Paeds · clinical-assessment-and-reasoning
Developmental surveillance and milestone assessment
Also known as Developmental screening · Milestone assessment · Developmental surveillance · ASQ developmental screen · M-CHAT autism screen
Fellowship approach to developmental surveillance, evidence-informed milestones, standardised screening including autism tools, early referral, equity and exam performance from infancy through early childhood.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
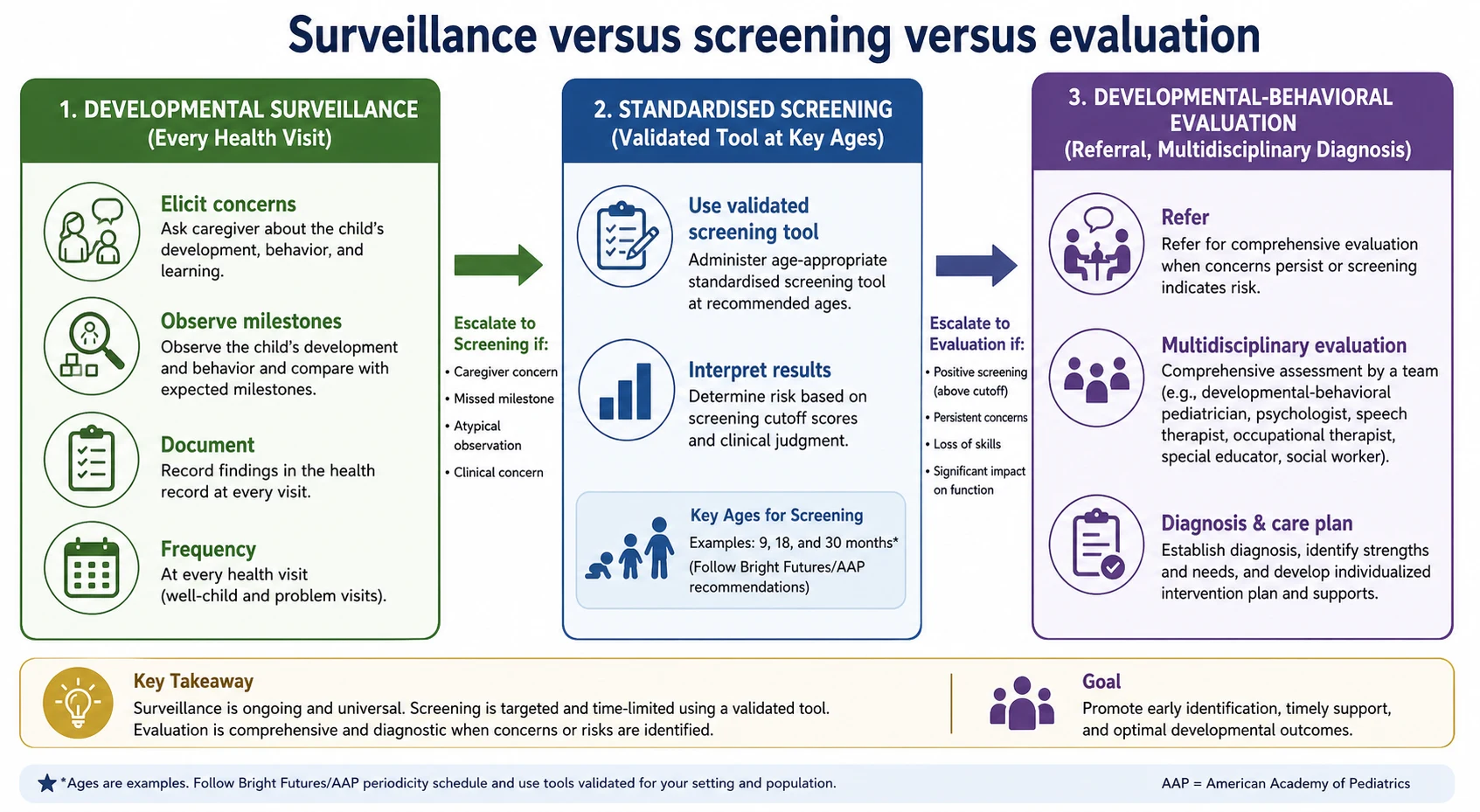
These distinctions are central to AAP guidance on identifying developmental disorders early. [1]
S.C.R.E.E.N. in clinic
Overview & Definition
Parents often notice first. Your job is to turn that notice into a structured process that does not lose the child in a “wait and see” fog. Developmental surveillance is the continuous process of asking, watching and documenting. Developmental screening is the periodic use of a standardised tool with known performance characteristics. Developmental evaluation is the deeper assessment that can establish diagnoses and intervention plans. [1]
A milestone is an observable skill that most children of a given age have achieved. Tools and lists must be evidence-informed. CDC and AAP collaborative work revised surveillance milestones so that listed skills are achieved by most children at that age, reducing false reassurance from outdated “average age” lists. [2]
This page owns surveillance and screening logic. Cross-link growth charting, physical examination, autism management, genetics and school-age learning topics rather than hiding full specialty chapters here. [1]
Classification
Classify the encounter purpose. A well-child visit needs full surveillance. An acute fever visit still needs a quick check if the caregiver raises a developmental worry or if regression is mentioned. Classify the finding: isolated skill lag, multi-domain delay, social communication pattern concerning for autism, plateau, or true regression. [1] [3]
Autism-specific tools such as M-CHAT-R/F are not general developmental screens. They target social communication risk and need the follow-up interview pathway described in validation work. [3]
Epidemiology & Risk Factors
Missed or late identification is common when services are fragmented, visits are rushed, or families face language and transport barriers. Children with medical complexity can have diagnostic overshadowing: clinicians attribute everything to the known condition and stop looking for treatable developmental needs. [4]
Caregiver concern is a high-value signal in acute illness work and the same clinical habit applies here: take “I am worried about speech” seriously even before a score exists. [5] Language discordance without professional interpreting degrades both history and counselling about results. [6]
Pathophysiology
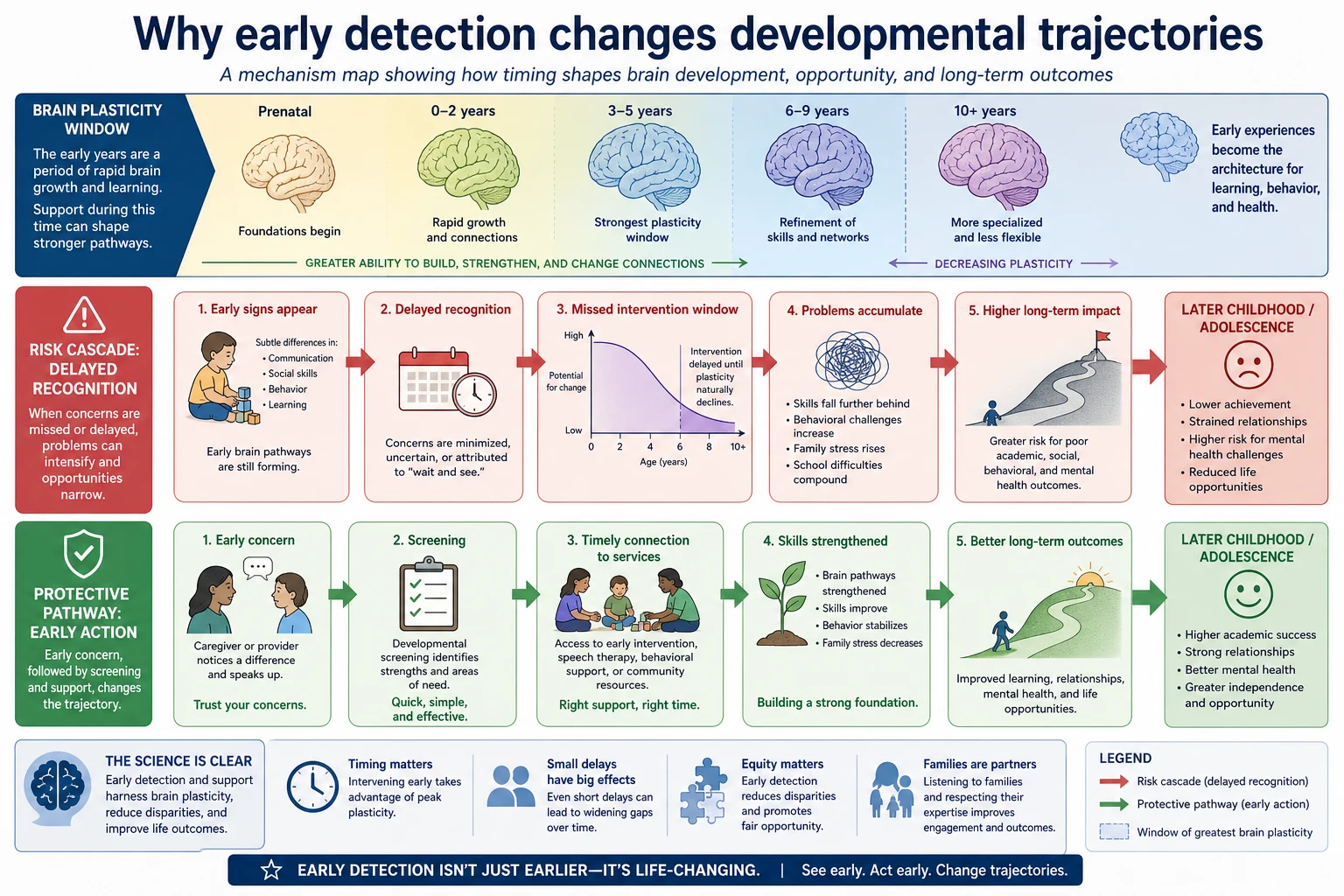
Early childhood is a period of high developmental plasticity. Skills build on prior skills. When hearing loss, severe visual impairment, untreated seizures, severe malnutrition, toxic stress or lack of opportunity interrupt input, the visible milestone pattern changes. That does not mean every delay is environmental, and it does not mean biology is destiny. It means timing of detection changes how much catch-up support can do. [1] [2] [9]
Trauma and adversity can alter behaviour, attention and social engagement. Trauma-informed care avoids blaming families while still completing a careful developmental assessment. [9]
Clinical Presentation
A caregiver may say the child is “in their own world,” “not talking like cousins,” or “was saying words and stopped.” You may see reduced joint attention, limited gesture, toe-walking with language delay, or a preschooler who cannot follow simple dual commands. Regression of language or social skills is never a routine “wait.” It needs prompt evaluation for autism-related regression, neurological disease and hearing problems. [1] [3]
Differential Diagnosis
Separate global developmental delay from isolated speech delay. Consider hearing impairment in any language concern. Consider autism spectrum when social communication and restricted patterns dominate. Consider intellectual disability evaluation pathways when adaptive skills and cognition are broadly affected. Consider neglect or extreme psychosocial deprivation when the environment cannot support development — and open safeguarding routes without abandoning medical evaluation. [1] [9]
Clinical & Bedside Assessment
Start with open questions: “Do you have any concerns about how your child is learning, playing, speaking or moving?” Then watch the child on the floor or in the caregiver’s lap. Note eye contact, response to name, gesture, babble or words, pincer, sit/stand/walk, and how the child uses the caregiver for comfort. [1] [2]
Use an evidence-informed milestone list appropriate to age. Do not invent personal cut-offs. If surveillance raises concern, or the child reaches a recommended screening age, administer a validated general developmental screen used by your service. For autism risk at the toddler ages supported by evidence, use M-CHAT-R/F with follow-up interview rather than treating a single checkbox form as diagnosis. [2] [3]
Document domain by domain. Source-attribute who reported each skill. Hand over clearly if another clinician will complete screening. [7]
Investigations
Screens guide referral; they rarely replace hearing and vision checks when communication is delayed. Targeted medical testing belongs with evaluation teams unless red flags demand urgent neurology review. Avoid ordering broad genetic panels from a single missed milestone without context. [1]
Management — Resuscitation
True developmental surveillance is usually outpatient. Exceptions: acute regression with encephalopathy, seizures, severe dehydration with collapse, or safeguarding emergencies. Those use acute paediatric pathways first. [1] [9]
Management — Definitive & Stepwise
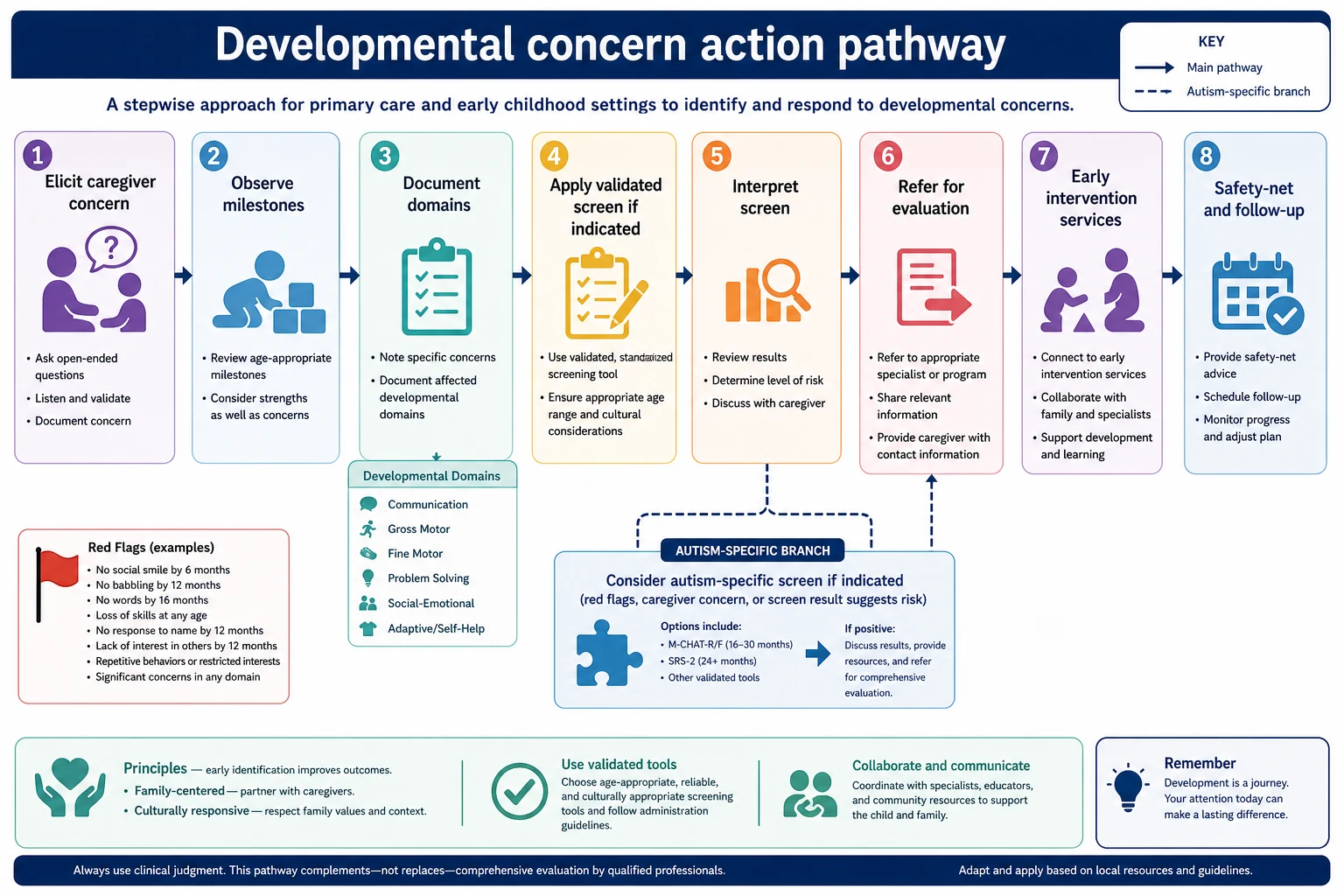
- Complete surveillance every visit.
- Deploy validated screening on schedule or on concern.
- Interpret with clinical judgement — strong concern can justify referral even if a family declines a tool.
- Refer early to developmental-behavioural, allied health and early intervention services per local pathways.
- Explain results with teach-back and a written plan.
- Safety-net: what to watch for, when to return, how to chase referrals. [1] [3] [10]
Consent and assent principles still apply when you discuss referral and information sharing with schools or agencies. [8]
Specific Subtypes & Scenarios
Ex-preterm infant. Use corrected age for early milestones as your local developmental follow-up protocol advises, and do not skip surveillance because the neonatal course was “explained.” [1]
Medical complexity. Ask what is new for this child, not only what is typical for the diagnosis. [4]
Language-discordant family. Use professional interpreters for screening questions and result counselling. [6]
Possible autism at 18–24 months. Use autism-specific screening with follow-up and refer promptly on positive pathways or strong clinical concern. [3]
Regression. Urgent structured evaluation; do not rebook in six months as first action. [1]
Complications & Pitfalls
“Wait and see” after clear caregiver concern. Treating a screen as a diagnosis. Reassuring on an outdated milestone list. Ignoring hearing. Losing families on long waitlists without interim support. Incomplete handover of screening results. [1] [2] [7]
Prognosis & Disposition
Earlier access to intervention services improves functional outcomes for many children with developmental disorders. Disposition is not only “refer and forget”: give interim strategies, community supports and a clear chase plan for appointments. [1] [10]
Special Populations
NICU graduates, children with known genetic syndromes, neurodiverse families seeking affirming care, Indigenous families needing culturally safe services, migrant and refugee families with interrupted care, and children in out-of-home care all need active surveillance rather than passive assumptions. [4] [6] [9]
Evidence, Guidelines & Regional Differences
AAP clinical guidance (Lipkin and colleagues) sets the surveillance-plus-screening framework for identifying developmental disorders. [1] Zubler and colleagues provide evidence-informed milestone content for surveillance tools. [2] Robins and colleagues validated M-CHAT-R/F for toddler autism risk screening with follow-up. [3]
Use local child health books, jurisdictional screening schedules and early childhood early intervention pathways. Cultural safety and interpreter access are part of valid surveillance. [6]
NICE autism recognition guidance and healthy child programme schedules shape referral thresholds; map local community paediatric and SALT pathways. [1]
Bright Futures and AAP schedules drive screening ages; provincial Canadian programmes vary — state the local tool rather than inventing universal cut-offs. [1] [2]
Exam Pearls
- Surveillance is every visit, not only immunisation days. [1]
- Use evidence-informed milestones, not memory folklore. [2]
- A screen is not a diagnosis. [3]
- Strong concern can justify referral even when paperwork is incomplete. [1]
- Always consider hearing in language delay. [1]
- Document domains and source of each skill report. [7]
- Safety-net the referral wait. [10]
References
- [1]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [2]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [3]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [4]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [5]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [6]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [7]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [8]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [9]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [10]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428