Paeds · clinical-assessment-and-reasoning
Diagnostic test selection and Bayesian reasoning in paediatrics
Also known as Bayesian reasoning paediatrics · Likelihood ratios children · Sensitivity specificity paediatrics · Pre-test probability children · Diagnostic test interpretation paediatrics · Choosing investigations children
A fellowship approach to choosing and interpreting paediatric tests: pre-test probability, sensitivity, specificity, predictive values, likelihood ratios, residual risk, over-testing traps, age-specific reference intervals, and shared decisions from neonate to transition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
You are about to order a test for a child. The useful question is not “what can I order?” It is “what do I believe now, and will this result change what I do next?” That is Bayesian reasoning in ordinary English. You start with a clinical story and a rough pre-test probability. The test updates that probability. Then you act on the new probability and the residual risk that remains. [2] [5] [26]
A pre-test probability is your estimate that the target condition is present before the result returns. It comes from age, tempo, findings, exposure, comorbidity and local epidemiology. It does not need false decimal precision. High, intermediate or low is often enough if you are honest about uncertainty. [2] [7]
A diagnostic test is any information that changes probability. History and examination are tests. Glucose, urine culture, rapid antigen assay, decision rules and imaging are tests. So is watching the child for two hours. The laboratory is not the only place Bayesian thinking lives. [2] [26]
The bedside Bayesian pathway
Name the question
What condition am I trying to raise or lower, and why does that matter now?
Estimate pre-test risk
Use age, findings, trajectory and caregiver concern. Keep must-not-miss risk explicit.
Decide if a test is needed
If no result will change action or residual risk, observe and safety-net instead.
Choose the discriminating test
Prefer the least harmful method that actually separates the active scripts.
Update and act
Convert the result into post-test probability, residual risk, plan and handover.
Classification
Diagnostic metrics answer different questions. Mixing them is the classic exam trap. [1] [2]
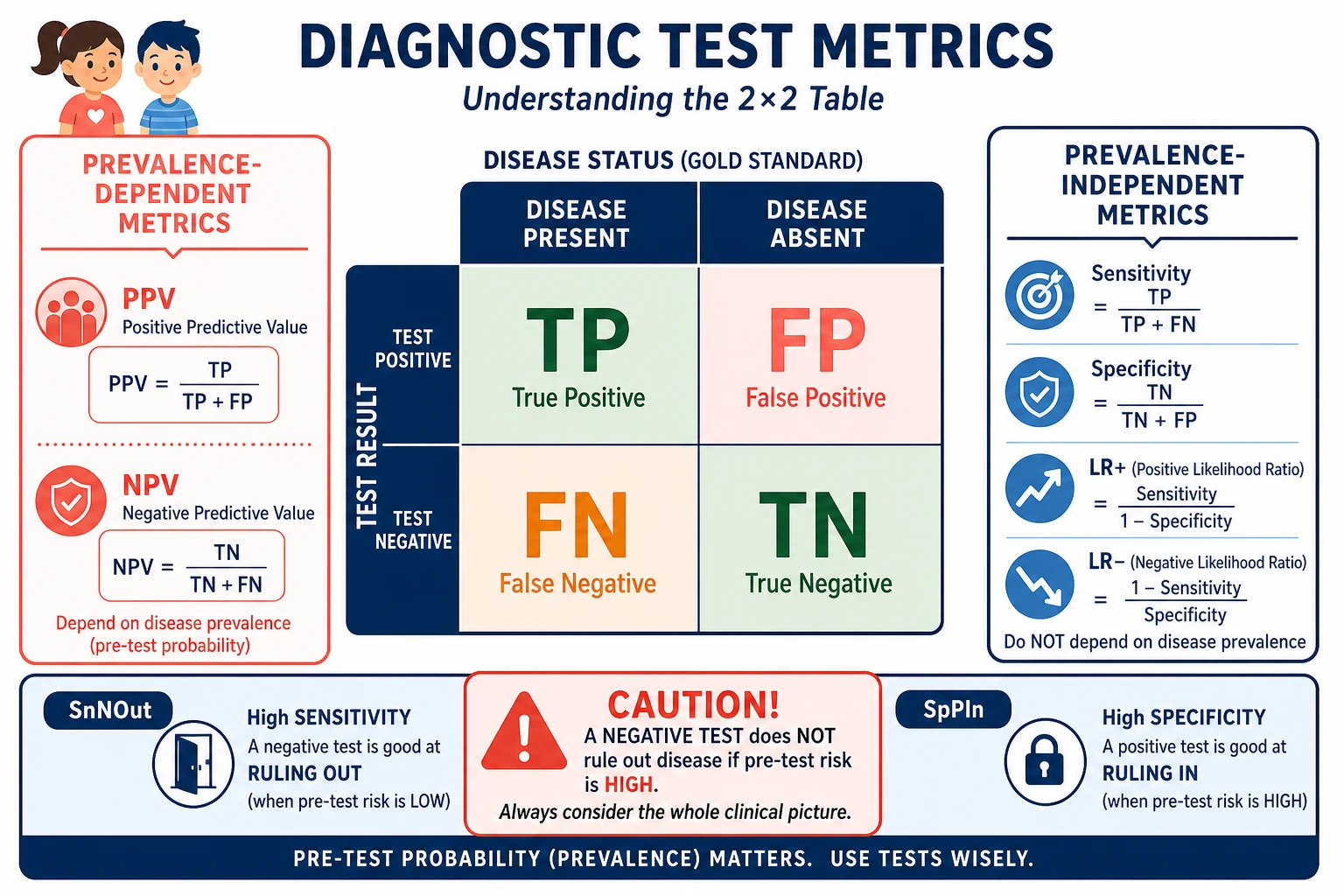
Read the figure like this: if the stem asks whether a test “rules out” disease, you need sensitivity, pre-test risk and residual risk — not PPV. If the stem asks what a positive result means in a rare disease, prevalence and PPV dominate. [1] [4]
| Metric | Plain question it answers | Prevalence dependent? |
|---|---|---|
| Sensitivity | Among children with disease, how often is the test positive? | No (in formula) |
| Specificity | Among children without disease, how often is the test negative? | No (in formula) |
| PPV | Among positive tests, how often is disease truly present? | Yes |
| NPV | Among negative tests, how often is disease truly absent? | Yes |
| LR+ | How much does a positive result raise the odds of disease? | No (in formula) |
| LR− | How much does a negative result lower the odds of disease? | No (in formula) |
LR+ is sensitivity divided by (1 − specificity). LR− is (1 − sensitivity) divided by specificity. A larger LR+ is a stronger rule-in push. A smaller LR− is a stronger rule-out push. Rough teaching bands often used in viva language: LR+ above about 10 is strong; LR− below about 0.1 is strong. Those bands are guides, not laws. Always return to the child’s pre-test risk. [2] [4]
Tests also classify by purpose: [1] [7] [24]
- Screening accepts more false positives to avoid missing disease in asymptomatic groups.
- Diagnosis aims to change management in a symptomatic child.
- Monitoring tracks trajectory or treatment effect.
- Prognosis estimates future risk rather than current disease labels. [1] [7] [24]
Continuous tests need cut-offs. ROC thinking shows the trade between sensitivity and specificity as the threshold moves. A lower cut-off catches more disease and creates more false positives. Choose the cut-off for the clinical job, not for a prettier curve. [3]
Epidemiology & Risk Factors
There is no single rate of “wrong test use in childhood.” Overuse and underuse both appear, and they concentrate in different places. European Academy of Paediatrics statements and multi-country surveys highlight overtesting and overtreatment as real paediatric safety problems. Adult emergency pathways applied to children can add low-value panels. At the same time, high-risk neonates and complex children are harmed when weak negatives are trusted. [18] [19] [23] [25]
Raises pre-test risk
- Young infant or neonate with non-specific signs
- Immunocompromise or medical complexity
- Caregiver concern that the child is not themselves
- Return visit or night deterioration
- Focal findings that fit a dangerous script
Lowers pre-test risk
- Well appearance with a clear self-limited script
- Validated very-low-risk decision-rule features
- Short, improving trajectory
- No caregiver residual concern after shared review
- Local epidemiology against the feared disease
Distorts published accuracy
- Spectrum bias and referral filters
- Verification bias
- Imperfect reference standards
- Adult-derived cut-offs
- Case-mix unlike your ward or ED
Drives over-testing
- Order-set defaults
- Defensive culture
- Protocol stacking
- Incidental finding cascades
- Production pressure without senior pause
Disease rarity is not a theoretical nuisance. In low-prevalence settings, even a fairly specific test produces many false positives. That is base-rate arithmetic, not pessimism. It is why indiscriminate panels in well children manufacture work. [1] [24]
Pathophysiology
Bayes’ theorem is the mechanism. Pre-test odds times the likelihood ratio become post-test odds. Convert back to probability if you need a number families can hear. Fagan-style nomograms and teaching tools exist so you can see the update without pretending you do long arithmetic in a corridor. [2] [4] [5] [6]
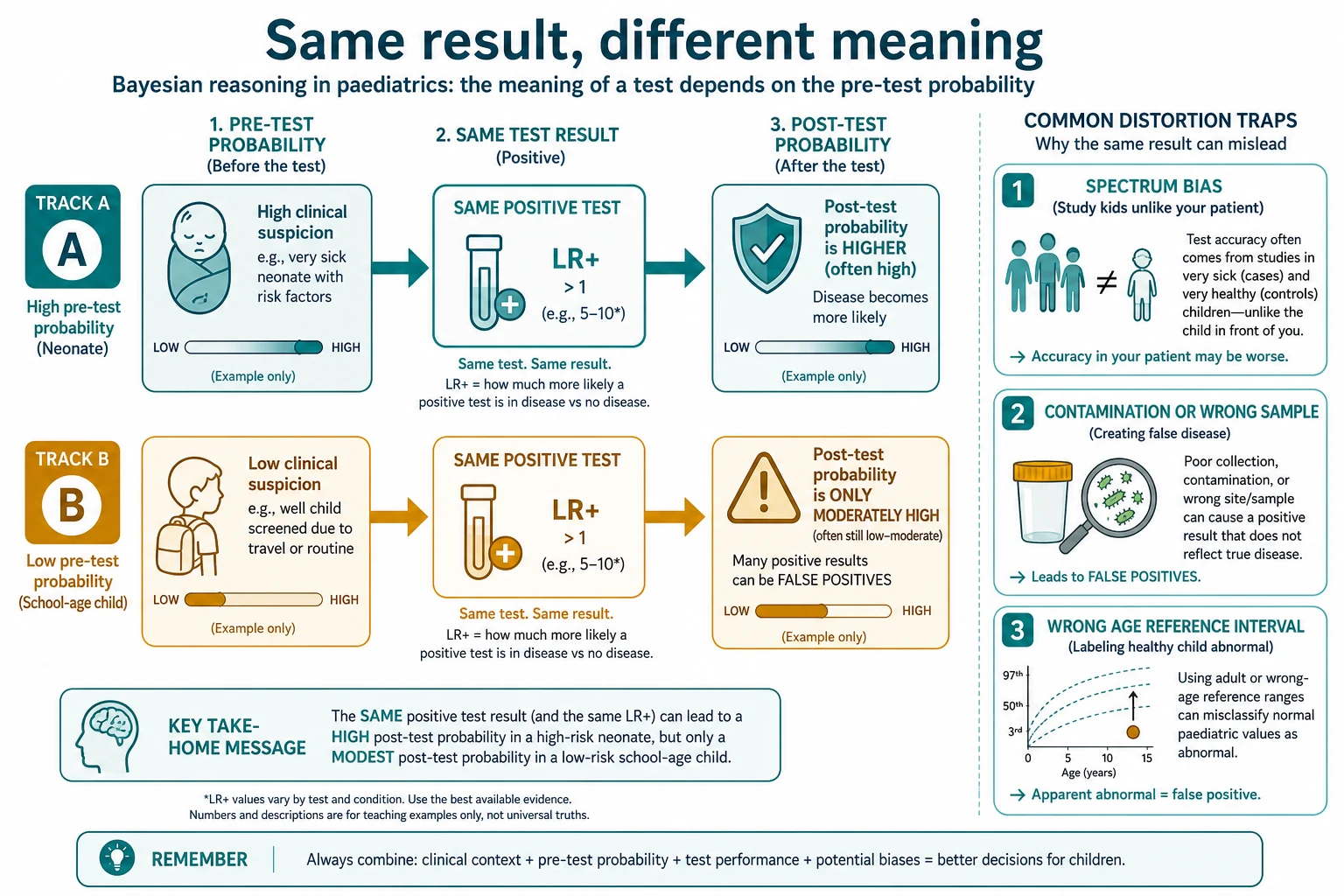
Read the figure like this: a positive result is not a diagnosis. It is a push. The size of the push depends on the LR. The meaning of the landing place depends on where you started. [2] [4]
Why children specially break lazy adult habits: [16] [17] [25]
- Compensation hides disease. Early markers can be normal while threat evolves.
- Age changes base rates and reference intervals. Adult ranges mislabel healthy children.
- Samples are hard. Bag urine, haemolysis and tiny volumes create false signals.
- Spectrum differs. Accuracy measured in severe tertiary cases may not match your clinic.
- Cascades hurt more. Radiation, sedation, blood loss and family burden are not free. [16] [17] [18] [25]
Threshold thinking closes the loop. Below a test threshold, observe. Between test and treatment thresholds, gather discriminating information. Above the treatment threshold, act for the condition even if some uncertainty remains. Those thresholds move with harm of delay, harm of treatment, setting and rescue capability. [7]
Clinical Presentation
Presentation is pre-test data. Before you open the order screen, ask what you already know. [26] [25]
A neonate with poor feeding, cool hands and a worried parent is already a high-risk story. An adolescent with two days of coryza and a normal examination is a different story. The same CRP request is not the same clinical act. [22] [25] [26]
Caregiver concern that the child is “not themselves” belongs in the pre-test estimate. So do return visits. A second story is new Bayesian data, not a nuisance. [25]
Age changes which findings carry weight: [26]
- Neonate: day of life, tone, colour, temperature, feeding, perinatal risk.
- Infant: consolability, intake, wet nappies, work of breathing, caregiver baseline.
- Toddler: play, limp, hydration, focus of infection, stranger distress as noise.
- School-age: focal pain maps, trauma mechanism, school and activity change.
- Adolescent: confidential exposures, mixed biomedical and psychosocial scripts, adult-sized physiology with paediatric disease lists still open. [26]
Unstable presentation changes the testing sequence. Protect airway, breathing, circulation and glucose first. Bedside tests that alter immediate action run in parallel. Non-discriminating panels wait. [7] [25]
Differential Diagnosis
Tests should separate the scripts still on the table. If your differential is “viral versus everything,” a shotgun panel will not think for you. Rebuild the problem representation, then pick the discriminator. [26] [25]
Threat-first testing means: [2] [7]
- What can kill or disable soon?
- Which reversible causes need a fast bedside answer?
- Which common scripts are still likely?
- Which test best moves the most important probabilities?
- Which residual risks stay open after a negative or positive result? [2] [7]
False positives create fake differentials. A contaminated urine culture can send you down pyelonephritis theatre while the real problem is viral sepsis or metabolic disease. An incidental imaging finding can steal the afternoon. Keep the original clinical question pinned to the top of the note. [16] [24]
Sometimes the correct differential management is no new test tonight. That is still a Bayesian decision: post-test probability after history and examination already sits below the test threshold, residual risk is acceptable, and safety-net is usable. [7] [18]
Clinical & Bedside Assessment
Before every order, say four lines out loud or write them: [2] [7] [21]
- Clinical question.
- Pre-test risk and must-not-miss residual.
- How a positive result would change action.
- How a negative result would change action. [2] [7] [21]
If you cannot answer lines 3 and 4, do not order the test. [2] [7]
History and examination have operating characteristics too. A clear croup bark raises one script. Peritonism raises another. Capillary refill, work of breathing and interaction are bedside tests with imperfect reliability, but they still update risk when used carefully. [20] [26]
Technique errors manufacture false data: [16] [17]
- leading questions in preschoolers
- bag urine treated as a clean sample
- wrong cuff size or agitated vitals treated as disease
- adult reference ranges on paediatric labs
- interpreting a single snapshot without trajectory [16] [17]
Use professional interpreters when language is limited. Poor history is a bad test. Do not upgrade laboratory noise to compensate for a missing story. [25]
Investigations
This section is the core skill. [2] [7]
1. Estimate pre-test probability without fake precision
Use bands: low, intermediate, high. Anchor on age, findings, epidemiology and validated rules when they fit the child in front of you. Decision rules for minor head trauma show how structured low-risk features can support imaging restraint when applied to the correct population. They do not replace examination or residual clinical concern. [12] [13] [2]
2. Choose tests that discriminate
For suspected appendicitis, history, examination, laboratory tests and point-of-care ultrasound each contribute imperfect information. The point is sequence and combination, not worship of one modality. [20]
For bronchiolitis that fits the script, chest radiography often fails to improve care and can increase unnecessary treatment. High-reliability programmes have reduced radiograph use without abandoning clinical judgement when the question changes. [10] [11]
For pharyngitis, rapid antigen testing sits inside stewardship and pre-test scoring, not as a stand-alone reflex in every red throat. [14] [15]
For suspected UTI, collection method changes the meaning of a positive culture. Contamination rates differ by method. A positive culture from a poor sample is not automatic disease. [16]
3. Interpret with LR thinking
Convert the result into a probability update. Teaching tools and nomograms help learners see the move. Then ask whether you have crossed a decision threshold. [2] [4] [5] [6] [21]
4. Respect paediatric reference intervals
Children are not small adults. CALIPER and related work show why age-partitioned intervals matter for laboratory interpretation. An “abnormal” flag can be a software error relative to childhood physiology. [17]
5. Appraise the accuracy paper before you trust the number
STARD tells authors what to report. QUADAS-style tools help you ask whether patient selection, index test, reference standard and flow were trustworthy. Spectrum and verification bias are not pedantry. They are why a glossy sensitivity fails on your shift. [8] [9]
6. Handle imperfect and pending results
Contaminated, haemolysed or mistimed samples need method review before treatment momentum. Pending cultures need an owner, a timeframe and a plan if positive or negative. A normal early marker in a high-risk infant is not a discharge stamp. [16] [22] [25]
Management — Resuscitation
When the child is unstable, testing serves resuscitation. It does not lead it. [7] [25]
- Call for help and start age-adapted ABCDE.
- Check immediately reversible threats, including glucose when consciousness or feeding is wrong.
- Draw the discriminating urgent samples while you secure access if that will not delay oxygen, airway or perfusion care.
- Give time-critical treatment on clinical probability when delay is more dangerous than residual uncertainty.
- Keep the differential open. A first lactate, gas or culture does not prove a single label. [7] [25]
Tell the family what you fear and what you are doing now. “We are treating for serious infection while we look for the source” is clearer than a catalogue of assays. [25]
Management — Definitive & Stepwise
After threat control, use a repeatable algorithm. [2] [7] [18]
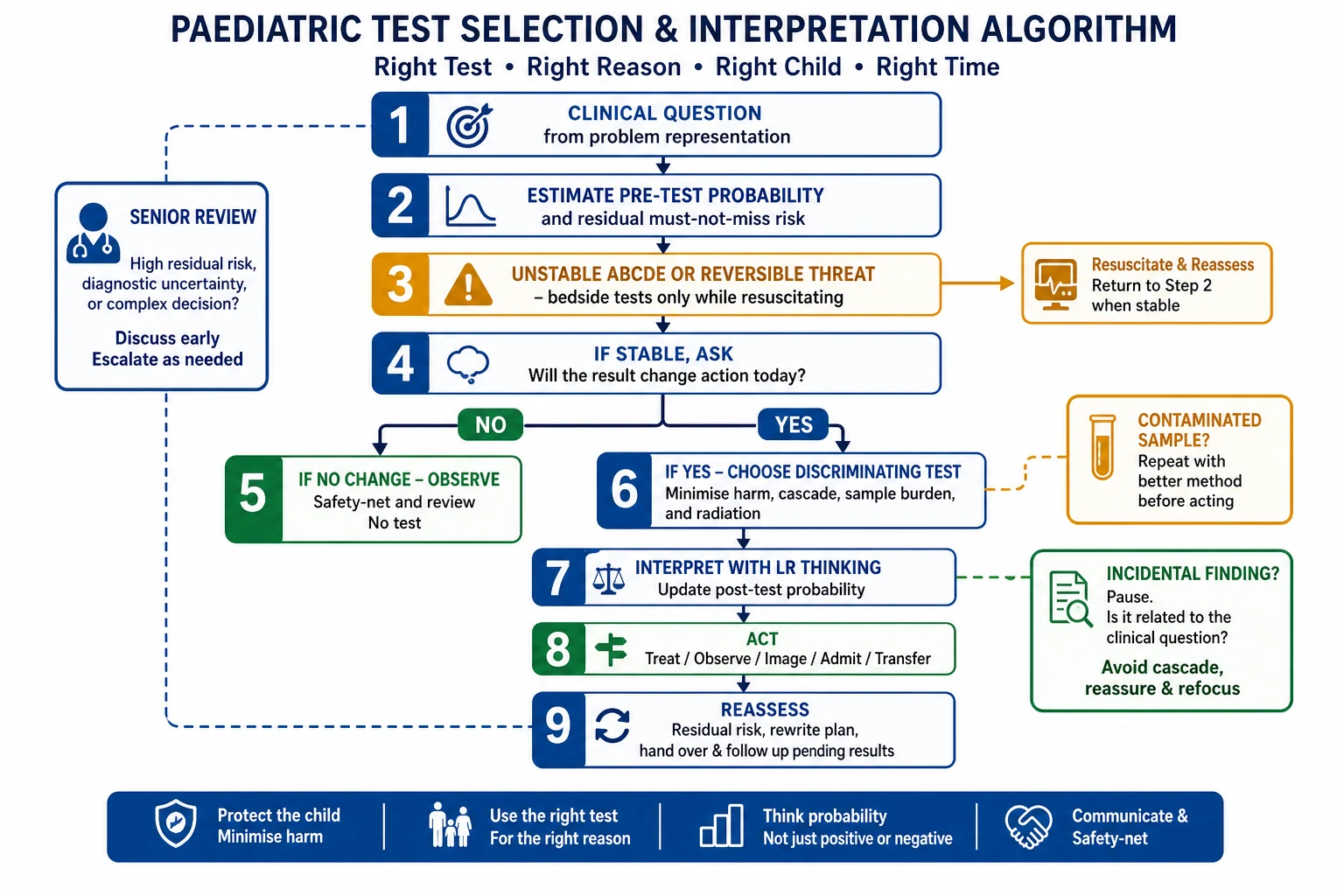
- Write the clinical question from the problem representation.
- Estimate pre-test probability and residual must-not-miss risk.
- If ABCDE is failing, limit to bedside tests that change immediate action.
- If stable, ask whether any result will change today’s action or safety-net.
- If not, observe, explain and safety-net.
- If yes, choose the least harmful discriminating test.
- Interpret with probability update, not binary magic.
- Act: treat, image, admit, transfer, or continue observation.
- Reassess residual risk after the result and after the response to treatment.
- Hand over pending results, owner, expected impact and residual risk.
- Seek later feedback when the final diagnosis differs from your working label. [2] [7] [21] [25]
Shared decisions need plain language: “I think the chance of X is low enough that more tests would more likely mislead than help. Here is what would make me change my mind.” Or: “The chance is high enough that we should treat now while confirmatory tests return.” [7] [18]
Specific Subtypes & Scenarios
Febrile young infant. Age band and appearance dominate pre-test risk. Prediction research can refine risk estimates, but local protocols and residual clinical concern still govern action. A single reassuring number does not erase a high-risk age band. [22]
Minor head trauma. Validated low-risk rules can identify children at very low risk of clinically important brain injury and support selective CT. Apply the rule only when the child matches the studied population, and never against evolving neurology. [12] [13]
Bronchiolitis. When history and examination fit, routine chest radiography is often low value and can increase unnecessary antibiotics or admissions. Reopen imaging if focal findings, severe course or alternative scripts appear. [10] [11]
Pharyngitis. Use pre-test clinical likelihood and stewardship principles around rapid antigen testing rather than testing every sore throat in a vacuum. [14] [15]
Suspected UTI. Choose collection method deliberately. Interpret culture in light of contamination risk and urinalysis context. [16]
Appendicitis pathway. Combine history, examination and selected imaging or laboratory data as a sequence of imperfect updates. No single finding is the whole story. [20]
Simple febrile seizure in an adult ED. Adult defaults can over-test children. Re-centre on paediatric pre-test risk and local paediatric guidance. [23]
Technology-dependent child. Compare with personal baseline, not only population ranges. Device issues can be the diagnosis. [17] [25]
Incidental abnormality. Ask whether it answers the original question. If not, avoid cascade unless independent red flags appear. [18] [24]
Rural or telehealth first contact. State what cannot be examined or sampled. Transfer earlier when residual risk is high and local testing cannot resolve it. [7]
Complications & Pitfalls
Base-rate neglect. Treating sensitivity as if it were PPV. [1]
False reassurance. Trusting a negative test that was never sensitive enough for the pre-test risk. [2] [25]
False disease. Contamination, wrong reference interval, colonisation or spectrum-mismatched accuracy claims. [16] [17] [9]
Anchoring on the first abnormal number. The child becomes “the hyponatraemia” while the real script is missed. [25]
Diagnostic momentum from a useless test. Once ordered, everyone feels obliged to chase it. [24]
Overdiagnosis and overtreatment cascades. More data create more labels and more harm without improving outcomes. [18] [24]
Under-testing the high-risk child. “They always have funny numbers” is not a safety strategy. [22] [25]
Repeating the same low-yield test on return without rewriting the clinical question. [25]
Handover of results without residual risk. The next team inherits a number, not a plan. [25]
Prognosis & Disposition
Disposition follows post-test probability, residual risk and rescue capability. A normal panel does not guarantee safe discharge if the story remains high risk or the family cannot use the safety-net. An abnormal but explained finding does not mandate admission if residual risk is low and follow-up is solid. [7] [18]
Pending results need: [25]
- who owns them
- when they are expected
- what action a positive or negative will trigger
- how the family is contacted [25]
Observation is a diagnostic strategy when thresholds are intermediate and the child can be watched safely. Timed reassessment updates probability with trajectory. [7]
When the final diagnosis differs from your working label, seek the feedback. That is how future pre-test estimates improve. [21] [25]
Special Populations
Neonates and young infants. High cost of false negatives. Non-specific signs. Sample-volume limits. Age-banded pathways matter. [22]
Immunocompromised children. Inflammatory markers and “well appearance” can mislead. Widen testing questions earlier. [25]
Medical complexity and technology dependence. Personal baselines, device failure and polypharmacy interactions change both pre-test risk and result meaning. [17] [25]
Disability and neurodiversity. Examination findings used as “tests” need baseline-aware interpretation. [25]
Indigenous, migrant and language-discordant families. Consent, explanation and follow-up access shape whether a testing plan is real. Use interpreters. Avoid stereotype-based pre-test guesses. [18]
Socioeconomic disadvantage. A plan that requires private transport, unpaid leave or phone access the family lacks is not a safe observe-without-testing plan. [18]
Out-of-home care. Fragmented prior results and historians increase uncertainty. Represent data-quality limits. [25]
Adolescents. Confidential sexual-health testing, consent capacity and adult ED defaults all change the pathway. [23]
Maltreatment contexts. Both under-investigation and over-calling create harm. Document carefully and follow mandatory pathways. [25]
Evidence, Guidelines & Regional Differences
Paediatric primers by Akobeng remain high-yield for sensitivity, specificity, predictive values, likelihood ratios and ROC curves. Deeks’ likelihood-ratio note and Fagan/Caraguel nomogram teaching support bedside update language. Pauker and Kassirer supply threshold logic for whether to test at all. [1] [2] [3] [4] [5] [6] [7]
STARD 2015 and QUADAS-2 frame critical appraisal of diagnostic accuracy evidence. Educational work on Bayesian apps shows the concept can be taught, but apps do not replace clinical thresholds. Diagnostic-error models remind us that underdiagnosis, overdiagnosis and misdiagnosis are related failure modes. [8] [9] [21] [24] [25]
Condition examples used in this topic are source-bound: bronchiolitis radiograph utility and reduction programmes; PECARN-style head-trauma rules and later validation work; rapid antigen testing for group A streptococcus; urine collection contamination; CALIPER reference-interval thinking; EAP overtesting statements; appendicitis modality synthesis; febrile-infant prediction research; adult-ED overtesting examples. Do not export any single study’s cut-offs as universal local protocol. [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] [22] [23]
Controversies remain. Numeric false precision flatters examiners and misleads families. AI diagnostic tools will need STARD-style reporting and spectrum checks before bedside trust. Adult accuracy claims often fail in neonates. Stewardship must not become denial of needed tests for high residual risk. [8] [18] [24]
Partnering-with-consumers and open-disclosure expectations shape how uncertain results are explained. Local laboratory intervals, radiation stewardship and retrieval capability change which tests are available on site versus after transfer. Cultural safety for Aboriginal and Torres Strait Islander families, and Te Tiriti-informed care for Māori whānau, belong inside shared testing decisions. [18]
MRCPCH theory loves metric definitions and interpretation traps. Clinical and communication stations reward residual-risk language after results. Local fever and head-injury style pathways operationalise thresholds; they do not abolish Bayesian thought. [1] [2] [12]
ABP epidemiology and diagnosis tasks, ACGME clinical-reasoning milestones and RCPSC medical-expert EPAs all treat test selection as core competence. PECARN-style rules and Choosing Wisely culture are influential teaching examples. CALIPER-informed paediatric interval thinking is especially visible in Canadian laboratory education. Remote geography changes transfer-before-test decisions. [12] [13] [17] [18]
Exam Pearls
- Write the clinical question before the order. [26]
- Sensitivity and specificity are not predictive values. [1]
- PPV falls when prevalence falls. [1]
- Post-test odds = pre-test odds × LR. [2] [4]
- A negative test does not rule out disease if pre-test risk is high and LR− is weak. [2]
- A positive test does not rule in disease if pre-test risk is tiny and false positives dominate. [1] [4]
- History and examination are Bayesian tests. [26]
- Decision rules reduce imaging only when the child matches the rule population. [12] [13]
- Bag urine contamination can manufacture UTI labels. [16]
- Use age-specific reference intervals. [17]
- Bronchiolitis that fits clinically often does not need a chest radiograph. [10] [11]
- STARD and QUADAS language wins critical-appraisal vivas. [8] [9]
- Threshold approach: observe, test or treat. [7]
- Hand over residual risk and pending-result ownership. [25]
- Over-testing and under-testing are both diagnostic errors. [18] [24]
PROBE before you order
References
- [1]Akobeng AK Understanding diagnostic tests 1: sensitivity, specificity and predictive values. Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17407452
- [2]Akobeng AK Understanding diagnostic tests 2: likelihood ratios, pre- and post-test probabilities and their use in clinical practice. Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17306009
- [3]Akobeng AK Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17376185
- [4]Deeks JJ Diagnostic tests 4: likelihood ratios. BMJ (Clinical research ed.), 2004.PMID 15258077
- [5]Fagan TJ Letter: Nomogram for Bayes's theorem. The New England journal of medicine, 1975.PMID 1143310
- [6]Caraguel CG The two-step Fagan's nomogram: ad hoc interpretation of a diagnostic test result without calculation. Evidence-based medicine, 2013.PMID 23468201
- [7]Pauker SG The threshold approach to clinical decision making. The New England journal of medicine, 1980.PMID 7366635
- [8]Bossuyt PM STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ (Clinical research ed.), 2015.PMID 26511519
- [9]Whiting PF QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Annals of internal medicine, 2011.PMID 22007046
- [10]Schuh S Evaluation of the utility of radiography in acute bronchiolitis. The Journal of pediatrics, 2007.PMID 17382126
- [11]Frazier SB Reducing Chest Radiographs in Bronchiolitis Through High-Reliability Interventions. Pediatrics, 2021.PMID 34344801
- [12]Kuppermann N Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet (London, England), 2009.PMID 19758692
- [13]Holmes JF PECARN prediction rules for CT imaging of children presenting to the emergency department with blunt abdominal or minor head trauma: a multicentre prospective validation study. The Lancet. Child & adolescent health, 2024.PMID 38609287
- [14]Cohen JF Rapid antigen detection test for group A streptococcus in children with pharyngitis. The Cochrane database of systematic reviews, 2016.PMID 27374000
- [15]Cohen JF Group A Streptococcus pharyngitis in Children: New Perspectives on Rapid Diagnostic Testing and Antimicrobial Stewardship. Journal of the Pediatric Infectious Diseases Society, 2024.PMID 38456797
- [16]Guri A Contamination rates of different methods of urine culture collection in children: A retrospective cohort study. Journal of paediatrics and child health, 2021.PMID 33760325
- [17]Adeli K The Canadian laboratory initiative on pediatric reference intervals: A CALIPER white paper. Critical reviews in clinical laboratory sciences, 2017.PMID 29017389
- [18]Størdal K Overtesting and overtreatment-statement from the European Academy of Paediatrics (EAP). European journal of pediatrics, 2019.PMID 31506723
- [19]Jankauskaite L Overuse of medical care in paediatrics: A survey from five countries in the European Academy of Pediatrics. Frontiers in pediatrics, 2022.PMID 36177454
- [20]Benabbas R Diagnostic Accuracy of History, Physical Examination, Laboratory Tests, and Point-of-care Ultrasound for Pediatric Acute Appendicitis in the Emergency Department: A Systematic Review and Meta-analysis. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, 2017.PMID 28214369
- [21]Kinnear B Integrating Bayesian reasoning into medical education using smartphone apps. Diagnosis (Berlin, Germany), 2019.PMID 30817298
- [22]Burstein B Prediction of Bacteremia and Bacterial Meningitis Among Febrile Infants Aged 28 Days or Younger. JAMA, 2026.PMID 41359314
- [23]Louie JP When less is more: Overdiagnosis and overtesting in pediatric febrile seizures in the adult emergency department. The American journal of emergency medicine, 2025.PMID 40532406
- [24]Newman-Toker DE A unified conceptual model for diagnostic errors: underdiagnosis, overdiagnosis, and misdiagnosis. Diagnosis (Berlin, Germany), 2014.PMID 28367397
- [25]Bordini BJ Overcoming Diagnostic Errors in Medical Practice. The Journal of pediatrics, 2017.PMID 28336147
- [26]Bowen JL Educational strategies to promote clinical diagnostic reasoning. The New England journal of medicine, 2006.PMID 17124019