Paeds · clinical-assessment-and-reasoning
Growth measurement, charting and interpretation
Also known as Growth charts · WHO CDC growth · Paediatric anthropometry
Fellowship guide to paediatric growth measurement, chart selection, plotting, interpretation and first actions for faltering or excess growth.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Name the chart before you argue a cut-off. [1]
P.L.O.T.
Overview & Definition
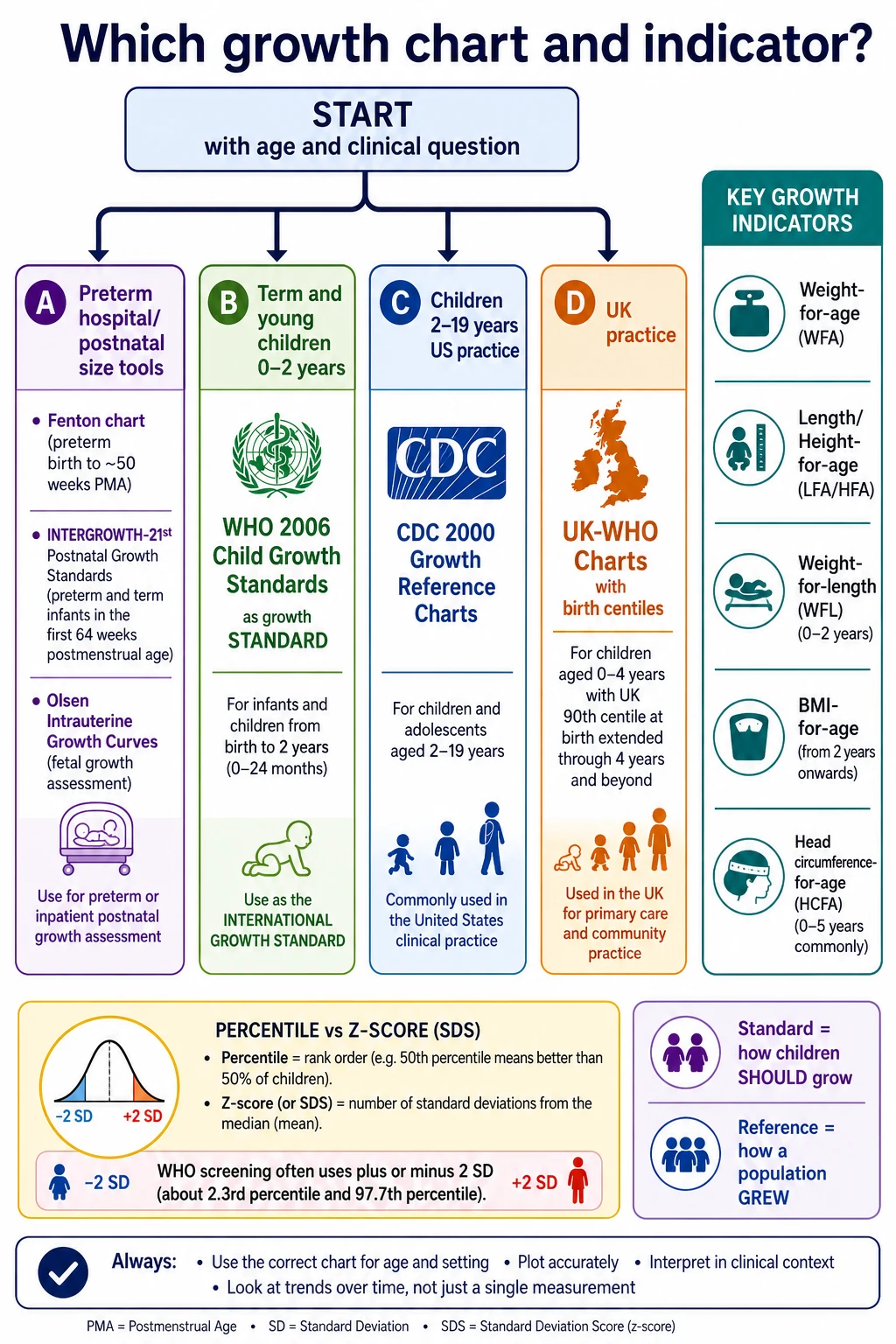
Growth charts turn measurements into a visual story. Fellowship candidates must measure accurately, choose WHO versus CDC versus preterm specialty charts correctly, and know when a crossing percentile is physiology, error or disease. [1]
Classification
Indicators: weight-for-age, length/height-for-age, weight-for-length, BMI-for-age, head circumference-for-age, and velocity. Percentiles versus z-scores matter at extremes. Preterm infants need corrected age and often specialty charts early. [1]
Epidemiology & Risk Factors
Poverty, food insecurity, chronic disease, untreated coeliac disease, congenital heart disease, genetic syndromes and neglect all change growth risk. Medical complexity needs baseline trajectories, not generic targets alone. [3] [8]
Pathophysiology
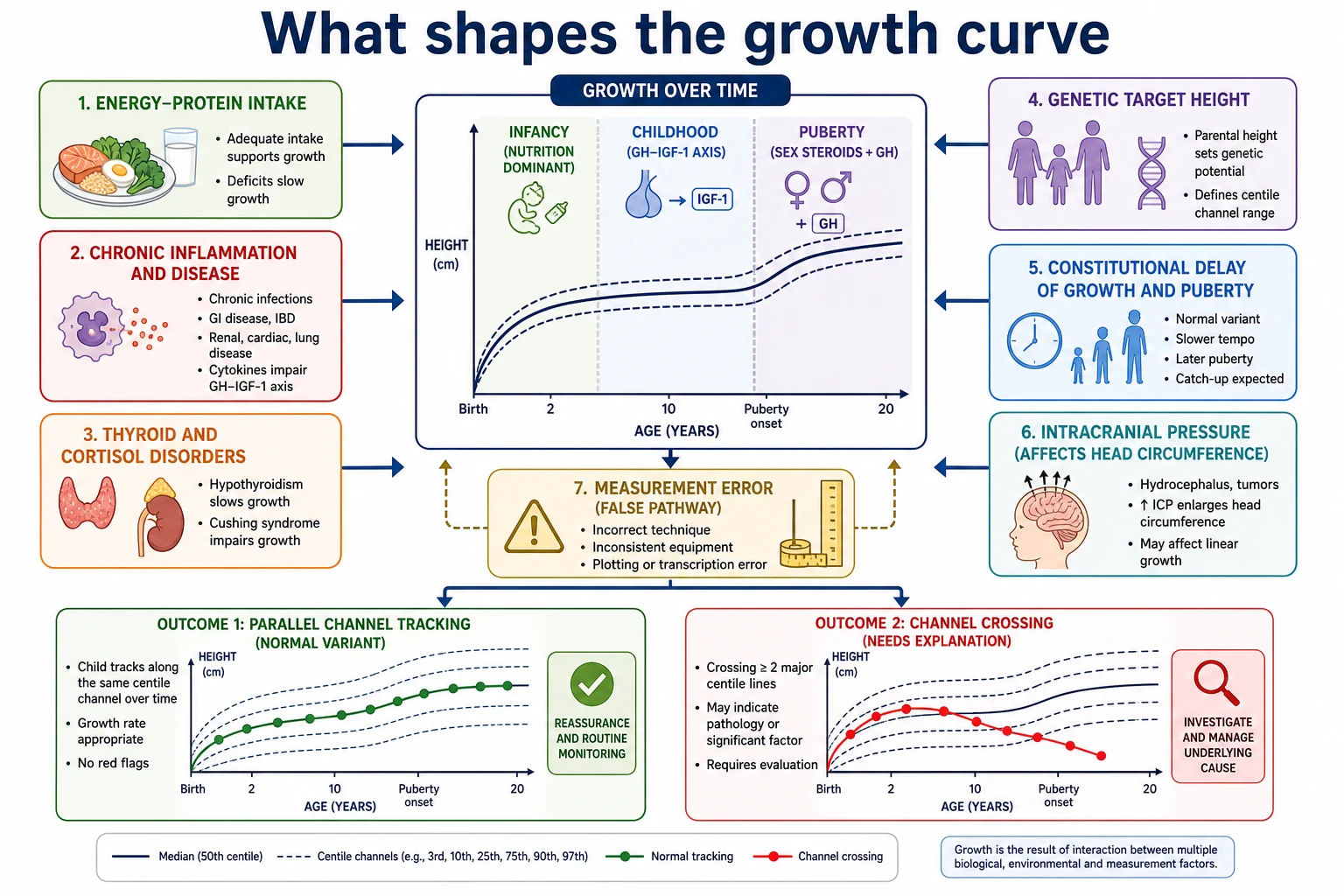
Linear growth reflects skeletal growth plates and hormonal axes; weight reflects energy balance and illness; head growth reflects brain growth in early life. Acute illness drops weight first; chronic disease and endocrine problems more often slow length/height. [1]
Clinical Presentation
Faltering growth may present as clothes staying large, crossing down centiles, or caregiver concern that the child is “tiny.” Excess weight may be silent until BMI plotting. Microcephaly or crossing head centiles needs early thought about brain growth and measurement error. [1] [4]
Differential Diagnosis
Measurement error versus true faltering. Familial short stature versus constitutional delay versus endocrine disease versus chronic illness versus neglect. Isolated heavy weight versus tall stature syndromes. Always ask: is the chart wrong, the measure wrong, or the child unwell? [1] [8]
Clinical & Bedside Assessment
Infants: supine length with two people; naked or dry nappy weight; OFC widest path. Older children: standing height, heels/buttocks/shoulders positioned. Plot immediately. Compare with mid-parental expectation qualitatively without inventing uncited formulas in the viva if unsure. [1]
Investigations
Directed by history and severity: coeliac screen, TFTs, urine, diet history, and specialist tests when indicated — not a fixed mega-panel for every low centile. [1]
Management — Resuscitation
Severe malnutrition with instability is an acute care problem first. Safeguarding pathways run in parallel when neglect is possible. [8]
Management — Definitive & Stepwise
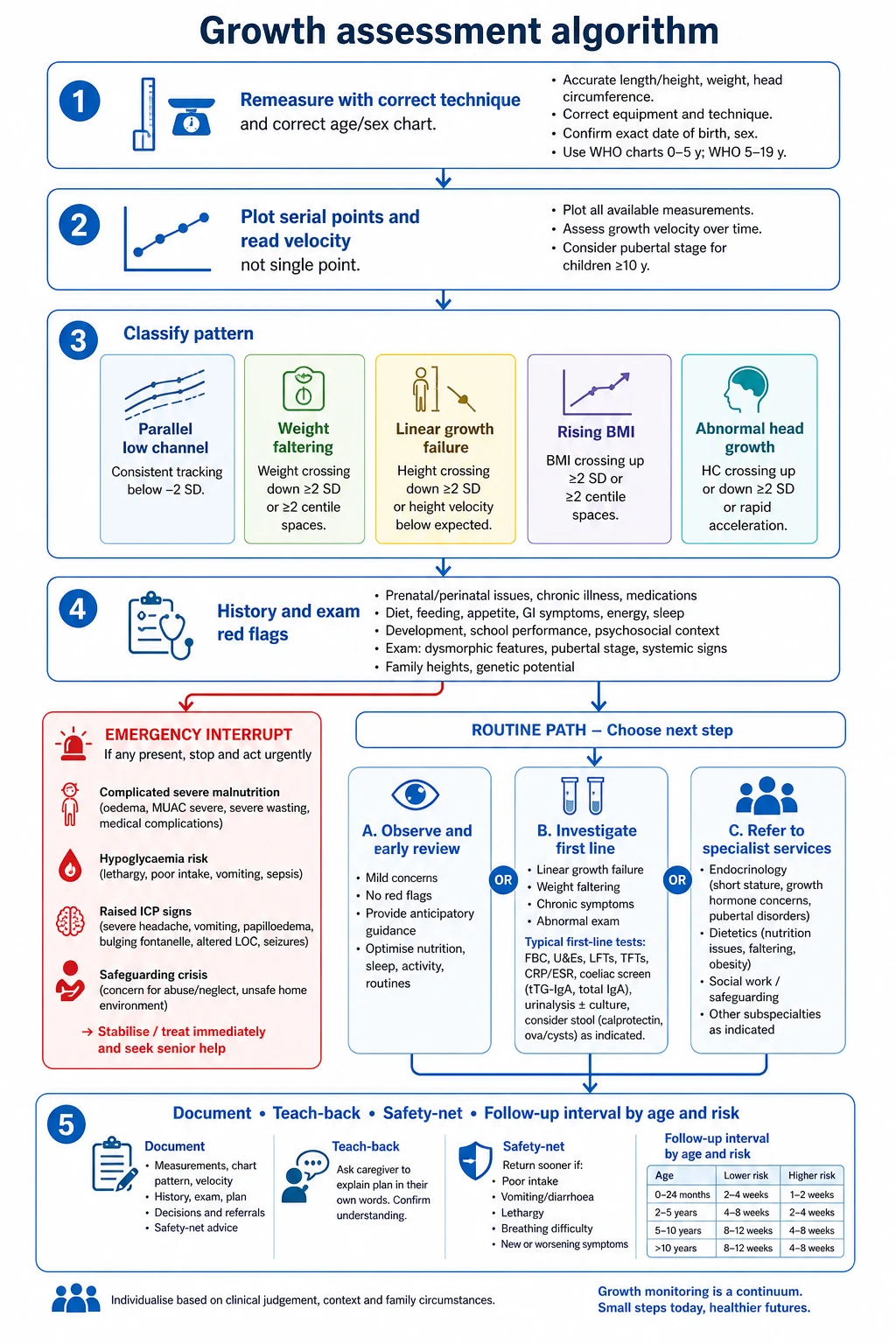
- Confirm measurements.
- Correct chart and age (including prematurity correction rules you are using).
- Interpret trend.
- Act on faltering or obesity pathways with local services.
- Explain the plot with teach-back; safety-net review timing. [1] [9]
Specific Subtypes & Scenarios
Ex-preterm. Correct age early; transition to chronological plotting per local protocol. [1]
Medical complexity. Individualised expectations and equipment (wheelchair scales). [3]
Language discordance. Interpreter for diet and chart explanation. [5]
Possible neglect. Careful documentation and safeguarding. [8]
Complications & Pitfalls
Clothes-on weights. Wrong age plotted. CDC vs WHO confusion. Calling a single low reading “FTT” without trend. Shaming families about BMI. [1]
Prognosis & Disposition
Early correction of energy intake and disease treatment can restore velocity; delayed recognition loses height potential. Disposition includes dietetic follow-up and clear review dates. [1] [9]
Special Populations
Syndromic growth charts when validated for that condition; otherwise plot on standard charts and annotate. Adolescents need sensitive BMI discussion. [1]
Evidence, Guidelines & Regional Differences
CDC 2000 methods paper documents US reference charts. [1] WHO standards are operationalised via official WHO tools (official source). Pair growth concern with developmental surveillance when delay coexists. [10]
Exam Pearls
- Technique before interpretation. [1]
- Name the chart. [1]
- Trend over single points. [1]
- Complexity changes targets. [3]
- Concern is data. [4]
References
- [1]Kuczmarski RJ 2000 CDC Growth Charts for the United States: methods and development. Vital and health statistics. Series 11, Data from the National Health Survey, 2002.PMID 12043359
- [2]Fleming S Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [3]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [4]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [5]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [6]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [7]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [8]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [9]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [10]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861