Paeds · clinical-assessment-and-reasoning
Interpreting common paediatric laboratory reference ranges
Also known as Paediatric laboratory reference intervals · Age-specific lab normals in children · Paediatric blood test interpretation · CALIPER paediatric reference intervals · Critical values in paediatric laboratory medicine
A fellowship approach to age-, sex- and assay-aware interpretation of common paediatric laboratory results, distinguishing reference intervals from decision limits and critical values, with developmental biology, pre-analytical traps, communication and safe escalation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
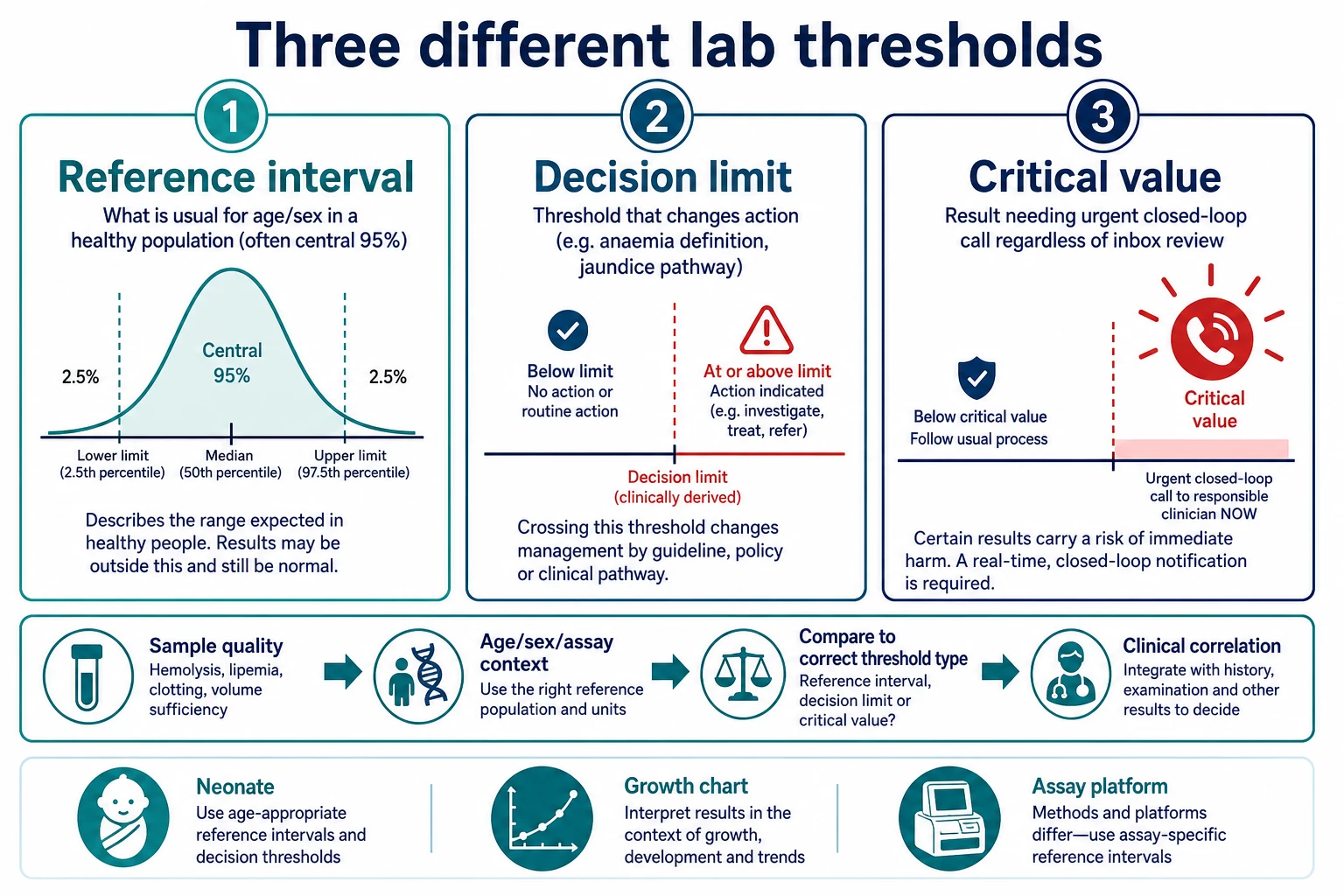
These three thresholds answer different questions and must not be collapsed into one red flag. [1] [8] [20]
Quote the source of the interval before you argue with a parent or an examiner. Local laboratory ranges on the report are the operational default after verification; large projects such as CALIPER and continuous multi-analyte work explain why those ranges move with age. [1] [9] [25]
A.S.S.A.Y.
Overview & Definition
You open a result and see a red flag. The first job is not to order five more tests. The first job is to ask: what question was this test answering, for which child, on which assay, and is this number even usable? [8]
A laboratory reference interval describes the distribution of results expected in a defined population under stated conditions. In children that population must respect developmental biology. Neonates are not toddlers; pubertal adolescents are not prepubertal schoolchildren. Establishing those intervals is hard because healthy children are difficult to sample at scale, ethics and phlebotomy limits bite hard, and many analytes change continuously with age rather than in neat bins. [8] [27] [28]
CALIPER (Canadian Laboratory Initiative on Pediatric Reference Intervals) was built to close that gap with healthy community children and multiethnic sampling for many biochemical markers. Continuous and big-data approaches later filled finer age resolution for haematology and chemistry where classical partitioning was too coarse. [1] [9] [11] [25]
Classification
Think in three layers before you speak. [8] [20]
1. Reference interval. Often the central 95% after exclusions, with age and sex partitions when needed. Some modern reports use continuous curves instead of step-bins. A value outside the RI is uncommon for the reference population; it is not a diagnosis. [1] [9]
2. Clinical decision limit. A threshold chosen because crossing it changes what you do. WHO anaemia haemoglobin cut-offs and AAP hyperbilirubinaemia treatment pathways are decision frameworks, not pure population RIs. [22] [23] [30]
3. Critical (panic) value. A result so extreme that the laboratory must notify a responsible clinician promptly and document closed-loop communication. Critical lists vary by hospital and country; national surveys show substantial inter-laboratory differences, so learn your list and the principle. [20] [21]
Also classify how the interval was made: direct sampling of healthy children (CALIPER-style), indirect/hospital data mining with statistical filtering, or transfer/verification of an existing interval onto a new analyser. Each method has strengths and failure modes. [5] [7] [25]
Epidemiology & Risk Factors
Paediatric RIs were historically incomplete. Many laboratories imported adult ranges or sparse textbook tables, then watched false “abnormals” flood paediatric inboxes. Initiatives such as CALIPER and continuous multi-analyte projects reduced that gap but did not abolish local verification work. [1] [27] [28]
Misclassification risk is highest when adult hospital LIS defaults are left on paediatric samples, day-of-life is ignored in the first week, non-fasting lipids or delayed samples are read as disease, ethnicity and iron status are ignored for haemoglobin and MCV, or critical-value policies differ between the laboratory and the clinician’s mental list. [3] [20] [29]
Community haemoglobin and MCV intervals in multiethnic toddlers still need careful local context; one Canadian community sample illustrates both the need for paediatric partitions and the influence of population mix. [29]
Pathophysiology
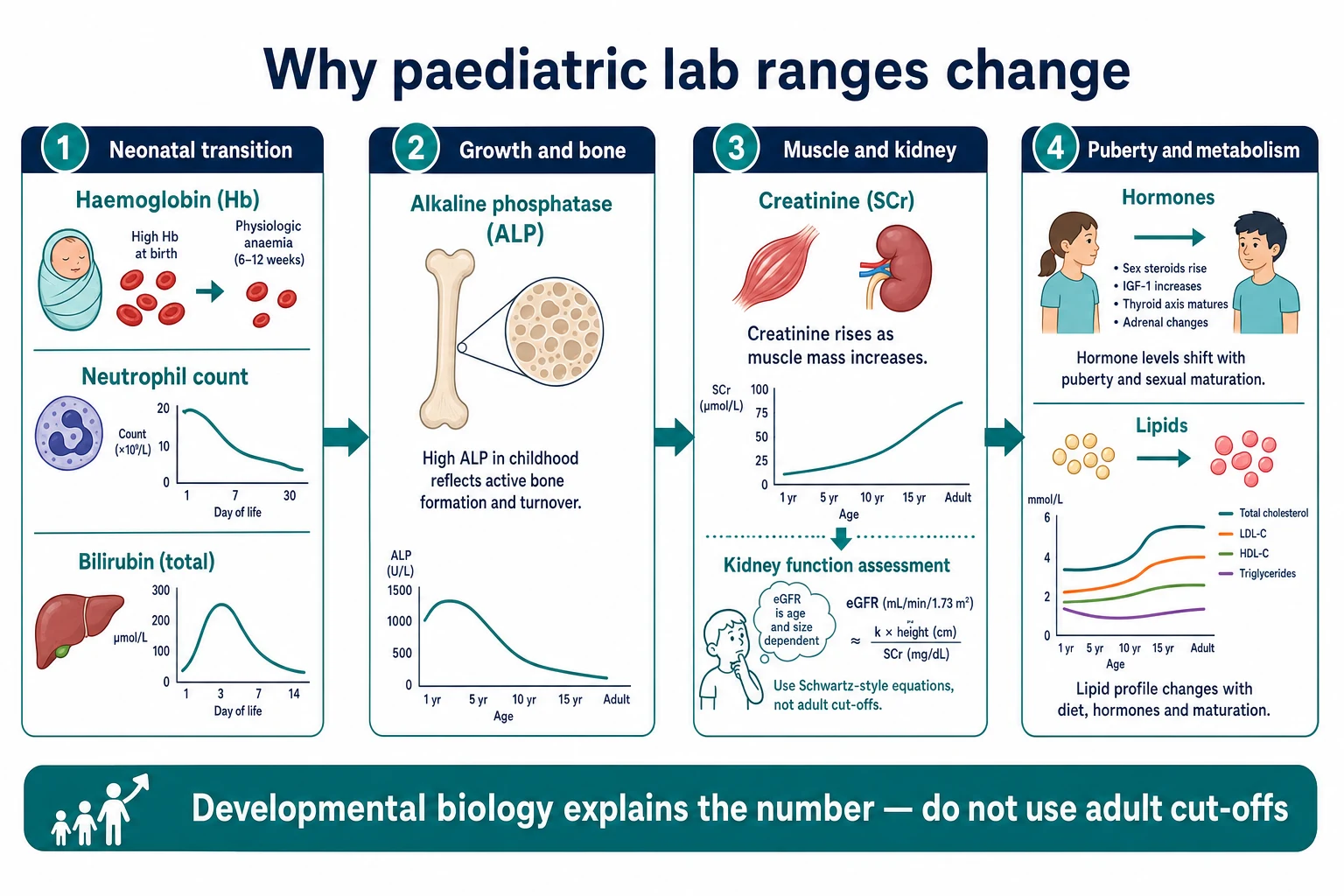
Neonatal transition. Haemoglobin is high at birth then falls toward a physiologic nadir in early infancy. Neutrophil counts swing across the first days of life; classic Manroe charts and later revisits show that postnatal age in hours matters. Platelets and red-cell indices also have neonatal-specific expected ranges derived from large multi-hospital datasets. Unconjugated bilirubin rises as the liver matures and red cells turn over, which is why jaundice pathways use age-in-hours charts rather than a single adult “normal”. [12] [13] [14] [15] [16] [22]
Growth and bone. Alkaline phosphatase is often high while bone turns over rapidly. Zierk and colleagues mapped paediatric ALP dynamics so that an isolated high ALP in a thriving child is not automatically “liver disease”. Look at the pattern (GGT, bilirubin, ALT/AST), growth and symptoms before cascading imaging. [10] [9]
Muscle and kidney. Serum creatinine tracks muscle mass as well as GFR. A low number in a small infant can be expected; the same absolute creatinine in an adolescent athlete is different. Paediatric eGFR equations such as the 2009 Schwartz bedside equation exist because adult eGFR tools misbehave in children. Creatinine RIs themselves need age-aware global scrutiny. [17] [18] [19]
Endocrine and metabolic variance. Childhood shows large biological variance in many endocrine and biochemical markers; CALIPER endocrine work quantified how wide “normal” can be across ages. Within-day biological variation and fasting/collection-time effects further move glucose, iron studies, lipids and other analytes. [2] [3] [4]
Puberty and lipids. Lipids and related cardiometabolic markers need paediatric reporting logic, not adult secondary-prevention cut-and-paste. Harmonised paediatric lipid reporting recommendations exist to reduce chaotic flags across laboratories. [24]
Clinical Presentation
Lab results arrive in four common stories: well-child or screening (mild flags, high risk of over-reaction); acute illness (numbers mixed with fever, dehydration and stress responses); chronic disease monitoring (the child’s own baseline matters more than the population band); and critical call (physiology may already be failing—treat and talk, do not debate percentiles). [8] [20]
Caregivers often hear “abnormal blood test” as “serious disease”. Your job is to translate: expected for age, needs recheck, needs targeted second test, or needs emergency care. Ask about symptoms, growth, diet, medicines (including biotin and supplements that wreck immunoassays), recent illness, and how the sample was taken. [3] [8]
Differential Diagnosis
Use the number as a clue, not a label. [8]
High ALP. Physiologic growth, healing fracture, vitamin D issues, biliary obstruction, drug effect, macro-ALP rarities. Cholestatic enzymes and clinical jaundice redirect you. [10]
High creatinine. True GFR fall, high muscle mass, recent meat/creatine context where relevant, assay interference, wrong age band, post-renal obstruction. Always estimate paediatric GFR thinking and urine output, not adult CKD staging alone. [17] [18]
Anaemia flag. Age-specific haemoglobin expectation, iron deficiency, thalassaemia trait, blood loss, marrow failure, laboratory error or wrong units. WHO anaemia definitions are decision tools layered on top of local RIs. [23] [29]
Neonatal neutrophil extremes. Sepsis until reasoned otherwise, but also know expected day-of-life curves so you do not both under-call and over-call. [13] [14] [12]
Thyroid and other endocrine flags. Age-specific physiology, non-thyroidal illness, assay problems. Do not apply adult TSH cut-offs to infants without paediatric context. [2]
Pre-analytical mimics. Haemolysis raising potassium, delayed separation, IV-fluid contamination, wrong patient, non-fasting triglycerides, capillary versus venous differences. If the child looks fine and the number looks lethal, recheck the sample pathway first while still protecting the child. [3] [20]
Clinical & Bedside Assessment
Stand next to the child before you stand next to the printer. Confirm identity, age in years and days if under one month, and clinical state. Look for dehydration, jaundice, purpura, growth failure, pubertal stage and medication lists. For chronic illness, find the usual creatinine, haemoglobin or gas values on the chart. If the draw was traumatic or delayed, say so in the notes; that is clinical data. For telehealth result review, you still need enough history to know whether this is a critical-value pathway or a counselling pathway. [3] [8] [20]
Document units, time of collection, fasting state when relevant, and the interval source you used. [3] [8]
Investigations
Common paediatric panels that demand age-aware reading include FBC, electrolytes, creatinine/eGFR, LFT/ALP, bilirubin, iron studies, thyroid tests and lipids. Each has characteristic traps: adult anaemia cut-offs, haemolysed potassium, adult eGFR apps on toddlers, imaging every high ALP in a thriving child, a single “normal bilirubin” idea, ferritin misread in inflammation, adult TSH panic in neonates, and adult statin decision cut-offs in children. [1] [10] [12] [17] [22] [23] [24]
Prefer the local verified paediatric range on the report for day-to-day work. Use CALIPER, continuous RI literature and harmonisation guidance to understand biology, transfer methods and why labs differ. When platforms change, intervals must be transferred or re-verified; Estey and Higgins showed CLSI-style transfer of CALIPER intervals across major chemistry systems is possible but not automatic. [1] [5] [6] [24] [26]
Hospital-derived indirect intervals can approximate healthy-child intervals for some analytes but are not automatically equivalent; Shaw and colleagues compared modified Hoffmann hospital approaches with CALIPER healthy-child intervals and highlighted validity limits. [7]
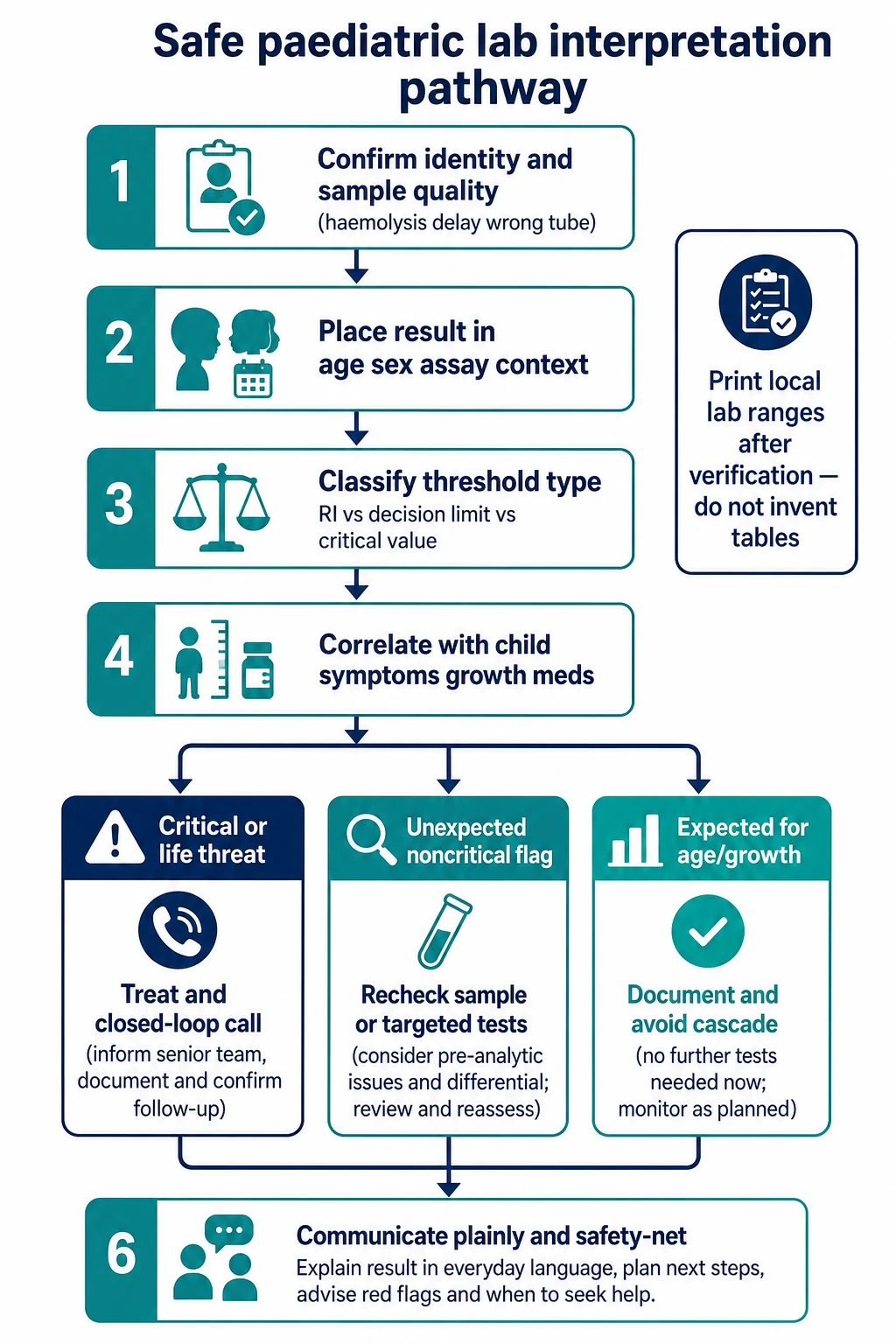
Retest before cascade when sample quality is doubtful and the child is stable. Escalate immediately when the pattern implies threat even if a second tube is on its way. [3] [20]
Management — Resuscitation
Some results are not “interesting flags”. They are emergencies wearing a lab coat. [20] [21]
Treat the child with ABCDE principles when the clinical picture or a verified critical result shows immediate danger: severe hyperkalaemia with ECG change, profound hypoglycaemia, extreme anaemia with shock, metabolic crisis patterns, or bilirubin risk needing urgent pathway care. Critical-value policy exists so these results never wait in an unread inbox. Know how your laboratory notifies, who receives the call, and how you document read-back. [20] [21] [22]
If the number is critically abnormal and the child looks well, protect both truths: start the safety pathway and simultaneously hunt for pre-analytical error without delaying care that would matter if the result is real. [3] [20]
Management — Definitive & Stepwise
Use a repeatable pathway: identity and sample quality; age, sex, day of life, fasting, meds and assay/units; threshold type (RI vs decision limit vs critical value); clinical correlation; then branch to treat/call, targeted retest, or expected-for-age documentation; finish with communication, safety-netting and handover that includes trend, units and next check time. [3] [8] [20]
Harmonisation efforts aim to reduce meaningless inter-lab differences where biology allows shared intervals; they do not remove the need for local verification or clinical judgement. [25] [26]
Specific Subtypes & Scenarios
Day-2 neonate with “high neutrophils”. Plot postnatal age before diagnosing sepsis or dismissing it. Use neonatal expected ranges and the whole baby. [12] [13] [14]
Thriving toddler, ALP twice the adult upper limit. Think bone growth first; check other liver tests and the child. [10]
Adolescent with creatinine “just above adult normal”. Assess muscle mass, hydration, urine findings and paediatric eGFR; do not shrug because the number looks mild on an adult scale. [17] [18]
Infant anaemia work-up. Use age-aware haemoglobin expectations and decision definitions; interpret MCV with population context. [23] [29]
Non-fasting lipid panel in clinic. Collection state changes interpretation; paediatric lipid reporting guidance exists to standardise what labs print. [3] [24]
Platform change in the hospital lab. Ask whether paediatric intervals were transferred/verified; do not assume old cut-offs still apply. [5] [6]
Technology-dependent child. Baseline gases, haemoglobin and inflammatory markers may sit outside population RIs forever; document personal baselines on the problem list. [8] [12]
Complications & Pitfalls
- Adult RIs on paediatric samples.
- Treating every red flag as disease.
- Ignoring haemolysis and delayed samples.
- Confusing RI, decision limit and critical value.
- Inventing memorised multi-analyte tables in viva instead of naming sources and principles.
- Missing closed-loop critical notification.
- Ordering expansive cascades that harm children through more blood loss and false positives.
- Explaining numbers without age context, creating lasting parental anxiety. [8] [20] [7]
Prognosis & Disposition
Disposition follows the combination of result severity, trajectory and whole-child assessment. A critical potassium with ECG changes is resuscitation and monitored care. A mild out-of-range ALP in a well child may be primary-care review or a planned recheck. Borderline creatinine with oliguria is not a “repeat next week” problem. [10] [17] [20]
For rural and telehealth settings, transport time lowers your threshold to move a child when the result and physiology both worry you. Handover must include age, units, collection time, haemolysis flags, actions taken and the next expected value. [20]
Special Populations
Preterm and ex-preterm infants. Haematology and creatinine trajectories differ from term norms; day-of-life and corrected age both matter. [12]
CKD, cyanotic heart disease, chronic liver disease. Population RIs are starting points only; personal baselines and disease-specific decision limits dominate. [17] [18]
Immunocompromised children. Inflammatory markers may under-call illness; do not require a “hot CRP” to believe danger. [8]
Indigenous, migrant and refugee families. Iron deficiency risk, language access and trust shape both testing and counselling; avoid deficit language and ensure interpreter use when needed. [29]
Disability and needle fear. Stewardship of blood volume and test indication is part of interpreting ranges—every unnecessary tube is a procedure. [8] [28]
Adolescents and transition. Adult lab formats appear; keep paediatric thinking until biology and services truly transition, and consider pregnancy possibility when relevant. [17] [24]
Evidence, Guidelines & Regional Differences
Landmark healthy-child biochemical RIs come from CALIPER, including Colantonio’s 40-marker multiethnic database and Bailey’s endocrine/biochemical variance work. Pre-analytical and biological-variation substudies refine how you read a single draw. Platform transfer papers show how those intervals move across analysers. [1] [2] [3] [4] [5] [6]
Continuous age-sex dynamics for many haematologic and biochemical analytes, dedicated ALP intervals, and next-generation haematology RIs come from Zierk and colleagues. Neonatal haematology rests on Manroe, Christensen, Schmutz and Wiedmeier-era datasets. [9] [10] [11] [12] [13] [14] [15]
Schwartz 2009 equations remain core teaching for paediatric eGFR estimation alongside careful creatinine RI assessment. Critical-value surveys from Canada and older US children’s hospital data prove that panic limits are policy choices requiring local mastery. AAP 2022 hyperbilirubinaemia guidance and WHO anaemia haemoglobin guidance exemplify decision limits layered on biology. CSCC lipid reporting and RI harmonisation best practice address cross-lab chaos. [17] [18] [19] [20] [21] [22] [23] [24] [26]
Exam Pearls
- Say the triad out loud: RI ≠ decision limit ≠ critical value. [20]
- Age and day-of-life before adjective (“high”, “low”). [12]
- ALP high in growing bones is common; pattern-read the liver panel. [10]
- Creatinine needs paediatric eGFR thinking. [17]
- Neonatal neutrophils move by hours of life. [13]
- CALIPER is healthy-community multiethnic biochemistry; still verify locally and transfer across platforms. [1] [5]
- If child and number disagree, recheck both. [3]
- Critical results need closed-loop communication. [20]
Teaching anchors (principles, not memorised tables)
References
- [1]Colantonio DA Closing the gaps in pediatric laboratory reference intervals: a CALIPER database of 40 biochemical markers in a healthy and multiethnic population of children. Clinical chemistry, 2012.PMID 22371482
- [2]Bailey D Marked biological variance in endocrine and biochemical markers in childhood: establishment of pediatric reference intervals using healthy community children from the CALIPER cohort. Clinical chemistry, 2013.PMID 23637247
- [3]Pasic MD Influence of fasting and sample collection time on 38 biochemical markers in healthy children: a CALIPER substudy. Clinical biochemistry, 2012.PMID 22820439
- [4]Bailey D Pediatric within-day biological variation and quality specifications for 38 biochemical markers in the CALIPER cohort. Clinical chemistry, 2014.PMID 24366727
- [5]Estey MP CLSI-based transference of the CALIPER database of pediatric reference intervals from Abbott to Beckman, Ortho, Roche and Siemens Clinical Chemistry Assays: direct validation using reference samples from the CALIPER cohort. Clinical biochemistry, 2013.PMID 23578738
- [6]Higgins V Transference of CALIPER pediatric reference intervals to biochemical assays on the Roche cobas 6000 and the Roche Modular P. Clinical biochemistry, 2016.PMID 26297116
- [7]Shaw JL Validity of establishing pediatric reference intervals based on hospital patient data: a comparison of the modified Hoffmann approach to CALIPER reference intervals obtained in healthy children. Clinical biochemistry, 2014.PMID 24316101
- [8]Ceriotti F Establishing pediatric reference intervals: a challenging task. Clinical chemistry, 2012.PMID 22377530
- [9]Zierk J Age- and sex-specific dynamics in 22 hematologic and biochemical analytes from birth to adolescence. Clinical chemistry, 2015.PMID 25967371
- [10]Zierk J Pediatric reference intervals for alkaline phosphatase. Clinical chemistry and laboratory medicine, 2017.PMID 27505090
- [11]Zierk J Next-generation reference intervals for pediatric hematology. Clinical chemistry and laboratory medicine, 2019.PMID 31005947
- [12]Christensen RD Expected erythrocyte, platelet and neutrophil values for term and preterm neonates. The journal of maternal-fetal & neonatal medicine, 2012.PMID 23025775
- [13]Manroe BL The neonatal blood count in health and disease. I. Reference values for neutrophilic cells. The Journal of pediatrics, 1979.PMID 480023
- [14]Schmutz N Expected ranges for blood neutrophil concentrations of neonates: the Manroe and Mouzinho charts revisited. Journal of perinatology, 2008.PMID 18200025
- [15]Wiedmeier SE Platelet reference ranges for neonates, defined using data from over 47,000 patients in a multihospital healthcare system. Journal of perinatology, 2009.PMID 18818663
- [16]Christensen RD The erythrocyte indices of neonates, defined using data from over 12,000 patients in a multihospital health care system. Journal of perinatology, 2008.PMID 17972890
- [17]Schwartz GJ New equations to estimate GFR in children with CKD. Journal of the American Society of Nephrology : JASN, 2009.PMID 19158356
- [18]Schwartz GJ Measurement and estimation of GFR in children and adolescents. Clinical journal of the American Society of Nephrology : CJASN, 2009.PMID 19820136
- [19]Ceriotti F Reference intervals for serum creatinine concentrations: assessment of available data for global application. Clinical chemistry, 2008.PMID 18202155
- [20]Gong Y A national survey on pediatric critical values used in clinical laboratories across Canada. Clinical biochemistry, 2009.PMID 19683519
- [21]Kost GJ Critical limits for emergency clinician notification at United States children's hospitals. Pediatrics, 1991.PMID 1881742
- [22]Kemper AR Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics, 2022.PMID 35927462
- [23]Pasricha SR Measuring haemoglobin concentration to define anaemia: WHO guidelines. Lancet (London, England), 2024.PMID 38493792
- [24]Higgins V Canadian Society of Clinical Chemists Harmonized Pediatric Lipid Reporting Recommendations for Clinical Laboratories. The Canadian journal of cardiology, 2024.PMID 38336003
- [25]Bohn MK Reference Interval Harmonization: Harnessing the Power of Big Data Analytics to Derive Common Reference Intervals across Populations and Testing Platforms. Clinical chemistry, 2023.PMID 37478022
- [26]Bohn MK Best practice guidelines on reference interval harmonization in Canada: Evidence-based recommendations from the CSCC working group on reference interval harmonization (CSCC WG-hRI). Clinical biochemistry, 2025.PMID 40763882
- [27]Jung B Clinical laboratory reference intervals in pediatrics: the CALIPER initiative. Clinical biochemistry, 2009.PMID 19591815
- [28]Shaw JL Pediatric reference intervals: challenges and recent initiatives. Critical reviews in clinical laboratory sciences, 2013.PMID 23656169
- [29]Hamid JS Reference intervals for hemoglobin and mean corpuscular volume in an ethnically diverse community sample of Canadian children 2 to 36 months. BMC pediatrics, 2021.PMID 34011305
- [30]Slaughter JL Technical Report: Diagnosis and Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics, 2022.PMID 35927519