Paeds · clinical-assessment-and-reasoning
Multimorbidity and diagnostic overshadowing in children
Also known as Paediatric multimorbidity · Childhood multimorbidity · Diagnostic overshadowing · Physical-mental multimorbidity · Co-occurring conditions · Polypharmacy and multimorbidity · Second diagnosis missed
Fellowship approach to paediatric multimorbidity and diagnostic overshadowing: definitions versus comorbidity and CMC, physical-mental co-occurrence, cognitive traps that hide second diagnoses, baseline-aware assessment, polypharmacy safety, pain and behaviour as medical data, residual-risk communication and exam-ready reasoning.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a 9-year-old with cerebral palsy, epilepsy, gastrostomy feeds and constipation. Tonight the usual carer says she is quieter, biting her hand and not smiling. A junior note reads “behavioural — known disability.” That sentence can delay the search for tooth pain, urinary retention, shunt failure or a new infection. The clinical job is not to ignore the known diagnoses. The job is to hold them and still ask what else is new. [1] [13] [24]
Multimorbidity means two or more chronic conditions coexist in one child. No single “index disease” is required for the definition. That framing differs from comorbidity, which usually means a secondary condition attached to one primary disease. Both words appear in papers. At the bedside, use multimorbidity when several active problems share ownership of the child’s risk. [6] [7]
Diagnostic overshadowing is the cognitive error first framed experimentally by Reiss and colleagues: the presence of intellectual disability reduces the likelihood that clinicians will diagnose a coexisting emotional or behavioural disorder. Later work extended the idea beyond psychiatry. Any strong label — autism, “complex child,” “baseline seizures,” “always chesty” — can hide a second treatable process. Jopp reviewed the construct. Dell’Armo’s systematic review and later experimental work show the bias remains relevant for psychological disorders in people with intellectual disability. [1] [2] [3] [4]
Children with medical complexity (CMC) are a related but narrower population. Cohen’s domains combine chronic conditions, functional limits, high health-care use and family-identified needs. Kuo’s AAP report turns that into recognition and management work. Many CMC children have multimorbidity. Not every multimorbid child meets CMC criteria. Atopic multimorbidity (asthma, eczema and allergic rhinitis together) is common and usually not CMC. Keep the frames separate so you choose the right tools. [9] [10]
Write a problem representation the way you would hand over: age; active conditions that matter today; personal baseline; what changed; whether the threat looks like flare, new illness, medicine harm or an overshadowed process; residual risks still open; and what you need next. [14] [21]
Classification
Use the frame that matches the decision you are making. Do not force every multi-condition child into a CMC pathway, and do not call every second diagnosis “comorbidity” if no index disease truly owns the chart. [6] [9]
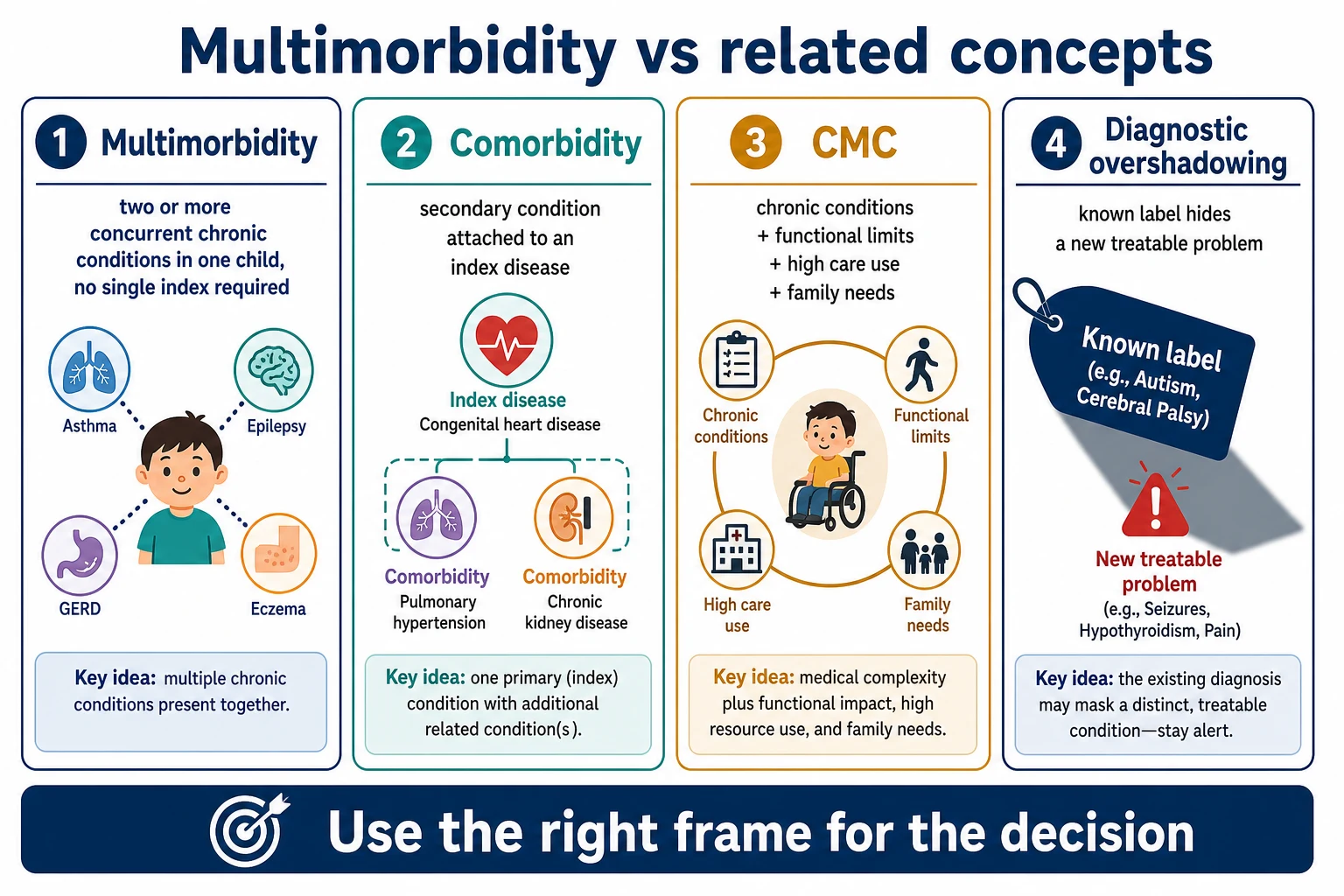
Multimorbidity
Two or more chronic conditions
- No single index required
- Physical, mental or mixed clusters
- Problem list is ranked and active
- Common and complex forms both exist
Comorbidity
Secondary to an index disease
- One disease is primary by framing
- Useful in disease-specific research
- Can understate mutual interactions
- Do not force every chart into this
CMC
Highest-need complex care
- Chronic conditions plus function limits
- High multi-setting care use
- Family-identified service needs
- May include technology dependence
Overshadowing
Reasoning safety trap
- Known label explains too much
- Second diagnosis delayed
- Behaviour blamed on disability
- Needs explicit diagnostic pause
Physical-mental multimorbidity is the co-occurrence of chronic physical and mental health conditions. Romano’s scoping review mapped the paediatric literature. Ferro and colleagues described outpatient prevalence correlates and lower health-related quality of life when both domains are active. Treat mental health as part of the medical problem list, not an optional add-on. [6] [7] [8]
Co-occurrence in autism and intellectual disability is expected, not exceptional. Psychiatric and medical conditions commonly travel with autism spectrum disorder. Structured evaluation reduces masking of mental health conditions in intellectual disability. “Baseline autism” is never a complete medical endpoint for a new change. [3] [5]
Epidemiology & Risk Factors
Childhood multimorbidity is real and heterogeneous. Definitions, age bands and data sources differ across studies, so do not invent a single global prevalence for the viva. A global systematic review of magnitude is one signal that the field is consolidating, not that one cut-off now rules practice. Use local epidemiology carefully and stay honest about uncertainty. [6]
Physical-mental multimorbidity is common enough in paediatric hospital outpatients that generalists will meet it weekly in many services. Correlates cluster around greater health-service use and family strain. Quality of life falls when both physical and mental domains are active. That is a reason to measure function and school participation, not only disease control numbers. [7] [8]
Risk of missed second diagnoses rises with limited communication, multi-specialty fragmentation, long medicine lists, recent hospital contact, language barriers, racism or discrimination, and the cultural habit of treating complexity as “always like this.” Caregiver burden is high in more medically complex households. Cook’s commentary warns that discrimination against children with medical complexity can lower urgency. Mills’ prospective work supports caregiver concern as data linked to critical illness risk — without turning one study into a universal likelihood ratio. [10] [17] [18]
Polypharmacy is both a marker and a driver of harm in multi-condition care. Children and young people with life-limiting conditions often carry long medicine lists. Feinstein and Orth argue for coordinated medication therapy management rather than endless additions. Home administration error risk is high when regimens are complex. [11] [12] [19]
Pathophysiology
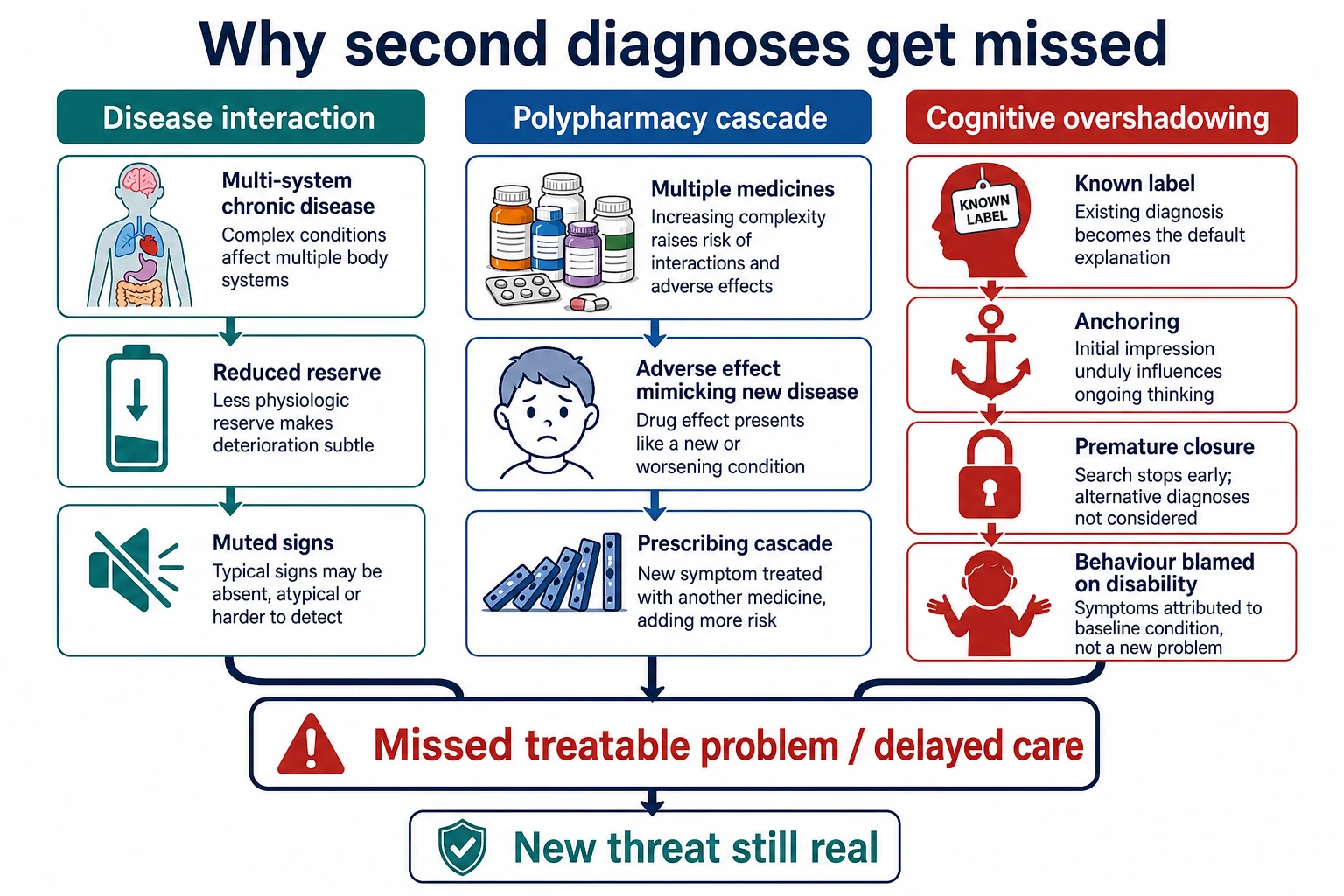
Multimorbidity is not just a list. Interacting diseases change reserve. Chronic lung disease plus weak cough plus reflux raises aspiration risk. Epilepsy medicines plus sedating polypharmacy blunt protective responses. Constipation and urinary retention drive autonomic distress in children with significant neurological impairment. Infection may present with muted fever or only a change in interaction. The physiology can look “soft” while the threat is hard. [10] [13]
Medicines create a second physiology. An anticholinergic load worsens constipation and urinary retention. A new medicine treats the side effect of the last one. That prescribing cascade can mimic new organ disease. Feinstein’s safety agenda is practical: reconcile, review indication, reduce where possible, and teach safe home administration. [11] [19]
The cognitive pathway matters as much as the body pathway. Anchoring on the first label, premature closure after a familiar script, and attributing behaviour to disability all stop the search. Croskerry describes origins of bias and the need for deliberate debiasing. Berkwitt maps common inpatient paediatric traps. Bordini frames paediatric diagnostic error as something teams can interrupt with structured reasoning, not heroics. [14] [15] [16]
Pain physiology is often the missing link. Children with significant central nervous system impairment may not point to a tooth, ear, hip or abdomen. They may self-injure, arch, sweat, sleep poorly or become quieter. Hauer’s AAP clinical report requires clinicians to treat pain assessment as a core skill in this population, not an optional specialty task. Dental and head-and-neck pain can present as self-injury when the label “behaviour” wins too early. [13] [24]
Neuroregression and catatonia can be misread as baseline developmental difference. Case-based teaching shows autism labels can delay recognition of progressive neurological disease, and developmental diagnoses can delay recognition of paediatric catatonia. Those are not rare-exam curiosities. They are high-harm overshadowing patterns. [22] [23]
Clinical Presentation
Multimorbid children present everywhere: clinic, school health rooms, ED, wards, telehealth and home-care escalation. The earliest useful signal is often change from personal baseline, not a dramatic new number. Caregivers may say the child is less interactive, secretions smell different, seizures cluster, hand-biting is new, or sleep has collapsed. Write those words into the note. [10] [17]
Age changes the cluster. Infants may show feeding intolerance, poor weight gain and evolving atopic multimorbidity. Toddlers show behaviour and sleep as main languages of pain. School-age children may present with school refusal layered on chronic disease and anxiety. Adolescents add mood disorders, adherence conflict, risk behaviours and transition gaps while still carrying childhood chronic disease. [6] [7]
Return visits after a single-label discharge are high-risk presentations. “Still viral,” “still behavioural,” or “known complex” after an unplanned return should force a rewrite of the problem representation, not a copy-paste of yesterday’s plan. [14] [15]
Differential Diagnosis
When a multimorbid child looks worse, sort by immediate threat and reversibility, not by which specialty owns the last letter. [14] [15]
- Flare of known disease: genuine asthma exacerbation, breakthrough seizures, inflammatory flare — still confirm, still look for triggers. [10]
- New intercurrent illness: sepsis, pneumonia, urinary infection, viral illness with decompensation. [10]
- Medicine harm: toxicity, withdrawal, interaction, dosing error at home. [11] [19]
- Overshadowed second process: pain, constipation, dental disease, shunt failure, neuroregression, catatonia, safeguarding injury, endocrine crisis. [13] [22] [23] [24]
“Behavioural” and “baseline disability” are unsafe endpoints until reversible medical drivers have been considered in proportion to risk. “Likely viral” can remain a working label only if residual risks stay explicit. [1] [14]
Clinical & Bedside Assessment
Establish baseline before you interpret the now. Ask about usual interaction, communication method, seizure pattern, feeds, stool and urine, pain behaviours, school function and the emergency plan. Compare today’s findings with that baseline, not only with age-based charts. [10] [13]
History must cover the full active problem list, every medicine with dose and recent changes, complementary products, recent procedures, missed doses, and the caregiver’s exact concern. Use a professional interpreter when language access is needed. Do not default to a sibling as interpreter for critical decisions. [10] [19]
Examine with dignity and adapted communication. Look for dental disease, ear disease, abdomen, hips, skin, constipation signs, urinary retention clues, device sites and neurological change from baseline. For children with significant CNS impairment, use a structured pain approach rather than waiting for a self-report that cannot come. [13] [24]
Insert a diagnostic pause when the chart is tempting: What else could this be? What would change my mind? Who else should look? What residual risk must stay open if I act on the leading label? That is bedside debiasing, not academic theatre. [14] [16] [21]
Investigations
Order tests that answer a hypothesis or protect against a high-harm miss. Do not order sprawling panels to soothe anxiety after the reasoning has already closed. First-line choices often include glucose, blood gas when respiratory or perfusion threat is plausible, electrolytes with polypharmacy, targeted cultures, and imaging only when it changes immediate management or destination. [14]
Interpret results against the child’s chronic baseline and medicines. A “normal for age” sodium may not be normal for this child on multiple CNS-active drugs. A normal inflammatory marker does not erase caregiver concern or progressive clinical change. Structured mental-health or developmental evaluation can unmask co-occurring psychiatric disease that a rushed medical visit misses. [5] [11]
Low-value testing includes indiscriminate panels with no linked hypothesis, repeated imaging that will not change care, and investigations that require unsafe transfers without stabilisation. Name the question each test is meant to answer. [14]
Management — Resuscitation
If the child is deteriorating, treat airway, breathing and circulation threats first. Do not let a long problem list delay oxygen, glucose check, seizure care or sepsis pathways. Use the emergency care plan when one exists. Compare with personal baseline while you act. [10] [17]
Caregiver concern that the child is critically different should raise urgency even when first numbers look near baseline. Escalate through local MET or senior routes when complexity is delaying recognition. Complexity is context. It is not a diagnosis of reassurance. [17] [18]
Management — Definitive & Stepwise
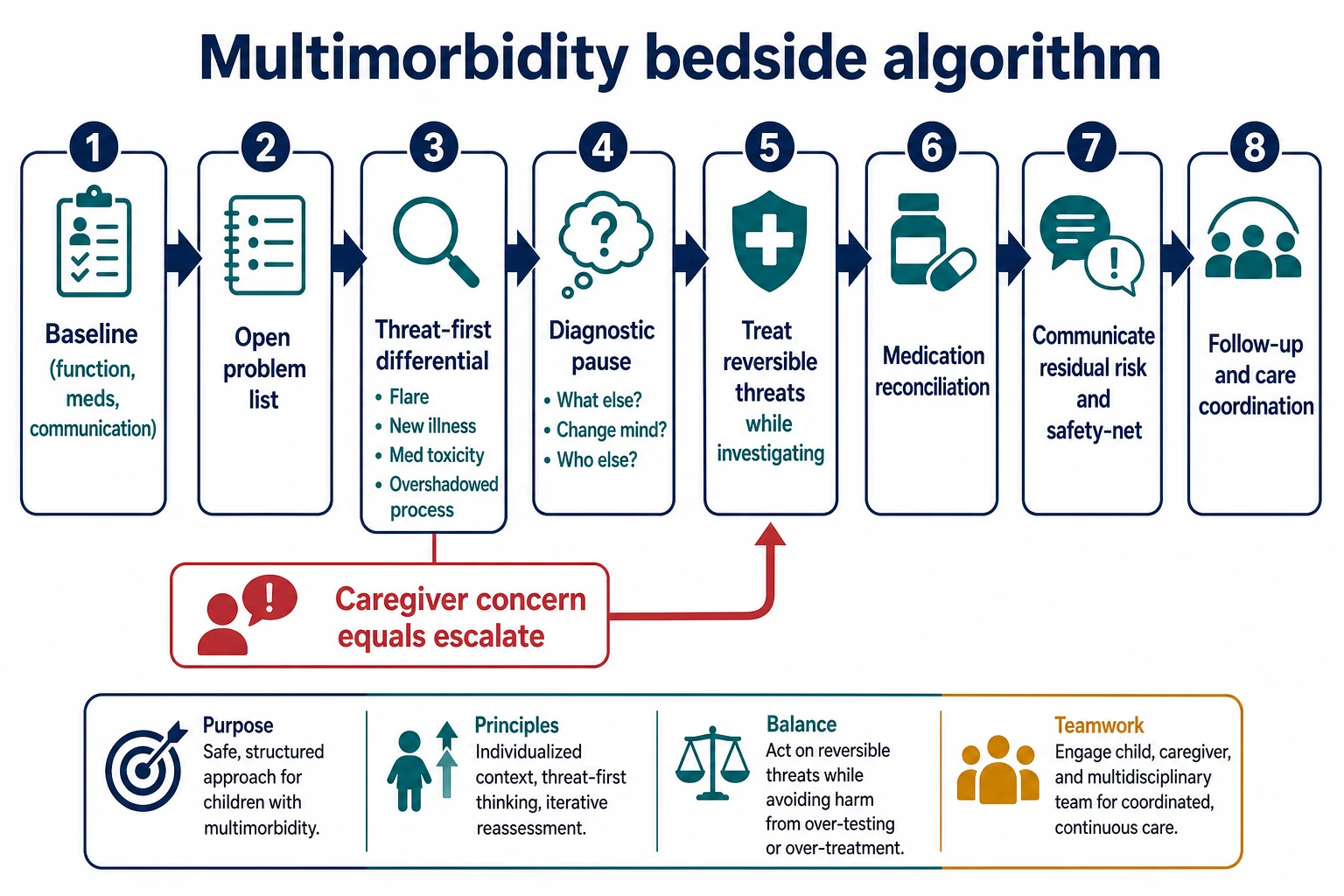
- Baseline. Function, communication, usual observations, devices, emergency plan. [10]
- Open problem list. Rank active issues. Retire historical codes that no longer drive risk. [9] [21]
- Threat-first differential. Flare versus new illness versus medicine harm versus overshadowed process. [14] [15]
- Diagnostic pause. What else, what would change my mind, who else looks. [16]
- Treat and test in parallel. Reverse immediate threats while the differential stays flexible. [14]
- Medication reconciliation. Indication, dose, interaction, deprescribe when safe, teach home administration. [11] [12] [19]
- Communicate residual risk. Say the leading working diagnosis and what remains protected against. [14] [20]
- Follow-up and coordination. Name owners, review times, school or community actions, and re-presentation criteria. [10] [20]
Structured handover preserves open residual risks. Starmer’s handoff programme evidence supports system-level attention to information transfer. A multimorbid handover that says only “stable complex child” is incomplete. [20]
Specific Subtypes & Scenarios
Nonverbal child with new self-injury. Search for pain: dental, ENT, abdomen, constipation, fracture, device site. Behaviour support still matters, but medicine comes first when change is acute. [13] [24]
Autistic adolescent with escalating aggression. Hold medical illness, sensory overload, medication effect, anxiety or mood disorder, and environment in parallel. Co-occurrence is expected. [5]
“Usual chestiness” in neurodisability. Ask what is different this time. Consider aspiration pattern change, infection, secretion burden and fatigue. [10]
Neuroregression labelled as autism. Look for loss of skills, new neurology and progressive clues. Do not freeze the developmental label against new data. [23]
Possible paediatric catatonia. Reduced movement, mutism or autonomic signs in a child with a developmental diagnosis need specific recognition, not only “behaviour.” [22]
Polypharmacy toxicity versus new organ disease. Reconcile first. Compare timing of medicine changes with symptom onset. [11]
Physical-mental multimorbidity clinic visit. Measure quality of life and school function. Treat both domains as active medical work. [7] [8]
Transition-age fragmentation. Adult services may split the problem list by organ. Your job is to transfer the whole child, open risks and medicine map. [10]
Complications & Pitfalls
The headline pitfall is delayed recognition of a treatable second disease because the first label felt sufficient. Related failures include anchoring on the first specialty letter, prescribing cascades, ignoring caregiver expertise, safeguarding blindness, and lower urgency because staff treat the child as “always complex.” Handover that closes residual risk multiplies all of the above across shifts. [14] [15] [18] [20]
Prognosis & Disposition
Outcomes that matter include function, school participation, quality of life, family wellbeing and unplanned care — not survival alone. Physical-mental multimorbidity is linked with poorer quality of life than physical disease alone in comparative work. Disposition should match residual risk: home with clear safety-net, ward observation, mental-health pathway, HDU/ICU or retrieval. [8] [10]
Safety-net advice must name residual risks. “Come back if not themselves, if pain behaviours worsen, if breathing changes, if medicines cannot be given, or if you are more worried” is more useful than a single closed label. Follow-up intensity should reflect polypharmacy, recent changes and coordination gaps. [11] [17]
Special Populations
Neonates and infants may enter multimorbidity through congenital multi-system disease or early technology dependence. Children with intellectual disability or limited communication need baseline-aware exam and pain search skills. Autistic children need co-occurrence literacy. CMC and technology-dependent children need device-aware differentials without collapsing every symptom into complexity. Indigenous, migrant and refugee families need culturally safe care and professional interpreters. Out-of-home care and youth justice settings often hold fragmented histories. Adolescents need confidential mental-health enquiry and transition planning. Socioeconomic disadvantage multiplies missed follow-up and medicine error risk. [6] [10] [13] [19]
Evidence, Guidelines & Regional Differences
Anchor overshadowing in Reiss 1982, Jopp’s review, and Dell’Armo’s contemporary synthesis and experimental work. Anchor physical-mental multimorbidity in Romano and Ferro. Anchor polypharmacy safety in Feinstein, Orth’s pMTM programme design, and AAP home medication safety. Anchor pain assessment in Hauer’s AAP clinical report. Use Bordini, Berkwitt and Croskerry for diagnostic-error teaching without claiming paediatric trial proof for every bias name. [1] [3] [6] [11] [13] [14]
Regionally, ANZ practice sits in complex-care clinics, retrieval networks and disability support interfaces that vary by jurisdiction — do not invent eligibility rules. The UK has integrated-care guidance for disabled children and young people with severe complex needs (NICE NG213) as system context. US practice is shaped by AAP medical-home and CMC reports. Canadian services contribute much of the paediatric physical-mental multimorbidity research base. Bedside anti-overshadowing rules travel better than funding packages. [10]
ANZ: Use local complex-care and retrieval pathways; keep NDIS or disability-support detail jurisdiction-named and verified. UK: NICE NG213 is system organisation guidance, not a bedside score. US/Canada: Medical-home and CMC reports guide models; Ferro/Romano inform physical-mental multimorbidity teaching. Everywhere: residual-risk communication and medicine reconciliation remain universal safety moves. [10] [11]
Exam Pearls
- Multimorbidity = two or more concurrent chronic conditions; comorbidity usually implies an index disease. [6]
- Diagnostic overshadowing = known label reduces recognition of a second condition. Give a paediatric example every time. [1] [3]
- Problem representation must include baseline, new change and residual risk. [21]
- Behaviour change in limited communication is a medical presentation until proven otherwise. [13] [24]
- Polypharmacy safety: reconcile, review indication, deprescribe when safe, teach home administration. [11] [19]
- Caregiver concern is data. Discrimination that lowers urgency is a safety failure. [17] [18]
- Handover must carry open residual risks, not only the leading label. [20]
References
- [1]Reiss, S Emotional disturbance and mental retardation: diagnostic overshadowing. American journal of mental deficiency, 1982.PMID 7102729
- [2]Jopp, DA Diagnostic overshadowing reviewed and reconsidered. American journal of mental retardation : AJMR, 2001.PMID 11531461
- [3]Dell'Armo, K Diagnostic Overshadowing of Psychological Disorders in People With Intellectual Disability: A Systematic Review. American journal on intellectual and developmental disabilities, 2024.PMID 38411245
- [4]Dell'Armo, K How intellectual disability may bias psychologists' clinical impressions: An examination of diagnostic overshadowing. Psychological assessment, 2025.PMID 40167540
- [5]Manohar, H Diagnostic Masking and Overshadowing in Intellectual Disability-How Structured Evaluation Helps. Journal of child and adolescent psychiatric nursing, 2016.PMID 27901303
- [6]Romano, I Physical-mental multimorbidity in children and youth: a scoping review. BMJ open, 2021.PMID 34016659
- [7]Ferro, MA Prevalence and Correlates of Physical-mental Multimorbidity in Outpatient Children From a Pediatric Hospital in Canada. Canadian journal of psychiatry. Revue canadienne de psychiatrie, 2022.PMID 35060408
- [8]Ferro, MA Health-related quality of life in children with and without physical-mental multimorbidity. Quality of life research, 2021.PMID 34331638
- [9]Cohen, E Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics, 2011.PMID 21339266
- [10]Kuo, DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [11]Feinstein, JA Making Polypharmacy Safer for Children with Medical Complexity. The Journal of pediatrics, 2023.PMID 36252865
- [12]Orth, LE A coordinated approach for managing polypharmacy among children with medical complexity: rationale and design of the Pediatric Medication Therapy Management (pMTM) randomized controlled trial. BMC health services research, 2023.PMID 37120509
- [13]Hauer, J Pain Assessment and Treatment in Children With Significant Impairment of the Central Nervous System. Pediatrics, 2017.PMID 28562301
- [14]Bordini, BJ Overcoming Diagnostic Errors in Medical Practice. The Journal of pediatrics, 2017.PMID 28336147
- [15]Berkwitt, A Cognitive bias in inpatient pediatrics. Hospital pediatrics, 2014.PMID 24785565
- [16]Croskerry, P Cognitive debiasing 1: origins of bias and theory of debiasing. BMJ quality & safety, 2013.PMID 23882089
- [17]Mills, E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [18]Cook, S Discriminating Against Children With Medical Complexity. Pediatrics, 2023.PMID 37357723
- [19]Yin, HS Preventing Home Medication Administration Errors. Pediatrics, 2021.PMID 34851406
- [20]Starmer, AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [21]Bowen, JL Educational strategies to promote clinical diagnostic reasoning. The New England journal of medicine, 2006.PMID 17124019
- [22]Reinfeld, S Diagnostic overshadowing clouding the efficient recognition of pediatric catatonia: a case series. CNS spectrums, 2023.PMID 36440510
- [23]Loo, KK Diagnostic Overshadowing: Insidious Neuroregression Mimicking Presentation of Autism Spectrum Disorder. Journal of developmental and behavioral pediatrics : JDBP, 2022.PMID 35943376
- [24]Yekezare, M Diagnostic overshadowing: self-injurious behaviour as a manifestation of pain in the head and neck. British dental journal, 2024.PMID 38877248