Paeds · clinical-assessment-and-reasoning
Illness severity, deterioration and track-and-trigger systems
Also known as PEWS · Paediatric early warning system · Track and trigger · Paediatric MET · Rapid response system · Failure to rescue · BedsidePEWS · Clinical deterioration
Fellowship approach to illness severity versus risk of deterioration, paediatric track-and-trigger tools and PEWS architecture, rapid-response systems, EPOCH and systematic-review evidence, caregiver concern, incomplete charts, escalation culture and safe disposition across age bands.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child on the ward can look “a bit off” long before cardiac arrest. Illness severity is how heavy the disease burden feels now. Physiological instability is whether breathing, circulation or consciousness is failing this minute. Risk of deterioration is what may happen in the next hour if nothing changes. Diagnostic seriousness is the harm of a possible diagnosis even when physiology still looks preserved. Failure-to-rescue is the system failure when that trajectory was visible and the team did not act in time. [4] [12]
The doorway first impression — Appearance, Work of Breathing and Circulation to Skin — belongs primarily to the linked Paediatric Assessment Triangle topic. This page owns what happens next on the chart: track-and-trigger design, PEWS performance, MET/RRT response, incomplete documentation, escalation culture and disposition. [1] [2]
A track-and-trigger tool records observations over time (“track”) and defines when a response must start (“trigger”). A paediatric early warning score is one kind of multi-parameter tool. A paediatric early warning system is larger than the score: documentation design, escalation recommendations, education, family activation and governance all sit around the number. [4] [6] [15]
State a problem representation the way you would on the phone to the MET: age and baseline, current score and trajectory, which observations are missing, what the caregiver is worried about, what you have already done, and what response you need now. [1] [2]
Classification
Track-and-trigger tools fall into three practical families. A single-parameter trigger fires when any one vital sign crosses a critical threshold. A multi-parameter scoring tool adds several age-banded items into a total score. A hybrid system combines score bands with single extreme triggers so one catastrophic value still forces action even if the total looks modest. [4] [5]
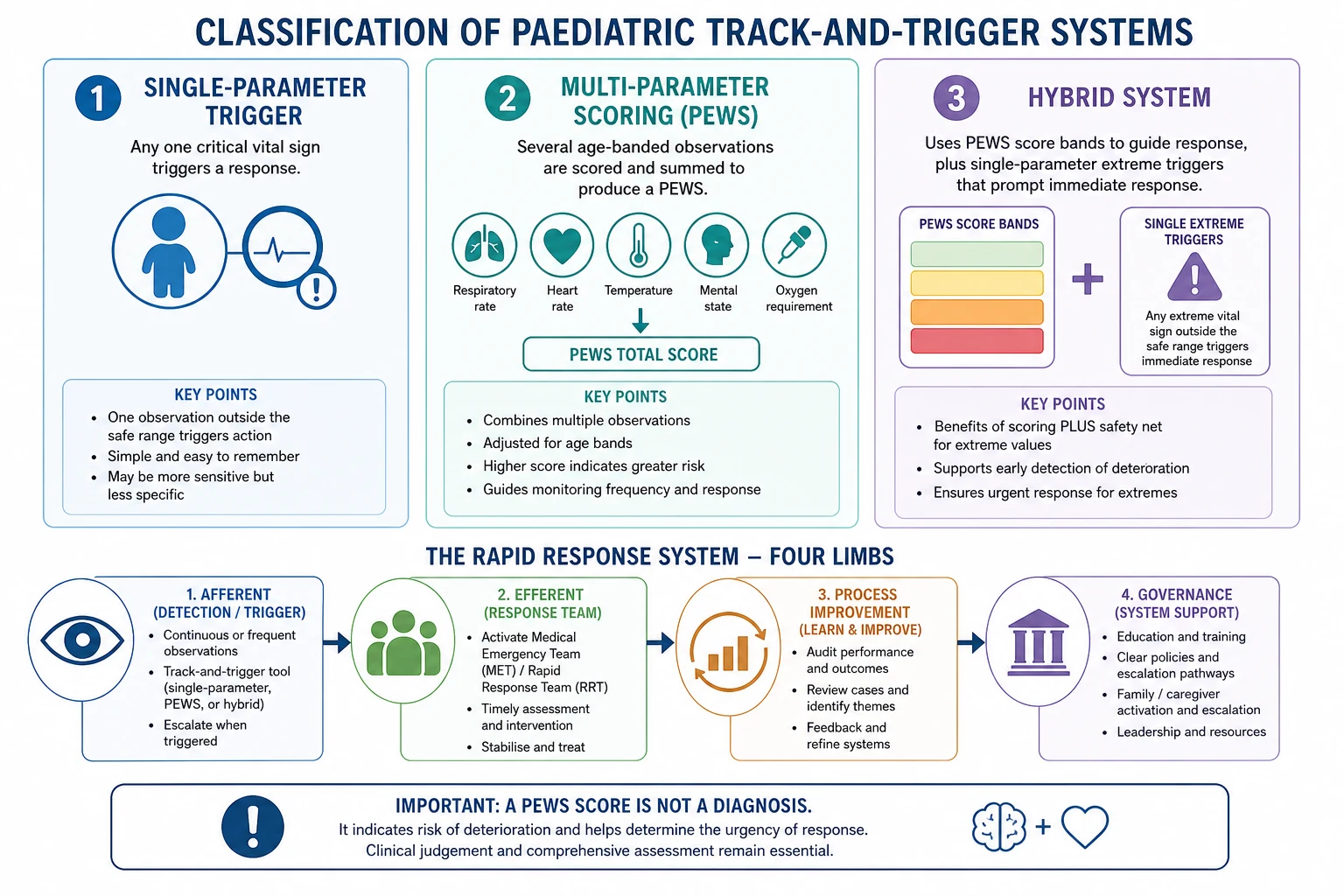
BedsidePEWS is the seven-item multi-parameter score developed and validated by Parshuram and colleagues. The seven items are heart rate, systolic blood pressure, capillary refill time, respiratory rate, respiratory effort, transcutaneous oxygen saturation and oxygen therapy. The total ranges from 0 to 26. Age-band cut-offs for each item are chart-specific; do not invent them from memory. In multicentre validation, the median maximum score in the 12 hours ending 1 hour before a clinical deterioration event was 8 (IQR 5–12) in cases versus 2 (IQR 1–4) in controls, with AUCROC 0.87 (95% CI 0.85–0.89). [1] [2]
Compare the tool with the team that answers it: [1] [2]
Track-and-trigger tool
The chart and score
- Age-banded observations
- Single-parameter, multi-parameter or hybrid design
- Documents trajectory
- Never replaces clinical judgement
Early-warning system
The whole programme
- Education and simulation
- Escalation recommendations
- Family activation
- Audit of underscoring and response times
Rapid-response system
Hospital safety architecture
- Afferent limb: detect and call
- Efferent limb: MET/RRT/code team
- Process improvement
- Governance and resources
A medical emergency team (MET) or rapid response team (RRT) is the efferent limb that arrives when criteria are met. Code blue is reserved for cardiac or respiratory arrest or peri-arrest. Family-activated escalation lets caregivers bypass hierarchy when they believe the child is getting worse. None of these replace the observation chart; they complete it. [10] [11] [13]
Epidemiology & Risk Factors
Ward cardiac arrest and unexpected death are rare in modern paediatric hospitals. That is why they are poor sole quality metrics. Critical deterioration — unplanned ICU transfer with need for ventilation or vasoactive support soon after transfer — is a more useful proximate outcome. In one interrupted time-series study, rapid-response system implementation was associated with a 62% net decrease in critical deterioration relative to the pre-intervention trend (adjusted incidence rate ratio 0.38, 95% CI 0.20–0.75), while absolute reductions in ward cardiac arrest and death were not statistically significant because baseline rates were already tiny. [12]
Risk rises with younger age, complex chronic disease, technology dependence, recent surgery, recent ICU step-down, incomplete vital-sign sets, night-time observation gaps and high patient-to-nurse ratios. Language barriers and low health literacy delay recognition of caregiver concern. Predictive performance of published PEWS instruments varies widely; Chapman and colleagues found AUROC ranging such that three of 18 systems reached 0.87 or higher, while trigger-only systems occupied the six lowest ranks. Choice of tool is therefore clinically meaningful. [5] [16]
Pathophysiology
Children compensate hard and then fall off a cliff. Tachycardia and increased work of breathing buy time while stroke volume and gas exchange are still salvageable. Blood pressure often stays normal until late circulatory failure. A falling respiratory rate or a quieter, less interactive child after a period of high effort often means exhaustion, not recovery. Hypoxia, hypercapnia, hypoglycaemia, raised intracranial pressure, toxins and systemic inflammation can all blunt consciousness. [7]
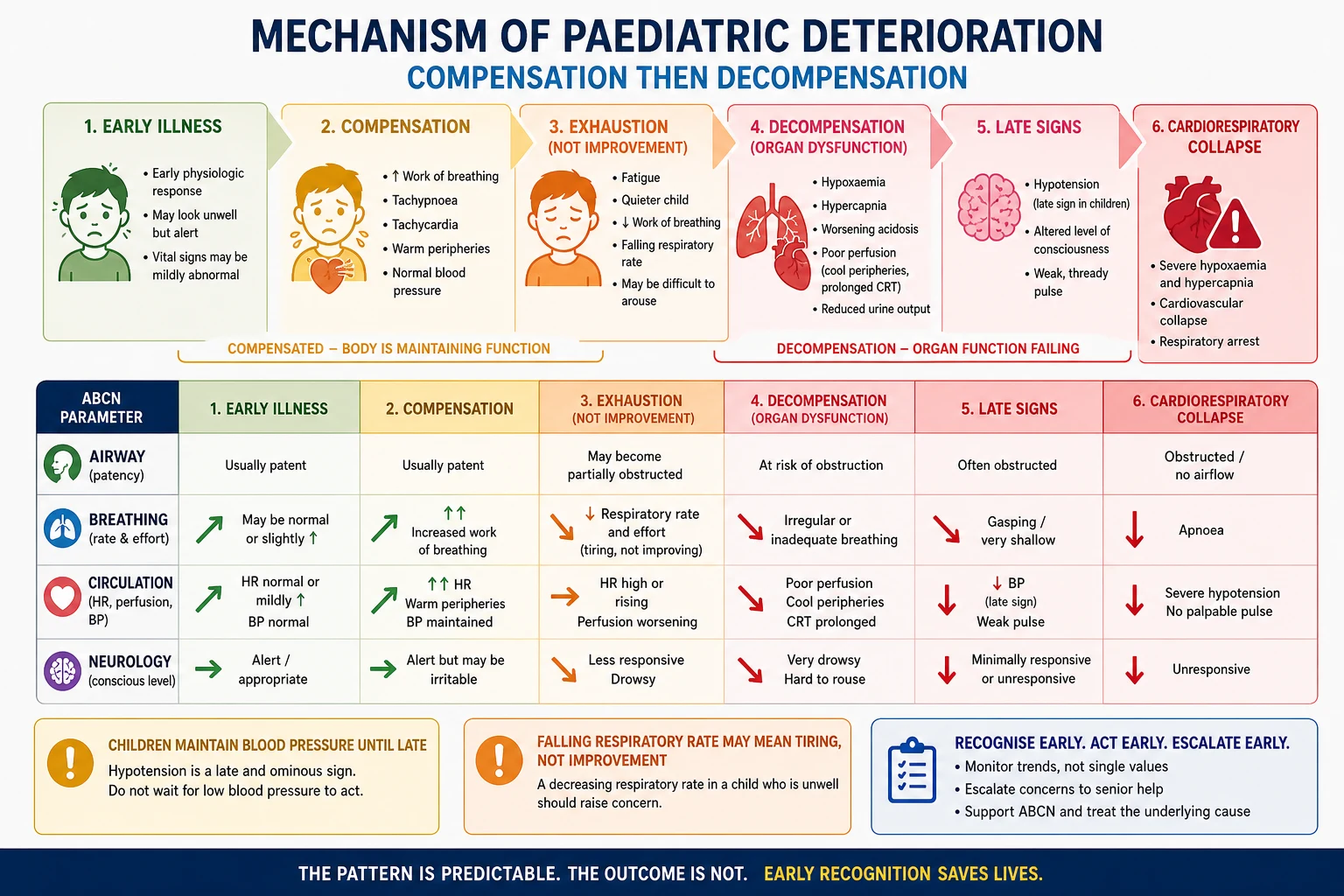
Heart rate and respiratory rate normal ranges change steeply with age; adult thresholds misclassify infants. Fever raises expected heart rate in hospitalised children, so temperature must be read with the pulse rather than used as an excuse to ignore tachycardia. Chronic baselines — cyanotic heart disease, home oxygen, neuromuscular weakness — shift what “normal for this child” means. Response to oxygen, fluid or bronchodilator is a trend, not proof of diagnosis. [7] [8] [16]
Clinical Presentation
Ward deterioration usually declares itself as a pattern, not a single red number. Respiratory rate climbs, effort increases, oxygen requirement creeps up, heart rate stays high after fever settles, urine output falls, and interaction drops. Caregivers often report “they are not themselves” before the score fully rises. In a prospective Australian cohort, documented caregiver concern for deterioration was associated with ICU admission (adjusted odds ratio 1.72, 95% CI 1.40–2.11) and mechanical ventilation (aOR 1.85, 95% CI 1.36–3.15) after adjustment including abnormal vital signs; concern was more strongly associated with ICU admission than any single abnormal vital sign in that analysis. [9]
Neonates and young infants may show only poor feeding, colour change, temperature instability or reduced tone. School-age children can localise symptoms; adolescents may minimise or conceal substance use and self-harm risk that alter observations. Immunocompromised and technology-dependent children may present with attenuated classical signs or with device alarms that are either true physiology or equipment failure. Incomplete, underscored or overscored charts are themselves clinical findings: treat the child and fix the documentation. [16]
Differential Diagnosis
When a trigger fires, sort causes by immediate threat, not by which specialty owns the ward: [1] [2]
- Airway and breathing: upper-airway obstruction, pneumonia, bronchiolitis, asthma, aspiration, pneumothorax, fatigue. [1] [2]
- Circulation: hypovolaemic, distributive, cardiogenic or obstructive shock; arrhythmia; bleeding; anaphylaxis. [1] [2]
- Neurology: seizure, raised intracranial pressure, encephalopathy, intoxication. [1] [2]
- Metabolic: hypoglycaemia, electrolyte crisis, adrenal crisis, diabetic ketoacidosis. [1] [2]
- Device and environment: blocked tracheostomy, disconnected oxygen, failed pump, pain, fever, anxiety, measurement error. [1] [2]
Congenital heart disease can mimic primary respiratory disease on a chart. Pain and fever can raise scores without implying sepsis — but never use them as a blanket explanation. Dangerous diagnoses can still sit under a currently low score: evolving meningococcal disease, button-battery ingestion, non-accidental injury, or a child whose observations have simply not been completed. [9] [21] [25]
Clinical & Bedside Assessment
Measure age-banded vital signs carefully. Count respiratory rate over a full window when the child is as calm as possible. Use an appropriately sized blood-pressure cuff. Document oxygen delivery with SpO2. Capillary refill has diagnostic value for serious illness when measured carefully, but technique variation is large. Pulse oximetry can under-read or over-read depending on skin pigmentation and device; interpret SpO2 with the whole picture. Consciousness tools such as AVPU remain useful for rapid screening alongside fuller scales when needed. [7] [20] [21] [22] [23]
A valid multi-parameter score needs the items the chart requires. If items are missing, say so out loud, complete them if safe, and escalate on clinical concern rather than waiting for a perfect total. Establish baseline for complex chronic disease: usual SpO2, home oxygen flow, baseline heart-rate range, seizure threshold, feeding route and emergency care plan. Ask the caregiver the exact question used in the Mills study language: are you worried your child is getting worse? [2] [9] [16]
Reassess after every intervention. Record the intended effect, the actual response and the new score. Common technique errors — counting a crying infant’s respiratory rate as “normal,” using the wrong age band, ignoring oxygen therapy in the score, or documenting a single post-nebuliser SpO2 as reassurance — convert a good chart into a false story. [1] [2]
Investigations
Bedside tests that change immediate care come first: glucose, blood gas when available, lactate when shock is possible, point-of-care electrolytes, and rapid identification of device failure. Cultures and imaging follow once airway, breathing and circulation are addressed. A normal blood gas does not cancel a rising multi-parameter score or caregiver concern. Indiscriminate panels, trips to radiology without a resuscitation-capable escort, and false reassurance from one normal test all cause harm. PEWS performance metrics such as AUROC must be quoted from verified sources only; incomplete documentation invalidates retrospective score research as well as bedside care. [2] [5]
Management — Resuscitation
When a PEWS or single-parameter trigger fires — or when concern is high despite a low score — go to the bedside. Call for help early. Name a leader. Allocate roles. Start age-adapted ABCDE while the chart trajectory is reviewed. Check immediately reversible threats: airway patency, oxygen delivery and device connections, severe work of breathing or fatigue, shock, seizure, hypoglycaemia, anaphylaxis, bleeding and tension physiology. Use closed-loop communication. Escalate from increased observation frequency to senior review to MET/RRT attendance to code-blue activation according to local criteria and the child’s trajectory, not according to pride. [10] [11] [13]
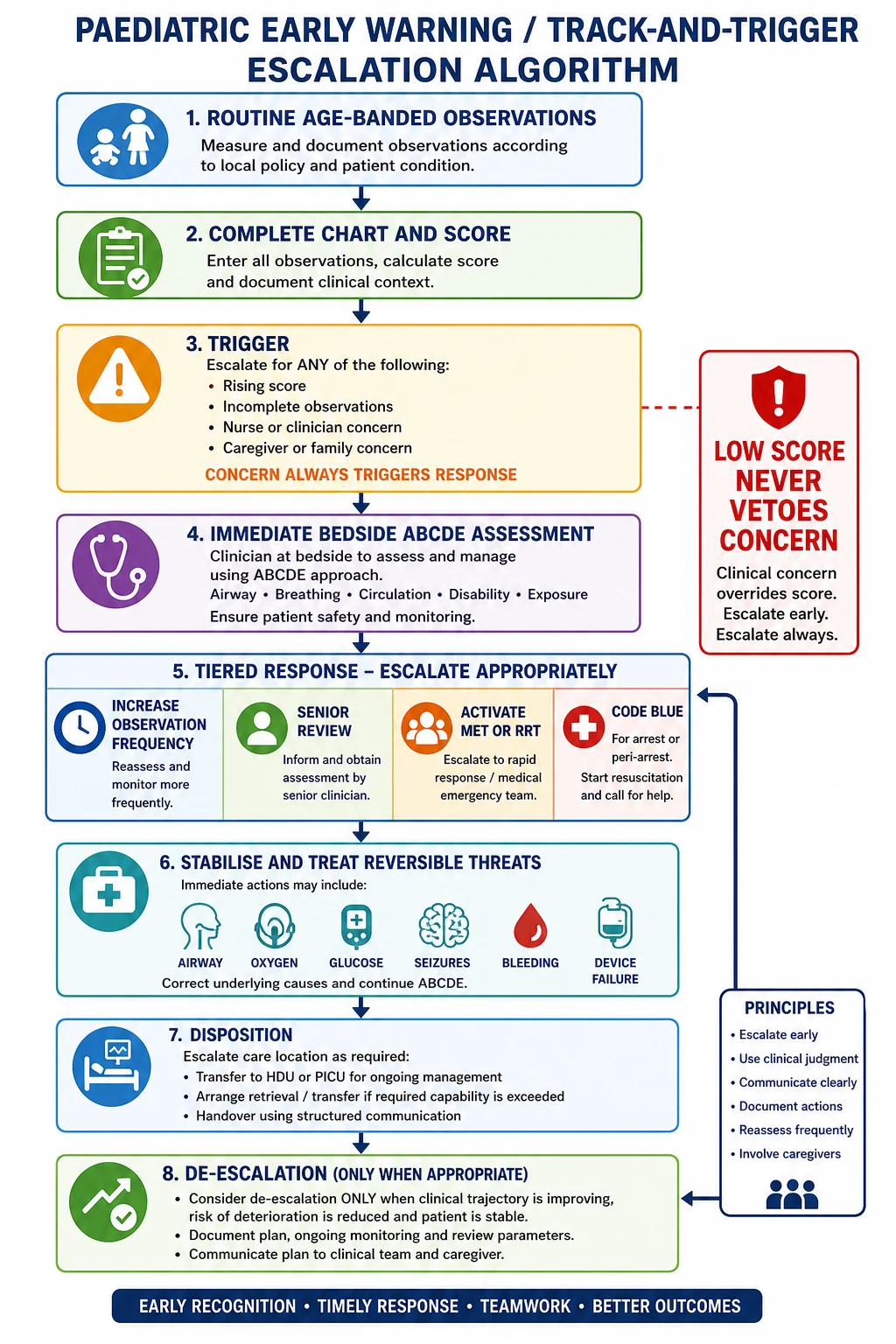
Hand over with a structured format (ISBAR or equivalent): identity and baseline, current score and missing items, situation and trajectory, background diagnoses and devices, assessment of threat category, and recommendation for the response you need. Structured handoff programmes reduce medical errors and preventable adverse events in paediatric settings. [17]
Management — Definitive & Stepwise
Design the hospital system, not only the chart. The consensus architecture of a rapid-response system has four elements: an afferent crisis-detection and response-triggering mechanism; an efferent predetermined team; governance and resources; and a process-improvement loop that studies antecedents of crises. Score-matched escalation recommendations guide frequency of review, but nurse and clinician discretion and caregiver concern must still be able to upgrade the response. [13]
Family-activated rapid response empowers parents to escalate when they believe staff have not recognised deterioration. Electronic PEWS can reduce arithmetic error but can also hide incomplete fields if the interface allows underscoring. Education, simulation and audit sustain performance; the PUMA programme showed that context-specific system improvement can shift adverse-event trends, with one organisationally supported site showing a significant decline. De-escalate observation frequency only when the trajectory is improving, the plan is documented, and the child and caregivers understand the safety net. [9] [14] [15]
Rural and interhospital transfer decisions turn on capability, not on defending a local bed. Prepare airway equipment, monitoring, documentation of trend and timed treatments, and a receiving team brief before the journey. Transport quality affects outcome; do not improvise an unstable transfer. [19]
Specific Subtypes & Scenarios
Overnight rising multi-parameter score with incomplete observations. Complete the missing items if safe, treat what you find, and escalate rather than waiting for the morning ward round. [1] [2]
Young infant with non-specific behavioural change. Borderline scores plus poor feeding or reduced interaction still warrant senior review because reserve is small. [1] [2]
Cyanotic heart disease or home oxygen. Score against the child’s baseline SpO2 and heart-rate physiology, not against a pink-child chart. [1] [2]
Technology-dependent child. Separate device failure from true physiological deterioration; both can kill, and both need immediate action. [16]
Post-operative or post-ICU step-down. Pre-test risk is higher; a “soft” trigger deserves a harder look. [1] [2]
Emergency department versus inpatient PEWS. ED tools often prioritise triage and disposition; inpatient PEWS prioritises trajectory on the ward. Do not assume one chart’s bands apply to the other setting without local policy. [4]
Caregiver concern with a low numerical score. Escalate. Document the concern. Reassess fully. The Mills data support treating concern as an independent signal. [9]
Adolescent intoxication or self-harm risk. Privacy, pregnancy possibility and safeguarding alter both assessment and observation planning. [1] [2]
Possible safeguarding presentation. Illness and injury can coexist; do not label every abnormal finding as medical deterioration alone. [25]
Complications & Pitfalls
Other traps: score fixation that replaces judgement; alarm fatigue from oversensitive systems; hierarchy that blocks MET calls; blaming all abnormal observations on fever, pain or anxiety; applying adult norms or the wrong age band; ignoring caregiver or nurse concern; handover failures at shift change and ICU transfer; and missed safeguarding when every bruise is explained as “sepsis-related”. [7] [17] [25]
Prognosis & Disposition
Disposition follows trajectory and response more than any single number. Critical deterioration as a proximate outcome tracks risk better than rare cardiac arrest. Increased ward observation can be safe when the child is improving, help is immediately available and the diagnosis is clear. Transfer to HDU/ICU or retrieval is mandatory when support needs exceed local capability, when compensation is failing, or when recurrent triggers remain unexplained. After a resolved trigger, safety-net advice must name specific return features and who to call. Recurrent triggers without diagnosis force deeper work-up and a safeguarding lens. [12] [24]
Special Populations
Neonates and ex-preterm infants have different vital-sign baselines and non-specific early signs. Children with medical complexity need personalised baselines and emergency care plans. Immunocompromised children may lack fever or inflammatory signs until late. Disability and communication difference shift behavioural cues; use the people who know the child best. Indigenous, migrant and refugee families need culturally safe care and professional interpreters; ad-hoc bilingual relatives are not an equivalent safety system. Out-of-home care and youth justice settings complicate consent and history access. Adolescents approaching transition may move onto adult early-warning tools; the emergency plan and technology baseline must travel with them. [16] [18]
Evidence, Guidelines & Regional Differences
EPOCH (cluster RCT, 21 hospitals, 144,539 discharges). BedsidePEWS versus usual care without a severity-of-illness score did not reduce all-cause hospital mortality (1.93 vs 1.56 per 1000 discharges; adjusted OR 1.01, 95% CI 0.61–1.69; P = 0.96). Significant clinical deterioration events were lower with BedsidePEWS (0.50 vs 0.84 per 1000 patient-days; adjusted rate ratio 0.77, 95% CI 0.61–0.97; P = 0.03). Quote both findings; do not claim a mortality benefit that the trial did not show. [3]
Trubey and Lambert systematic reviews. PEWS tools can show predictive validity for deterioration, but evidence that implementing a system reduces hard outcomes is mixed and methodologically heterogeneous. Validity is not the same as effectiveness. [4] [6]
Chapman. Predictive performance of 18 paediatric track-and-trigger systems varies widely; scoring systems generally outperformed pure trigger systems in that comparison. [5]
Tibballs MET before–after studies. Introduction of a paediatric MET was associated with reductions in hospital mortality and preventable cardiac arrest/death in a single centre; design limitations of before–after studies apply. [10] [11]
Bonafide. Critical deterioration is a more sensitive proximate metric than rare ward arrest. [12]
Mills 2025. Caregiver concern associates with critical illness after adjustment for vital signs. [9]
PUMA. Systems approaches that improve documentation, culture and response — not score selection alone — matter. [14] [15]
Regionally, NHS England national PEWS observation and escalation charts standardise inpatient documentation in England. Australia’s ACSQHC Recognising and Responding to Acute Deterioration Standard requires observation, escalation and governance systems without mandating one universal paediatric score. Canadian centres contributed to BedsidePEWS development and validation. US hospitals show wide local PEWS/RRS variation within AHA/AAP resuscitation context. Aotearoa New Zealand retrieval geography and culturally safe whānau participation shape escalation practice. Do not universalise one hospital’s colour bands. [1] [2]
Exam Pearls
- Cardiac arrest is too rare to be the only quality metric; use critical deterioration and process measures. [12]
- Fever modifies expected heart rate; it does not licence ignored tachycardia. [8]
- Incomplete charts are escalations, not excuses. [2]
- Distinguish track-and-trigger tool from early-warning system from rapid-response system. [4] [13]
- Give a structured MET activation sentence and ISBAR handover every time. [17]
- Cross-link the PAT first impression, then own the chart, the team and the culture on this page. [1] [2]
TRACK the deteriorating child
References
- [1]Parshuram, Christopher S Development and initial validation of the Bedside Paediatric Early Warning System score. Critical care (London, England), 2009.PMID 19678924
- [2]Parshuram, Christopher S Multicentre validation of the bedside paediatric early warning system score: a severity of illness score to detect evolving critical illness in hospitalised children. Critical care (London, England), 2011.PMID 21812993
- [3]Parshuram, Christopher S Effect of a Pediatric Early Warning System on All-Cause Mortality in Hospitalized Pediatric Patients: The EPOCH Randomized Clinical Trial. JAMA, 2018.PMID 29486493
- [4]Trubey, Rob Validity and effectiveness of paediatric early warning systems and track and trigger tools for identifying and reducing clinical deterioration in hospitalised children: a systematic review. BMJ open, 2019.PMID 31061010
- [5]Chapman, Susan M 'The Score Matters': wide variations in predictive performance of 18 paediatric track and trigger systems. Archives of disease in childhood, 2017.PMID 28292743
- [6]Lambert, Veronica Paediatric early warning systems for detecting and responding to clinical deterioration in children: a systematic review. BMJ open, 2017.PMID 28289051
- [7]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [8]Daymont, Carrie Heart rates in hospitalized children by age and body temperature. Pediatrics, 2015.PMID 25917984
- [9]Mills, Erin Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [10]Tibballs, James Reduction of paediatric in-patient cardiac arrest and death with a medical emergency team: preliminary results. Archives of disease in childhood, 2005.PMID 16243869
- [11]Tibballs, James Reduction of hospital mortality and of preventable cardiac arrest and death on introduction of a pediatric medical emergency team. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2009.PMID 19307806
- [12]Bonafide, Christopher P Impact of rapid response system implementation on critical deterioration events in children. JAMA pediatrics, 2014.PMID 24217295
- [13]Devita, Michael A Findings of the first consensus conference on medical emergency teams. Critical care medicine, 2006.PMID 16878033
- [14]Allen, Davina Development, implementation and evaluation of an evidence-based paediatric early warning system improvement programme: the PUMA mixed methods study. BMC health services research, 2022.PMID 34974841
- [15]Thomas-Jones, Emma A prospective, mixed-methods, before and after study to identify the evidence base for the core components of an effective Paediatric Early Warning System and the development of an implementation package containing those core recommendations for use in the UK: Paediatric early warning system - utilisation and mortality avoidance- the PUMA study protocol. BMC pediatrics, 2018.PMID 30045717
- [16]Kuo, Dennis Z Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [17]Starmer, Amy J Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [18]Boylen, Susan Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [19]Chaichotjinda, Krittiya Assessment of interhospital transport care for pediatric patients. Clinical and experimental pediatrics, 2020.PMID 31477679
- [20]Fleming, Susannah Validity and reliability of measurement of capillary refill time in children: a systematic review. Archives of disease in childhood, 2015.PMID 25260515
- [21]Fleming, Susannah The Diagnostic Value of Capillary Refill Time for Detecting Serious Illness in Children: A Systematic Review and Meta-Analysis. PloS one, 2015.PMID 26375953
- [22]Sharma, Megha Racial and skin color mediated disparities in pulse oximetry in infants and young children. Paediatric respiratory reviews, 2024.PMID 38233229
- [23]Ramgopal, Sriram Comparing AVPU and Glasgow Coma Scales Among Children Seen by Emergency Medical Services. Pediatrics, 2024.PMID 38993159
- [24]Burvenich, Ruben Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [25]Bragança-Souza, Kátia Kely Health Professionals: Identifying and Reporting Child Physical Abuse-a Scoping Review. Trauma, violence & abuse, 2024.PMID 36747372