Paeds · clinical-assessment-and-reasoning
Fatigue and lethargy in children and adolescents
Also known as Paediatric fatigue · Childhood lethargy · Tired child · ME/CFS children · Chronic fatigue children
An age-aware fellowship approach to fatigue and lethargy in children and adolescents: distinguish emergency lethargy from tiredness, build a threat-first differential, investigate directed, stabilise acute presentations, and plan stepwise care including sleep, iron deficiency, post-viral and ME/CFS pathways without harmful forced exercise.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A parent says their child is “always tired.” That sentence can mean three different problems. The first is ordinary sleep debt after late nights and early school. The second is medical energy failure — anaemia, heart or lung disease, infection, endocrine disease, or evolving malignancy. The third is a chronic multi-domain fatigue pattern, sometimes after infection, where activity is followed by a delayed crash. Your job is to sort these without missing the child who looks quiet because they are seriously ill. [1] [5] [6]
Sister pages own deep disease algorithms: recognising the seriously ill child, pallor and anaemia pathways, weight-loss work-up, and sleep or mental-health leaves. This page owns the presentation logic for fatigue and lethargy. [8] [13]
T.I.R.E.D. G.A.T.E.
Overview & Definition
Picture two children in the waiting room. One school-age child sits up, answers questions, and says they feel wiped after late gaming. Another infant lies still, barely tracks your face, and the parent says “this is not my baby.” Both may be labelled “tired” by a triage note. Only one is using emergency language. [8] [14]
Fatigue means reduced energy or stamina with preserved interaction. The child can still engage, though they may stop sport or need more rest. Lethargy means reduced responsiveness or spontaneous activity that worries a clinician. In infants and young children, lethargy sits next to altered consciousness. Treat it as a threat until you prove otherwise. [8] [15]
Chronic labels such as myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) are clinical diagnoses made after a careful process. They are not a bin for every unexplained tired child on day three of a viral illness. Severe paediatric ME/CFS is uncommon but highly disabling when present, as British Paediatric Surveillance Unit work shows. [2] [3] [2]
Classification
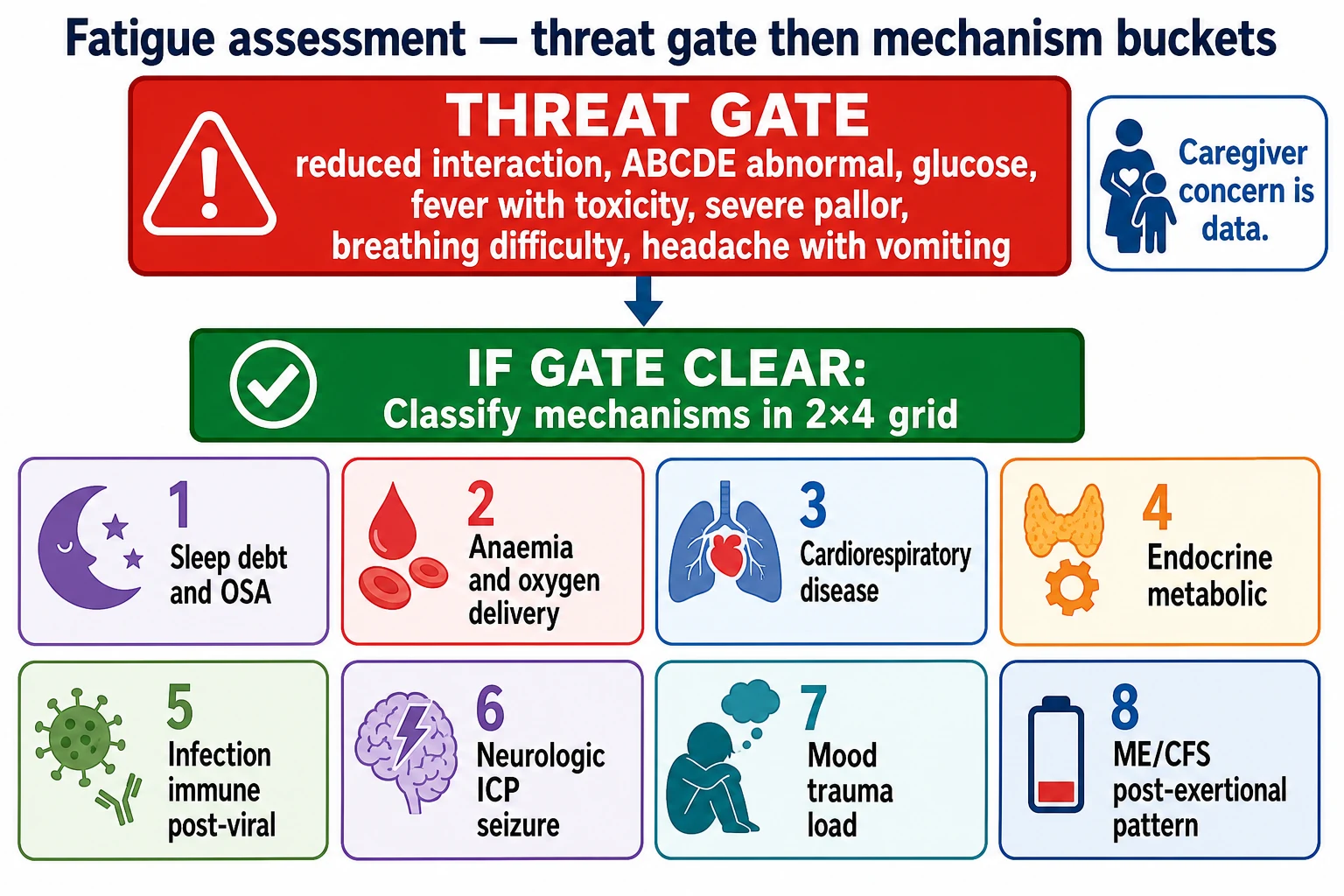
Classify in two moves, not twenty. [1] [6]
Move 1 — acuity gate. Is this an emergency lethargy picture? Reduced interaction, abnormal airway or breathing, poor perfusion, low glucose risk, fever with toxicity, severe pallor, or neurologic red flags push you into ABCDE and sepsis-capable care. Caregiver concern that the child is worse belongs in this gate. [8] [14] [15]
Move 2 — mechanism buckets once the child is stable enough to think in systems: [1] [4] [6]
- Sleep opportunity debt and sleep-disordered breathing.
- Anaemia and oxygen-delivery failure.
- Cardiorespiratory disease and high work of breathing or low cardiac output.
- Endocrine and metabolic energy failure.
- Infection, post-infectious and immune inflammatory states.
- Neurologic threat, including raised intracranial pressure and post-ictal states.
- Mood, trauma load and school stress — concurrent, not last-resort only.
- Post-exertional ME/CFS pattern after directed exclusion. [1] [4] [5] [6] [12] [16]
Duration helps. Hours to days with toxicity suggests acute disease. Weeks suggest subacute organic or post-viral patterns. Months with post-exertional crashes raise ME/CFS considerations after you have looked for treatable disease. [2] [5] [17]
Epidemiology & Risk Factors
Tiredness is one of the commonest non-specific complaints in school-age and adolescent clinics. True emergency lethargy is less common and clusters with infection, metabolic crisis, trauma, intoxication and severe anaemia. [1] [15]
Sleep debt rises with late bedtimes, early school starts, screens in bedrooms and competitive sport schedules. Obstructive sleep apnoea risk rises with adenotonsillar hypertrophy, obesity, craniofacial difference and some neuromuscular disease. [6]
Iron deficiency remains a major reversible contributor across infancy dietary risk groups and menstruating adolescents with heavy periods. Powers and colleagues summarise prevention, screening and treatment principles for paediatric iron deficiency and iron-deficiency anaemia. [4] [19]
Infection and post-infectious states matter. Infectious mononucleosis classically leaves adolescents exhausted for weeks. EBV and other infections can precipitate longer post-viral syndromes and, in some children, ME/CFS phenotypes. Post-COVID condition research in children and young people is evolving; use it as context, not as a single diagnostic shortcut. [5] [16] [17]
Social determinants change detection. Food insecurity, crowded housing, trauma, racism and language discordance delay care and hide history. Medical complexity raises baseline fatigue and can hide new deterioration if you do not ask “what is different from usual?” [11] [12] [13]
Severe ME/CFS in children and young people is rare at population level but devastating for affected families. BPSU surveillance described recognition delays and major functional loss, including education collapse. [2] [3]
Pathophysiology
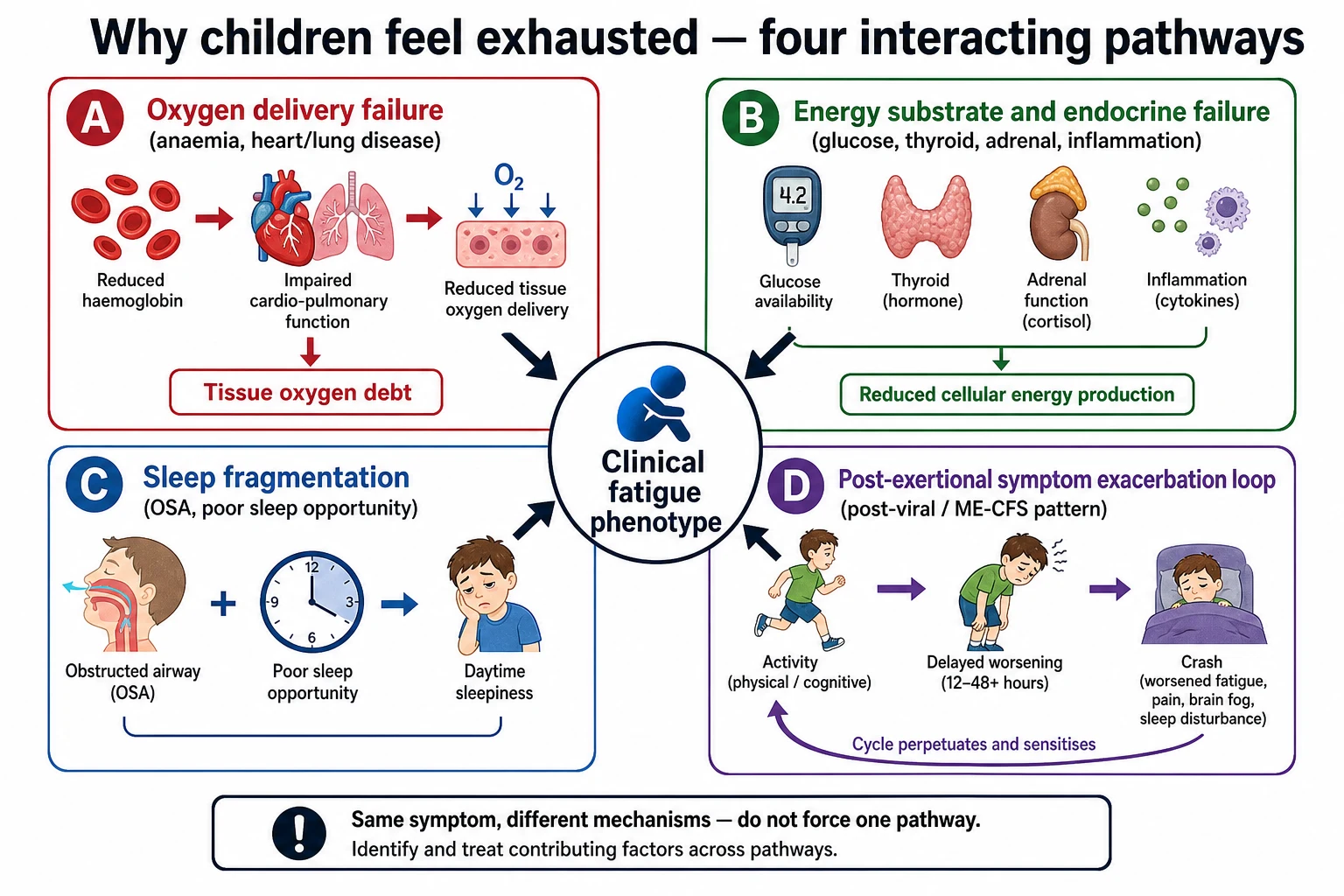
Fatigue is a final common symptom, not a single pathway. [1] [4]
Oxygen delivery fails when haemoglobin is low, lungs cannot oxygenate, or the heart cannot deliver flow. The child may look pale, tachypnoeic or tachycardic before they look “dramatic.” Age-normal ranges matter; a heart rate that is fine for an adult can be wrong for a toddler. [4] [14]
Substrate and endocrine failure include hypoglycaemia, thyroid disease, adrenal crisis and systemic inflammation that raises resting energy need while suppressing appetite. Polyuria and polydipsia with weight loss should make you think of new diabetes before you call the problem “tiredness.” [15]
Sleep fragmentation from obstructive apnoea prevents restorative sleep. Daytime sleepiness, behavioural change, mouth breathing and snoring are clues. Treating the airway problem treats the daytime phenotype. [6]
Post-exertional symptom exacerbation is the ME/CFS teaching point examiners want. Activity is followed by a delayed crash that is out of proportion to the effort. Older exam folklore sometimes pushed forced graded exercise as universal therapy. Contemporary NICE-aligned teaching emphasises energy management and avoids GET as a default. Research continues on remote activity-management and psychological supports; do not twist that into “exercise them harder.” [2] [3] [18] [2]
Mood and trauma pathways alter effort perception, sleep and school engagement. They are real mechanisms. They do not license you to skip anaemia, malignancy or cardiorespiratory disease. [12]
Clinical Presentation
Infants and young children rarely say “I am fatigued.” Parents report sleeping through feeds, weak cry, less play, colour change or “not interested in me.” That is lethargy language. Pair it with fever, vomiting, breathing difficulty or reduced wet nappies and your threshold for full assessment should be low. [8] [15]
School-age children may drop sport, fall asleep in class, or need naps that never used to happen. Teachers often notice first. Ask about snoring, mouth breathing, headaches on waking, abdominal pain, bruising and school attendance. [1] [6]
Adolescents present with grades slipping, training collapse, heavy periods, low mood, orthostatic light-headedness, or a post-viral stall after mononucleosis. Confidential history matters for mood, substances, disordered eating and menstrual blood loss. [5] [19]
Malignancy-related presentations are uncommon but high stakes. Clarke’s systematic review of childhood leukaemia presentations emphasises how often early features are non-specific — including fatigue and pallor — before classic textbook combinations assemble. Persistent bone pain, night sweats, unexplained fever, bleeding, lymphadenopathy or organomegaly raise urgency. [1]
Coeliac disease can present with extraintestinal fatigue, especially with more severe disease activity, not only with classic diarrhoea. [7] [20]
Medical complexity presents as a change from the child’s own baseline. A technology-dependent child who is “usually tired” can still have a new dangerous problem. Ask the expert caregiver what is different. [13]
Differential Diagnosis
Hold common and catastrophic lists together. [1] [15]
Must-not-miss now: sepsis and septic shock, meningitis or encephalitis, raised intracranial pressure, severe anaemia, myocarditis or heart failure, arrhythmia, adrenal crisis, hypoglycaemia, intoxication, non-accidental injury with head injury, and diabetic ketoacidosis presenting as tiredness plus dehydration. [14] [15]
Common reversible: inadequate sleep opportunity, iron deficiency, deconditioning after illness, mononucleosis convalescence, allergic rhinitis with poor sleep, and school overload. [4] [5] [6]
Important subacute: OSA, coeliac disease, thyroid disease, inflammatory bowel disease, chronic infection, renal disease, and evolving haematologic malignancy. [1] [6] [7]
Chronic multi-domain: ME/CFS after directed exclusion, post-COVID condition phenotypes, depression and anxiety with somatic fatigue, and trauma-related sleep disruption. These can coexist with biomedical disease. [2] [12] [16] [17]
Age shifts the ranking. Neonates and infants: infection, metabolic, cardiac, anaemia, non-accidental injury. School-age: sleep, iron, post-viral, coeliac, rare malignancy. Adolescents: sleep phase delay, menstrual iron loss, mono, mood, orthostatic symptoms, ME/CFS. [4] [5] [19]
Clinical & Bedside Assessment
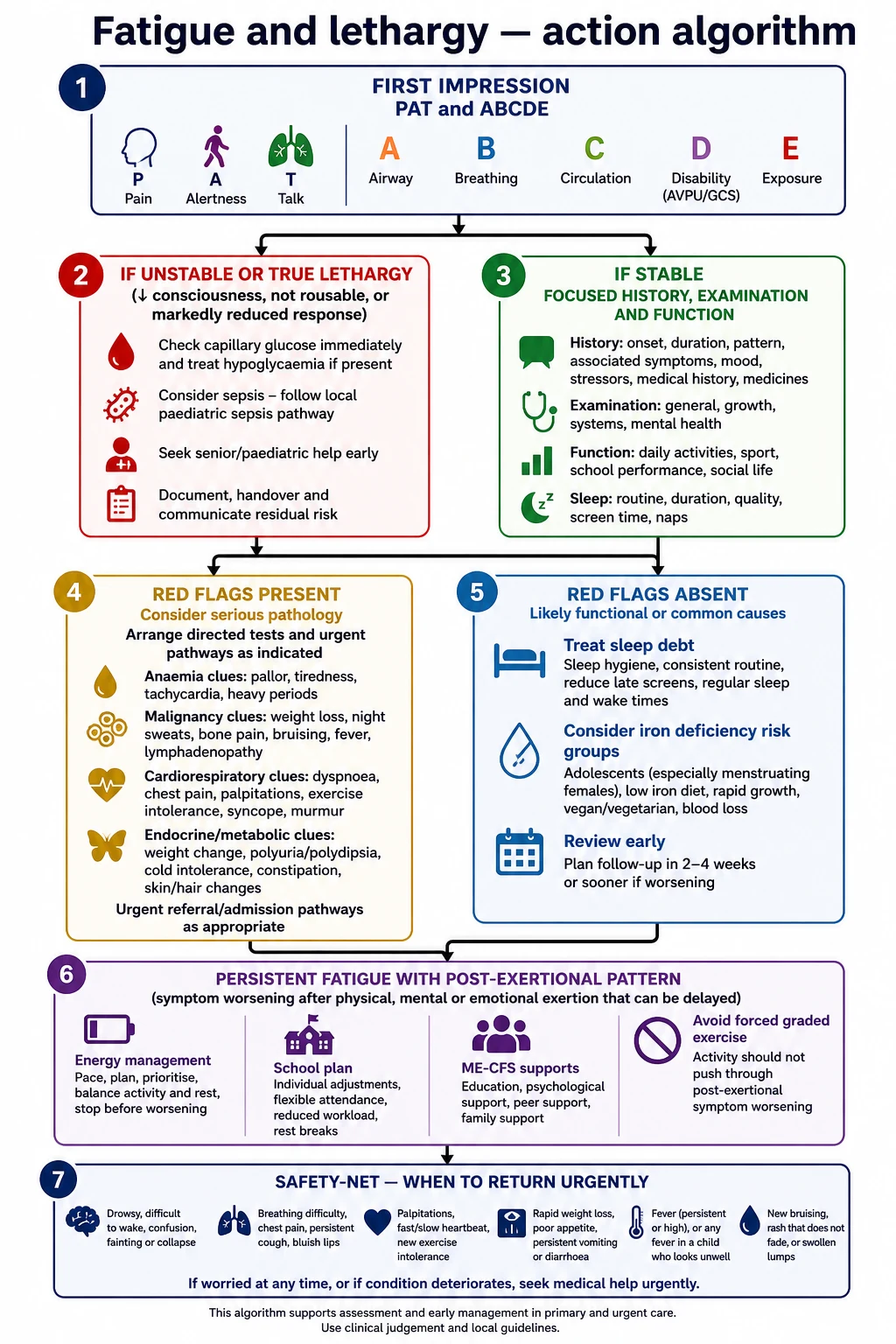
1. First impression before the story. Use a paediatric assessment triangle style glance: appearance and interaction, work of breathing, circulation to skin. A quiet, poorly interactive child is not “good because they are calm.” [8] [14]
2. ABCDE if any threat feature exists. Airway, breathing, circulation, disability including glucose, exposure. Start time-critical care while history continues in parallel. [15]
3. History that changes mechanism. Onset and tempo. Sleep timing and snoring. Fever, cough, sore throat, lymph nodes. Pallor, bleeding, bone pain. Polyuria, polydipsia, weight change. Headache, morning vomiting, visual change. Mood, bullying, trauma, school avoidance. Menstrual flow in adolescents. Medicines and complementary products. What the child can still do, and what triggers a crash. [1] [5] [6] [19]
4. Function score in plain language. School days missed, metres walked, stairs, sport, self-care, and whether exertion today causes a two-day collapse. This separates mild fatigue from severe ME/CFS phenotypes. [2] [3]
5. Examination with intent. Interaction and consciousness. Growth parameters. Pallor, petechiae, lymphadenopathy, organomegaly. Heart rate and respiratory rate against age norms. Work of breathing, heart sounds, perfusion. Thyroid, pubertal stage, neurological signs including fundi when indicated and skilled. Tonsillar size and nasal obstruction clues for OSA risk. [1] [6] [14]
6. Caregiver concern. Mills and colleagues showed caregiver concern for deterioration associates with critical illness in hospital-presenting children. Do not talk families out of a change you have not assessed. [8]
7. Communication access. Use a professional interpreter when language discordance exists. Fatigue histories are full of subtle functional detail that ad-hoc translation loses. [11]
Investigations
Tests should discriminate the active differential, not decorate the chart. [1] [4]
Often no same-day panel is needed when the story is clear sleep debt, examination is normal, red flags are absent, and early review is reliable. Fix sleep opportunity and safety-net. [6] [9]
Reasonable first-line tests for progressive, unexplained or red-flag fatigue include full blood count, iron studies when iron deficiency is plausible, electrolytes and glucose if unwell, coeliac serology in gluten-exposed children with compatible clues, thyroid function when indicated, inflammatory markers selectively, and urinalysis. Add monospot or EBV serology when the clinical picture fits older child or adolescent pharyngitis and fatigue patterns. [4] [5] [7]
ECG, chest radiograph, sleep study referral, imaging or oncology-directed tests follow hypothesis. Bone pain with cytopenias is not a “reassure and review” pattern. Exertional syncope or severe dyspnoea is not a lifestyle lecture. [1] [6]
Normal tests can lie early. Evolving leukaemia, early raised ICP and intermittent hypoglycaemia may not announce themselves on a single afternoon panel. Trajectory and red flags outrank one reassuring number. [1]
Avoid shotgun panels that create incidental findings and diagnostic momentum. Avoid removing gluten before coeliac testing if that pathway is live. [7] [20]
Management — Resuscitation
If the child is lethargic or unstable, stop debating chronic fatigue frameworks. [15]
Protect airway and breathing. Support oxygen delivery and circulation using local paediatric emergency protocols. Check and treat hypoglycaemia. Consider sepsis early when infection is possible and follow current paediatric sepsis guidance principles for recognition and escalation. Seek adrenal crisis clues in children on chronic steroids or with suggestive examination. [15]
Severe symptomatic anaemia needs urgent senior haematology-informed care rather than a delayed outpatient iron plan. Cardiorespiratory failure needs critical-care capable support. [4] [15]
Escalate beyond local capability early. Retrieval and PICU pathways exist for a reason. Hand over the problem representation, actions, response and residual risks with a structured tool. Handoff redesign work shows communication quality changes error rates. [10] [15]
Management — Definitive & Stepwise
Step 1 — Write the problem representation.
Example: “Fourteen-year-old with eight weeks of fatigue after mononucleosis, preserved interaction, snoring, heavy menses, falling grades, no bone pain or focal neurology — priority list sleep-disordered breathing, iron deficiency, prolonged post-viral fatigue; keep mood concurrent.” [5] [6] [19]
Step 2 — Treat reversible causes you have found.
Sleep opportunity coaching is concrete: fixed wake time, dark quiet sleep space, caffeine limits, and device curfew. Refer suspected OSA along local ENT/sleep pathways guided by AAP-aligned principles. Treat iron deficiency using current paediatric guidance and local dosing resources; state agent, elemental iron intent, duration and follow-up rather than vague “give iron.” Manage heavy menstrual bleeding with gynaecology or adolescent-health collaboration when needed. [4] [6] [19]
Step 3 — Infection-related fatigue.
Explain the expected convalescence after mononucleosis. Safety-net for breathing difficulty, dehydration, abdominal pain over the spleen region after trauma risk, and failure to improve on the expected timeline. [5]
Step 4 — Suspected ME/CFS or prolonged post-viral pattern.
After directed exclusion, name the pattern honestly. Emphasise energy management, rest after crashes, education access, and multidisciplinary support. Avoid GET as a default. BPSU work shows severe disease needs proactive medical and educational planning, not therapeutic nihilism. Remote activity-management and CBT research exists; frame psychological care as support for coping and function, not as proof the illness is “all in the mind.” [2] [3] [18] [2]
Step 5 — Mood and trauma care in parallel.
Screen and refer. Use trauma-informed posture. Do not make mental health the only story when red flags remain. [12]
Step 6 — School and family plan.
Agree attendance targets that do not punish crashes. Share a written plan with the school when families consent. Involve social work when transport, housing or caregiver capacity blocks recovery. [2] [3]
Step 7 — Review and safety-net.
Set a review date that matches risk. Tell families when to return today: reduced interaction, breathing difficulty, severe headache with vomiting, petechiae, ongoing vomiting, collapse, or a parent who feels the child is worse. Specific safety-netting improves care for acutely ill children. [8] [9]
Specific Subtypes & Scenarios
Febrile infant with progressive lethargy. Emergency assessment. Do not reframe as tiredness. Follow sepsis-capable pathways and local febrile-infant protocols. [15]
School-age snorer with daytime sleepiness. Think OSA. Examine airway, growth and blood pressure context; refer along sleep/ENT pathways. [6]
Adolescent heavy periods and declining sport. Think iron deficiency and anaemia. Take a menstrual history. Check bloods and treat with a complete plan, not a single tablet advice line without follow-up. [4] [19]
Post-EBV fatigue with post-exertional crashes. Support convalescence, watch for red flags, and if prolonged with ME/CFS features, shift to energy management and specialist supports. [5] [16]
Bone pain, pallor and fatigue. Malignancy pathway until proven otherwise. Urgent FBC and senior review. [1]
School refusal with fatigue and normal initial labs. Keep mood, sleep, bullying, orthostatic symptoms and rare organic disease concurrent. Trauma-informed enquiry. [12]
Technology-dependent child “more tired than usual.” Baseline-aware assessment for infection, device issues, anaemia, aspiration and caregiver-system strain. [13]
Refugee family, incomplete records. Interpreter, rebuild timeline, avoid racialised minimisation of symptoms. [11]
Severe housebound ME/CFS. Medical follow-up still required. Plan education, nutrition, orthostatic symptom support and home-based care access. Royston management data highlight service gaps you should not reproduce in your plan. [2] [3]
Complications & Pitfalls
- Calling a poorly interactive infant “tired” and sending them home. [8]
- Reassuring on “just a virus” despite malignancy or sepsis red flags. [1] [15]
- Missing iron deficiency in menstruating adolescents. [4] [19]
- Forcing graded exercise that worsens post-exertional exacerbation. [2] [2]
- Labelling ME/CFS before directed exclusion of treatable disease. [2] [4]
- Ignoring caregiver concern. [8]
- No interpreter for a subtle functional history. [11]
- Handover that drops residual risk and the school plan. [10]
- Diagnostic overshadowing in disability: attributing new lethargy to “the usual baseline.” [13]
Prognosis & Disposition
Many children recover when sleep debt, iron deficiency or convalescence is handled and school load is adjusted. Post-viral fatigue often improves over weeks, though a minority enter prolonged patterns. [5] [17]
Severe ME/CFS can persist and destroy education and social participation without active support. Early recognition of severity, home tuition planning and specialist input improve the chance of a humane trajectory even when recovery is slow. [2] [3]
Disposition is capability-matched. Unstable lethargy needs ED/ward/PICU pathways. Stable mild fatigue can leave with a written plan and early review. Unresolved red flags do not belong on a distant routine waitlist. [9] [15]
Special Populations
Neonates and infants: lethargy is emergency language. Pair with feeding, temperature and colour. [15]
Adolescents: confidential history for mood, substances, disordered eating, menstrual loss and orthostatic symptoms. [19]
Medical complexity: ask for baseline comparison; involve the usual team early. [13]
Disability and neurodiversity: distinguish new reduced interaction from baseline communication style. [13]
Indigenous families: culturally safe care without minimising symptoms or racialising “stoicism.” [12]
Migrant and refugee families: interpreters, interrupted records, infection and nutrition dual risk. [11]
Out-of-home care and trauma-exposed children: trauma-informed assessment; fatigue may reflect sleep threat, depression or unrecognised medical disease. [12]
Evidence, Guidelines & Regional Differences
Clarke’s meta-analysis remains the high-yield reminder that childhood leukaemia often starts with non-specific symptoms including fatigue and pallor. [1]
Royston’s BPSU studies quantify how severe paediatric ME/CFS presents and how uneven management can be in real services. [2] [3]
Powers’ AAP clinical report frames iron deficiency prevention, diagnosis and treatment across paediatric ages; the adolescent heavy-menstrual-bleeding paper targets a classic exam trap. [4] [19]
Marcus AAP guidance anchors childhood OSA recognition and management principles for daytime sleepiness pathways. [6]
Leung’s mononucleosis review supports counselling on prolonged fatigue after EBV. [5]
Nurminen and Laurikka support extraintestinal coeliac presentations, including fatigue-related burden. [7] [20]
Mills, Burvenich and Starmer supply the safety triad: caregiver concern, safety-netting, and structured handover. [8] [9] [10]
NICE NG206 is the key UK operational language for ME/CFS diagnosis and energy management. Do not quote outdated GET-as-default teaching as if it were current UK standard. [2]
Use local acute assessment pathways for lethargy and sepsis concern. Iron and sleep referrals run through primary care, paediatrics, ENT and adolescent services. Pair chronic fatigue care with school liaison and culturally safe family support. [4] [8] [8]
NICE NG206 shapes ME/CFS language: energy management, careful diagnosis, and avoidance of GET as default. BPSU evidence is fair game in exams for severe disease service gaps. [2] [3] [2]
AAP iron-deficiency and OSA documents are high-yield. ME/CFS care should still avoid punitive exercise prescriptions and should address school function explicitly. [4] [6]
Align anaemia, sleep and chronic-fatigue supports with provincial primary-care and paediatric pathways; keep threat-first assessment universal. [4] [15]
Exam Pearls
- Interaction first: fatigue versus lethargy changes the whole encounter. [8]
- Infants do not “look tired” — they look lethargic or they do not. [15]
- Malignancy can start vague; bone pain plus cytopenia is not vague. [1]
- Iron deficiency and sleep debt are common; missing them is embarrassing, missing sepsis is lethal. [4] [6]
- Post-exertional crashes argue against forced exercise programmes. [2] [2]
- Caregiver concern is data. [8]
- Safety-net with specific return criteria. [9]
- Hand over residual risk, not only today’s label. [10]
- Use interpreters for functional histories. [11]
- Baseline-aware assessment in medical complexity. [13]
High-yield anchors
References
- [1]Clarke RT Clinical presentation of childhood leukaemia: a systematic review and meta-analysis. Archives of disease in childhood, 2016.PMID 27647842
- [2]Royston AP Severe myalgic encephalomyelitis/chronic fatigue syndrome in children and young people: a British Paediatric Surveillance Unit study. Archives of disease in childhood, 2023.PMID 36456114
- [3]Royston AP Management of severe ME/CFS in children and young people in the UK: a British Paediatric Surveillance Unit study. BMJ paediatrics open, 2024.PMID 38453418
- [4]Powers JM Prevention, Screening, Diagnosis, and Treatment of Iron Deficiency and Iron Deficiency Anemia in Infants, Children, and Adolescents: Clinical Report. Pediatrics, 2026.PMID 42324084
- [5]Leung AKC Infectious Mononucleosis: An Updated Review. Current pediatric reviews, 2024.PMID 37526456
- [6]Marcus CL Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics, 2012.PMID 22926173
- [7]Nurminen S Extraintestinal manifestations were common in children with coeliac disease and were more prevalent in patients with more severe clinical and histological presentation. Acta paediatrica, 2019.PMID 29569302
- [8]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [9]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice, 2025.PMID 39117428
- [10]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [11]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [12]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [13]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [14]Fleming S Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [15]Weiss SL Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatric critical care medicine, 2026.PMID 41869844
- [16]Jason LA Predisposing and Precipitating Factors in Epstein-Barr Virus-Caused Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Microorganisms, 2025.PMID 40284540
- [17]Nugawela MD Predicting post-COVID-19 condition in children and young people up to 24 months after a positive SARS-CoV-2 PCR-test: the CLoCk study. BMC medicine, 2024.PMID 39511637
- [18]Crawley E Comparison of cognitive behaviour therapy versus activity management, both delivered remotely, to treat paediatric chronic fatigue syndrome/myalgic encephalomyelitis (MAGENTA). Health technology assessment, 2024.PMID 39485730
- [19]Powers JM Hematologic Considerations and Management of Adolescent Girls with Heavy Menstrual Bleeding and Anemia in US Children's Hospitals. Journal of pediatric and adolescent gynecology, 2018.PMID 29940313
- [20]Laurikka P Extraintestinal Manifestations of Celiac Disease: Early Detection for Better Long-Term Outcomes. Nutrients, 2018.PMID 30081502