Paeds · clinical-assessment-and-reasoning
Pallor in children: diagnostic approach
Also known as Paediatric pallor · Anemia diagnostic approach children · Anaemia in children · Pale child assessment · Childhood iron deficiency anaemia
Fellowship diagnostic approach to paediatric pallor: bedside recognition across skin tones, threat-first stabilisation, MCV–reticulocyte classification of anaemia, directed investigations, iron and haemolysis pathways, and safe disposition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A caregiver says, “She looks washed out.” That sentence can mean a tired toddler after a viral illness, a child who has always been fair like a parent, or a child whose oxygen-carrying capacity is falling. Your job is to turn colour into a mechanism without either panicking every fair child or missing leukaemia because the story “sounded dietary.” [1] [4]
General deterioration frameworks — first impression, work of breathing, circulation and appearance — still apply. Cross-link the seriously-ill-child and vital-sign pages for physiology detail. This leaf owns the pallor-to-anaemia diagnostic path. [17]
P.A.L.E. C.B.C.
Overview & Definition
Pallor means the child looks paler than their usual baseline in places where haemoglobin colour should show — conjunctivae, oral mucosa, nail beds and palms. It is not the same thing as anaemia. Anaemia is a laboratory finding: haemoglobin below the age-appropriate reference range. Many pale-looking children are not anaemic. Some anaemic children are missed because their skin tone, jaundice or ambient light hid the clue. [1] [4] [14]
Clinical pallor is most useful when anaemia is severe and when you examine sites less confounded by melanin. Population studies in high-prevalence settings showed that trained observers using pallor can detect severe anaemia better than mild anaemia. In mixed skin-tone communities the same sign is less reliable, so you lower your threshold for a blood count when the history is concerning. [4] [14]
Once the CBC confirms anaemia, you still do not have a diagnosis. You have a pattern. The diagnosis is the reason red-cell mass fell or failed to rise: not enough iron or other substrates, blood leaving the body, red cells breaking, or the marrow not making enough. [1] [2] [23]
Classification
Hold two grids in your head at once. [1] [23]
Grid one — is the child stable?
A pale child who is floppy, tachypnoeic, poorly perfused or unresponsive is an emergency first and a haematology puzzle second. A playful clinic toddler with gradual pallor is a structured outpatient problem. [1] [17]
Grid two — what is the red-cell pattern?
Mean corpuscular volume (MCV) sorts microcytic, normocytic and macrocytic anaemia. Reticulocyte count asks whether the marrow is responding. High reticulocytes usually mean loss or destruction. Low reticulocytes in the face of significant anaemia usually mean production failure or substrate lack. The film adds morphology: hypochromia, spherocytes, blasts, fragments. [1] [16] [23]
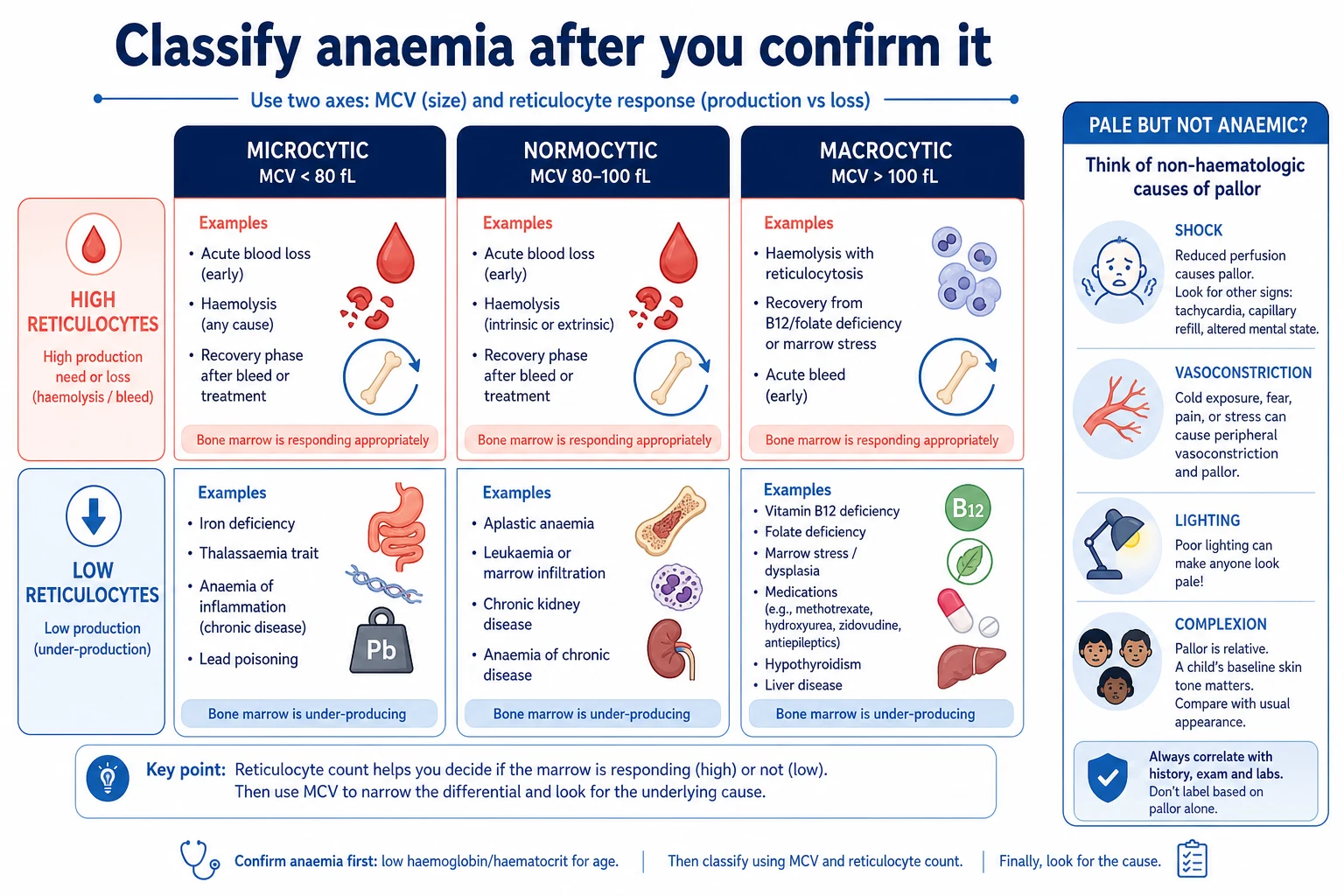
Microcytic patterns classically include iron deficiency, thalassaemia trait or disease, anaemia of inflammation, and lead toxicity. Normocytic patterns include acute blood loss (early), haemolysis, chronic disease, and marrow failure or infiltration. Macrocytic patterns push you toward B12 or folate deficiency, some medications, liver disease, marrow stress or rare marrow disorders. Overlap exists; the film and clinical story still rule. [1] [5] [6] [13]
Non-anaemic pallor sits outside the grid: shock with vasoconstriction, cold exposure, hypothyroidism facies, nephrotic puffiness misread as “pale,” or simply a fair family phenotype under fluorescent lights. If the child is well and mucosae are pink, you may observe — but caregiver concern that something changed still deserves respect. [14] [17]
Epidemiology & Risk Factors
Iron deficiency is the dominant anaemia story in many paediatric clinics worldwide. Risk rises when iron demand outstrips supply: rapid growth in later infancy and adolescence, premature birth with lower stores, diets low in bioavailable iron, and blood loss. Prolonged exclusive milk feeding without an iron source, and heavy cow’s-milk intake that displaces iron-rich foods and can irritate the gut, are classic toddler pathways. [1] [2] [3]
Adolescent girls add menstrual blood loss. Restrictive eating, food insecurity and developmental feeding problems all lower iron intake. Inflammatory disease and chronic kidney disease shift iron handling and suppress erythropoiesis. [2] [3] [13]
Inherited disorders cluster by ancestry and geography: alpha and beta thalassaemia traits and diseases, sickle cell disease, G6PD deficiency, and hereditary spherocytosis. Newborn screening programmes differ by region, so a migrant child may arrive without a known haemoglobinopathy label. [5] [6] [7] [16]
Leukaemia and aplastic anaemia are less common than iron deficiency, but they present in the same waiting room. Age peaks and associated cytopenias help, yet no age is exempt from a first presentation of serious marrow disease. [10] [11]
Pathophysiology
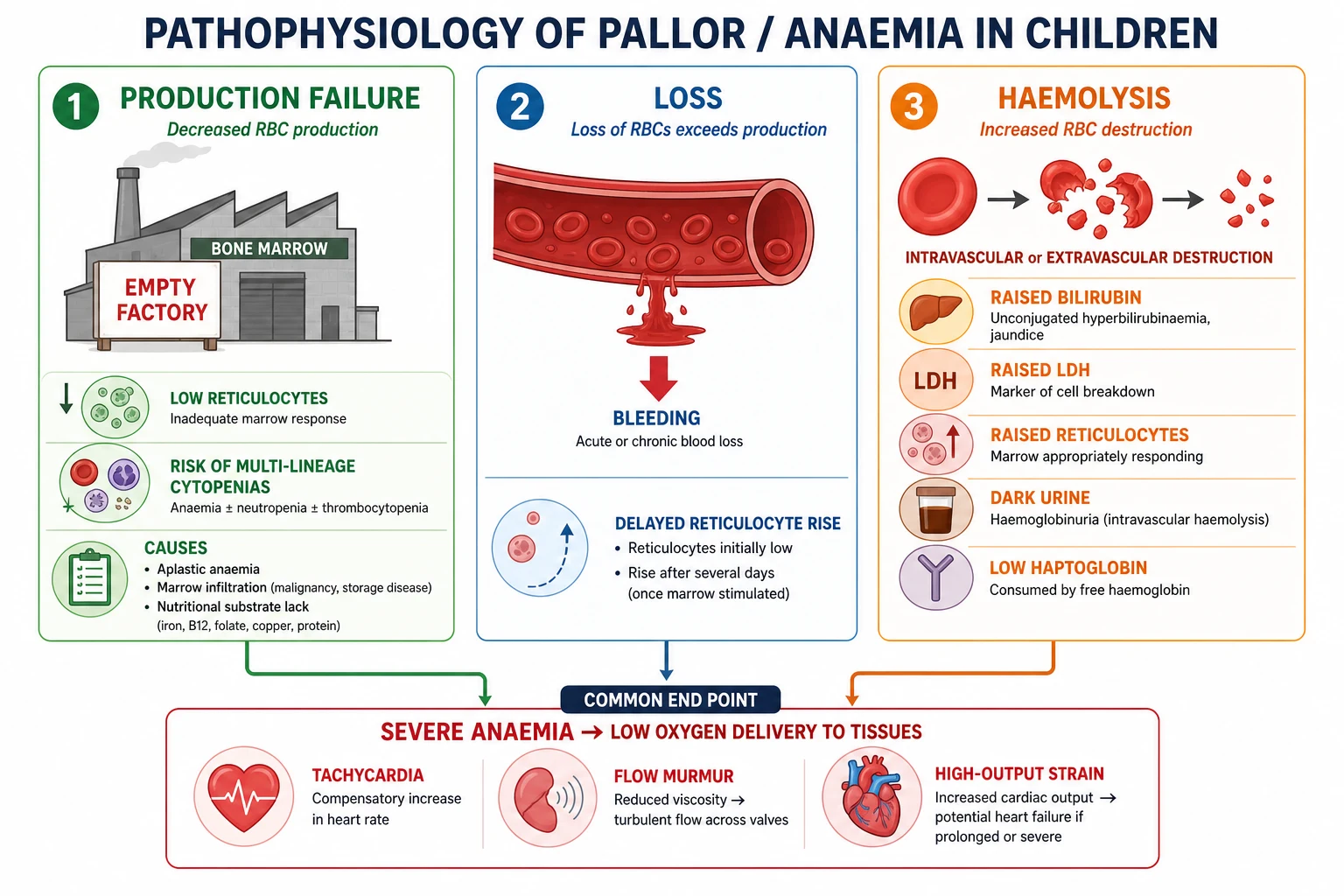
Haemoglobin carries oxygen. When circulating haemoglobin falls, tissues extract more oxygen and the heart raises cardiac output. You see tachycardia, a flow murmur, fatigue and reduced exercise tolerance. If the fall is severe or rapid, high-output strain and decompensation appear. [1] [2]
Iron deficiency starves haemoglobin synthesis. Red cells leave the marrow small and pale — microcytic and hypochromic. Iron is also needed for muscle and brain enzymes, which is one reason prolonged deficiency is more than a cosmetic colour change. [2] [3]
Blood loss removes whole red cells. Early on the MCV is often normal. After a lag, reticulocytes rise if the marrow is healthy and iron is available. Occult gastrointestinal loss or heavy menses can be slow enough that iron deficiency becomes the final common pathway. [1] [13]
Haemolysis shortens red-cell survival. The marrow tries to keep up, so reticulocytes usually rise. Breakdown products raise indirect bilirubin and LDH; haptoglobin may fall; urine may darken with haemoglobinuria in intravascular haemolysis. Immune haemolysis (DAT-positive patterns), membrane disorders such as spherocytosis, enzyme defects such as G6PD, and haemoglobinopathies each break cells for different reasons. [8] [9] [15] [16]
Production failure — aplastic anaemia, infiltration, transient erythroblastopenia, severe substrate lack — leaves reticulocytes inappropriately low. Multi-lineage cytopenias suggest a marrow problem broader than isolated iron lack. [10] [11] [23]
Clinical Presentation
Caregivers may not say “anaemia.” They say the child is tired, less playful, eating ice or dirt, breathing harder on the stairs, or “looking yellow-white.” Teachers may notice school fatigue. Infants may feed poorly or tire mid-feed. [1] [3]
Gradual dietary iron deficiency often looks deceptively well until haemoglobin is quite low. Irritability, pica and a flow murmur are common. Severe cases can still present with heart failure signs. [1] [3]
Acute haemolysis looks different: sudden pallor, jaundice, dark urine, abdominal or back pain, and sometimes fever after infection or an oxidant drug in G6PD deficiency. Family history of neonatal jaundice, gallstones or splenectomy hints at spherocytosis. [7] [8] [16]
Marrow failure or leukaemia may add fever, bruising, petechiae, bone pain, limp, lymphadenopathy or organomegaly. Isolated pallor without those features does not exclude serious disease, but their presence collapses your timeline to same-day action. [10] [11]
Never let “he has always been pale like his father” close the case if activity, growth or caregiver concern has changed. Baseline family colour is real; progressive limitation is data. [14] [17]
Differential Diagnosis
Rank by threat and likelihood at the same time. [1]
- Life threats: shock of any cause with vasoconstriction misread as “just pale,” acute massive haemorrhage, fulminant haemolysis, severe anaemia with cardiac strain, sepsis with marrow suppression, leukaemia with infection risk.
- Common clinic pathways: iron deficiency from diet or blood loss; thalassaemia trait discovered on indices; post-viral transient suppression.
- Important not-to-miss: hereditary haemolytic disorders, AIHA, aplastic anaemia, lead toxicity, B12/folate deficiency in restrictive diets, chronic disease anaemia, occult GI loss, non-accidental injury with blood loss or bruising. [1] [5] [9] [10]
Age shifts priors. Neonates push you toward haemolysis, blood loss and congenital marrow failure. Toddlers push diet and iron. School-age children raise chronic disease and marrow pathology proportions. Adolescents add menstrual loss, sports and restrictive eating. Ancestry raises pre-test probability for specific haemoglobinopathies without becoming a stereotype — use it to choose tests, not to assume destiny. [1] [5] [6]
Clinical & Bedside Assessment
First impression. Is the child interacting? Breathing comfortably? Perfusing? A pale child who fails the first impression is resuscitated, not debated. Caregiver concern that the child is “not himself” associates with critical illness risk in hospital cohorts and should sharpen, not soothe, your attention. [17]
Confirm pallor thoughtfully. Use good light. Inspect conjunctivae, tongue and oral mucosa, palms and nail beds. Compare with the caregiver’s description of baseline. In darker skin, rely more on mucosae and on symptoms than on general facial colour alone. [4] [14]
History that changes the branch.
Diet (milk volume, iron-rich foods, restrictive patterns), growth, development, birth gestation, ethnicity and family blood disorders, jaundice, dark urine, drugs and oxidant exposures (including mothballs/naphthalene and certain antimalarials or antibiotics in G6PD risk), menstrual history, stool colour, bruising, fever, bone pain, travel, and social determinants including food security. Use a professional interpreter when language discordance exists — diet and bleeding histories are easy to get wrong. [1] [7] [20]
Examination. Vital signs with age-normal interpretation, growth parameters, lymphadenopathy, liver and spleen, cardiac failure signs, petechiae, bruising pattern, jaundice, glossitis, neurological signs in severe B12 deficiency, and developmental status. Observe play: a truly limited child tells you more than a single colour judgment. [1] [16]
Investigations
Not every slightly fair well child needs bloods today. Any child with progressive pallor, reduced activity, dietary red flags, ethnicity-linked risk with symptoms, or abnormal examination does. When you decide to test, start with a CBC with indices, reticulocyte count and blood film. That trio is the map. [1] [23]
Directed second-line tests follow the map:
- Microcytic pattern: ferritin and iron studies; consider haemoglobinopathy investigation when indices or ancestry suggest thalassaemia trait, especially if iron studies are discordant. [1] [5] [6]
- Haemolysis pattern: bilirubin, LDH, haptoglobin, DAT, film for spherocytes/fragments; G6PD assay with timing awareness. [8] [9] [16]
- Production failure pattern: urgent film review, other cell lines, reticulocytes, and early haematology involvement for aplastic or infiltrative work-up. [10] [11]
- Consider lead level, B12/folate, renal function and inflammatory markers when the story points there. [1] [13]
G6PD pitfall: during acute haemolysis, older deficient cells may already have lysed, so a single normal assay does not always exclude deficiency — retest later if suspicion remains. [7] [8]
Transfusion sampling: if the child is stable enough, draw diagnostic samples before transfusion so the film and special tests remain interpretable. If the child is unstable, treat first and document what was missed. [12]
Management — Resuscitation
Unstable pale children get the same first actions as any critically ill child: airway, oxygen as needed, support breathing, restore circulation, check glucose if altered, call for senior help early. Severe anaemia can present as high-output failure or shock; volume and blood-product decisions follow local paediatric critical-care and haematology protocols rather than improvised adult recipes. [12]
Massive haemolysis needs trigger removal when known, supportive care, monitoring for acute kidney injury, and specialist input. AIHA and aplastic pathways are haematology emergencies when severe. Fever with neutropenia and pallor is treated as a time-critical infection risk while the diagnosis is sorted. [8] [9] [10] [11]
Handoffs must name haemoglobin, trajectory, bleeding, transfusion decisions and outstanding tests — structured handoff reduces error. [21]
Management — Definitive & Stepwise
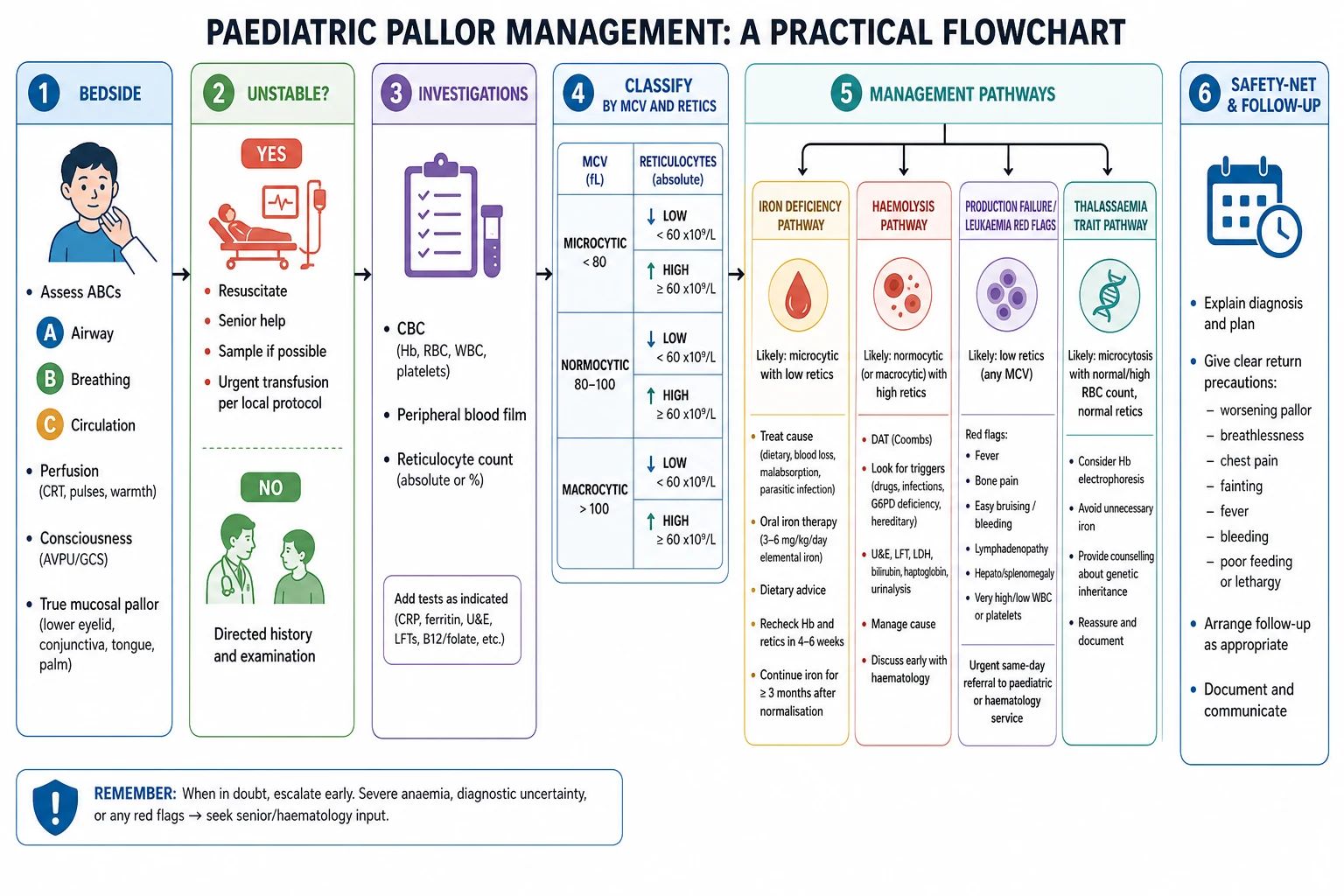
Step 1 — Stabilise and decide location of care.
Clinic, same-day paediatric assessment, ward or critical care. Severe symptoms, very low haemoglobin, active haemolysis, suspected marrow failure or unsafe follow-up push toward hospital. [1] [12]
Step 2 — Confirm and classify.
CBC, film, reticulocytes; add directed tests. Write a one-line problem representation: “18-month-old with dietary risk, microcytic anaemia, low ferritin, no red flags for marrow disease.” [1] [23]
Step 3 — Treat the common pathway correctly.
For iron deficiency: fix the cause (reduce excessive cow’s milk, improve diet, treat menorrhagia or occult loss), start iron therapy per local product guidance, and plan a response check. Practical reviews emphasise cause correction plus replacement, not tablets alone. Expected early marrow response is reticulocytosis followed by haemoglobin rise over subsequent weeks; exact product dosing follows your formulary. [1] [3] [13]
Step 4 — Do not iron-blind yourself.
If microcytosis is out of proportion, iron studies are not deficient, or family history/ancestry suggests it, investigate thalassaemia trait or disease. Empiric iron in non-iron-deficient thalassaemia is the wrong lesson. [5] [6]
Step 5 — Haemolysis and marrow pathways.
DAT-positive AIHA, spherocytosis, G6PD crises and aplastic presentations need haematology partnership. Spherocytosis diagnosis uses film, family history, and specialist tests per guidelines rather than a single bedside guess. [9] [15] [16]
Step 6 — Transfusion principles.
Transfuse for physiological need and local thresholds, not for a number alone in a compensated well child — and do not withhold blood from a decompensating child while waiting for a perfect diagnosis. Cochrane synthesis on thresholds supports thoughtful, context-specific strategies rather than one universal adult cut-off applied to every child. Follow your hospital’s paediatric blood rules. [12]
Step 7 — Communicate, consent, safety-net.
Explain findings in plain language. Agree diet and medicine plans with teach-back. Share uncertainty when tests are pending. Safety-net for worse pallor, dark urine, bleeding, fever, breathing difficulty or reduced responsiveness. Written plus verbal advice helps families act. [18] [22]
Specific Subtypes & Scenarios
Toddler cow’s-milk iron deficiency. High milk volume, limited solids, microcytic anaemia, low ferritin. Reduce milk, improve iron intake, treat iron, recheck. [1] [3]
Adolescent menorrhagia. Quantify periods, examine for other bleeding clues, treat iron and address gynaecological drivers with appropriate colleagues. [13]
Thalassaemia trait. Mild microcytosis, often higher red-cell count, iron studies not deficient; confirm with appropriate haemoglobinopathy testing and counsel families, including future reproductive implications at the right time. [5] [6]
G6PD acute haemolysis. Sudden anaemia after trigger; stop the trigger, support, know assay timing limits, prevent next exposure using CPIC-informed medication caution. [7] [8]
Leukaemia pathway. Pallor plus fever, bruises, bone pain or abnormal film — same-day senior review, not iron trial. [10]
Aplastic anaemia. Severe anaemia with low reticulocytes and often other cytopenias; structured diagnostic work-up per paediatric consensus once stabilised. [10] [11]
Hereditary spherocytosis. Neonatal jaundice history, family gallstones/splenectomy, spherocytes on film; use guideline-based diagnosis and severity staging. [15] [16]
Refugee child. Incomplete screens, interpreter for diet, dual infection–nutrition awareness, non-stigmatising haemoglobinopathy testing. [20]
Neonate. Early jaundice and pallor shift to haemolysis and blood-loss pathways; this leaf flags urgency and handoff rather than replacing neonatology protocols. [16]
Complications & Pitfalls
- Trusting facial colour alone across diverse skin tones. [14]
- Calling every microcytosis iron deficiency. [5] [6]
- Starting iron without asking about ongoing blood loss. [13]
- Missing leukaemia or aplastic anaemia while “trying iron for a month.” [10] [11]
- Checking G6PD only once during crisis and closing the book. [8]
- Transfusing a stable child before samples — or delaying blood in instability. [12]
- Ignoring caregiver concern. [17]
- No interpreter for diet and bleeding history. [20]
- Fragmented handoffs that drop pending film review. [21]
- Shame-based diet counselling that destroys trust. [19]
Prognosis & Disposition
Most dietary iron deficiency improves when cause and replacement are both handled and adherence is real. Failure of expected response means wrong diagnosis, ongoing loss, malabsorption or non-adherence — not “give up.” [1] [3] [13]
Haemolytic and marrow disorders have disease-specific trajectories; early haematology involvement improves safety. Prolonged severe anaemia risks developmental and cardiac effects, which is one reason you do not normalise months of progressive limitation. [2] [10]
Safe discharge needs a named review plan, clear safety-net advice, medicine access, and a family who can return. If food insecurity or chaos blocks iron and diet change, treat social determinants as part of the prescription. [18]
Special Populations
Neonates and young infants need haemolysis and congenital pathways in the first differential. [16]
Toddlers are the dietary iron teaching core. [1]
Adolescents need confidential menstrual and eating histories. [13]
Medical complexity may hide chronic disease anaemia and procedural blood-loss burden. [1]
Ancestry-linked risk guides testing with respectful counselling, not racialised assumptions. [5] [6]
Indigenous families deserve culturally safe diet and access conversations. [19]
Migrant and refugee families need interpreters and catch-up screening logic. [20]
Out-of-home care documents growth, diet and unexplained injury carefully when pallor and bruising coexist. [19]
Evidence, Guidelines & Regional Differences
Wang’s AFP review remains a high-yield practical map of iron deficiency and other anaemias in infants and children. Short’s evaluation-and-management article and Leung’s updated review reinforce cause-directed iron care. [1] [3] [13]
Pasricha’s Lancet review frames global iron-deficiency biology and burden — useful for why this common problem still damages development and capacity. [2]
Stoltzfus and later skin-tone studies remind you that pallor is a tool with limits, strongest for severe anaemia and weaker as a stand-alone screen across complexions. [4] [14]
Thalassaemia rapid reviews (Muncie, Baird) prevent the iron-for-everyone error. CPIC G6PD guidance modernises medication safety. Paediatric AIHA, spherocytosis and aplastic consensus documents set referral and work-up expectations. Cochrane transfusion threshold evidence supports protocolised, context-aware red-cell use. [5] [6] [7] [9] [11] [12] [16]
Local hospital anaemia and transfusion pathways, newborn screening panels, and culturally safe care for Aboriginal, Torres Strait Islander and Māori whānau shape real practice. Use RCH-style clinical guidelines as operational anchors where applicable. [1]
NICE-aligned iron and anaemia pathways and regional haemoglobinopathy services often structure clinic answers; use local referral thresholds. [3]
AAP-aligned iron prevention/screening ages and AFP practical reviews dominate outpatient teaching language; follow institutional transfusion committees for thresholds. [1] [13]
Provincial newborn screening and paediatric haematology networks determine haemoglobinopathy detection and referral flow. [6]
Exam Pearls
- Pallor → confirm → classify by MCV + reticulocytes. [23]
- Iron deficiency is common; thalassaemia trait is the classic microcytic trap. [1] [5]
- Low reticulocytes + severe anaemia = production problem. [10] [23]
- Fever + pallor + cytopenias/bruising = same-day serious pathway. [11]
- G6PD assay timing can fool you in acute haemolysis. [8]
- Mucosal pallor beats general face colour across skin tones — still use the CBC. [4] [14]
- Prove iron response; no rise means rethink. [3] [13]
- Caregiver concern is data; safety-net every plan. [17] [18]
- State transfusion principles, not invented mL/kg theatre numbers, unless your local protocol is in front of you. [12]
High-yield anchors
References
- [1]Wang M Iron Deficiency and Other Types of Anemia in Infants and Children. American family physician, 2016.PMID 26926814
- [2]Pasricha SR Iron deficiency. Lancet (London, England), 2021.PMID 33285139
- [3]Leung AKC Iron Deficiency Anemia: An Updated Review. Current pediatric reviews, 2024.PMID 37497686
- [4]Stoltzfus RJ Clinical pallor is useful to detect severe anemia in populations where anemia is prevalent and severe. The Journal of nutrition, 1999.PMID 10460203
- [5]Muncie HL Jr Alpha and beta thalassemia. American family physician, 2009.PMID 19678601
- [6]Baird DC Alpha- and Beta-thalassemia: Rapid Evidence Review. American family physician, 2022.PMID 35289581
- [7]Gammal RS Expanded Clinical Pharmacogenetics Implementation Consortium Guideline for Medication Use in the Context of G6PD Genotype. Clinical pharmacology and therapeutics, 2023.PMID 36049896
- [8]Lau HK Acute massive haemolysis in children with glucose-6-phosphate dehydrogenase deficiency. Hong Kong medical journal, 2006.PMID 16603783
- [9]Blackall D Autoimmune Hemolytic Anemia in Children: Laboratory Investigation, Disease Associations, and Treatment Strategies. Journal of pediatric hematology/oncology, 2022.PMID 35235549
- [10]Furlong E Aplastic anaemia: Current concepts in diagnosis and management. Journal of paediatrics and child health, 2020.PMID 32619069
- [11]Shimano KA Diagnostic work-up for severe aplastic anemia in children: Consensus of the North American Pediatric Aplastic Anemia Consortium. American journal of hematology, 2021.PMID 34342889
- [12]Carson JL Transfusion thresholds and other strategies for guiding red blood cell transfusion. The Cochrane database of systematic reviews, 2025.PMID 41114449
- [13]Short MW Iron deficiency anemia: evaluation and management. American family physician, 2013.PMID 23317073
- [14]Ughasoro MD Clinical Anaemia Detection in Children of Varied Skin Complexion: A Community-based Study in Southeast, Nigeria. Journal of tropical pediatrics, 2017.PMID 27449936
- [15]Tole S Genotype-phenotype correlation in children with hereditary spherocytosis. British journal of haematology, 2020.PMID 32436265
- [16]Bolton-Maggs PH Guidelines for the diagnosis and management of hereditary spherocytosis--2011 update. British journal of haematology, 2012.PMID 22055020
- [17]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [18]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [19]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [20]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [21]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [22]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [23]Celkan TT What does a hemogram say to us? Turkish archives of pediatrics, 2020.PMID 32684755