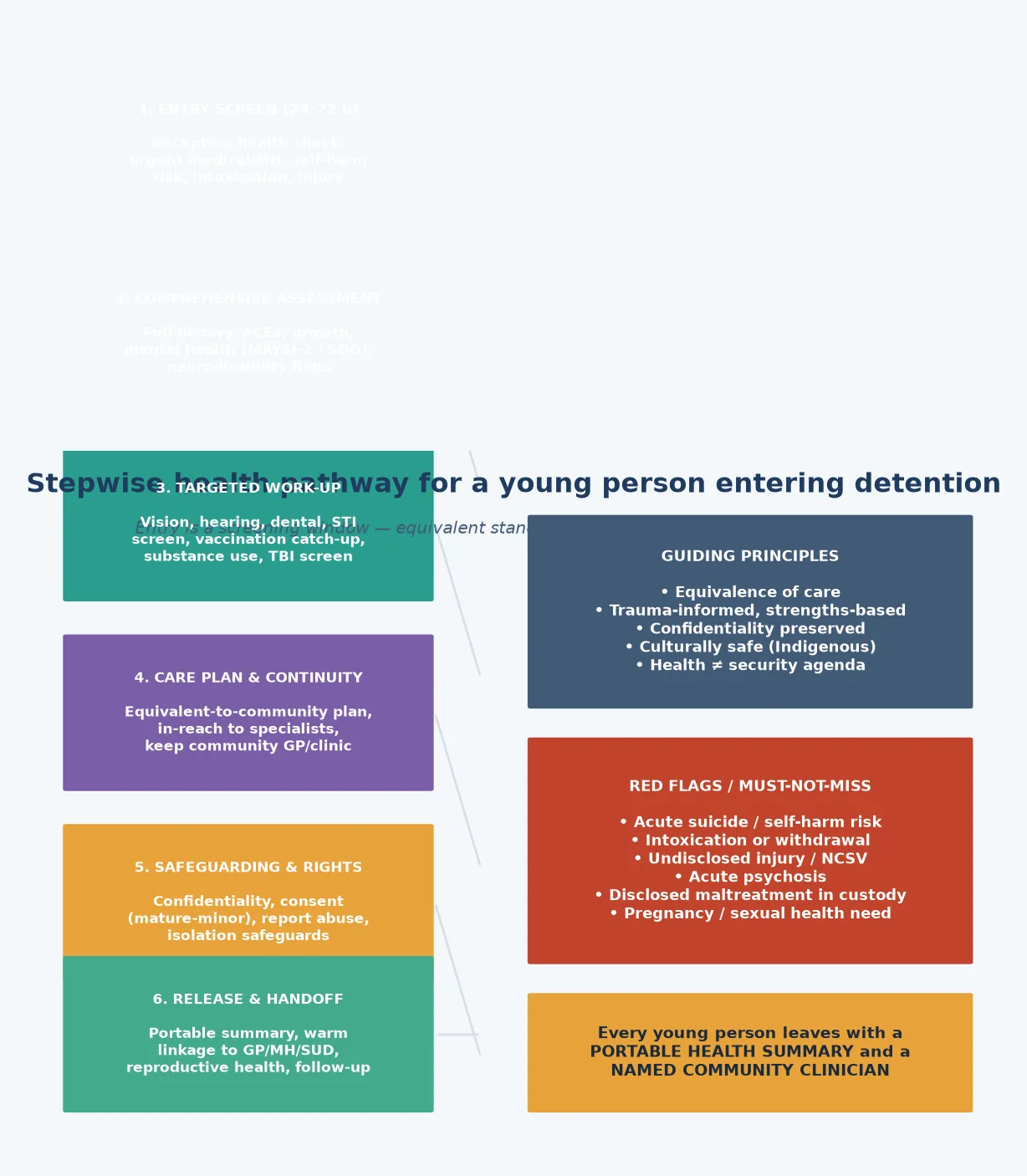
Entry-to-release health pathway
Entry screen (24–72 h) — reception health check: acute medical and mental-health need, suicide and self-harm risk, intoxication, injury
Comprehensive assessment — full history, ACEs, growth, mental health (MAYSI-2 / SDQ), neurodisability and language flags
Targeted work-up — vision, hearing, dental, STI screen, vaccination catch-up, substance-use and TBI assessment
Care plan and continuity — equivalent-to-community plan, in-reach to specialists, maintain community GP and clinic links
Safeguarding and rights — confidentiality, consent (mature-minor), report abuse, isolation safeguards
Release and handoff — portable summary, warm linkage to GP / mental health / substance-use services, reproductive health, follow-up
Treat what you find. Mental illness, substance-use disorder, dental disease, chronic disease and unmet reproductive-health need should each receive an evidence-based management plan. Beaudry and colleagues' systematic review showed that psychological interventions in custodial settings can reduce recidivism, so treatment serves both health and justice outcomes. [18]
Maintain continuity with the community. Identify the young person's general practitioner, mental-health clinician, paediatrician or substance-use worker, and — with consent — keep them informed. Continuity protects against the fragmentation that deepens disadvantage, and it makes the release handoff possible. [10]
Plan for release from the day of entry. A portable health summary, a named community clinician, and a confirmed follow-up appointment close the loop that the post-release mortality spike opens. Barnert and colleagues' work on reentry health needs showed that reproductive and primary care linkage is frequently the gap that determines outcome. [15] [17]
Advocate beyond the individual. The paediatrician's role extends to the system — flagging when custodial practices harm health, advocating for diversion of vulnerable young people, and supporting community-based alternatives to detention for those whose underlying need is health rather than security. Equivalence of care includes the right to the least restrictive setting consistent with safety. [6] [16]
Specific Subtypes & Scenarios
The suicidal young person on reception. A sixteen-year-old discloses suicidal thoughts during the entry screen. Manage this as an acute mental-health emergency — risk assessment, observation level, removal of means, supportive contact, urgent mental-health review, and a documented safety plan. Do not allow the custodial setting to normalise the risk. [5] [11]
The young person with possible fetal alcohol spectrum disorder. A fifteen-year-old with a history of prenatal alcohol exposure, learning difficulty, facial features and impulsive offending is referred for behavioural concerns. Coordinate formal FASD assessment, recognise the brain-based basis of the behaviour, and advocate for environmental adaptation and support rather than purely punitive responses. Bower's prevalence data show this is common, not rare. [2]
The young person in withdrawal. A seventeen-year-old enters shakier and more irritable each hour after heavy alcohol and cannabis use. Distinguish withdrawal from behavioural disturbance, monitor for severity, treat symptomatically, and escalate to hospital if withdrawal exceeds the facility's capacity. Alcohol withdrawal can kill. [13]
The pregnant young woman in custody. A young woman discloses a missed period and possible pregnancy. Arrange pregnancy confirmation, antenatal care and reproductive-health counselling with full confidentiality, and plan for continuity through release. Barnert's review confirms that reproductive health needs are common and frequently unmet. [15]
The young person with undisclosed trauma. During assessment, a young person discloses recent non-consensual sexual violence or ongoing family violence. This is a safeguarding and health issue, not an internal custodial matter — follow your child-protection and forensic pathway, arrange forensic examination within the evidence-gathering window, and link to support services. [14] [16]
The Indigenous young person. Apply trauma-informed, culturally safe practice. Acknowledge the history and ongoing impact of justice-system involvement in Indigenous communities, identify kinship and community supports, and advocate for culturally appropriate diversion and support. Doolan's birth-cohort work points to early prevention as the real leverage point. [6]
The young person with traumatic brain injury. A history of multiple concussions or a significant head injury, with attention, memory and impulse-control problems, should trigger a TBI-informed approach — recognise the cognitive load, avoid overstimulating environments, and adapt instructions and expectations. Moore's data show TBI is common and under-recognised in custody. [13]
The young person approaching release. As release nears, the risk profile shifts — the post-release mortality spike looms. Finalise the portable summary, confirm the community appointments, ensure prescriptions bridge the gap, and arrange a warm handoff to a named clinician. The release plan is the preventive intervention. [15] [17]
Complications & Pitfalls
- Treating detention as a security problem rather than a health encounter — equivalence of care is the standard. [16]
- Missing neurodisability — FASD, ADHD, intellectual disability and language disorder are the rule here, not the exception. [2] [3]
- Overlooking acute suicide or self-harm risk in the first days of custody — the highest-risk window. [5] [11]
- Confusing the health role with the forensic or investigative role — you treat and advocate, you do not interrogate. [16]
- Assuming capacity without checking comprehension, literacy and language. [12]
- Using isolation, restraint or observation punitively rather than clinically, and re-traumatising in the process. [7]
- Letting the care plan die at the gate — without a warm handoff, the post-release spike takes the gain back. [17]
- Failing to maintain confidentiality, or sharing health information for security purposes beyond what care requires. [16]
- Missing pregnancy, sexually transmitted infection or reproductive-health need in young women. [15]
- Forgetting that the paediatrician advocates for diversion and the least restrictive setting for vulnerable youth. [6]
Prognosis & Disposition
The prognosis for a justice-involved young person depends less on the offence than on whether their health needs are met. A young person whose mental illness, neurodisability, substance use and trauma are recognised and treated has a far better trajectory than one whose needs are punished rather than addressed. [1] [16]
Recidivism is the outcome the justice system tracks, but it is a health outcome too. Yohros' meta-analysis linked adverse childhood experiences to juvenile recidivism, and Beaudry and colleagues showed that psychological interventions in custody reduce it — so treating the health need changes the justice prognosis. [4] [18]
The immediate disposition within custody depends on the assessment. Acute risk may require hospital transfer, a higher observation level, or a mental-health admission. Chronic needs are managed in the facility with in-reach, or in the community with supervised attendance. The principle is the least restrictive setting consistent with safety and the standard of care. [7]
The post-release period is where the prognosis is most fragile. Borschmann and colleagues' mortality meta-analysis made clear that the weeks after release carry a sharply elevated death risk — suicide, overdose and injury. The young person who leaves with a linked clinician, a portable summary and a confirmed appointment has a real chance; the one who does not is exposed. [17]
Longer-term, justice-involved youth carry elevated risks of adult incarceration, mental illness, substance-use disorder and premature death across the life course. Early recognition and treatment, diversion of vulnerable young people, and continuity of care through and beyond detention are the interventions that bend the curve — and they are the paediatrician's contribution. [1] [6]
Special Populations
Young women in detention. Girls are fewer in number but carry a particularly high burden of trauma, mental illness and reproductive-health need. Screen for pregnancy, sexually transmitted infection, history of exploitation and intimate-partner violence, and recognise that the justice system is often a late touchpoint for young women whose primary need is protection and treatment. [8] [15]
Indigenous young people. Apply trauma-informed, culturally safe care, acknowledge intergenerational trauma and the legacy of systemic overrepresentation, and engage with community-controlled services wherever possible. Advocate for diversion and community-based alternatives that address the structural drivers Doolan and colleagues identified. [6]
Young people with neurodevelopmental disability. FASD, ADHD, intellectual disability, language disorder and traumatic brain injury cluster in this group and drive much of the behaviour that brings young people to custody. Screen for them, recognise the brain-based basis of the presentation, and adapt the environment and expectations accordingly. [2] [3] [13]
Young people with mental illness. Depression, anxiety, post-traumatic stress disorder, psychosis and self-harm are common and frequently untreated before detention. Treat them to community-equivalent standards, and arrange continuity of mental-health care through release. [8] [9]
Young people in out-of-home care. A disproportionate number of detained youth are or have been in out-of-home care, reflecting the shared upstream drivers of maltreatment, instability and exclusion. Coordinate with the child-protection system and the carer or caseworker, and recognise that detention may be one displacement in a trajectory of displacement. [14] [16]
Young people from migrant, refugee or asylum-seeking backgrounds. Language barriers, trauma, disrupted education and uncertain legal status complicate both health need and access. Use professional interpreters, pace for trauma, and advocate for services that recognise the additional layers of vulnerability. [1]
Evidence, Guidelines & Regional Differences
Borschmann and colleagues' 2020 global scoping review in The Lancet Public Health is the foundational synthesis of adolescent detention health, documenting the consistent concentration of mental, neurodevelopmental, substance-use and physical morbidity across settings and the potential for detention itself to harm. [1]
The neurodisability evidence has reshaped the field. Bower's Western Australian FASD prevalence study, Billstedt's work on overlapping neurodevelopmental disorders in violent offenders, and Kippin's study of language disorder and FASD in sentenced youth together establish that unrecognised brain-based disability is a defining, addressable feature of youth justice populations. [2] [3] [12]
The trauma and recidivism evidence closes the causal loop. Moore and colleagues linked childhood maltreatment and PTSD to incarceration, and Yohros' meta-analysis linked ACEs to juvenile recidivism — confirming that the pathway from adversity to justice contact is measurable and modifiable. [4] [14]
The mortality evidence sets the stakes. Borschmann's 2024 individual-participant-data meta-analysis of over 1.4 million people quantified the post-release death risk, and the self-harm work of Borschmann and Casiano established the in-custody risk — together framing detention and release as periods of acute and preventable mortality. [5] [11] [17]
In Australia, state and territory youth justice systems administer detention, and each operates reception health screening with varying models of in-reach, on-site nursing and visiting medical and mental-health staff. Indigenous young people are vastly overrepresented, and culturally safe practice is a core requirement. The Australian Institute of Health and Welfare reports national youth justice data, and the Royal Australasian College of Physicians advocates for equivalence of care and diversion. In Aotearoa New Zealand, Oranga Tamariki administers youth justice residences, with attention to obligations under Te Tiriti o Waitangi and the overrepresentation of Māori young people. State the principle — equivalence of care, trauma-informed and culturally safe screening on entry, and warm handoff at release — and verify the local model and referral pathways. [1] [6]
Exam Pearls
SCREEN
References
- [1]Borschmann R, Janca E, Carter A, Willoughby M, Hughes N, Snow K, et al. The health of adolescents in detention: a global scoping review. The Lancet Public Health, 2020.PMID 31954434
- [2]Bower C, Watkins RE, Mutch RC, Marriott R, Freeman J, Kippin NR, et al. Fetal alcohol spectrum disorder and youth justice: a prevalence study among young people sentenced to detention in Western Australia. BMJ Open, 2018.PMID 29440216
- [3]Billstedt E, Anckarsäter H, Wallinius M, Hofvander B Neurodevelopmental disorders in young violent offenders: overlap and background characteristics. Psychiatry Research, 2017.PMID 28285251
- [4]Yohros A Examining the relationship between adverse childhood experiences and juvenile recidivism: a systematic review and meta-analysis. Trauma, Violence & Abuse, 2023.PMID 35166600
- [5]Borschmann R, Coffey C, Moran P, Hearps S, Degenhardt L, Kinner SA, et al. Self-harm in young offenders. Suicide & Life-Threatening Behavior, 2014.PMID 24773535
- [6]Doolan I, Najman JM, Mills R, Cherney A, Strathearn L Does child abuse and neglect explain the overrepresentation of Aboriginal and Torres Strait Islander young people in youth detention? Findings from a birth cohort study. Child Abuse & Neglect, 2013.PMID 23352083
- [7]Balogun T, Troisi C, Swartz MD, Lloyd L, Beyda R Does juvenile detention impact health? Journal of Correctional Health Care, 2018.PMID 29544377
- [8]Vincent GM, Grisso T, Terry A, Banks S Sex and race differences in mental health symptoms in juvenile justice: the MAYSI-2 national meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 2008.PMID 18216730
- [9]McBride AB Editorial: Justice-involved youth — a national state of emergency in children's mental health. Journal of the American Academy of Child and Adolescent Psychiatry, 2024.PMID 37992853
- [10]Balogun T, Troisi C, Swartz MD, Beyda R Juvenile justice-involved youth: preventive health services received prior to detention. Journal of Correctional Health Care, 2021.PMID 34402679
- [11]Casiano H, Bolton SL, Hildahl K, Katz LY, Bolton J, Sareen J A population-based study of the prevalence and correlates of self-harm in juvenile detention. PLoS One, 2016.PMID 26760497
- [12]Kippin NR, Leitão S, Watkins R, Finlay-Jones A, Condon C, Marriott R, et al. Language diversity, language disorder, and fetal alcohol spectrum disorder among youth sentenced to detention in Western Australia. International Journal of Law and Psychiatry, 2018.PMID 30420110
- [13]Moore E, Indig D, Haysom L Traumatic brain injury, mental health, substance use, and offending among incarcerated young people. The Journal of Head Trauma Rehabilitation, 2014.PMID 23656964
- [14]Moore E, Gaskin C, Indig D Childhood maltreatment and post-traumatic stress disorder among incarcerated young offenders. Child Abuse & Neglect, 2013.PMID 23978574
- [15]Barnert E, Sun A, Abrams L, Chung PJ Reproductive health needs of recently incarcerated youth during community reentry: a systematic review. BMJ Sexual & Reproductive Health, 2020.PMID 31722933
- [16]Barnert ES, Perry R, Morris RE Juvenile incarceration and health. Academic Pediatrics, 2016.PMID 26548359
- [17]Borschmann R, Mortality After Release from Incarceration Consortium (MARIC) collaborators, Kinner SA Rates and causes of death after release from incarceration among 1 471 526 people in eight high-income and middle-income countries: an individual participant data meta-analysis. The Lancet, 2024.PMID 38614112
- [18]Beaudry G, Yu R, Perry AE, Fazel S Effectiveness of psychological interventions in prison to reduce recidivism: a systematic review and meta-analysis of randomised controlled trials. The Lancet Psychiatry, 2021.PMID 34419185