Paeds · clinical-assessment-and-reasoning
Medication reconciliation and polypharmacy in children
Also known as Medicines reconciliation in children · Paediatric medication reconciliation · Polypharmacy in children · Best Possible Medication History · Paediatric deprescribing
A fellowship approach to paediatric medication reconciliation and polypharmacy: Best Possible Medication History, intentional versus unintentional discrepancies, high-risk transitions, children with medical complexity, liquid dosing safety, deprescribing and teach-back communication across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a seven-year-old with epilepsy arriving in ED after a seizure. The electronic list shows “levetiracetam.” Mother says the dose changed last week. A second bottle of clobazam is in the bag but missing from the chart. The last discharge summary still lists a temporary lorazepam PRN from a prior admission. If you prescribe from the screen alone, you are guessing. That guess is how children are harmed. [13] [17] [1]
Medication reconciliation is the structured process of obtaining the best possible list of a child’s current medicines, comparing it with what is ordered or dispensed at a transition of care, resolving differences, and communicating the final plan. It is work, not a click. [1] [23] [24]
A Best Possible Medication History (BPMH) is that verified list. You build it from more than one source: caregiver interview, medicine bottles or photos, pharmacy records, specialty letters and the electronic record. Copying the last discharge list is not a BPMH. [1] [18]
Polypharmacy in children means a child is taking multiple medicines in a way that raises complexity, interaction risk, administration burden or uncertainty about ongoing need. Adult cut-offs such as “five drugs” are a weak exam answer on their own. In children with medical complexity, many concurrent medicines are common; the clinical task is to make the regimen safer and purposeful, not to shame the count. [6] [7] [8] [27]
What reconciliation actually does
Gather sources
Interview caregivers, inspect bottles or photos, call pharmacy, read specialty notes and prior discharges.
Build the BPMH
For each medicine capture name, strength or concentration, dose, route, frequency, indication, last dose and adherence.
Compare and classify
Match the BPMH to current orders. Label each difference intentional or unintentional.
Fix what matters
Correct clinically important unintentional gaps the same shift; document intentional holds.
Teach and hand off
Use teach-back, supply the right devices, and send the final list to the medical home and family.
Classification
Start with the child and the bottles in front of you, then classify the list problem as carefully as the disease problem. [1] [18]
Intentional versus unintentional discrepancies
An intentional discrepancy is a documented clinical decision: a temporary hold for surgery, a deliberate dose change, a medicine stopped for toxicity. It still needs clear communication so the next team does not “correct” it back into harm. [1] [21]
An unintentional discrepancy is an unexplained difference between what the child should be taking and what the orders or discharge list show. Classic patterns include omission, commission (an extra medicine), wrong dose, wrong frequency, wrong form, wrong route and therapeutic duplication. [21] [22] [17]
Not every discrepancy is equally dangerous. Missing a multivitamin is not the same as missing an anticonvulsant. Train yourself to ask three questions: Is it intended? Is it clinically important? Who owns the fix and by when? [23] [25]
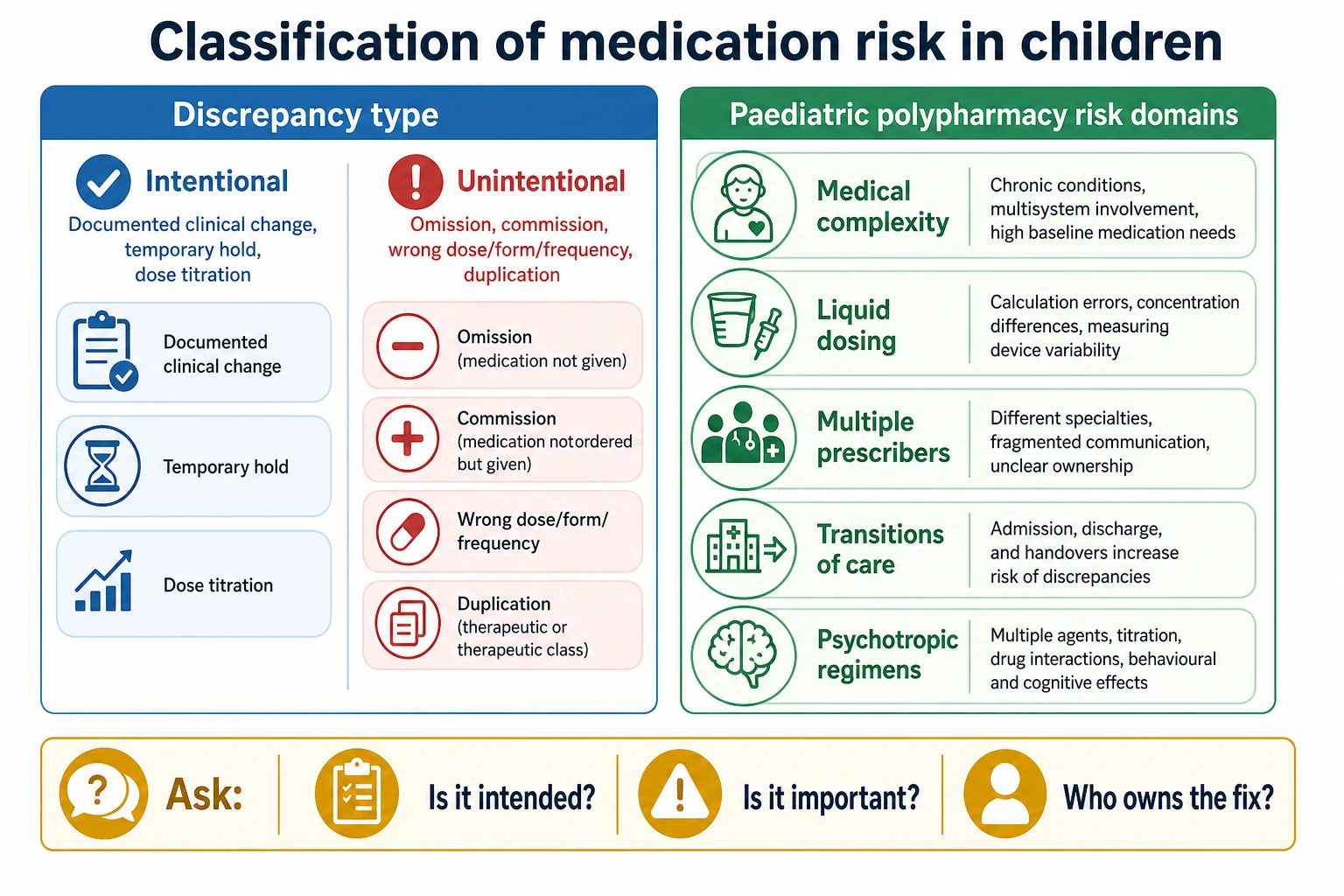
Read the figure like this: if a medicine disappeared from the list without a reason in the notes, treat it as unintentional until proven otherwise—especially anticonvulsants, steroids, insulin, anticoagulants and immunosuppressants. [13] [16]
Ways polypharmacy shows up in children
| Pattern | What you see | Why it matters |
|---|---|---|
| CMC polypharmacy | Many scheduled and PRN medicines across organ systems | High interaction, administration and omission risk |
| Psychotropic polypharmacy | Multiple CNS-active agents, sometimes without clear indication review | Measurement and safety require careful methods, not slogans |
| Antiepileptic polytherapy | Several anticonvulsants, brand/formulation switches | Admission discrepancy risk is high |
| Temporary cascade | Inpatient laxative, PPI, hypnotic left on home list | Creates avoidable chronic exposure |
| OTC and complementary stack | Antipyretics, herbal products, shared household medicines | Invisible on the EHR until you ask |
BPMH
Verified truth for today
- Multiple sources
- Dose and concentration explicit
- Includes OTCs and devices
- Names who provided each fact
EHR list alone
A starting hypothesis
- Often stale after specialty visits
- May omit school doses
- May retain stopped medicines
- Never sufficient alone at transitions
Family bag of bottles
High-yield evidence
- Shows what is actually used
- Reveals duplicates and old scripts
- Needs interpretation with dates
- Still confirm adherence and last dose
Epidemiology & Risk Factors
Medication discrepancies are common at paediatric transitions. Admission and discharge studies repeatedly find mismatches between home therapy and hospital documentation, and a portion are clinically important. Exact percentages vary by setting and method, so examiners care more about the risk pattern than one memorised rate. [25] [17] [12] [10]
After hospital discharge into the community, medication errors and medication-related harm remain a major safety theme across populations; children inherit the transition risk and add dosing-form complexity. [9] [19] [4]
Risk clusters you should name in exams: [7] [16]
- Child factors: medical complexity, technology dependence, epilepsy, polypharmacy, age under five, recent dose changes. [6] [13] [30]
- Medicine factors: high-alert agents, narrow therapeutic index, look-alike/sound-alike names, multiple concentrations of the same liquid. [7] [1]
- System factors: fragmented records, multiple specialists, incomplete handoffs, weekend discharges, rural shared care. [7] [11] [3]
- Communication factors: language discordance, low health literacy, multiple caregivers, school dosing not visible to hospital teams. [34] [35]
Children with medical complexity concentrate the problem: many medicines, many teams and high caregiver load. Polypharmacy is both a marker of complexity and a modifiable safety target. [6] [8] [27] [28]
Pathophysiology
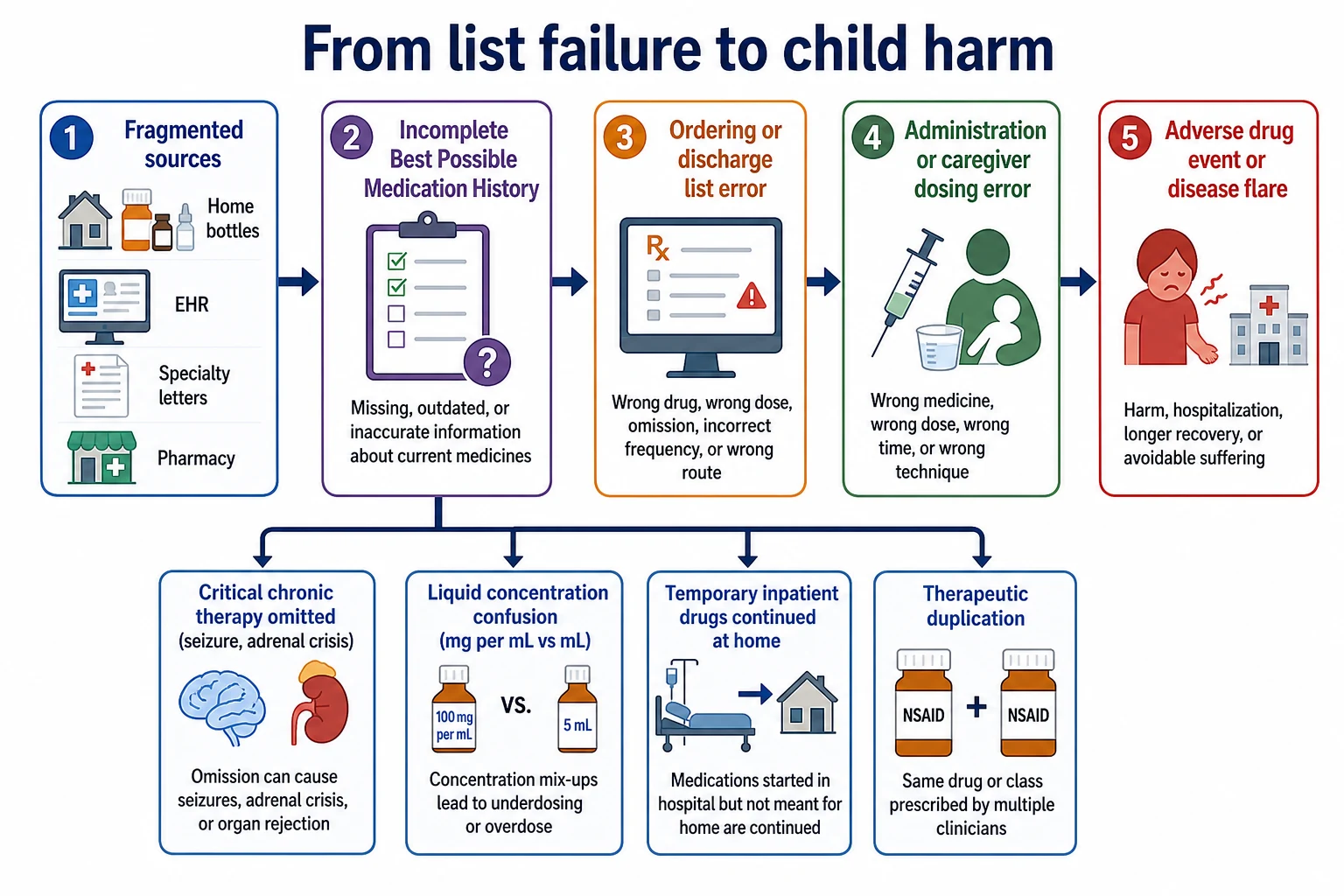
Think in a chain, not a slogan. Incomplete history becomes wrong orders. Wrong orders become wrong administration. Wrong administration becomes toxicity, withdrawal or disease flare. [21] [9]
Omission of critical chronic therapy is the classic paediatric catastrophe path. A missed anticonvulsant can present as status epilepticus. A missed steroid in adrenal insufficiency can present as shock. A missed immunosuppressant can present as graft threat or disease rebound. The physiology is the underlying disease unmasked by the list failure. [13] [16] [7]
Commission and duplication push exposure up. Two sedating agents, two antipyretic products containing the same drug, or brand-plus-generic double prescribing create additive toxicity. [12] [1]
Liquid dosing failure is a paediatric-specific mechanism. Labels in teaspoons, kitchen spoons, and confusion between milligrams and millilitres all drive home administration errors. Parent randomised studies show that units, pictograms and dosing tools change error risk. [34] [35] [36]
Prescribing cascades appear when a side effect is treated with a new medicine instead of reviewing the first one. Constipation after opioids, sleep disruption after stimulants, or reflux labels after some anticonvulsants can quietly lengthen the list. [6] [14]
Cognitive load matters. Caregivers of children with medical complexity may administer many timed doses through tubes, pumps and oral syringes. Complexity itself becomes a causal pathway to missed or delayed doses. [7] [28]
Clinical Presentation
Reconciliation problems present as system stories before they present as textbook toxidromes. [1] [3]
At the front door: a plastic bag of bottles, conflicting caregiver accounts, “we changed the dose last month,” or an EHR list that the family does not recognise. [5] [17]
As acute illness: breakthrough seizures, asthma flare after controller omission, adrenal crisis physiology after steroid gaps, withdrawal after abrupt psychotropic loss, or sedation after duplication. [13] [16]
As “new disease”: unexplained lethargy, vomiting, arrhythmia symptoms, rash labelled allergy without detail, or behavioural change that is actually a drug effect. Always ask what changed in the medicine list. [7] [6]
After discharge: early unplanned return, caregiver confusion, leftover inpatient medicines still being given, or an antibiotic liquid measured with a kitchen spoon. [9] [12] [34]
In clinic: polypharmacy without clear indications, expired PRNs still active, specialty letters that never updated primary care, and adolescents who take a different regimen from the one parents report. [3] [15]
Differential Diagnosis
| What it looks like | Discriminator | First move |
|---|---|---|
| Unintentional omission | No documented reason; family still has the medicine | Restore critical therapy and document |
| Intentional hold | Clear clinical reason and plan to restart | Communicate; do not blindly restart |
| Non-adherence | Family understands plan but barriers block execution | Fix access, schedule, taste, cost, beliefs |
| Unworkable regimen | Too complex for real life | Simplify with the team |
| True allergy | Specific reaction detail and timing | Record reaction; avoid re-challenge if serious |
| Intolerance or side effect | Predictable adverse effect, not immune allergy | Consider deprescribe or dose change |
| Dispensing or administration error | Pharmacy label or measurement tool mismatch | Correct tool and teach-back |
| Disease progression | List is accurate; condition is worse | Treat disease; still recheck high-risk drugs |
| Safeguarding concern | Covert dosing, unexplained toxicity, concealment | Follow local safeguarding pathway in parallel |
Do not diagnose “non-compliant family” until you have tested whether the regimen is understandable, measurable and affordable. [28] [34]
Clinical & Bedside Assessment
You can run a high-yield medication assessment in minutes if you are systematic. [1] [5]
1. Open with purpose.
“I need to check every medicine your child actually takes so we do not miss or double anything.” Invite bottles, blister packs, pump settings and school forms. [1]
2. Build the BPMH line by line.
For each medicine ask: name, strength or concentration, dose, route, frequency, indication, time of last dose, who gives it, and whether any doses are missed. Include OTCs, vitamins, herbal products, shared household medicines and contraceptive or adolescent-only medicines. [1] [18]
3. Capture paediatric specifics.
Liquid concentration in mg/mL, dose in mL and mg, oral syringe size, feeds around enteral medicines, crushed or opened capsules, and device-related drugs. [34] [7]
4. Map the network.
Who prescribes? Which pharmacy fills? Which doses are given at school, respite or by a second caregiver? [3] [31]
5. Allergy detail, not labels alone.
“What happened, how soon, and what was done?” Separate allergy from intolerance. [1]
6. Assess understanding with teach-back.
Ask the caregiver to show you how they would draw up the next liquid dose. Watching beats asking “do you understand?” [34] [35]
7. Grade source reliability.
Document which facts came from bottles, pharmacy, caregiver memory or letters. Source attribution protects the next clinician. [1] [5]
Investigations
The first investigation is often information retrieval, not another blood test. [1] [3]
High-value data sources: [1] [24]
- Caregiver interview and medicine containers. [1]
- Community pharmacy dispensing history. [3]
- Specialty letters and recent dose-change notes. [32]
- Prior discharge summaries and transfer lists. [12] [29]
- Device downloads or pump settings where relevant. [7]
- Pharmacist-led medication history, especially for complex regimens. [26] [32]
When laboratories help: suspected toxicity, unexplained altered consciousness, electrolyte effects of medicines, drug levels for selected anticonvulsants when clinically indicated, or glucose when hypoglycaemic agents are possible. Labs support the clinical story; they do not replace the list. [7]
Service metrics such as discrepancy rates and discharge error counts are quality tools. They guide unit improvement and should not be treated as a bedside severity score for one child. [4] [2] [5]
Avoid harm from duplicated tests ordered only because prior results or drug levels are inaccessible. Fix retrieval while you treat the child. [3]
Management — Resuscitation
Medication safety never outranks airway, breathing, circulation, seizure control, glucose or anaphylaxis care. [16] [7]
If the child is critically unwell and drugs may be involved: [16]
- Call for help and run age-adapted ABCDE.
- Ask for last doses of critical home medicines and any possible overdose or missed doses.
- Use emergency plans, steroid cards, device settings and medical-home summaries in parallel.
- Stop further wrong-dose administration until the list is safe enough to use.
- Involve pharmacy and toxicology pathways according to local practice when toxicity is likely.
- After stabilisation, complete full reconciliation so the ICU or ward does not inherit the same gap. [16] [11]
For retrieval, the medication list is a core handoff element. Name recent changes explicitly; handoff programmes that standardise communication reduce medical errors and are relevant whenever medicines change at shift or site transfer. [11]
Management — Definitive & Stepwise
This is the constructive algorithm examiners want. [1] [23]
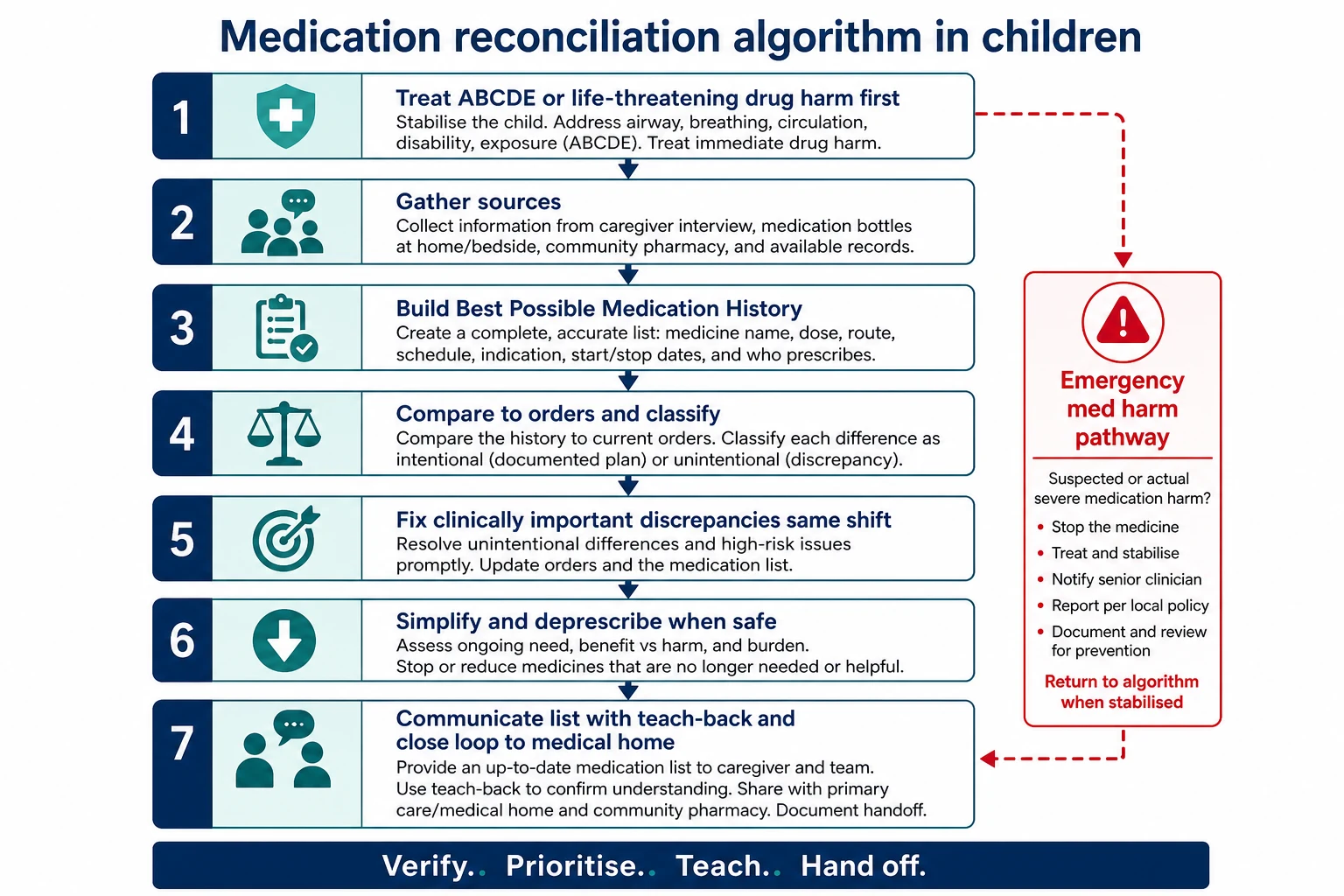
Step 1 — Make the child safe first
If there is ABCDE threat or high-alert toxicity, resuscitate first. Reconciliation continues in parallel once immediate risk is controlled. [16]
Step 2 — Gather sources and build the BPMH
Use at least two independent sources whenever possible. Prefer bottles plus caregiver interview plus pharmacy or chart data for complex children. [1] [24]
Step 3 — Compare orders with the BPMH
Mark every difference. Decide intentional versus unintentional. Escalate clinically important unintentional discrepancies for same-shift correction. [21] [25]
Step 4 — Prioritise high-risk gaps
Critical chronic therapy, high-alert medicines, anticoagulants, insulin, opioids, anticonvulsants, systemic steroids and immunosuppressants come first. Administrative tidy-ups can wait; seizures cannot. [13] [7]
Step 5 — Reconcile at every transition
Admission, ward transfer, ICU step-down, ED discharge and hospital discharge each need a fresh comparison. Transfer between wards is an under-recognised discrepancy point. [29] [2] [12]
Step 6 — Discharge like it is a procedure
Match the final list to what the family will actually give at home. Remove temporary inpatient medicines. Align supply, devices and school forms. Pharmacist-supported discharge reconciliation can catch residual errors; local models vary. [26] [4] [19]
Step 7 — Teach with teach-back
Explain changes in plain language. Demonstrate liquid measurement with an oral syringe. Ask the caregiver to teach the plan back. Use professional interpreters when language discordance exists. [34] [35]
Step 8 — Deprescribe with intention
For every medicine ask: indication, effectiveness, safety, adherence burden and family goals. Stop or taper what no longer serves the child. UK clinicians report barriers to paediatric deprescribing; name the barriers and still attempt structured review. [14] [6] [27]
Step 9 — Close the loop
Send the final list to the medical home, relevant specialists and the family. Document owners and timing for outstanding clarifications. Ambulatory reconciliation after external visits belongs in the paediatric medical home. [3] [31]
Step 10 — Improve the system
Standardise ED and ward workflows, enable pharmacist partnership, and measure clinically important discrepancies rather than checkbox completion alone. Local QI can raise completion and accuracy, but accuracy needs ongoing attention even when steps are “done.” [2] [5] [24]
Specific Subtypes & Scenarios
ED discharge after a simple illness. New antipyretic or antibiotic instructions must not overwrite chronic therapy. Reconfirm the long-term list before the family leaves. [2] [34]
Epilepsy admission. Expect formulation changes and high discrepancy risk. Confirm total daily anticonvulsant dose in mg/kg only after the true home regimen is known. [13] [32] [33]
PICU and intermediate care for chronic disease. Reconciliation failures are common when many infusions and home medicines coexist. Reconcile on arrival and at every major transition. [16]
Children with medical complexity. Treat polypharmacy review as core complex care, not a pharmacy hobby. Align specialists, reduce cascade prescribing and support caregivers. [6] [7] [30] [28]
Ward-to-ward transfer. Temporary medicines and incomplete lists travel with the patient. Re-check before the next team inherits the error. [29]
Adolescent psychotropic regimens. Clarify indications, prescribers and self-administration. Methodologic caution matters when counting psychotropic polypharmacy; still review safety and monitoring. [15]
Foster or kinship care. Expect missing history. Use pharmacy records, prior hospital systems and child-protection information-sharing rules while treating acute needs. [3]
Language-discordant families. Professional interpreter for medication counselling is a safety intervention, not a courtesy. [34]
Neonates and young infants. Weight-based liquids, rapid weight change and multiple caregivers demand frequent re-checks of dose volume. [34] [7]
Complications & Pitfalls
- Checkbox reconciliation without verification leaves harm rates unchanged in spirit even if the form is complete. [5] [23]
- Copy-forward discharge lists reintroduce stopped medicines. [12] [4]
- Volume-only liquid orders without concentration invite ten-fold thinking errors. [34] [36]
- Allergy dumping blocks essential therapy when reaction detail is absent. [1]
- Ignoring school doses creates daytime gaps or double dosing. [3]
- Abrupt deprescribing of steroids or some CNS agents without a taper plan. [14]
- Blaming families for system-created complexity. [28] [7]
- Handoffs that omit medication changes recreate the same error on the next shift. [11]
Prognosis & Disposition
Process reliability improves when teams standardise reconciliation and involve pharmacists, but outcome evidence is stronger for reducing discrepancies than for guaranteeing mortality reduction. Say that nuance in exams. [23] [24] [2]
Safe disposition requires: [19] [3]
- No unresolved high-risk unintentional discrepancy. [13]
- A written final list the caregiver can use. [1]
- Teach-back completed for new or changed medicines. [34]
- Supply and dosing tools arranged. [35]
- Medical-home or primary team informed with timed follow-up when regimens are complex. [3]
If a critical home medicine remains uncertain and the child needs it, keep the child in a supervised setting until the BPMH is good enough or a safe interim plan is explicit. [16] [13]
For CMC polypharmacy, success looks like fewer preventable adverse drug events, clearer indications, reduced burden and better family confidence—not a trophy for the lowest tablet count. [6] [27]
Special Populations
Neonates and infants. Liquids, weight changes and off-label use dominate. Re-check doses when weight moves. [34]
Toddlers and preschoolers. Highest home liquid-error risk; antipyretic duplication is common. [34] [35]
School-age children. Capture school-nurse schedules and after-school carers. [3]
Adolescents. Private history for self-medication, contraception, mental-health medicines and adherence. Transition planning must transfer the regimen, not only the diagnosis list. [15]
Children with medical complexity and technology dependence. Highest polypharmacy and discrepancy stakes; build pharmacist and care-coordination support into the model. [6] [7] [30] [31]
Disability and neurodiversity. Adapt communication and administration supports; do not equate non-standard communication with non-adherence. [28]
Immunocompromised children. Omission of critical therapy is an emergency pathway. [16]
Indigenous families. Culturally safe counselling, community pharmacy access and trust affect whether the list is shared honestly. [7]
Migrant and refugee families. Overseas product names, interrupted records and interpreter needs are expected, not rare. [34]
Out-of-home care. Discontinuous prescribers make pharmacy and hospital record retrieval essential. [3]
Socioeconomic disadvantage. Cost-related non-adherence and supply gaps can look like list errors until you ask. [28]
Evidence, Guidelines & Regional Differences
Paediatric transition evidence. Huynh and colleagues synthesised and studied medication discrepancies in children at hospital transitions, supporting medicines reconciliation as a paediatric safety process rather than an adult-only import. Coffey documented clinically important admission discrepancies in children. Discharge and transfer studies continue to show residual mismatches. [18] [17] [25] [12] [10] [29]
Adult landmark studies still teach mechanism. Cornish and Tam established how often admission medication histories are wrong and how often errors matter. Transfer the method, not adult percentages as paediatric constants. [21] [22]
Systematic reviews of reconciliation programmes. Kwan and Mueller show reconciliation is a key safety strategy with strongest effects on discrepancy reduction; design and implementation quality matter. [23] [24]
Paediatric QI and complex care. ED standardisation, ward accuracy projects, neurology discharge work and pharmacist pilots show local improvement is possible. Feinstein, Huth, Grossberg and Reedy frame CMC polypharmacy as a core safety and coordination problem. [2] [5] [33] [26] [6] [7] [27] [28]
Home dosing science. Yin and colleagues provide randomised and policy-facing evidence that units, tools and pictograms change parental liquid-dosing errors. [34] [35] [36]
Handoff communication. Starmer’s multicentre handoff programme reduced medical errors; use it to justify explicit medication-change communication, not to claim I-PASS replaces reconciliation. [11]
ACSQHC Medication Safety Standard expects systems for medication history, reconciliation, high-risk medicines and patient information. Local hospitals operationalise BPMH with pharmacy partnership; name the principle rather than inventing one hospital’s form as national law. Culturally safe counselling and primary-care enrolment support informational continuity of medicines. [1] [3]
NICE medicines optimisation guidance supports medicines reconciliation at transfers of care and structured medication reviews. Paediatric deprescribing is recognised as needed but practically difficult; exam answers should include shared decision-making and specialist liaison where relevant. [14]
Joint Commission National Patient Safety Goals and AAP patient-safety principles keep reconciliation on the safety agenda. Medical-home and complex-care programmes are natural homes for ambulatory reconciliation after external specialty care. Canadian complex-care and pharmacist models emphasise coordinated transitions for CMC. [3] [6] [31]
Global WHO High 5s medication-reconciliation thinking and ISMP high-alert lists supply shared vocabulary; still adapt to local paediatric formularies and devices. [1] [23]
Exam Pearls
- Say the sequence aloud: sources → BPMH → compare → classify → fix → teach → hand off. [1]
- Unintentional omission of critical chronic therapy is an emergency risk, not paperwork. [13] [16]
- Always capture liquid concentration and the measuring device. [34] [36]
- Discharge is a procedure: temporary medicines must not travel home by accident. [12] [4]
- Polypharmacy in CMC needs indication review and burden reduction, not moral panic about drug count. [6] [27]
- Language discordance requires a professional interpreter for medication counselling. [34]
- Handoffs must state medication changes explicitly. [11]
- Deprescribe with a monitoring plan and family partnership. [14]
- If the child is sick now, resuscitate first; then repair the list. [16]
- A list no caregiver can execute is still unsafe. [34] [28]
RECONCILE at the bedside
References
- [1]Merandi, Jenna Medication Reconciliation. Pediatrics in review, 2017.PMID 28044039
- [2]Sheth, Sarika Standardizing Medication Reconciliation in a Pediatric Emergency Department. Pediatrics, 2024.PMID 38273780
- [3]Condren, Michelle Medication Reconciliation Across Care Transitions in the Pediatric Medical Home. Joint Commission journal on quality and patient safety, 2019.PMID 30898508
- [4]Morse, Keith E Quantifying Discharge Medication Reconciliation Errors at 2 Pediatric Hospitals. Pediatric quality & safety, 2021.PMID 34345749
- [5]Gunkelman, Samantha M Improving Accuracy of Medication Reconciliation for Hospitalized Children: A Quality Project. Hospital pediatrics, 2024.PMID 38529561
- [6]Feinstein, James A Making Polypharmacy Safer for Children with Medical Complexity. The Journal of pediatrics, 2023.PMID 36252865
- [7]Huth, Kathleen Medication safety for children with medical complexity. Paediatrics & child health, 2020.PMID 33178368
- [8]Zanin, Anna Polypharmacy in Children with Medical Complexity: A Cross-Sectional Study in a Pediatric Palliative Care Center. Children (Basel, Switzerland), 2024.PMID 39062270
- [9]Alqenae, Fatema A Prevalence and Nature of Medication Errors and Medication-Related Harm Following Discharge from Hospital to Community Settings: A Systematic Review. Drug safety, 2020.PMID 32125666
- [10]Aires-Moreno, Giulyane Targino Medication discrepancies in transition of care of hospitalised children in Brazil: a multicentric study. Archives of disease in childhood, 2021.PMID 33958348
- [11]Starmer, Amy J Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [12]Gattari, Theresa B Medication Discrepancies at Pediatric Hospital Discharge. Hospital pediatrics, 2015.PMID 26231634
- [13]Louiselle, Katie Medication Discrepancy Risk Factors for Pediatric Patients With Epilepsy at Hospital Admission. The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG, 2021.PMID 34035684
- [14]Moss, James G Paediatric polypharmacy and deprescribing: the views of UK healthcare professionals. Archives of disease in childhood, 2023.PMID 35701176
- [15]Zito, Julie M Psychotropic Polypharmacy in the US Pediatric Population: A Methodologic Critique and Commentary. Frontiers in psychiatry, 2021.PMID 34194346
- [16]DeCourcey, Danielle D Medication Reconciliation Failures in Children and Young Adults With Chronic Disease During Intensive and Intermediate Care. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2017.PMID 28198758
- [17]Huynh, Chi An evaluation of the epidemiology of medication discrepancies and clinical significance of medicines reconciliation in children admitted to hospital. Archives of disease in childhood, 2016.PMID 26566687
- [18]Huynh, Chi Medication discrepancies at transitions in pediatrics: a review of the literature. Paediatric drugs, 2013.PMID 23670796
- [19]Huynh, Chi An evaluation of paediatric medicines reconciliation at hospital discharge into the community. The International journal of pharmacy practice, 2016.PMID 26670624
- [20]Wong, Jacqueline D Medication reconciliation at hospital discharge: evaluating discrepancies. The Annals of pharmacotherapy, 2008.PMID 18780806
- [21]Cornish, Patricia L Unintended medication discrepancies at the time of hospital admission. Archives of internal medicine, 2005.PMID 15738372
- [22]Tam, Vincent C Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 2005.PMID 16129874
- [23]Kwan, Janice L Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Annals of internal medicine, 2013.PMID 23460096
- [24]Mueller, Stephanie K Hospital-based medication reconciliation practices: a systematic review. Archives of internal medicine, 2012.PMID 22733210
- [25]Coffey, Maitreya Prevalence and clinical significance of medication discrepancies at pediatric hospital admission. Academic pediatrics, 2009.PMID 19640822
- [26]Kulawiak, Jessica Evaluation of a Pharmacist-Driven Discharge Medication Reconciliation Service Pilot at a Children's Hospital. The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG, 2024.PMID 39411418
- [27]Grossberg, Richard Polypharmacy-An Important Contributor to Health and Safety for Children With Medical Complexity: How Can We Improve Care for This Vulnerable Population? The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG, 2024.PMID 38596412
- [28]Reedy, Julia Challenges of managing pediatric polypharmacy in a pediatric complex care program: A qualitative pilot study. Journal of the American Pharmacists Association : JAPhA, 2025.PMID 40127839
- [29]Alcântara, Thaciana Dos Santos Prevalence of medication discrepancies in pediatric patients transferred between hospital wards. International journal of clinical pharmacy, 2021.PMID 33175294
- [30]Kuo, Dennis Z Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [31]Kuo, Dennis Z Care Coordination for Children With Medical Complexity: Whose Care Is It, Anyway? Pediatrics, 2018.PMID 29496973
- [32]Zennaro, Margherita Improving Medication Safety Through Medication Reconciliation in Pediatric Neurology: Clinical Pharmacist Recommendations and Physician Uptake in a 13-Week Study. Children (Basel, Switzerland), 2025.PMID 40426804
- [33]Adducchio, Sara Reducing Discharge Medication Reconciliation Errors at a Pediatric Neurology Inpatient Unit. Neurology. Clinical practice, 2024.PMID 38524835
- [34]Yin, H Shonna Preventing Home Medication Administration Errors. Pediatrics, 2021.PMID 34851406
- [35]Yin, H Shonna Pictograms, Units and Dosing Tools, and Parent Medication Errors: A Randomized Study. Pediatrics, 2017.PMID 28759396
- [36]Yin, H Shonna Effect of Medication Label Units of Measure on Parent Choice of Dosing Tool: A Randomized Experiment. Academic pediatrics, 2016.PMID 27155289