Paeds · clinical-assessment-and-reasoning
Clinical reasoning, problem representation and differential diagnosis
Also known as Problem representation · Illness scripts · Paediatric differential diagnosis · Diagnostic reasoning · Clinical reasoning paediatrics
A fellowship approach to paediatric clinical reasoning: build an age-aware problem representation, prioritise a threat-first differential, use illness scripts and analytic checks deliberately, detect cognitive and system traps, revise with tests and response, and communicate residual risk from neonate to transition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Clinical reasoning is the work of turning messy paediatric data into a usable clinical story, a prioritised list of possibilities, and a plan that stays safe while certainty is incomplete. It is not a personality trait. It is a bedside method you can practise. [1] [6]
A problem representation is that one-sentence clinical summary. It is more than the chief complaint and less than the final diagnosis. Experts compress age, context, tempo and discriminating features into a sentence that activates the right illness scripts. Novices often retell the whole history instead. [1] [5]
An illness script is a compact mental model of a disease: who gets it, what goes wrong, and what follows. You match the child’s story to scripts, then test the match. Paediatric scripts must be age-banded. “Pneumonia” in a neonate, a toddler and an adolescent are not the same mental object. [2] [20] [21]
A differential diagnosis is the short, ranked list of scripts still in play. A working diagnosis is the current best label for action. It is provisional. Diagnostic uncertainty is not failure; unspoken uncertainty is. [8] [9]
The observable reasoning pathway
First look
If airway, breathing, circulation or consciousness is failing, treat while you gather a focused story. Reasoning never blocks ABCDE.
Compress the story
Write one sentence: age, baseline, tempo, key semantic features, physiology and leading threat.
Open the list
Build a short threat-first differential. Keep must-not-miss items even when a common script fits.
Pause
Ask what would change your mind, what you must not miss, and who else should look.
Test and treat
Choose discriminating data. Give time-critical treatment without treating response as proof of one cause.
Rewrite and hand over
Update the representation. State residual risk, next discriminating step, safety-net and follow-up.
Classification
Reasoning tools are not interchangeable. Problem representation compresses the case. Illness scripts store disease knowledge. Dual-process language describes when you recognise a pattern quickly and when you should slow down. Diagnostic-error language describes wrong, delayed or missed labels after the fact. Keep the jobs separate. [2] [3] [4]
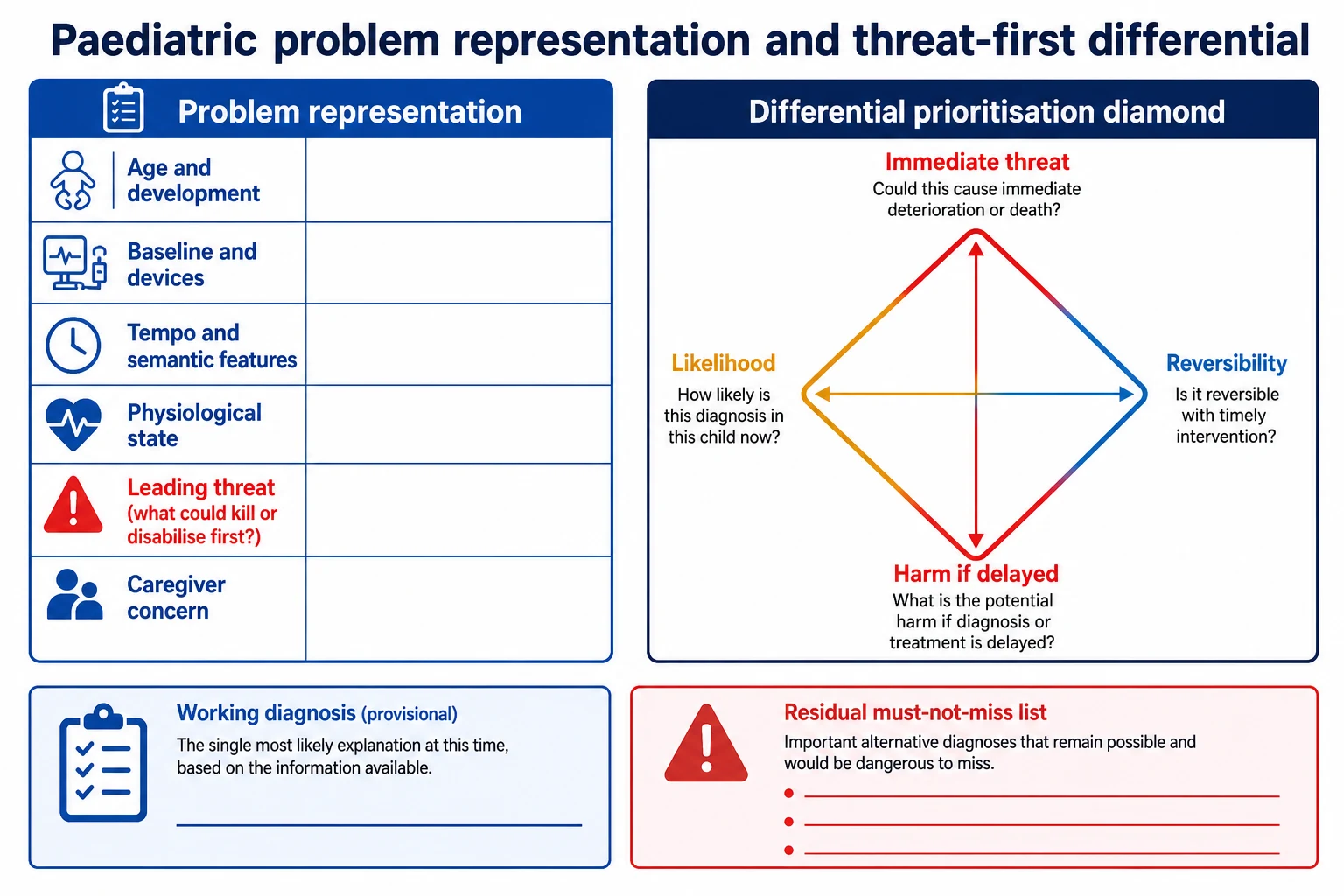
Read the figure like this: if your sentence omits age, baseline or threat, your differential will drift. If your list is ordered only by specialty interest, you will miss what can kill the child first. [1] [5]
Problem representation
The clinical sentence
- Compresses age, baseline, tempo and threat
- Activates the right illness scripts
- Changes after new data
- Not a final diagnosis
Illness script
Stored disease model
- Enabling conditions, fault, consequences
- Needs paediatric age variants
- Built by deliberate case practice
- Can misfire if features are incomplete
Differential
Ranked open list
- Threat first, then likelihood
- Includes reversible and must-not-miss items
- Usually short at the bedside
- Must stay flexible
Working diagnosis
Label for action now
- Guides immediate tests and treatment
- Remains provisional
- Needs residual-risk statement
- Never silences caregiver concern
Semantic qualifiers make scripts fire correctly: acute versus chronic, continuous versus intermittent, focal versus diffuse, progressive versus static, febrile versus afebrile, first episode versus recurrent. “Three days of progressive focal limp after a minor trip” is a different sentence from “six weeks of migratory pains with morning stiffness.” [1] [20]
The Assessment of Reasoning Tool (ART) gives teachers a shared language for feedback on hypothesis generation, representation, differential prioritisation and metacognition. Use it as a coaching scaffold, not as a bedside score. [6] [7]
Epidemiology & Risk Factors
There is no single incidence of “missed diagnosis in childhood.” Settings differ. Emergency, ward, perinatal and critical-care studies include different children and different reference standards. The practical lesson is where risk concentrates. [11] [19]
Diagnostic error has been synthesised in paediatric critical care, and paediatric diagnostic-safety priorities have been ranked in modified Delphi work. Time pressure, non-specific early signs, complex chronic disease, rare disease, fragmented information and weak feedback loops recur. [11] [19] [9]
Child and disease risk
- Young infant and neonate with non-specific signs
- Immunocompromise with muted inflammation
- Medical complexity and technology dependence
- Rare or undiagnosed disease contexts
- Presentations that evolve over hours
Clinician and team risk
- Fatigue, interruption and cognitive load
- Anchoring on the triage label
- Hierarchy that silences concern
- Handover loss of residual risk
- Overconfidence after a first treatment response
System and access risk
- Language discordance without interpreters
- Missing records or growth charts
- Night staffing and rural distance
- Telehealth limits
- Production pressure to discharge
Family and equity risk
- Caregiver concern discounted
- Racism or prior adverse care
- Transport and literacy barriers
- Out-of-home care with fragmented historians
- Safeguarding complexity
Caregiver concern that the child is different from usual is not soft colour. In prospective hospital work it associates with critical illness. Put it in the problem representation. [15]
Return visits are new data. Previous reassurance is not evidence of current safety. Night deterioration after a daytime “likely viral” label is a classic second story. [9] [12]
Pathophysiology
Children can look deceptively stable while compensation hides a dangerous process. That physiology matters for reasoning because the early script may look mild. Your representation must include trajectory, not only the snapshot. [14] [9]
Dual-process accounts describe fast recognition and slower analytic checking. Fast thinking is not the enemy. Experts use it constantly. The danger is unmonitored fast thinking in a high-stakes, poorly fitting case. Slow thinking is not automatically safe either; it can become endless listing. The skill is knowing when to switch. [3] [4] [14]
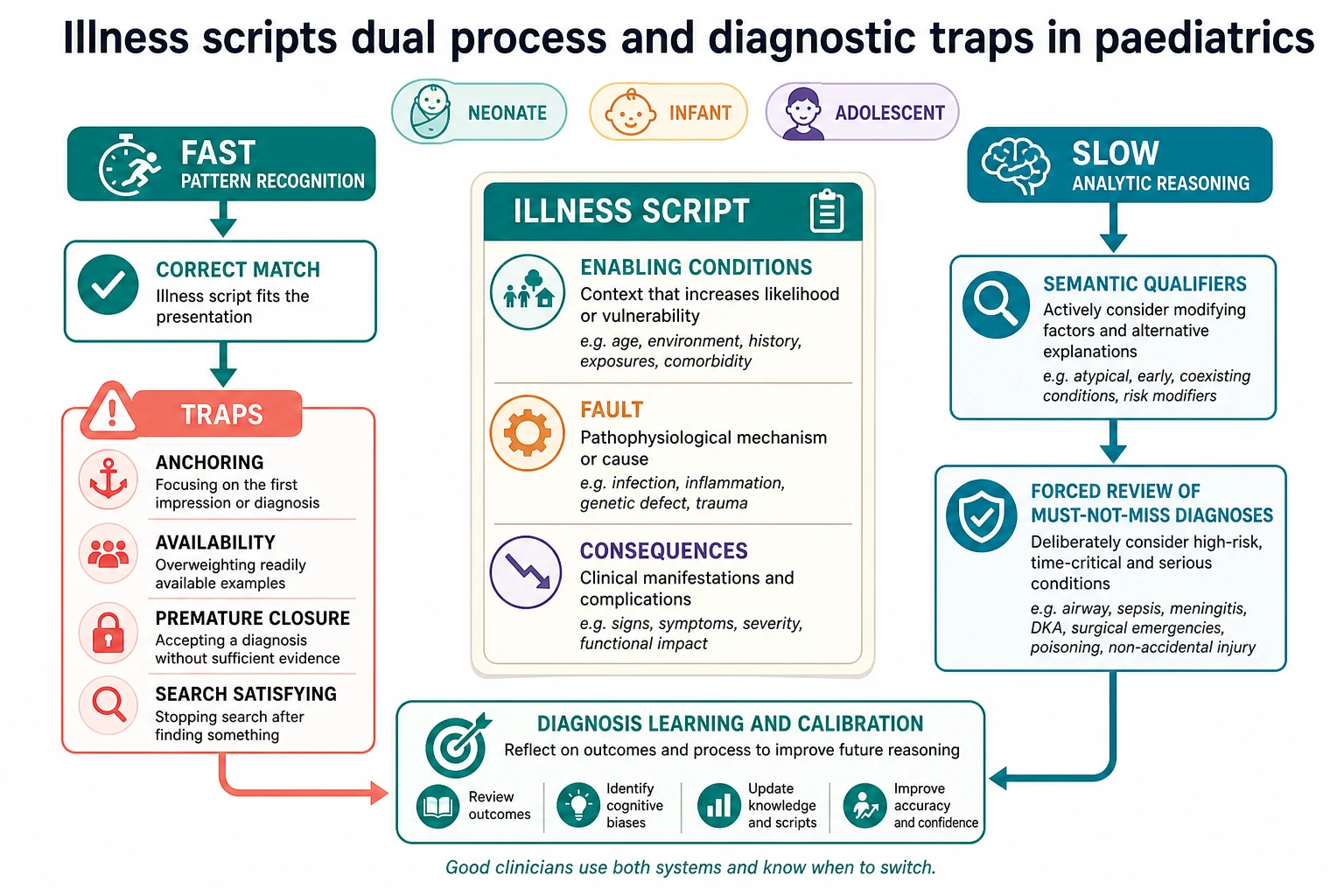
Read the figure like this: if the child matches a clean script and physiology is stable, act on the match while watching for mismatch. If the story is non-specific, high risk or “almost viral but not quite,” force the analytic branch. [2] [3] [4]
Illness scripts form through deliberate case practice. Worksheet and case-based approaches help learners build usable scripts rather than isolated facts. Enabling conditions include age, season, exposures and comorbidity. Fault is the mechanism. Consequences are the findings you expect. [2] [20] [21]
Common traps have plain English meanings. Anchoring is sticking to the first label. Availability is over-calling whatever you saw last week. Confirmation bias is hunting only for data that fit. Search-satisfying is stopping at the first positive finding. Diagnostic momentum is copying a previous label without re-thinking. Premature closure is ending the search too early. Context and production pressure make all of them more likely. [3] [12] [22]
Heuristics can be healthy. A toddler with coryza, wheeze and seasonal exposure may correctly trigger a bronchiolitis script. Bias begins when the heuristic silences competing threats or ignores mismatch. [14]
Feedback closes the learning loop. Without knowing what the diagnosis became, your future confidence is uncalibrated. The diagnosis learning cycle treats feedback as essential infrastructure, not a courtesy. [18]
Clinical Presentation
Reasoning starts before the first question. Who looks frightened? Is the adolescent silent while an adult answers everything? Is the medically complex child’s carer already saying “this is not their normal”? Those observations belong in the representation. [15] [17]
Age changes the same disease into different stories. Neonates offer feeding, tone, colour and temperature. Infants offer consolability, gaze and wet nappies. Toddlers offer play, limp and proxy history. School-age children can locate pain but may hide school fear. Adolescents may delay help until a confidential space opens. [1] [10]
| Life stage | High-value features for the sentence | Classic premature-closure trap |
|---|---|---|
| Neonate | Gestation, day of life, feeding, tone, colour, temperature, perinatal risk | Labelling non-specific signs as 'poor feeding' only |
| Young infant | Consolability, gaze, intake, wet nappies, caregiver baseline change | 'Just a virus' despite 'not right' |
| Toddler | Play, limp, breathing effort, ingestion opportunity, injury mechanism | Accepting an implausible fall story without curiosity |
| Preschool | Speech change, gait, fever pattern, abdominal pain location if reliable | Leading questions that invent a tidy script |
| School-age | Child's own symptom account, school function, focal findings | 'Growing pains' or 'attention seeking' without examination |
| Adolescent | Private agenda, collapse context, substances, self-harm, pregnancy possibility | Adult assumptions because of body size |
| Complex chronic | What is different from usual, devices, emergency plan | Attributing everything to the known diagnosis |
Serious disease often hides inside ordinary complaints: fever, vomiting, limp, abdominal pain, headache, behavioural change or school refusal. Your job is not to panic at every common symptom. Your job is to notice mismatch, tempo, red-flag clusters and caregiver concern. [9] [12]
Apparently reassuring fragments do not end the story. A smiling toddler can still have evolving surgical abdomen. An afebrile neonate can still be septic. A normal oxygen saturation does not prove safe ventilation. A low early-warning score does not cancel a dangerous differential. [9] [14]
Differential Diagnosis
Build the list in this order: what can kill now, what is likely, what is reversible, and what is most harmful to miss. Specialty silos come later. [8] [9]
Keep the bedside list short enough to use. Three to five active items is common. Expand when the child is unstable, the data are poor, or the first script fails. Always name the residual must-not-miss items that remain open even if you act on a common working diagnosis. [8]
Immediate threat categories
- Airway threat or respiratory failure
- Shock or evolving circulatory failure
- Seizure, raised intracranial pressure or reduced consciousness
- Time-critical infection in a young infant
- Metabolic crisis, dangerous hypoglycaemia or adrenal crisis
Common high-volume scripts
- Self-limited viral illness
- Reactive airway patterns in season
- Gastroenteritis with preserved perfusion
- Minor injury with plausible mechanism
- Only after threat screen and mismatch check
Hidden serious scripts
- Cardiac disease mimicking respiratory disease
- Inborn error or endocrine crisis mimicking sepsis
- Non-accidental injury inside an 'accident' label
- Ingestion inside behavioural change
- Surgical abdomen inside 'gastro'
Context scripts
- Technology failure in complex children
- Safeguarding and fabricated illness concerns
- Psychosocial crisis with medical mimicry
- Medication effect or withdrawal
- Travel, outbreak and exposure-modified infection risk
Flexible differentials are a taught skill. After the first positive test, ask what else could still be true. After the first treatment response, ask what has not been ruled out. [8]
Safeguarding differentials need calm curiosity. Inconsistent mechanism, delayed presentation, injury incompatible with development, or repeated unexplained events keep non-accidental injury or neglect open. That is not the same as public accusation. Document exact words and follow local pathways. [13]
Clinical & Bedside Assessment
If the child is unstable, treat first. Gather AMPLE history in parallel: allergies, medicines, past history, last meal, events. Reasoning continues, but oxygen, airway support, glucose and seizure control do not wait for a perfect sentence. [14] [17]
When you can pause for thirty seconds, write or say the representation. [1] [5]
- Age and developmental stage.
- Baseline health, devices and usual carers.
- Tempo and semantic features of the present illness.
- Current physiological state and trajectory.
- Leading threat and top working scripts.
- Caregiver concern and data-quality limits. [1] [5] [15]
Example: “Previously well 9-day-old with 12 hours of poor feeding and cool peripheries; possible late-onset sepsis or cardiac ductal emergency; caregiver says the baby is not himself; needs immediate senior review.” That sentence is more useful than a five-minute chronology. [10] [15]
Use professional interpreters for clinical content. Records, growth charts, prior discharges and device downloads are part of assessment. For complex children, ask what is different from usual and read the emergency plan. [17]
Perform a diagnostic pause when the fit is poor, the stakes are high, or several people are uneasy. [6] [9]
- What is the one-sentence representation now?
- What are the top three threats?
- What would change my mind?
- What must I not miss?
- Who else should look? [6] [9] [14]
Common technique errors manufacture bad data: leading preschool questions, talking only to one parent, ignoring the child’s own words, accepting a sibling as interpreter, and examining so roughly that fear is misread as neurological change. [1] [13]
Investigations
Tests should discriminate among the active differential. A reflex panel is not reasoning. Ask, before each test: which script does this support or weaken, and will the result change tonight’s plan? [9] [14]
Bedside checks for immediately reversible threats continue during assessment: glucose when consciousness or feeding is off, oximetry when breathing is the concern, and other local time-critical bedside tests. These are part of threat control, not a full diagnostic panel. [14]
Interpret results against pre-test concern. A normal early inflammatory marker does not cancel a high-risk neonate story. A single normal imaging study does not end a must-not-miss differential if the clinical trajectory is wrong. Conversely, an incidental abnormality should not create diagnostic momentum away from the real problem. [9] [11]
Age and baseline change interpretation. Children with medical complexity often live with abnormal numbers. Compare with their usual, not only with a population reference. [17]
Harms of over-testing include delay, distress, sample-volume burden, false positives and cascading procedures. Harms of under-testing include delayed source control and missed reversible disease. Choose the discriminating middle. [9] [19]
Management — Resuscitation
When life threat and uncertainty coexist, treat the threat. Call for help. Start age-adapted ABCDE. Keep the differential open while you act. Empiric antimicrobials, airway support or glucose correction are treatments of time-critical risk, not proof of one diagnosis. [9] [14]
Allocate cognitive roles if you can. One clinician leads the hands-on tasks. Another watches for mismatch, tracks the differential and prepares handover. Closed-loop communication protects both action and thinking. [14] [16]
Family presence needs a brief explanation: what you fear, what you are doing, and that the exact cause may still be uncertain. Do not invent certainty to sound kind. Kindness is clarity plus competence. [15]
Personalised emergency plans, steroid cards, shunt or ventilator baselines and allergy alerts enter both resuscitation and the representation immediately. [17]
Management — Definitive & Stepwise
After immediate threats are controlled, follow a repeatable algorithm. [1] [8] [9]
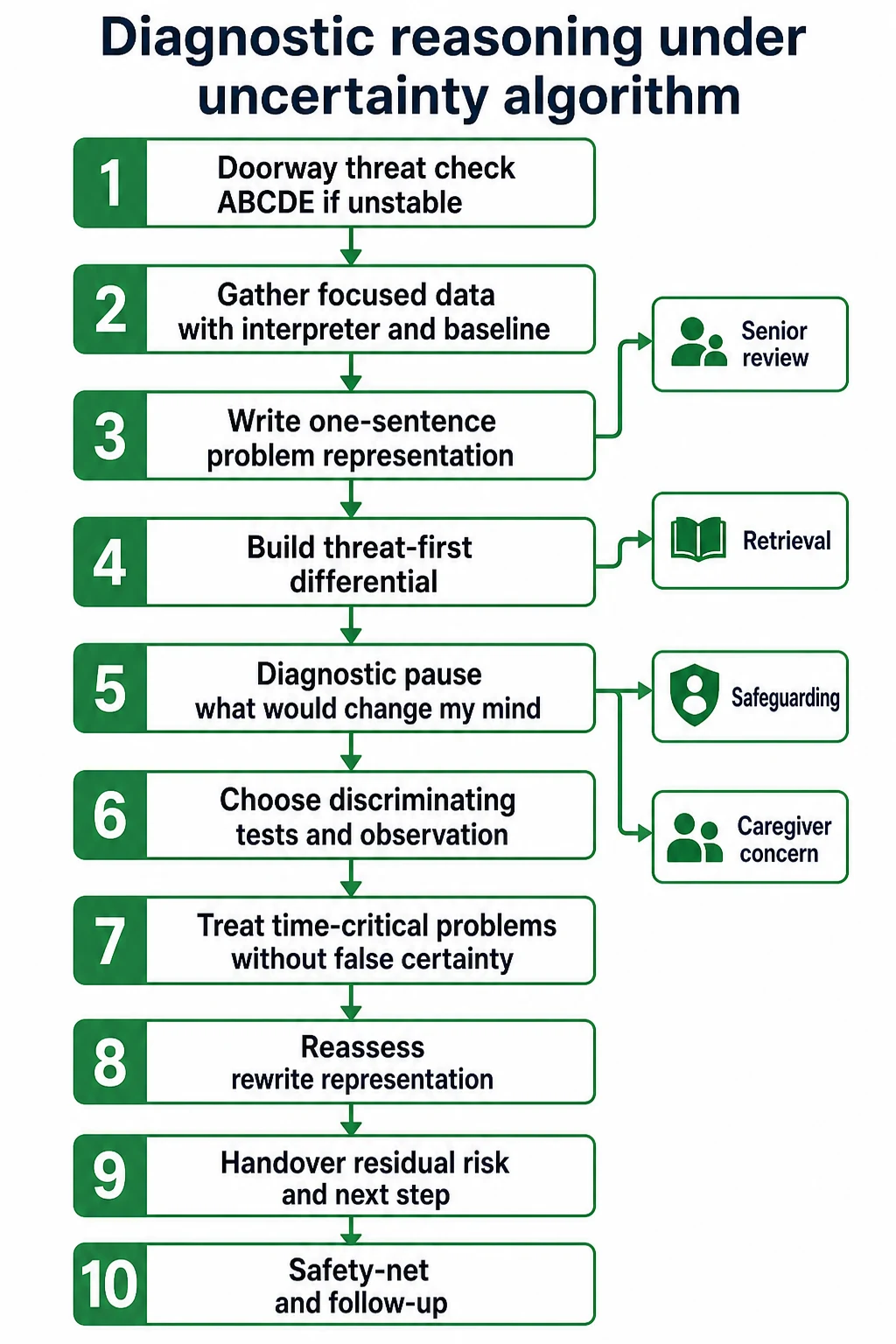
- Update the problem representation with the latest physiology and data quality.
- Rank the differential by threat, likelihood, reversibility and harm of delay.
- Hold a diagnostic pause if the fit is poor or the stakes are high.
- Choose tests and observation intervals that discriminate.
- Treat time-critical problems while naming residual risks.
- Reassess and rewrite the sentence after each major result or response.
- Decide disposition by residual risk and rescue capability, not by label alone.
- Hand over representation, differential, actions, response and next discriminating step.
- Safety-net the family with concrete return triggers and teach-back.
- Seek later diagnostic feedback so your calibration improves. [8] [16] [18]
Structured handoff programmes reduce medical errors in multicentre paediatric work. Use whatever local tool you have, but never drop residual diagnostic risk from the packet. [16]
Shared decisions under uncertainty sound like this: “I think the most likely problem is X. I am still protecting against Y. Here is what we will do now, what we will watch for, and when to come back.” That is safer than false reassurance or an unsorted catalogue of rare diseases. [8] [15]
Specific Subtypes & Scenarios
Neonate with poor feeding. Represent day of life, gestation, feeding, tone, colour and temperature. Keep sepsis, cardiac ductal emergency, metabolic disease and non-accidental injury open until the data allow narrowing. [10]
Infant “not right”. Encode caregiver concern explicitly. Mild numbers do not cancel the sentence. Escalate observation threshold. [15]
Fever without source. Age band changes the must-not-miss list. Young infants need a different threat posture from vaccinated toddlers with a clear focus. Do not let “viral season” erase bacteraemia, urinary infection or evolving sepsis scripts. [9]
Breathing difficulty. Separate upper airway, lower airway, parenchyma, cardiac mimic, metabolic acidosis and disordered drive. A cardiac script can look respiratory. [9] [14]
Limp or refusal to walk. Infection, inflammation, trauma, malignancy and safeguarding all compete. “Pulled muscle” is a late label, not a first sentence. [12] [13]
Vomiting and abdominal pain. Medical, surgical, metabolic, migraine, ingestion and psychosocial scripts can coexist. Trajectory and examination discriminators matter more than the first symptom word. [9]
Altered behaviour or consciousness. Infection, seizure, toxin, metabolic disease, trauma and non-accidental injury remain open while you protect airway and glucose. [9] [13]
Return after a viral label. Rewrite from scratch. Compare with the first visit. Ask what changed and whether the safety net was usable. [9] [12]
Medical complexity. Baseline abnormal findings are not the new problem. Ask what is different. Device failure can be the diagnosis. [17]
Language-discordant family. Poor data quality is part of the representation. Use a professional interpreter before you trust subtle history. [19]
Telehealth or rural first contact. State what cannot be examined. Escalate earlier when residual risk is high. [14] [19]
Possible maltreatment. Hold the differential open. Document. Treat injuries. Follow mandatory pathways. Avoid corridor confrontation. [13]
Adolescent mixed agenda. Keep biomedical and psychosocial differentials concurrent. Confidentiality limits still apply when safety is at risk. [1]
Rare or undiagnosed disease. When the common scripts fail and perinatal or multi-system clues accumulate, widen deliberately rather than forcing a common label. [10]
Complications & Pitfalls
Premature closure is the headline error: the search ends while a dangerous script is still plausible. The damage may appear hours later as a return visit, an arrest call or a delayed theatre transfer. [9] [11]
False reassurance from a single normal number is next. Normal blood pressure, temperature, saturation, early-warning score or first laboratory panel can coexist with evolving disaster. [9] [14]
Anchoring on the triage note, availability from the last case, confirmation bias in the notes, search-satisfying after one positive finding, and diagnostic momentum from a previous discharge letter are daily risks on paediatric wards. Hierarchy can silence the nurse or student who sees the mismatch. [3] [12] [22]
Ignoring caregiver concern discards high-value data. Over-calling “anxiety” or “social” without a medical look is the mirror-image error. [15] [13]
Over-testing harms. Under-testing harms. Treating a presumed label so hard that the true problem is masked also harms. Handover that keeps the label but drops residual risk restarts the error on the next shift. [16] [19]
Prognosis & Disposition
Disposition follows residual risk and rescue capability more than the neatness of the label. A provisional viral working diagnosis may be acceptable for home only if red flags are absent, understanding is checked, return is feasible, and caregiver concern is not unresolved. [15] [8]
Trajectory matters. Improving physiology with a coherent script supports step-down. Flat or worsening trajectory with an uncertain script supports observation, admission, senior review or retrieval. [14]
Safety-net in concrete language: what to watch for, when to return, how to get help overnight, and what the next planned review is. Pending results need an owner. [18]
When the true diagnosis later differs from your working label, seek the feedback. That is how calibration improves for the next child. [18]
Recurrent presentations, unexplained deterioration or ongoing caregiver concern should widen both the biomedical differential and the safeguarding review. [13] [15]
Special Populations
Neonates and ex-preterm infants need wide early differentials and perinatal precision. Non-specific signs are the rule, not the exception. [10]
Immunocompromised children may lack classic inflammatory cues. Represent the immune context explicitly. [9]
Medical complexity and technology dependence require baseline-aware scripts and device failure on the list. Caregiver expertise is data. [17]
Disability and neurodiversity change communication and pain behaviour. Do not force typical scripts onto atypical baselines. [17]
Indigenous families need culturally safe partnership without stereotype. Ask who should be present and what support structures matter. [19]
Migrant and refugee families need interpreters, trauma-aware pacing and respect for interrupted records. [19]
Socioeconomic disadvantage changes whether a safety net is usable. A plan the family cannot enact is not a plan. [19]
Out-of-home care and youth justice bring fragmented historians and legal complexity. Represent data-quality limits. [13]
Gender and sexually diverse youth need affirming language and concurrent psychosocial differentials without voyeurism. [1]
Maltreatment contexts require open differentials, careful documentation and mandatory pathways. Cognitive traps are common here. [13]
Evidence, Guidelines & Regional Differences
Educational evidence supports teaching problem representation and illness scripts as practical tools rather than abstract theory. Bowen’s synthesis remains a core map of diagnostic-reasoning education. Illness-script theory has three decades of development and classroom application. Case-based worksheets help learners build scripts deliberately. [1] [2] [20] [21]
Empirical work shows expert–novice differences in problem-representation synthesis. ART and its validation studies give teachers a structured way to coach hypothesis generation and metacognition. Flexible-differential exercises make residual risk visible. [5] [6] [7] [8]
Dual-process and debiasing literature explains origins of bias and the limits of simple “think harder” advice. Context shapes error. Healthy heuristics and betraying biases both appear in acute decision-making reviews. [3] [4] [14] [22]
Paediatric diagnostic-error evidence includes critical-care systematic review, inpatient cognitive-bias teaching cases, perinatal rare-disease reasoning, maltreatment-specific cognitive traps, and recent paediatric diagnostic-safety priority setting. Caregiver concern has prospective association with critical illness. Handoff redesign reduces medical errors. Medical-complexity guidance explains baseline-aware reasoning. Feedback frameworks support calibration. [11] [12] [10] [13] [19] [15] [16] [17] [18] [9]
Controversies remain. Debiasing training is not a magic shield. Forced analytic checklists can help or can become paperwork. Adult emergency diagnostic-error literature should not be copied wholesale into neonates. State uncertainty honestly. [3] [11] [19]
Partnering-with-consumers and open-disclosure expectations shape how uncertainty is explained, not the physiology of disease. State, territory and New Zealand retrieval and mandatory-reporting rules change who you call and what you document. Cultural safety for Aboriginal and Torres Strait Islander families, and Te Tiriti-informed care for Māori whānau, belong inside diagnostic partnership. [19]
MRCPCH history, communication and clinical stations reward a clear representation, prioritised differential and honest uncertainty. Four-nation safeguarding and information-sharing rules affect documentation language. Local NHS diagnostic-safety programmes change governance vocabulary more than bedside ABCDE. [1] [8]
ABP diagnosis tasks and ACGME clinical-reasoning milestones treat reasoning as a core competency. RCPSC medical-expert and communicator EPAs do the same through entrustable activities. Local malpractice climate may change documentation tone; it should not invent false certainty. [5] [6] [19]
Exam Pearls
- Lead with a one-sentence problem representation before any differential list. [1] [5]
- Include age, baseline, tempo, key features, physiology and leading threat in that sentence. [1]
- Rank differentials by threat, likelihood, reversibility and harm of delay. [8]
- Name residual must-not-miss items even when a common working diagnosis is reasonable. [8] [9]
- Use fast recognition for clean matches; force analytic checks for mismatch and high stakes. [3] [4]
- Put caregiver concern into the representation. [15]
- Rewrite after every major data point or treatment response. [8] [18]
- Do not close on one normal number, score or early test. [9] [14]
- Hand over residual risk and the next discriminating step. [16]
- In long case, the representation is the spine of the presentation. [1] [5]
- In communication stations, explain uncertainty without flooding families with unsorted rare lists. [8]
- Classic traps: “just viral,” “just gastro,” “just a pulled muscle,” “just anxiety,” “known complex child being usual.” [9] [12] [17]
- Safeguarding stays on the list through curiosity and documentation, not corridor accusation. [13]
- Seek diagnostic feedback later; calibration is part of competence. [18]
SCRIPT pause before you lock the label
References
- [1]Bowen JL Educational strategies to promote clinical diagnostic reasoning. The New England journal of medicine, 2006.PMID 17124019
- [2]Custers EJ Thirty years of illness scripts: Theoretical origins and practical applications. Medical teacher, 2015.PMID 25180878
- [3]Croskerry P Cognitive debiasing 1: origins of bias and theory of debiasing. BMJ quality & safety, 2013.PMID 23882089
- [4]Croskerry P Deciding about fast and slow decisions. Academic medicine : journal of the Association of American Medical Colleges, 2014.PMID 24362398
- [5]McQuade CN Characteristics differentiating problem representation synthesis between novices and experts. Journal of hospital medicine, 2024.PMID 38528679
- [6]Thammasitboon S The Assessment of Reasoning Tool (ART): structuring the conversation between teachers and learners. Diagnosis (Berlin, Germany), 2018.PMID 30407911
- [7]Thammasitboon S Psychometric validation of the reconstructed version of the assessment of reasoning tool. Medical teacher, 2021.PMID 33073665
- [8]Bergl PA Keeping a Flexible Differential Diagnosis: an Exercise in Clinical Reasoning. Journal of general internal medicine, 2019.PMID 30847831
- [9]Bordini BJ Overcoming Diagnostic Errors in Medical Practice. The Journal of pediatrics, 2017.PMID 28336147
- [10]Bordini BJ Undiagnosed and Rare Diseases in Perinatal Medicine: Lessons in Context and Cognitive Diagnostic Error. Clinics in perinatology, 2020.PMID 32000918
- [11]Cifra CL Diagnostic Errors in Pediatric Critical Care: A Systematic Review. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2021.PMID 33833203
- [12]Berkwitt A Cognitive bias in inpatient pediatrics. Hospital pediatrics, 2014.PMID 24785565
- [13]Laskey AL Cognitive errors: thinking clearly when it could be child maltreatment. Pediatric clinics of North America, 2014.PMID 25242711
- [14]Mangus CW Decision Making: Healthy Heuristics and Betraying Biases. Critical care clinics, 2022.PMID 34794630
- [15]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [16]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [17]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [18]Fernandez Branson C Improving diagnostic performance through feedback: the Diagnosis Learning Cycle. BMJ quality & safety, 2021.PMID 34417335
- [19]Rasooly IR Priorities for improving paediatric diagnosis: findings from a modified Delphi study. BMJ quality & safety, 2026.PMID 42362363
- [20]Levin M Teaching Clinical Reasoning to Medical Students: A Case-Based Illness Script Worksheet Approach. MedEdPORTAL : the journal of teaching and learning resources, 2016.PMID 31008223
- [21]Keemink Y Illness script development in pre-clinical education through case-based clinical reasoning training. International journal of medical education, 2018.PMID 29428911
- [22]Croskerry P Context is everything or how could I have been that stupid? Healthcare quarterly (Toronto, Ont.), 2009.PMID 19667765