Paeds · clinical-assessment-and-reasoning
Lymphadenopathy and organomegaly: diagnostic approach
Also known as Lymphadenopathy · Enlarged lymph nodes · Cervical lymphadenopathy · Hepatomegaly · Splenomegaly · Hepatosplenomegaly · Organomegaly
Fellowship diagnostic approach to paediatric lymphadenopathy and organomegaly: bedside mapping, red-flag recognition, infection–inflammation–malignancy ranking, investigation and biopsy gates, common scenarios (EBV, Bartonella, NTM, TB risk), counselling and exam-ready plans.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A lymph node is a filter station for the immune system. Children often have palpable nodes because they meet many new antigens. Lymphadenopathy means nodes that are enlarged, abnormal in character, or present in a pattern that needs explanation. It is a finding, not a final diagnosis. [2] [14]
Organomegaly here means an enlarged liver (hepatomegaly), enlarged spleen (splenomegaly), or both (hepatosplenomegaly). Like nodes, organomegaly is a sign that points to infection, congestion, infiltration, haemolysis, storage disease or inflammation. Your job is to decide urgency, build a ranked differential, and choose the next action that changes care. [14]
Most paediatric cervical lymphadenopathy in large series is infectious or reactive rather than malignant. That fact should calm panic, not stop thinking. You still look for the few children who need same-day work-up. [1] [8]
From doorway lump to plan
First look
Is the child toxic, struggling to breathe, or showing mediastinal/airway warning signs? Stabilise first.
Map
Document node sites, size trend, tenderness, mobility, skin change, drainage territory, liver span and spleen tip.
Sort pattern
Acute localised tender, chronic unilateral cervicofacial, generalised systemic, or high-risk character.
Act
Observe with safety-net, treat clear bacterial adenitis, test for targeted infections, image, or arrange tissue and specialty review.
Close the loop
Give return criteria, review timing, and a written problem representation.
Classification
Classify every case on four axes that change management: duration, distribution, character, and systemic context. [2] [3] [14]
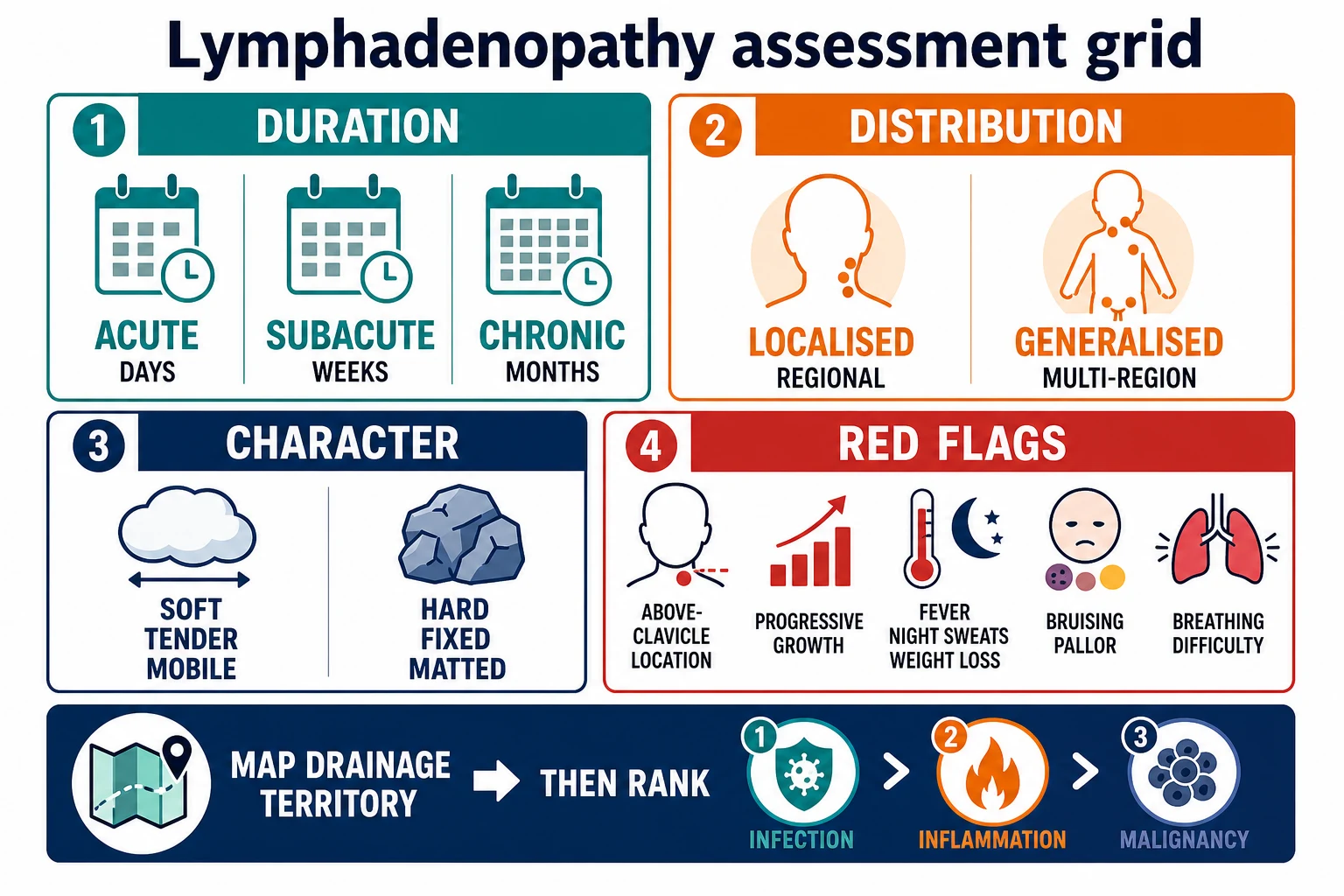
Duration. Acute means days. Subacute means weeks. Chronic means months. Reactive post-viral nodes often shrink over weeks. Persistence without improvement is a reason to reassess, not an automatic cancer label. [2] [5]
Distribution. Localised or regional nodes usually share a drainage territory (for example cervical nodes after pharyngitis or scalp infection). Generalised lymphadenopathy means multiple non-contiguous regions and should trigger a systemic differential. [2] [14]
Character. Soft, mobile and tender often fits inflammation. Hard, fixed, matted, rubbery or non-tender progressive masses raise concern for malignancy or granulomatous disease. Fluctuance suggests abscess. Violaceous skin over a chronic unilateral neck node raises nontuberculous mycobacteria (NTM) in the right age group. [2] [11] [17]
Supraclavicular nodes deserve special respect. They sit near deep drainage pathways and feature in malignancy-predictor discussions; treat them as high-concern until explained. [4] [7]
Likely reactive
Common community pattern
- Short history after URI or local skin/ENT source
- Tender, mobile, warm or mildly enlarged
- Child otherwise well or mildly unwell
- Improving trajectory with time or source control
Specific infection pattern
Named syndromes
- EBV: pharyngitis, fatigue, often generalised nodes ± spleen
- Bartonella: regional node after cat scratch/bite exposure
- NTM: chronic unilateral cervicofacial node, skin colour change
- TB risk: epidemiology, exposure, chronic adenitis
High-concern pattern
Do not watch forever
- Supraclavicular, hard, fixed, progressive
- Generalised nodes with B symptoms or cytopenia clues
- Mediastinal symptoms, bruising, bone pain
- Organomegaly with systemic illness
Epidemiology & Risk Factors
Reactive cervical lymphadenopathy is common in preschool and school-age children because viral respiratory infections and local skin or dental sources are common. In a systematic review of paediatric cervical lymphadenopathy etiologies across 2687 subjects, infectious causes dominated reported diagnoses, while malignancy was uncommon but clinically important. Use that base rate, then update it with red flags. [1]
Risk shifts with exposure and host: daycare, siblings and season raise ordinary viral and streptococcal disease. [1] [2]
- Daycare, siblings and season raise ordinary viral and streptococcal disease.
- Cat exposure raises Bartonella henselae (cat-scratch disease). [9]
- Soil/water and preschool age appear in classic NTM cervicofacial stories. [11] [17]
- Household TB contact, migration from high-burden regions and immunodeficiency raise TB concern. [13]
- Immunosuppression, transplant and known cancer predisposition change both differential and urgency. [14]
Biopsy series over-represent serious disease because only selected children reach the operating list. Lake’s classic surgical series and Soldes’ predictors remind you that selection matters: the clinic population is not the biopsy population. [7] [8]
Pathophysiology
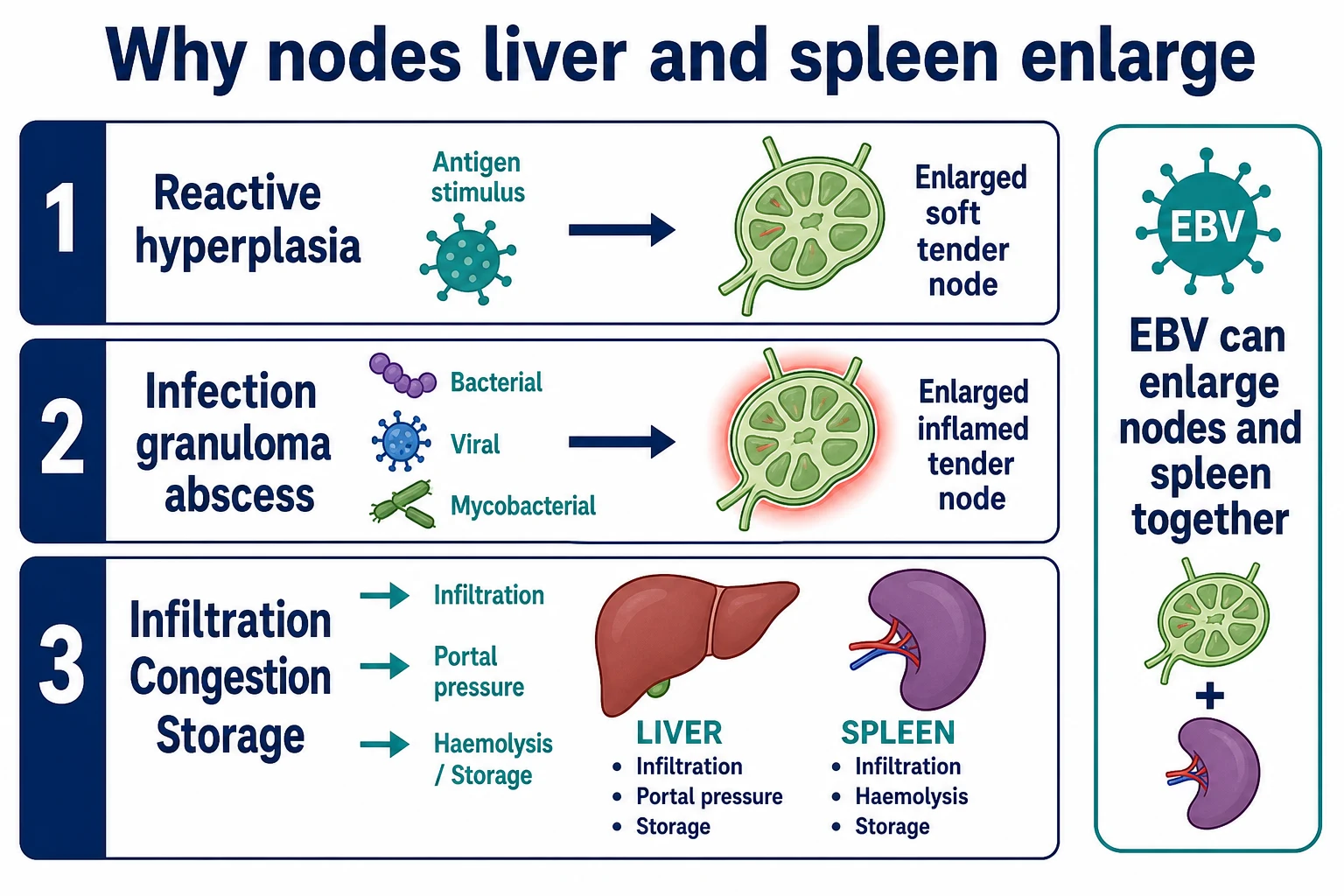
Lymph nodes enlarge when lymphoid tissue responds to antigen, when infection seeds the node, when granulomas form, or when malignant or storage cells infiltrate. Tender warmth fits acute inflammatory response. Hard fixation fits infiltration or chronic fibrosis and matting. [2] [14]
Drainage anatomy is practical, not decorative. Scalp and face infections drain to cervical stations. Oral and pharyngeal disease feed jugular chains. The arm feeds axillary nodes. The leg and perineum feed inguinal nodes. Finding the source often explains the node. [2] [3]
The spleen enlarges with infection (notably EBV), portal hypertension, extravascular haemolysis and infiltration. The liver enlarges with infection, congestion, infiltration, storage and some metabolic diseases. Combined hepato-spleno-lymphadenopathy points you toward systemic processes rather than a single local skin infection. [10] [14]
Clinical Presentation
Caregivers often say, “I felt a lump while washing her hair,” or “the doctor felt nodes with the throat infection.” Ask when it appeared, whether it is growing, whether it is tender, and what illnesses, bites, scratches, dental pain, travel, animal contact or TB exposures occurred. Ask about fever, night sweats, weight loss, pruritus, bone pain, bruising, pallor, cough, snoring change, noisy breathing and reduced activity. [2] [14]
Infectious mononucleosis may bring fatigue, sore throat, fever, cervical or generalised lymphadenopathy and splenomegaly. Adolescents often present with school or sport pressure to return quickly. [10]
Cat-scratch disease often brings a regional node weeks after a scratch or bite in the drainage territory, sometimes with low-grade fever. [9]
NTM cervicofacial disease classically brings a slowly progressive unilateral neck or preauricular node in a relatively well young child, later with skin discolouration or fistulisation. [11] [12] [17]
Malignancy concern rises with progressive non-tender masses, supraclavicular disease, mediastinal symptoms, cytopenia clues, bone pain or B symptoms. Do not wait for every classic feature. [4] [7]
Differential Diagnosis
Rank by pattern, not by alphabetical disease lists. [1] [2] [14]
- Reactive viral or local bacterial adenitis — common after URI or local infection. [1] [2]
- Named infections — EBV/CMV, streptococcal disease, Staphylococcus abscess, Bartonella, NTM, TB. [9] [10] [11] [13]
- Inflammatory and immune — Kawasaki disease context, autoimmune disease, haemophagocytic syndromes when extreme inflammation is present (cross-link specialty pages for full criteria). [14]
- Malignancy and infiltration — lymphoma, leukaemia, metastatic solid tumours, rare histiocytic disorders. [4] [7]
- Organomegaly-specific tracks — haemolysis, portal hypertension, storage disease, congestive cardiac disease, infiltrative marrow processes. [14]
| Pattern | Lead with | Do not miss |
|---|---|---|
| Short tender cervical after cold | Reactive adenopathy | Deep neck infection if toxic; abscess if fluctuance |
| Regional node + cat exposure | Bartonella | Atypical mycobacteria; bacterial abscess |
| Pharyngitis + fatigue ± spleen | EBV syndrome | Airway compromise; activity trauma risk to spleen |
| Chronic unilateral neck + skin colour change | NTM pathway | TB; incomplete bacterial treatment story |
| Hard / supraclavicular / progressive | Malignancy work-up | Mediastinal mass before anaesthesia |
| Generalised + cytopenia clues | Systemic disease / marrow | Leukaemia, HLH-spectrum illness, disseminated infection |
Clinical & Bedside Assessment
If the child looks seriously unwell, use your seriously-ill-child pathway first. Nodes wait for airway, breathing and circulation. Cross-link the PAT topic for doorway assessment. [2]
For the stable child, complete a full map before deciding on tests. [2] [3] [14]
- Inspect and palpate all major node stations — cervical levels, occipital, pre/post-auricular, submandibular, supraclavicular, axillary, epitrochlear if relevant, inguinal.
- Record size trend, number, tenderness, warmth, fluctuance, mobility, matting and overlying skin.
- Examine ENT, teeth, scalp, skin for a source.
- Examine the abdomen for liver edge/span and spleen tip; note any masses.
- Look for pallor, bruising, petechiae, gum changes, bone pain behaviour, growth and pubertal context.
- Plot growth if chronic disease or malignancy concern is live. [2] [3] [14]
Read the figure like this: start at the complaint site, then complete the map so you do not miss generalised disease. A single tender jaw-angle node after tonsillitis is a different problem from bilateral cervical plus axillary nodes with bruising. [2] [14]
Investigations
Tests should change management. Many well children with brief tender post-URI cervical nodes need observation and review, not a mega-panel. [2] [3] [5]
Consider first-line tests when nodes persist, generalise, feel high-risk, or come with systemic features. [2] [5] [14]
- Full blood count and film
- Inflammatory markers as clinically directed
- EBV (± CMV) serology when mononucleosis is plausible
- Throat testing when streptococcal disease would change care
- Bartonella serology with exposure and regional adenopathy
- TB risk-based testing when epidemiology fits
- Chest radiograph if mediastinal disease, TB risk or unexplained systemic adenopathy is plausible
- Ultrasound of the nodal basin to characterise architecture, suppuration and vascular pattern [2] [6] [9] [10] [13]
Thompson’s systematic review compares ultrasound and fine-needle aspiration (FNA) as initial evaluation strategies for paediatric cervical lymphadenopathy and supports careful pathway choice rather than automatic needling of every node. Ultrasound is often a useful first imaging step; FNA is not automatically first-line for every child. [6]
When lymphoma is a serious possibility, architecture-preserving biopsy (commonly excisional) is frequently preferred over FNA alone because lymphoma diagnosis and classification often need tissue architecture and adequate sample. Coordinate with ENT, surgery and oncology so the right node is sampled and staging needs are considered. Exclude critical mediastinal mass physiology before anaesthesia. [4] [6] [7]
Persistent asymptomatic cervical lymphadenopathy has dedicated modern management literature (Harris 2024): structured follow-up and selective investigation beat endless blind antibiotics. [5]
Management — Resuscitation
Treat life threats first. [2] [4] [10]
- Airway or deep-neck infection signs → senior airway help, imaging and surgical pathway as indicated.
- Suspected mediastinal mass → sit-up preference if needed, avoid unnecessary supine distress, urgent oncology/critical-care pathway, careful anaesthesia planning.
- Toxic bacterial adenitis or sepsis → local sepsis pathway, source control for abscess.
- Severe EBV with airway oedema → airway-aware supportive care.
- Massive splenomegaly with trauma risk → activity restriction counselling and avoid high-impact contact until risk is reassessed using local specialist advice and contemporary mono reviews. [10]
Do not invent a universal “return to contact sport on day X” rule in the exam if your source does not support a single number. State the principle: enlarged spleen raises rupture risk; restrict high-risk activity until clinical recovery and spleen risk are acceptable under local guidance. [10]
Management — Definitive & Stepwise
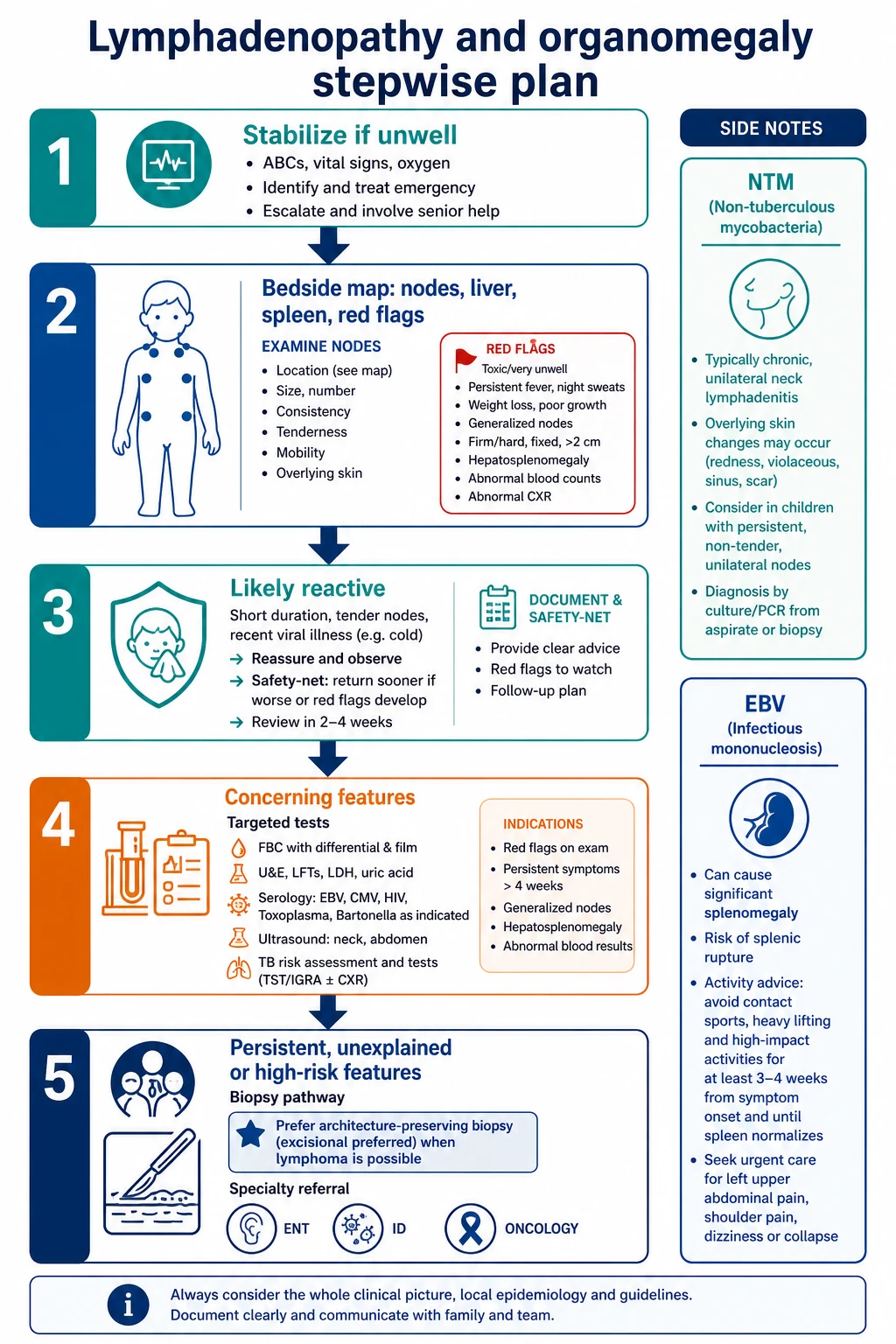
Step 1 — Likely reactive, well child. Explain the base rate, treat the source if needed, avoid serial unplanned antibiotics, give clear review timing and return precautions (rapid growth, fever, bruising, breathing difficulty, night sweats, weight loss). [2] [5]
Step 2 — Presumed acute bacterial lymphadenitis. If clinical bacterial adenitis is likely, use local antimicrobial guidance and arrange review. Fluctuance needs drainage planning, not antibiotics alone forever. [2]
Step 3 — Named infections.
- Bartonella: exposure history and serology-directed care per local ID advice. [9]
- EBV: supportive care, complication watch, spleen-aware activity advice. [10]
- NTM: use consensus-informed ENT/ID pathways; incomplete “abscess drainage only” without mycobacterial thinking is a classic pitfall. [11] [12] [16]
- TB risk: test and treat within public-health frameworks; Cruz highlights real management dilemmas. [13]
Step 4 — Persistent or high-risk. Structured imaging, laboratory evaluation, and surgical/oncology referral using streamlined approaches such as those discussed by Grant (APSA Cancer Committee) and Chang. [3] [4] [5]
Step 5 — Organomegaly track. If spleen or liver dominates, widen to haemolysis, portal hypertension, storage/metabolic disease, cardiac congestion and marrow infiltration while you still complete the node map. [14]
Specific Subtypes & Scenarios
Post-URI tender cervical node. Observe if improving and examination is otherwise normal; safety-net. [2]
Persistent asymptomatic cervical node. Follow a deliberate review and selective investigation plan rather than open-ended reassurance or endless antibiotics. [5]
Cat-scratch regional adenopathy. Ask about kittens and scratches; examine the inoculation site. [9]
EBV with sport pressure. Explain fatigue, contagious period concepts in plain language, and spleen protection principles. [10]
NTM-pattern neck mass. Relatively well preschool child, slow unilateral progression, skin change — involve ENT/ID early. [11] [17]
Supraclavicular or hard progressive mass. Same-week (or same-day if unwell) pathway toward imaging and tissue diagnosis. [4] [7]
Generalised lymphadenopathy with cytopenias. Think marrow and systemic disease; urgent FBC/film and specialty involvement. [14]
Complications & Pitfalls
- Reassuring on size alone without systemic review. [2]
- Missing supraclavicular disease. [7]
- Serial antibiotics without a diagnostic plan. [5]
- FNA when architecture-preserving biopsy is needed. [4] [6]
- Clearing contact sport with an enlarged spleen. [10]
- Treating NTM as ordinary bacterial abscess only. [11] [12]
- Biopsy anaesthesia without mediastinal risk assessment. [4]
- No interpreter for exposure and TB history.
Prognosis & Disposition
Most reactive nodes improve. Persistent or high-risk patterns need a timed plan with named ownership. Same-day care is for toxicity, airway/mediastinal threat, severe cytopenias, or rapidly progressive concerning masses. Clinic follow-up suits improving localised tender nodes with reliable caregivers. Document expected trajectory and what would change the plan. [2] [5]
Special Populations
- Young infants: lower threshold for serious bacterial work-up when febrile and node disease is part of systemic illness.
- Immunocompromised children: broader infection and malignancy risk; earlier specialty input. [14]
- Migrant/refugee families: TB and interrupted immunisation histories matter; use professional interpreters. [13]
- Indigenous families: culturally safe TB and infection conversations without stigma.
- Adolescents: confidential history when sexual transmission and lifestyle exposures are relevant; clear sport counselling in EBV. [10]
Evidence, Guidelines & Regional Differences
Deosthali’s systematic review quantifies how often infectious etiologies dominate cervical lymphadenopathy series. Weinstock, Chang and Stanford provide practical evaluation frames. Grant offers a surgeon-facing streamlined approach from APSA Cancer Committee work. Harris addresses persistent asymptomatic cervical nodes. Thompson compares ultrasound and FNA first strategies. Soldes and Lake inform malignancy-risk thinking in selected cohorts. Klotz, Leung, Roy/Gallois/Mandell/Suskind and Cruz anchor Bartonella, EBV, NTM and TB-risk care. Regional differences mainly affect TB testing pathways, specialty access and sports-medicine culture, not the core bedside map. [1] [2] [3] [4] [5] [6] [11] [13]
Exam Pearls
- Most childhood neck nodes are reactive — still examine red flags every time. [1]
- Supraclavicular, hard, fixed, progressive, generalised + systemic features → escalate. [4] [7]
- Map drainage territory; find the source. [2]
- Ultrasound characterises; trajectory and tissue still matter. [6]
- Lymphoma often needs architecture — know when not to rely on FNA alone. [4]
- EBV: supportive care plus spleen-aware activity advice. [10]
- NTM: chronic unilateral cervicofacial node with skin change. [11]
- Safety-net enlarging nodes, bruising, breathing difficulty, night sweats, weight loss. [2] [14]
Regional practice notes
ANZ. Use local TB screening and public-health pathways; culturally safe practice with Aboriginal, Torres Strait Islander and Māori/Pacific families.
UK. Secondary-care referral norms and feverish-illness frameworks sit beside node assessment; do not invent a non-existent single NICE “node size chart.”
US/Canada. Pediatrics in Review and APSA-aligned surgical approaches influence clinic and biopsy thresholds; access varies by system. [3] [4] [13] [14]
How Boards Test This
Written papers test pattern recognition and next best step. Long cases integrate chronic nodes with growth, infection risk and family impact. Short cases test neck and abdominal examination. Communication stations test biopsy explanation and EBV sport counselling without false certainty. Structured orals challenge you on malignancy predictors, NTM versus TB thinking, and when observation is defensible. [4] [5] [10] [11]
References
- [1]Deosthali A Etiologies of Pediatric Cervical Lymphadenopathy: A Systematic Review of 2687 Subjects Global pediatric health, 2019.PMID 31384630
- [2]Weinstock MS Pediatric Cervical Lymphadenopathy Pediatrics in review, 2018.PMID 30171054
- [3]Chang SSY An approach to cervical lymphadenopathy in children Singapore medical journal, 2020.PMID 33283242
- [4]Grant CN Lymphadenopathy in children: A streamlined approach for the surgeon - A report from the APSA Cancer Committee Journal of pediatric surgery, 2021.PMID 33109346
- [5]Harris JE Management of Pediatric Persistent Asymptomatic Cervical Lymphadenopathy Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery, 2024.PMID 37418178
- [6]Thompson JA Ultrasound versus fine needle aspiration for the initial evaluation of pediatric cervical lymphadenopathy-A systematic review International journal of pediatric otorhinolaryngology, 2023.PMID 36812785
- [7]Soldes OS Predictors of malignancy in childhood peripheral lymphadenopathy Journal of pediatric surgery, 1999.PMID 10549745
- [8]Lake AM Peripheral lymphadenopathy in childhood. Ten-year experience with excisional biopsy American journal of diseases of children (1960), 1978.PMID 645650
- [9]Klotz SA Cat-scratch Disease American family physician, 2011.PMID 21243990
- [10]Leung AKC Infectious Mononucleosis: An Updated Review Current pediatric reviews, 2024.PMID 37526456
- [11]Roy CF International Pediatric Otolaryngology Group: Consensus guidelines on the diagnosis and management of non-tuberculous mycobacterial cervicofacial lymphadenitis International journal of pediatric otorhinolaryngology, 2023.PMID 36764081
- [12]Gallois Y Nontuberculous lymphadenitis in children: What management strategy? International journal of pediatric otorhinolaryngology, 2019.PMID 31039497
- [13]Cruz AT Tuberculosis Cervical Adenitis: Management Dilemmas The Pediatric infectious disease journal, 2016.PMID 27273690
- [14]Stanford EF Lymphadenopathy: Differential Diagnosis and Indications for Evaluation Pediatrics in review, 2024.PMID 39085185
- [15]Tekgül H A prospective study of peripheral lymphadenopathy in childhood Journal of tropical pediatrics, 1997.PMID 9143186
- [16]Mandell DL Management of nontuberculous mycobacterial cervical lymphadenitis Archives of otolaryngology--head & neck surgery, 2003.PMID 12622546
- [17]Suskind DL Nontuberculous mycobacterial cervical adenitis Clinical pediatrics, 1997.PMID 9241478