Paeds · clinical-assessment-and-reasoning
Oedema in children: diagnostic approach
Also known as Edema in children · Anasarca · Peripheral oedema paediatric · Generalised oedema child · Periorbital oedema
Fellowship diagnostic approach to paediatric oedema: pattern and mechanism classification, threat-first assessment, nephrotic versus nephritic versus cardiac versus nutritional and angioedema pathways, investigation gates, stabilisation without blind diuresis, and exam-ready communication.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A parent brings a three-year-old because “his eyes are puffy every morning and his shoes feel tight.” The child looks well, plays, and has no fever. That scene is common. It can still be nephrotic syndrome. It can also be allergy, crying, or nothing serious. Your job is to sort threat, pattern and mechanism before you order a long panel or send everyone home reassured. [1] [7] [8]
US sources usually write edema. UK, Australian and many exam stems write oedema. Use the spelling your board expects, but define the same clinical problem: excess interstitial fluid that pits or expands soft tissues beyond normal age-related fullness. [1]
S.W.E.L.L.
Overview & Definition
Oedema means fluid has left the vascular space and settled in tissues. You see it as periorbital puffiness, pretibial swelling, sacral fluid in a bedbound child, ascites, or whole-body anasarca. The word does not tell you why. Nephrotic hypoalbuminaemia, heart failure, post-streptococcal nephritis, severe malnutrition, protein-losing enteropathy, sepsis-related leak and angioedema can all look swollen. [1] [2] [9]
Fellowship answers start with a problem representation, not a disease name: “Acute generalised pitting oedema in a preschool child with heavy proteinuria and normal blood pressure — nephrotic pattern until proven otherwise.” That sentence already steers tests and safety-netting. [3] [6] [8]
Local swelling from cellulitis, insect bite, trauma or osteomyelitis is not systemic oedema. Unilateral red, hot, tender limb needs an infection/trauma pathway, not a nephrotic panel first. Soft tissue “chubbiness” in infants is also not oedema if it does not pit and the child is thriving. [1]
Classification
Think in two layers at once: distribution/severity and mechanism. [1]
Distribution answers: where is the fluid? Periorbital and dependent leg oedema are classic early nephrotic clues. Generalised anasarca means a large fluid shift. Unilateral limb swelling points to local causes. Facial and tongue swelling with itch or airway noise points to angioedema, not dependent hydrostatic oedema. [1] [11]
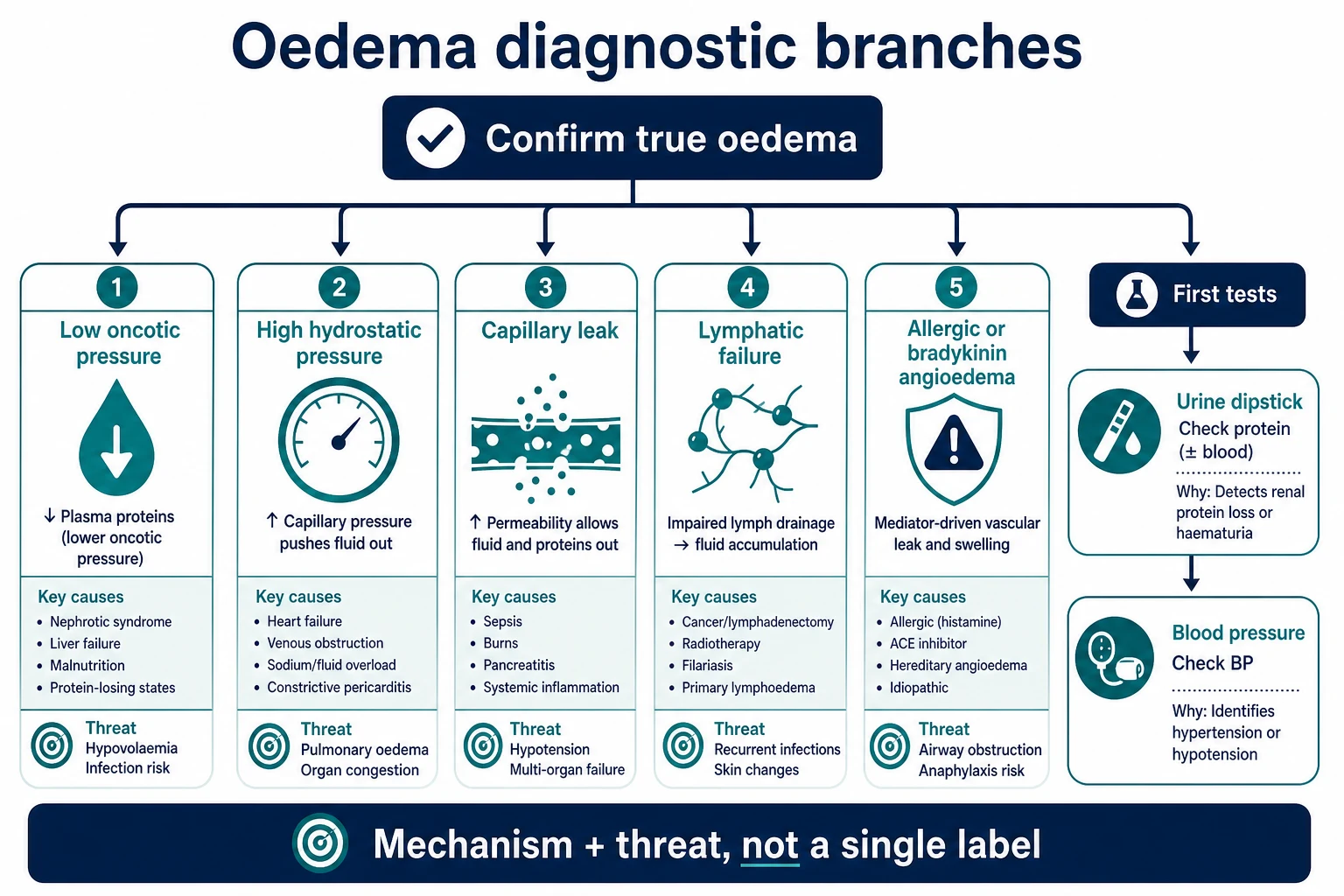
Mechanism answers: which Starling or lymphatic failure produced it? [1] [2]
- Low oncotic pressure — low plasma proteins (nephrotic syndrome, hepatic synthetic failure, malnutrition, protein-losing states).
- High hydrostatic pressure — heart failure, venous obstruction, fluid overload.
- Capillary leak — sepsis, burns, idiopathic systemic capillary leak.
- Lymphatic failure — primary lymphoedema, lymphatic anomalies, Fontan-related lymphatic failure.
- Mediator-driven angioedema — histamine (allergic) or bradykinin (hereditary angioedema, some drug reactions). [1] [2] [11] [15] [17]
Pitting favours free interstitial fluid from oncotic or hydrostatic causes. Non-pitting chronic limb swelling raises lymphatic disease. Acute non-pitting facial swelling with urticaria favours allergic angioedema; recurrent non-urticarial attacks with family history favour hereditary angioedema. [11] [12]
Epidemiology & Risk Factors
Idiopathic nephrotic syndrome is a leading cause of new generalised oedema in preschool and early school-age children in many high-resource clinics. Most first presentations of steroid-sensitive disease cluster in this band; IPNA recommendations frame diagnosis and first management for that group. [3] [6] [7]
Acute post-streptococcal glomerulonephritis (APSGN) still matters where group A streptococcal skin and throat disease is common. Australian primary-care refreshers and treatment-standard reviews remind clinicians that oedema with dark urine and hypertension after infection is a public-health as well as bedside problem. [9] [10]
Cardiac oedema risk rises with congenital heart disease, myocarditis and single-ventricle/Fontan physiology. Fontan-associated protein-losing enteropathy (PLE) creates chronic hypoalbuminaemic oedema years after palliative surgery. [13] [14] [16]
Nutritional oedema appears where severe acute malnutrition is prevalent. It can coexist with diarrhoea and infection, so fluid decisions are protocolised and not improvised. [18]
Allergy and hereditary angioedema are less common than nephrotic disease for generalised pitting oedema, but they dominate the airway-threat pathway. Family history, recurrent non-urticarial attacks and early onset change the pre-test probability of HAE. [11] [12]
Pathophysiology
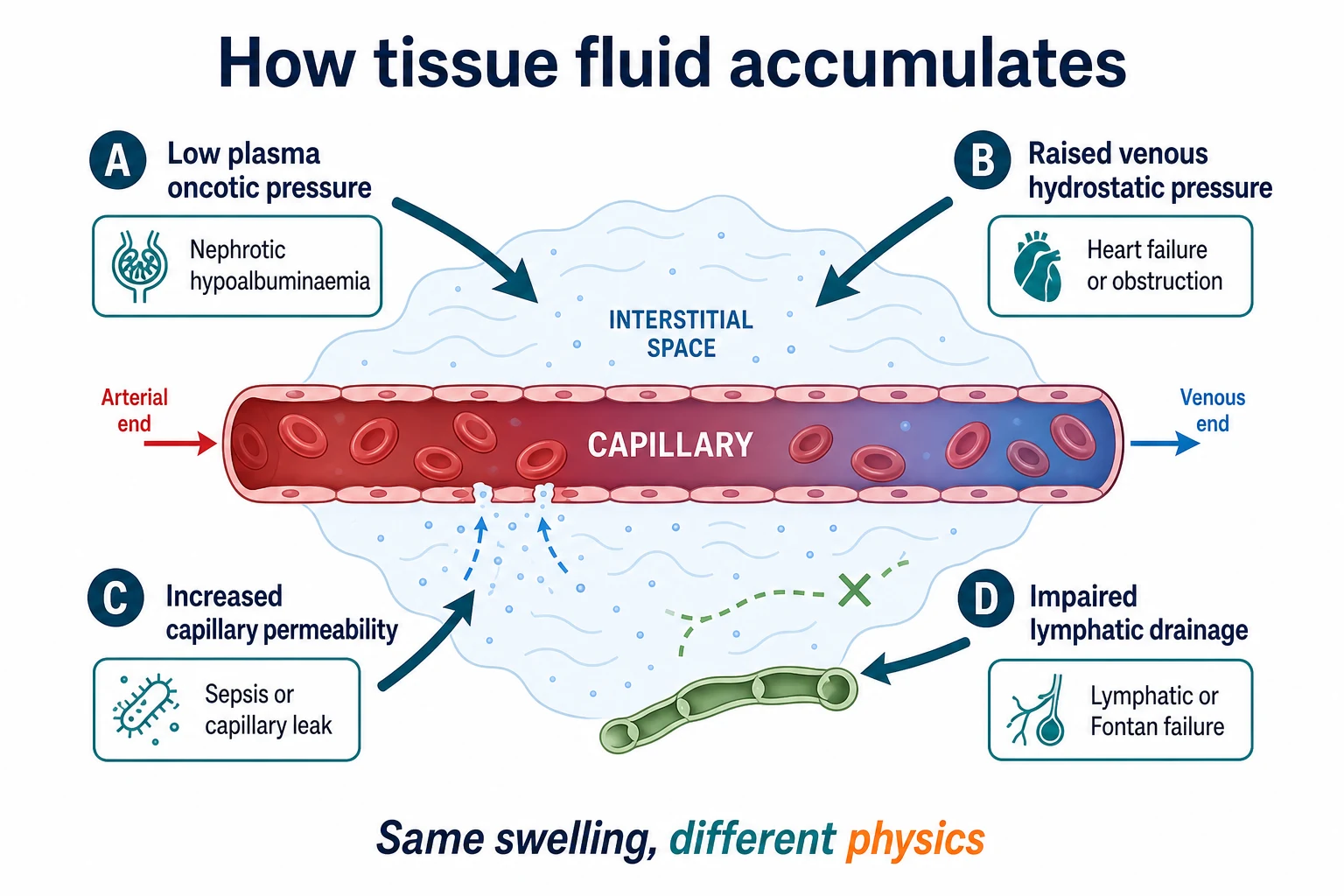
Fluid stays in vessels when the balance of hydrostatic push, oncotic pull, vessel leakiness and lymphatic clearance is intact. Break any limb of that balance and interstitium fills. [1] [2]
In nephrotic syndrome, heavy urinary protein loss lowers plasma oncotic pressure. Sodium retention and underfill versus overfill physiology refine why some children look volume-down despite swollen tissues. Ellis and Siddall review these pathways for childhood nephrotic oedema: the tissues are full, but intravascular volume may still be precarious. That is why blind loop diuretics can harm. [1] [2]
In heart failure and venous obstruction, capillary hydrostatic pressure rises. Fluid is pushed out, often into dependent sites and the liver capsule. Lymphatic overload in heart failure further impairs clearance. [15]
In capillary leak, the barrier itself fails. Protein-rich fluid leaves the vessel. The child can look oedematous while becoming shocked and haemoconcentrated. Idiopathic systemic capillary leak is rare but taught as an under-recognised PICU pattern. [17]
In lymphatic failure, protein-rich fluid cannot return. Fontan circulation is a paediatric prototype: high systemic venous pressure plus lymphatic congestion can produce PLE with oedema and hypoalbuminaemia. [13] [14] [15]
In angioedema, local mediator release increases permeability in deeper tissues. Histamine pathways often include urticaria. Bradykinin pathways (HAE) usually do not. Airway oedema is the life threat, not the ankle circumference. [11] [12]
Clinical Presentation
Caregivers may say “allergy,” “too much salt,” “crying eyes,” or “tight shoes.” Ask what changed, how fast, and whether urine looks frothy or dark. Frothy urine and progressive leg swelling after periorbital puffiness is a classic nephrotic story. Dark cola urine with headache or reduced urine output after a sore throat or impetigo points toward APSGN. [1] [8] [9] [10]
Cardiac presentations often mix oedema with poor feeding, tachypnoea, sweating, hepatomegaly or cool legs. Myocarditis may look like a viral illness that will not settle, with rising work of breathing rather than pure puffy eyes. [16]
Nutritional oedema may show bilateral limb swelling with wasted muscle, skin and hair changes, and recent food insecurity or chronic diarrhoea. Do not assume “just kidneys” in a wasted child. [18]
Angioedema presents with rapid face, lip, tongue or extremity swelling. Itch and hives favour allergy. Recurrent painful non-urticarial attacks, abdominal crises or family history favour HAE. Stridor or voice change is an airway emergency. [11] [12]
Differential Diagnosis
Hold common and dangerous lists together. [1] [7]
Common generalised pitting patterns in well-looking preschoolers: idiopathic nephrotic syndrome. Confirm with heavy proteinuria and hypoalbuminaemia once threat is addressed. [3] [6] [8]
Nephritic patterns: APSGN and other acute glomerulonephritides — oedema plus haematuria, hypertension, oliguria, rising creatinine. [9] [10]
Cardiac: myocarditis, cardiomyopathy, structural heart disease, pericardial constraint. Look for respiratory signs, hepatomegaly and perfusion clues. [16]
Hepatic synthetic failure and protein-losing states: low albumin without heavy urine protein, or with gastrointestinal protein loss. Fontan PLE is the exam classic in complex cardiology graduates. [13] [14]
Malnutrition: oedematous severe acute malnutrition in the right epidemiology. [18]
Allergy/HAE: facial/airway pathway more than dependent anasarca. [11] [12]
Local mimics: cellulitis, trauma, deep vein thrombosis (rare but real in complex/catheterised children), osteomyelitis. [1]
Neonates: hydrops pathways, congenital nephrotic syndrome, congenital heart disease — different urgency and teams. [1] [3]
Age shifts the ranking. Toddler with anasarca and 4+ protein: nephrotic first. School-age after skin infection with hypertension: APSGN first. Fontan adolescent with chronic oedema: PLE and liver/lymphatic complications first. [3] [9] [13]
Clinical & Bedside Assessment
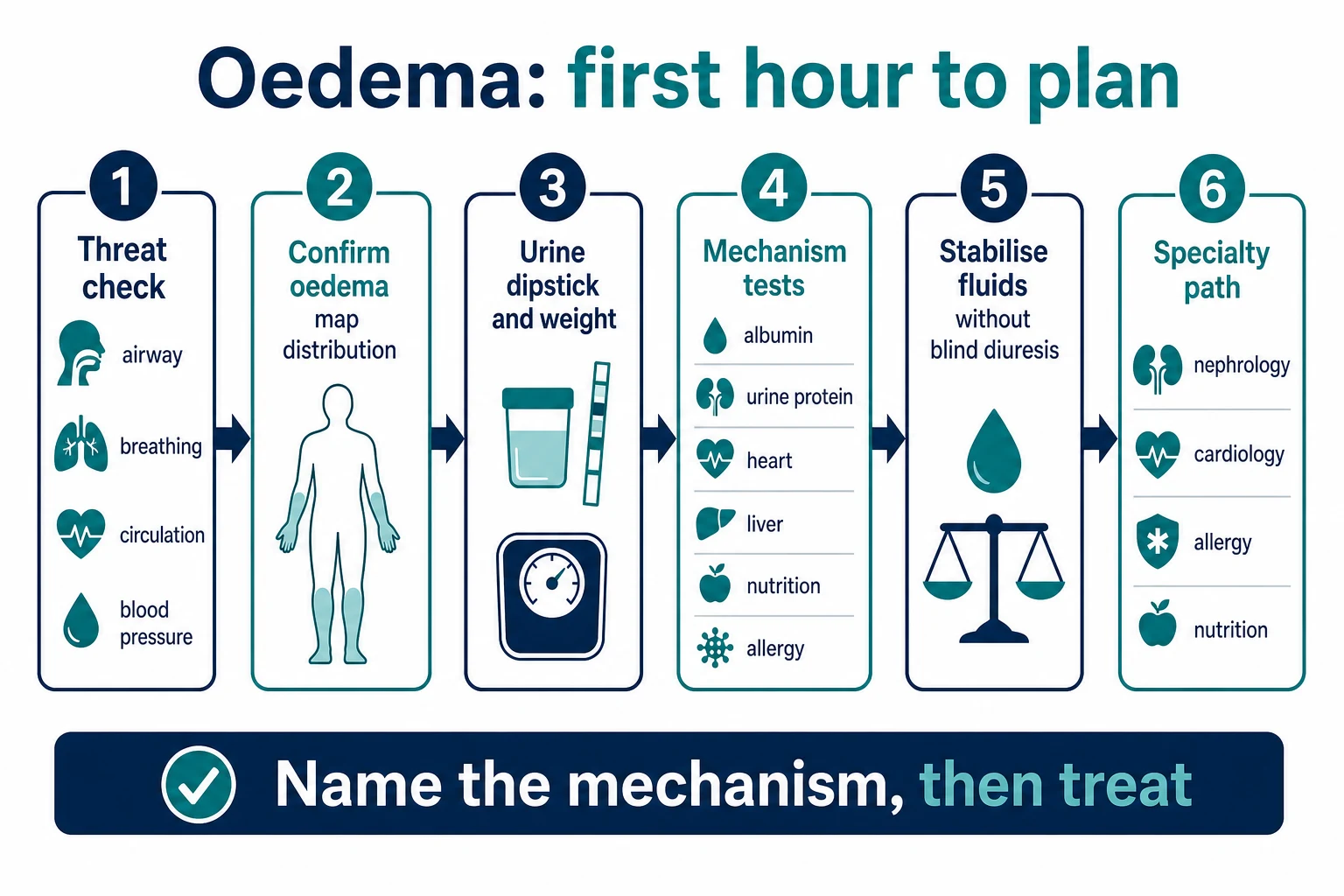
1. Threat first. Airway swelling, stridor, work of breathing, oxygen need, shock, hypertensive emergency and reduced consciousness outrank chart debates. If anaphylaxis criteria are met, treat that pathway immediately. [11] [16]
2. Confirm it is oedema. Press gently over shin, dorsum of foot or sacrum. Map periorbital, limb, sacral, abdominal and genital soft-tissue swelling. Note pitting, tenderness, colour and symmetry. Weigh the child — weight is a fluid vital sign. [1]
3. Blood pressure and urine dipstick early. These two tests split nephritic, nephrotic and many non-renal pathways in minutes. Heavy protein without blood and with normal BP supports nephrotic pattern. Blood and protein with high BP support nephritic pattern. Minimal urine findings push you toward cardiac, hepatic, nutritional, lymphatic or allergic causes. [1] [8] [9]
4. Focused systems exam. Heart rate, pulses, perfusion, precordium, liver edge, respiratory effort, ascites, skin infection, rash, joint swelling and nutritional state. In Fontan or complex cardiac patients, ask about baseline oxygen saturations and stool pattern. [13] [16]
5. History that changes management. Speed of swelling, urine colour/froth, sore throat or impetigo, diarrhoea, poor feeding, orthopnoea, known heart disease, medications (including ACE inhibitors in adolescents/carers’ shared meds), allergen exposures, previous similar episodes, family HAE or early kidney disease, food security. Use a professional interpreter when language discordance exists. [10] [11]
6. Intravascular status. Oedematous tissues do not prove vascular fullness. Look at perfusion, heart rate, mucous membranes, urea/creatinine trend and clinical response. This judgment protects against harmful diuresis. [1] [2]
Investigations
Start with bedside tests that branch care: urine dipstick, BP, weight, SpO2, glucose if unwell. [1] [8]
For generalised oedema with proteinuria, first-line studies usually include serum albumin, electrolytes, creatinine, full blood count, and quantification of proteinuria as locally available. Lipid profile often rises in nephrotic states and supports the pattern. IPNA and KDIGO frameworks define nephrotic-range disease using proteinuria plus hypoalbuminaemia; use the definitions your service and guideline set endorse rather than inventing numbers in a viva. [3] [5] [6] [8]
Add nephritic work-up when haematuria, hypertension or renal impairment dominate: streptococcal serology where relevant, complement levels, and urgent nephrology discussion. [9] [10]
Add cardiac tests when respiratory signs, hepatomegaly, gallop, known heart disease or poor perfusion are present: chest radiograph, ECG, BNP/NT-proBNP if available, and echocardiography. [16]
Add liver and protein-losing tests when albumin is low without heavy urine protein: LFTs, and consider stool alpha-1 antitrypsin and GI review, especially in Fontan circulation. [13] [14]
Add allergy/HAE pathway tests only after acute stabilisation and specialist advice; diagnosis of HAE is not a first-hour dipstick problem, but recognition of the clinical pattern is. [11] [12]
Avoid mega-panels in mild dependent swelling after prolonged immobility with normal exam, normal BP and negative dipstick — reassess and safety-net instead. [1]
Management — Resuscitation
Airway angioedema: call for help, position for airway comfort, give anaphylaxis treatment if criteria are met, and escalate early. HAE attacks need bradykinin-pathway specific therapy according to local/specialty protocols — antihistamine-only strategies fail for true HAE. [11] [12]
Pulmonary oedema or suspected cardiogenic shock: oxygen, senior support, careful fluid policy, and urgent cardiology/ICU pathways. Myocarditis is a clinical diagnosis that needs a high index of suspicion. [16]
Hypertensive emergency with nephritic oedema: controlled BP management and urgent nephrology — this is not “just puffy eyes.” [9]
Suspected capillary leak with shock: treat as critical illness; volume and vasopressor decisions belong in resuscitation systems, not ward diuretic charts. [17]
Nephrotic child with fever or severe abdominal pain: consider spontaneous bacterial peritonitis and other infections; do not delay antimicrobials for endless imaging if sepsis is likely. Thrombosis risk also rises in nephrotic states — report new focal neurology or limb pain urgently. [1] [3] [7]
Management — Definitive & Stepwise
After threat control, write a one-line mechanism and a plan. [1]
Likely first-presentation idiopathic nephrotic syndrome (typical age, heavy protein, low albumin, normal complement pattern as applicable): admit or arrange same-day specialist pathway per local practice; fluid and salt strategy; infection precautions; steroid therapy under IPNA/KDIGO-aligned paediatric nephrology frameworks. Do not invent mg/kg schedules from memory if you cannot cite your local/guideline card — say you will use the current IPNA/KDIGO-aligned protocol. [3] [5] [6] [7]
Nephritic/APSGN pattern: fluid and sodium restriction as indicated, BP control, treat volume complications, search for ongoing infection risks, public-health awareness in high-burden settings, nephrology follow-up. [9] [10]
Cardiac pattern: treat heart failure pathway; avoid pure “renal clinic” framing. [16]
Fontan PLE pattern: joint cardiology–gastroenterology–lymphatic expertise; albumin and oedema are markers of a circuit problem, not a primary kidney disease until proven. [13] [14]
Nutritional oedema: use WHO/local SAM protocols; rehydration and feeding are specialised. Recent trial work continues to refine oral rehydration approaches in malnourished dehydrated children — follow protocolised care rather than improvised ward fluids. [18]
Home plan when discharge is safe: daily weights if appropriate, urine dipstick teaching for nephrotic pathways, clear return triggers (airway swelling, breathing difficulty, fever, abdominal pain, headache/visual change, rapid weight rise, oliguria), written steroid/relapse plans when relevant, and early primary-care follow-up. [3] [7]
Specific Subtypes & Scenarios
Toddler nephrotic pattern. Periorbital then leg oedema, frothy urine, 3–4+ protein, low albumin. Teach infection and thrombosis red flags while starting guideline-aligned care. [1] [3]
APSGN school-age pattern. Recent impetigo or pharyngitis, dark urine, hypertension, mild oedema. Primary care recognition prevents missed hypertensive complications. [9] [10]
Infant cardiac pattern. Sweaty feeds, tachypnoea, hepatomegaly, cool legs — echo pathway, not only urine tests. [16]
Fontan adolescent. Chronic oedema, low albumin, diarrhoea or poor weight — PLE until reconsidered. [13] [14]
Allergic angioedema. Hives, itch, rapid face swelling after exposure — anaphylaxis pathway if systemic features. [11]
HAE. Recurrent non-urticarial attacks, family history, abdominal crises — specialty action plan. [11] [12]
Nutritional oedema. Wasting plus bilateral pitting oedema in high-risk settings — SAM protocol. [18]
Unilateral red limb. Infection/trauma first. [1]
PICU capillary leak. Oedema with shock and haemoconcentration — critical care diagnosis of exclusion after common causes. [17]
Complications & Pitfalls
Calling every puffy face “allergy” misses nephrotic syndrome. Giving large diuretics to an underfilled nephrotic child can precipitate shock. Missing hypertension in APSGN risks encephalopathy. Chasing only kidneys in a tachypnoeic infant misses myocarditis. Ignoring fever in nephrotic oedema misses peritonitis. Forgetting Fontan history misses PLE. Treating HAE as simple allergy fails. Skipping interpreters distorts urine and diet history. [1] [2] [9] [11] [13] [16]
Prognosis & Disposition
Many children with steroid-sensitive nephrotic syndrome remit, but relapses are common — families need a written plan, not false “one-off” reassurance. [3] [7]
APSGN often recovers with supportive care, but severe hypertension and renal complications need active management and follow-up. [9]
Cardiac and Fontan-related oedema prognosis follows the underlying circuit and PLE control. [13] [14]
Discharge only when threat is controlled, mechanism is named or safely narrowed, caregivers can describe return triggers, and follow-up is timed to acuity. [1] [3]
Special Populations
Neonates need perinatal and neonatal nephrology/cardiology frameworks for hydrops and congenital nephrotic disease. [1] [3]
Indigenous and high APSGN-burden communities need culturally safe infection and kidney conversations without stigma; primary-care vigilance matters. [10]
Migrant and refugee families may present late, with dual infection–nutrition risk and language barriers. [10] [18]
Technology-dependent and Fontan patients need their baseline experts early. [13] [14]
Adolescents need adherence support, confidential drug history and transition plans for chronic nephrotic, HAE or Fontan care. [11]
Malnutrition-endemic settings use WHO-framed pathways for oedematous malnutrition. [18]
Evidence, Guidelines & Regional Differences
Ellis (2015) remains a practical pathophysiology and evaluation anchor for childhood nephrotic oedema. Siddall (2012) deepens underfill/overfill thinking. [1] [2]
IPNA steroid-sensitive (2023) and steroid-resistant (2020) recommendations, KDIGO 2021 glomerular guidance, and the KDIGO 2025 nephrotic-in-children executive summary are the major international frames for definitions and care principles. Vasudevan (2026) and Bravo (2026) update bedside nephrotic and proteinuria teaching. [3] [4] [5] [6] [7] [8]
APSGN treatment-standard and Australian primary-care refreshers matter for ANZ exam answers in high-burden contexts. [9] [10]
Paediatric HAE international guidance and clinical yardsticks separate histamine from bradykinin pathways. Fontan PLE and lymphatic heart-failure reviews explain chronic non-nephrotic hypoalbuminaemic oedema. Myocarditis and capillary-leak papers remind you that not all oedema is renal. SAM rehydration research continues to refine malnutrition care — follow protocols. [11] [12] [13] [14] [15] [16] [17] [18]
Regional deltas are mostly epidemiology (APSGN/RHD/SAM), drug access (HAE agents), and referral thresholds — not different physics of oedema. [9] [10] [11] [18]
Exam Pearls
- Urine dipstick and BP in the first five minutes of generalised oedema.
- Morning periorbital puffiness + heavy protein = nephrotic pattern until proven otherwise.
- Nephritic = blood + hypertension + oedema more than pure protein.
- Swollen ≠ intravascularly full.
- Airway swelling is a different algorithm from pretibial pits.
- Fontan + low albumin + oedema → think PLE/lymphatics.
- Do not invent steroid or albumin recipes in a viva; name the guideline framework and local protocol.
- Safety-net fever, abdominal pain, breathing difficulty and rapid weight gain for nephrotic discharges. [1] [3] [6] [11] [13]
References
- [1]Ellis D Pathophysiology, Evaluation, and Management of Edema in Childhood Nephrotic Syndrome. Frontiers in pediatrics, 2015.PMID 26793696
- [2]Siddall EC The pathophysiology of edema formation in the nephrotic syndrome. Kidney international, 2012.PMID 22718186
- [3]Trautmann A IPNA clinical practice recommendations for the diagnosis and management of children with steroid-sensitive nephrotic syndrome. Pediatric nephrology (Berlin, Germany), 2023.PMID 36269406
- [4]Trautmann A IPNA clinical practice recommendations for the diagnosis and management of children with steroid-resistant nephrotic syndrome. Pediatric nephrology (Berlin, Germany), 2020.PMID 32382828
- [5]Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney international, 2021.PMID 34556256
- [6]Floege J Executive summary of the KDIGO 2025 Clinical Practice Guideline for the Management of Nephrotic Syndrome in Children. Kidney international, 2025.PMID 40254362
- [7]Vasudevan A Nephrotic Syndrome: Current Management. Indian journal of pediatrics, 2026.PMID 41910850
- [8]Bravo WC Proteinuria. Pediatrics in review, 2026.PMID 42219187
- [9]Dhakal AK Acute post-streptococcal glomerulonephritis in children-treatment standard. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association, 2025.PMID 40650562
- [10]Singh J A refresher on the primary care and public health management of acute post-streptococcal glomerulonephritis. Australian journal of general practice, 2025.PMID 40174621
- [11]Farkas H International Guideline on the Diagnosis and Management of Pediatric Patients With Hereditary Angioedema. Allergy, 2026.PMID 41618059
- [12]MacGinnitie A Diagnosis and management of pediatric and adolescent hereditary angioedema: A clinical yardstick. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology, 2026.PMID 41775294
- [13]Nawara-Węgrzyn N Protein-losing enteropathy after the Fontan procedure - A cardiologist's and gastroenterologist's perspective. Annals of pediatric cardiology, 2026.PMID 42404519
- [14]Jarasvaraparn C Long-Term Care in Fontan Circulation: Surveillance and Management of Fontan-Associated Liver Disease and Protein-Losing Enteropathy. Current cardiology reports, 2026.PMID 42154163
- [15]Itkin M Pathophysiology of the Lymphatic System in Patients With Heart Failure: JACC State-of-the-Art Review. Journal of the American College of Cardiology, 2021.PMID 34266581
- [16]Ling I Pediatric viral myocarditis: mechanisms, experimental models, and research gaps. Pediatric research, 2026.PMID 41760909
- [17]Piastra M Idiopathic systemic capillary leak syndrome and related shock in PICU: an underdiagnosed disease? Journal of anesthesia, analgesia and critical care, 2026.PMID 41514342
- [18]Maitland K Oral rehydration for severe malnutrition in children with moderate and severe dehydration (GASTROSAM): a phase 2, open-label, superiority randomised controlled trial. The Lancet. Child & adolescent health, 2026.PMID 41825474