Paeds · clinical-assessment-and-reasoning
Poor feeding in infants and children
Also known as Feeding difficulties · Feeding problems · Poor oral intake · Pediatric feeding disorder · Infant feeding difficulty · Dysphagia in children
A threat-first fellowship approach to poor feeding from neonate to school age: classify mechanism and acuity, reverse life-threatening causes, observe feeds safely, build a prioritised differential, investigate without shotgun harm, and deliver stepwise multidisciplinary feeding care with clear safety-nets.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A caregiver says the baby “is not feeding well.” That sentence can mean almost anything. It may mean half the usual milk volume. It may mean a 45-minute fight at the breast. It may mean coughing and turning blue with the bottle. It may mean a toddler who will only touch three foods. Your first job is not to name a syndrome. Your first job is to decide whether this child is in danger this hour. [5] [26]
Poor feeding means intake is inadequate, inefficient, unsafe, or so restricted that nutrition, hydration, growth or family function is threatened. That definition deliberately covers more than one disease. A day-3 neonate with sepsis and a school-age child with severe food selectivity both “feed poorly,” but the tempo and first actions differ. [1] [11]
Pediatric feeding disorder (PFD) is the consensus label for impaired oral intake that is not age-appropriate and is associated with medical, nutritional, feeding-skill or psychosocial dysfunction. It is a framework for chronic or recurrent feeding problems, not a substitute for acute triage. Avoidant/restrictive food intake disorder (ARFID) sits nearby and can overlap; current consensus work helps separate shared ground from distinct mental-health pathways. [1] [14] [15]
This page owns bedside reasoning for poor feeding. It links to dedicated growth charting, faltering-growth, disease-specific gastroenterology and resuscitation pages rather than hiding those whole chapters here. [3] [11]
Classification
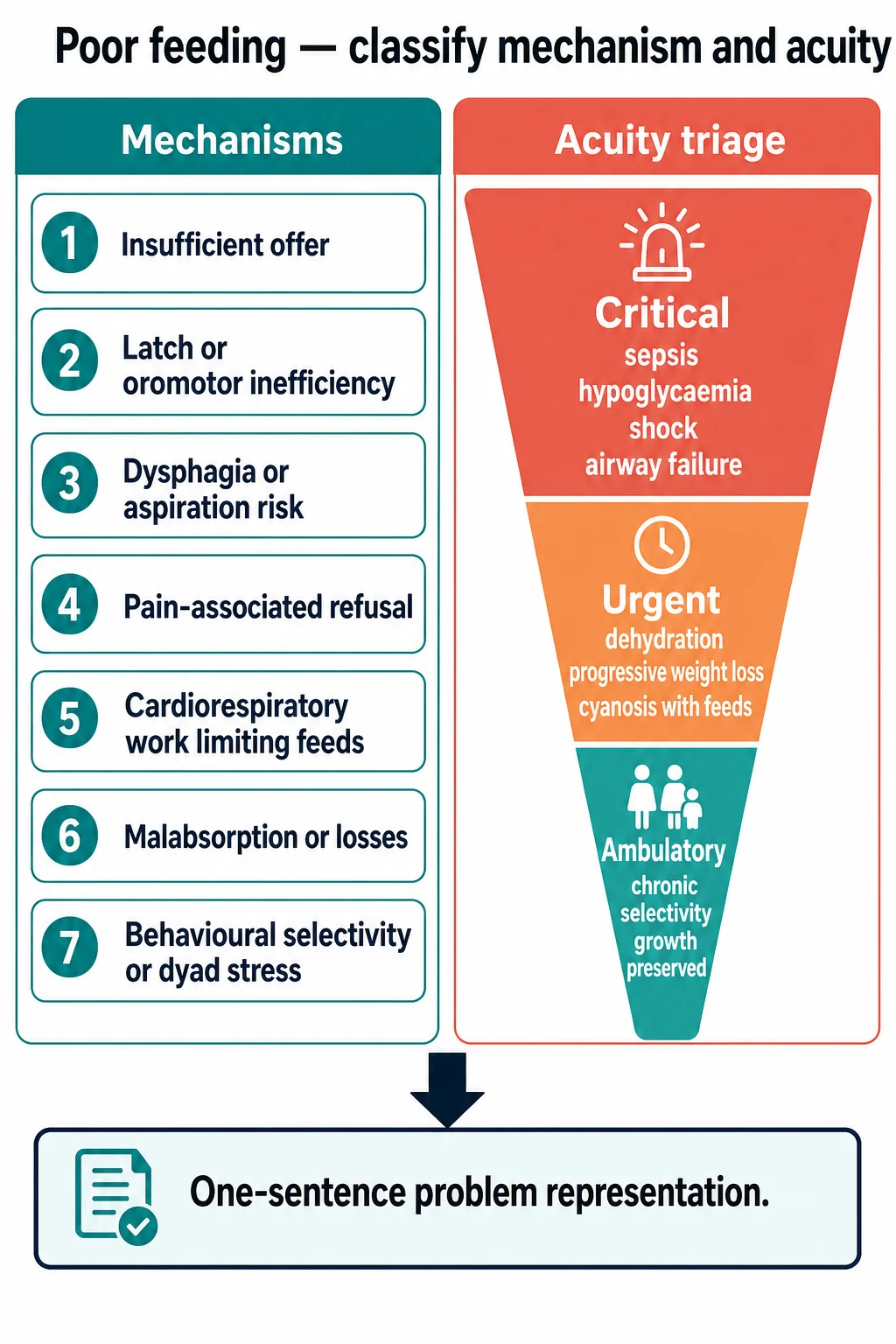
Classify acuity before you classify mechanism. Critical means life-threatening physiology now: shock, severe dehydration, hypoglycaemia, respiratory failure, progressive neuromuscular weakness or inability to protect the airway. Urgent means the child is currently perfusing but trajectory is unsafe: progressive weight loss, feed-associated cyanosis, bilious vomiting or a caregiver who cannot keep the child hydrated. Ambulatory means chronic restriction or inefficiency with preserved safety and a workable outpatient plan. [5] [11] [26]
Then classify mechanism. Most children sit in more than one box. [1] [5] [10]
- Insufficient offer — low milk supply, spaced feeds, diluted formula, food insecurity, or caregiver misinformation. [1]
- Latch or oromotor inefficiency — poor seal, weak suck, disorganised suck–swallow–breathe, structural limits such as cleft or restricted tongue mobility. [4]
- Dysphagia or aspiration risk — penetration, aspiration, wet voice, cough with liquids, recurrent chest infection. [2]
- Pain-associated refusal — thrush, otitis, oesophagitis, cow’s milk protein allergy (CMPA), severe reflux symptoms. [9]
- Cardiorespiratory work limiting feeds — heart failure, chronic lung disease, acute respiratory illness stealing energy and time from feeding. [19]
- Malabsorption or losses — diarrhoea, vomiting, high stoma output, metabolic disease. [5]
- Behavioural selectivity or dyad stress — sensory restriction, force-feeding cycles, maternal mental health strain, ARFID-pattern fear or interest loss. [14]
PFD, by consensus, spans four domains: medical, nutritional, feeding skill and psychosocial. Naming the active domains prevents the trap of treating only the tube, or only the behaviour, or only the reflux script. [1] [13]
Faltering growth is related but not identical. A child can feed poorly for 24 hours with normal growth charts. A child can also fall across centiles while still “finishing bottles” of energy-poor feeds. NICE-summary guidance on faltering growth helps you decide when growth concern changes the investigation and support threshold. [3] [11]
Epidemiology & Risk Factors
Feeding difficulty is common in hospital and community practice, but prevalence depends on definition. Nationwide administrative data using a PFD construct show a substantial paediatric burden, highest in younger children and those with medical complexity. That matters in viva: do not treat feeding clinics as rare specialty folklore. [12]
Neonates and young infants carry the highest risk that “poor feeding” is sepsis, cardiac disease, hypoglycaemia or a metabolic emergency. Late-preterm infants add a second epidemiology: inefficient oral skills, longer feeds, maternal exhaustion and disrupted early bonding, even when no surgical diagnosis exists. [26] [30] [4]
Risk rises with prematurity, NICU stay, delayed oral experience, congenital heart disease, chronic lung disease, neurodisability, Down syndrome, cleft or craniofacial difference, and previous tube feeding. Early feeding practices and forced or highly pressured feeding can also seed later parent-reported feeding difficulty. [19] [37] [29] [31]
Social risk is clinical risk. Food insecurity, language discordance, limited transport, racism in prior care, caregiver depression and out-of-home care all change what “not feeding well” means and how quickly help is sought. Ask about them. Do not wait for the dietitian to discover them three visits later. [1] [30]
Pathophysiology
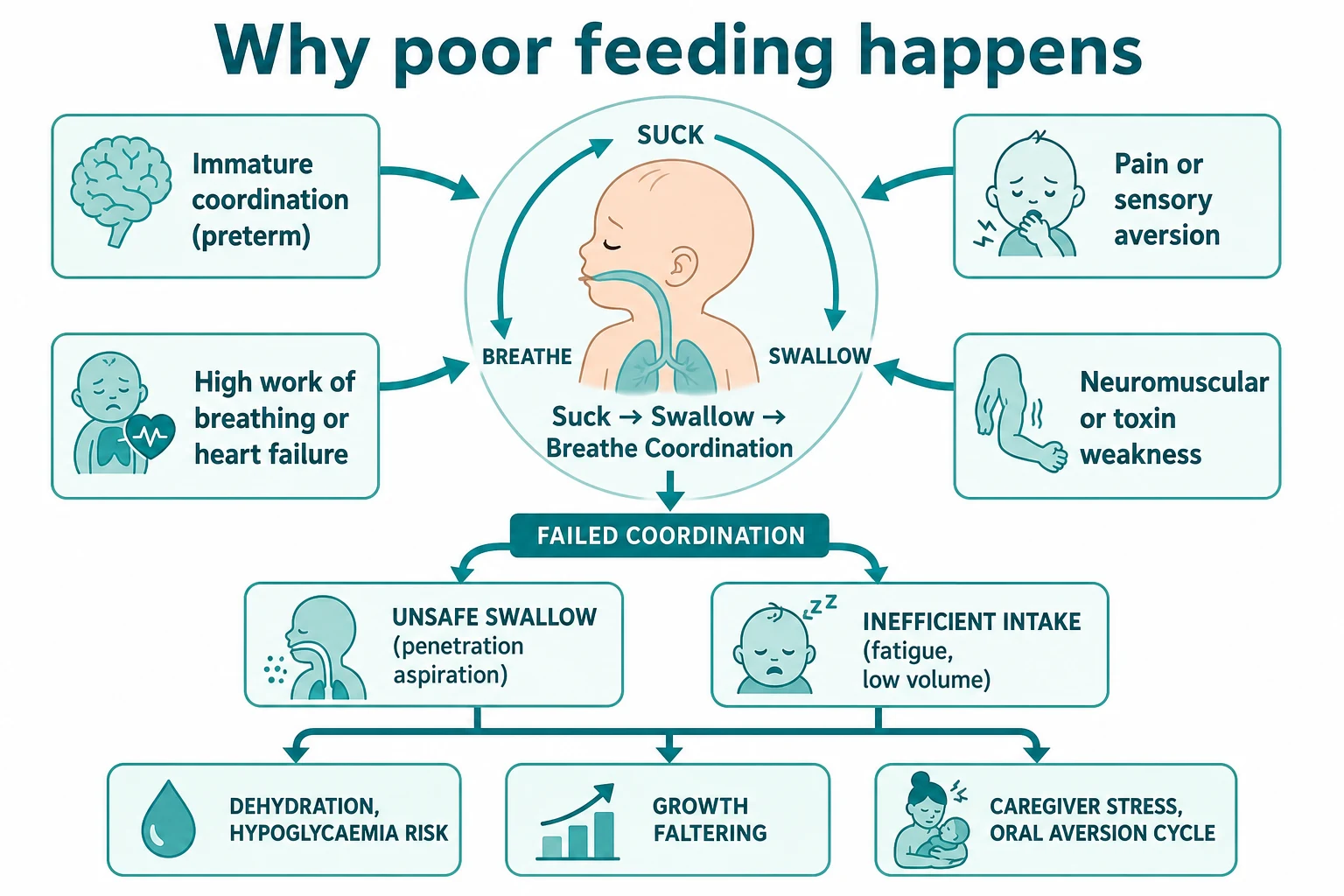
Safe oral feeding needs timed suck, swallow and breathe, intact airway protection, enough stamina, and a brain that still wants the next mouthful. In preterm and many term neonates those systems are still maturing. Immature coordination produces both inefficiency and aspiration risk. [4] [10]
When work of breathing or cardiac output demand is high, feeding becomes an endurance event the child cannot win. The infant starts well, then tiring, sweating, tachypnoea or colour change appear. Volume falls long before a textbook “failure to thrive” label is written. Congenital heart disease nutrition reviews make this energy-theft physiology explicit. [19] [5]
Pain and sensory threat rewrite the learning. A child who links milk with burning reflux, allergic gut pain or forced spooning will refuse earlier next time. That is adaptive learning, not naughtiness. Repeated aversive feeds create oral aversion and caregiver–child conflict, which then maintain the disorder. [1] [23] [9]
Neuromuscular disease and botulinum toxin blunt bulbar power. Infant botulism classically pairs constipation, weak cry, poor suck and descending weakness. The feed problem is the early window, not a side issue. [20] [21] [22]
Downstream, low intake produces dehydration, ketosis and hypoglycaemia risk, micronutrient gaps and growth faltering. Silent aspiration can continue without dramatic coughing, so absence of a cough does not prove a safe swallow. Instrumental studies and aspiration-pneumonia syntheses keep that caution alive. [10] [32] [33]
Clinical Presentation
Start from the doorway. Is the infant floppy and poorly responsive? Is a toddler grey and quiet in the car seat? Is a parent frantically offering a bottle every few minutes? Appearance is part of the feeding assessment. [5] [26]
Neonate and young infant. Caregivers report reduced volume, longer feeds, falling wet nappies, vomiting, colour change, or “not waking for feeds.” Serious infection may show only subtle feed refusal before vital signs crash. Hypoglycaemia may present as jitteriness, lethargy or seizures after poor intake. [26] [25]
Older infant. Look for latch pain, clicking feeds, milk spilling, fatigue halfway through, arching, cough with liquids, or blood in stool. Sweating and tachypnoea during feeds raise cardiac concern. Recurrent chest symptoms raise swallow-safety concern. [6] [19] [16]
Toddler and preschooler. Texture refusal, pocketing, gagging, extreme selectivity, mealtime battles and growth plateau are common scripts. Autism-related sensory restriction and ARFID-pattern fear or low interest can present here. The same age group can still have organic dysphagia; do not assume behaviour first if cough, wet voice or poor growth is present. [15] [34] [2]
School-age and adolescent. Selective intake, fear of choking after an aversive event, low appetite with mood change, or chronic tube dependence all appear. Growth, school lunch behaviour and family conflict become central data. [15] [14]
Differential Diagnosis
Build the differential by threat, not by specialty silo. [5] [11]
| Threat tier | Examples | Bedside clues |
|---|---|---|
| Immediate physiology | Sepsis, hypoglycaemia, shock, airway failure | Lethargy, abnormal tone/temp, poor perfusion, low glucose |
| Cardiorespiratory | CHD, bronchiolitis, pneumonia, chronic lung disease | Sweat, tachypnoea, desaturation, prolonged feeds |
| Surgical/metabolic | Obstruction, NEC risk age, inborn error | Bilious vomit, distension, encephalopathy, odd odour |
| Swallow safety | Oropharyngeal dysphagia, anatomical anomaly | Cough, wet voice, recurrent chest infection |
| Pain/allergy/reflux disease | CMPA, thrush, true GERD | Arching, blood/mucus stool, oral lesions, feed aversion |
| Structure/technique | Latch, supply, ankyloglossia, cleft | Nipple pain, clicking, inefficient transfer |
| Behavioural/psych | PFD psychosocial domain, ARFID, autism selectivity | Extreme restriction, fear, conflict, preserved or falling growth |
| Toxin/neuromuscular | Infant botulism, myopathy | Constipation, weak cry, descending weakness |
Normal regurgitation is not GERD. NASPGHAN/ESPGHAN guidance emphasises that uncomplicated reflux is common and does not justify automatic acid suppression. CMPA can mimic reflux and feed refusal; look for additional allergic or stool clues and use elimination/challenge logic rather than endless PPI trials. [23] [9]
Ankyloglossia may contribute to breastfeeding difficulty, but it is not the default explanation for every tired feeder. Assess function, milk transfer and alternative causes before promising that frenotomy will fix the story. Cochrane evidence and later quantitative reviews inform counselling without turning the consult into a procedure sales pitch. [6] [7] [8]
Clinical & Bedside Assessment
Immediate safety
Do not take a 20-minute diet history from a grey infant. Run ABCDE. Check capillary glucose early in any unwell neonate or poorly responsive child with low intake. Treat shock and respiratory failure on local pathways while you gather a focused AMPLE history. [26] [25] [5]
Feeding history that changes decisions
Ask for numbers, not adjectives. [5] [11]
- Usual and current feed type, volume or minutes at breast, frequency and night pattern. [5]
- How long each feed takes and whether the child tires halfway. [5]
- Cough, choke, wet voice, colour change, sweat or pause-and-pant pattern. [2]
- Wet nappies, stool pattern, vomiting character (forceful, bilious, blood). [11]
- Growth trajectory and any prior weights. [3]
- Pregnancy, birth gestation, NICU course, surgeries, medications. [5]
- Who feeds the child, food security, caregiver sleep and mood, conflicting advice. [1]
- What has already been tried: formulas, thickeners, tongue-tie release, reflux medicines, forced feeding. [5]
Observe a feed when safe
If the child is stable, watch. Note position, latch or bottle flow, suck–swallow–breathe rhythm, work of breathing, colour, fatigue and caregiver handling. LATCH is a simple charting scaffold for breastfeeding observation: latch, audible swallowing, type of nipple, comfort, hold. It supports documentation and coaching; it does not diagnose cardiac disease or sepsis. [17] [18] [31]
Oral-motor bedside tools exist but vary in quality; systematic review work cautions against treating any single checklist as definitive. Combine observation with history and growth. [36]
Examination
Undress the child. Assess hydration using several signs together rather than one magic feature; validated dehydration scales exist but still need clinical synthesis. Examine palate, tongue mobility, thrush, tone, alertness, fontanelle, chest, heart, abdomen, anus/stool if relevant, and neurological bulk/power in suspected botulism. Plot weight, length/height and head circumference on the appropriate WHO or local chart and compare with previous points. [27] [28] [20]
Problem representation
Write one sentence before tests. [5]
“Day-5 term infant with 24 hours of halved feed volume and three wet nappies, alert but cool peripherally, no cough, differential led by evolving infection or inadequate intake with hypoglycaemia risk.” [26] [5]
That sentence drives disposition more than a laboratory shopping list. [5] [11]
Investigations
Always consider first in the unwell or high-risk infant: point-of-care glucose; observations trended against age; septic work-up according to age and local early-onset/late-onset pathways; blood gas and electrolytes when dehydration, shock or metabolic disease is plausible. Do not delay antimicrobials in suspected neonatal sepsis for perfect cultures. [26] [25]
Growth-led testing. If faltering growth is confirmed on serial measurements, deepen the history and examine carefully before shotgun panels. NICE-summary and primary-care FTT reviews emphasise targeted testing based on clues, not every available assay on day one. [3] [11]
Swallow safety testing. Videofluoroscopic swallow study (VFSS) and fiberoptic endoscopic evaluation of swallowing (FEES) can detect penetration and aspiration when bedside concern persists and management will change. FEES has been studied in NICU infants for laryngeal penetration and aspiration detection. Choose the modality with SLP/ENT colleagues; never send an unstable child to radiology “just to complete the work-up.” [2] [32] [16]
Selective specialty tests. ECG/echo when cardiac load is suspected; allergy-informed elimination for CMPA; metabolic labs when encephalopathy, unexplained acidosis or consanguinity/family history raises concern; neuroimaging or genetics only with a clear developmental or neurological story. [19] [9] [5]
Low-value defaults to avoid. Routine acid-suppression trials without GERD features; unlimited formula switches without a plan; radiation exposure without management consequence; labelling “picky eater” without growth and safety review. [23] [1]
Management — Resuscitation
- Airway and breathing. Position, oxygen as needed, senior help if the child cannot protect the airway or is tiring. Stop oral trials if aspiration risk is high in an unstable child. [2] [16]
- Circulation. Treat shock on local paediatric pathways. Assess dehydration severity and replace deficits carefully; use clinical scales as adjuncts, not sole truth. [27]
- Glucose. Check early. Treat hypoglycaemia with age-appropriate glucose delivery and reassess neurology and feeding readiness. Neonatal monitoring thresholds and treatment steps should follow current local and ABM-informed neonatal guidance rather than remembered cut-offs alone. [25]
- Sepsis. In neonates and young infants with acute feed refusal plus risk features, start the sepsis clock. Poor feeding is a classic early non-specific sign. [26]
- Botulism pathway. If descending weakness, constipation and bulbar failure fit, involve senior, ICU and public-health/antitoxin pathways per current clinical guidelines. Do not wait for perfect laboratory confirmation to stabilise ventilation and stop unsafe oral feeds. [22] [20]
- Temporary nutrition route. Nil by mouth with intravenous glucose-containing fluids when oral intake is unsafe. Nasogastric support can bridge hydration and energy once airway risk is judged acceptable. [5] [35]
Management — Definitive & Stepwise
After threats are controlled, climb a ladder. Skip rungs only with a reason. [1] [31] [5]
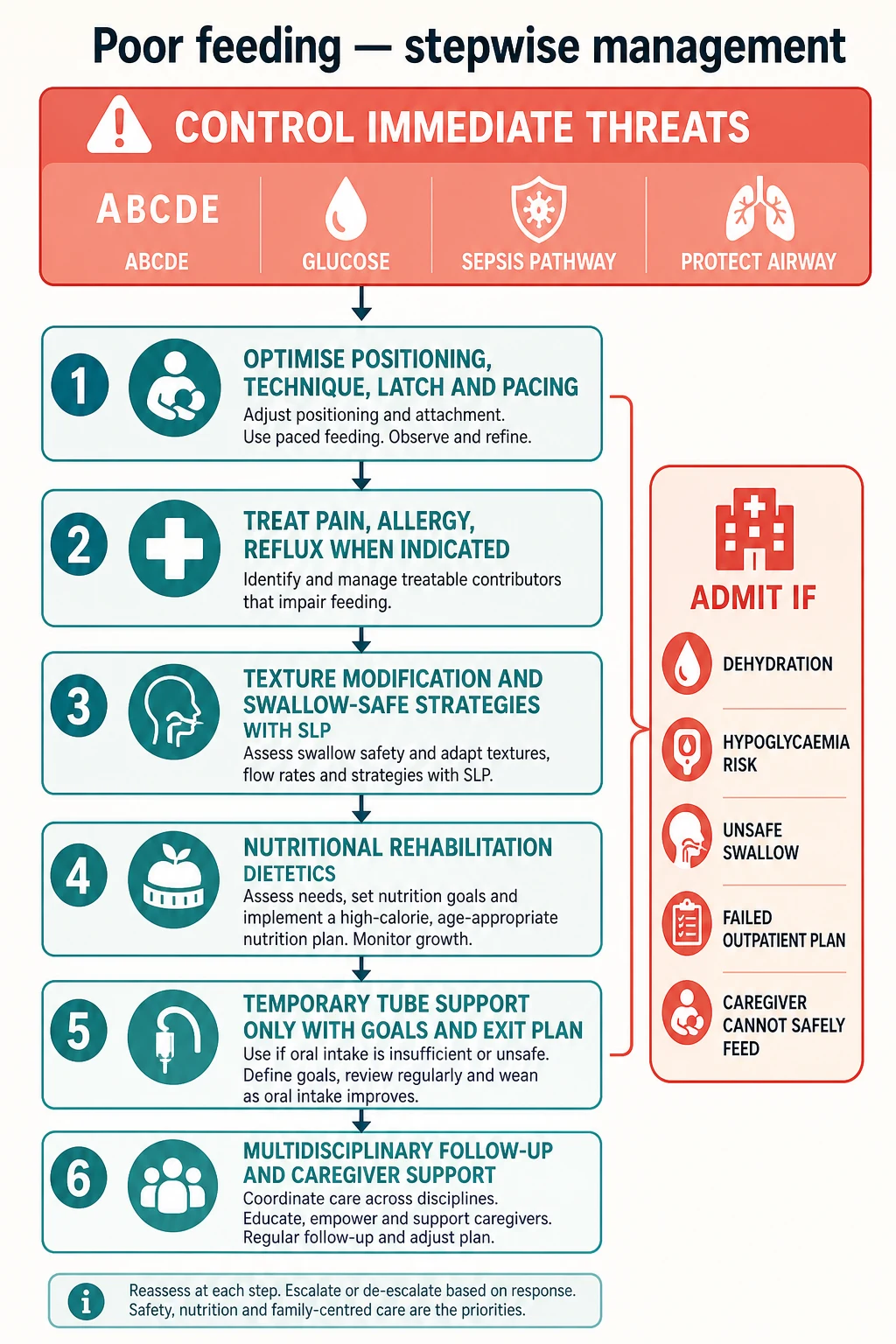
Step 1 — Optimise offer, position, latch and pacing
Lactation support for breastfeeding dyads. Correct positioning, paced bottle feeding, appropriate teat flow, and scheduled support for the exhausted late-preterm pair. Use LATCH-informed coaching and early weight checks. [17] [18] [30] [31]
Step 2 — Treat pain and medical drivers when indicated
Thrush, otitis, CMPA elimination under dietetic guidance, and true GERD care per NASPGHAN/ESPGHAN principles. Thickeners can help selected reflux or dysphagia phenotypes but are not harmless universal additives; age, thickening agent and aspiration goals matter. [9] [23] [24]
Step 3 — Swallow-safe strategies with feeding therapy
Speech-language pathology or specialist feeding therapy for texture progression, pacing, chin-down or side-lying strategies where appropriate, and skill building. Oral-motor work should be individualised; tool choice is secondary to a clear goal. [10] [2] [36]
Step 4 — Nutritional rehabilitation
Dietetics sets energy and protein targets, fortification and micronutrient repair while protecting the feeding relationship. Growth is re-measured on WHO or local standards. [28] [3] [1]
Step 5 — Tubes with an exit plan
Nasogastric tubes bridge acute gaps. Gastrostomy or jejunal feeding is for sustained need, unsafe swallow, or unavoidable energy debt — for example some children with Down syndrome or complex neurodisability — not for clinician impatience. ESPGHAN position work on jejunal feeding stresses indications, complications and multidisciplinary oversight. Every tube order should state goals, review date and weaning intent. [35] [37] [13]
Step 6 — Behavioural and mental-health pathways
For ARFID-pattern fear, low interest or sensory restriction, use developmentally appropriate behavioural feeding support and mental-health collaboration. Autism-associated severe selectivity needs the same safety and growth guardrails, not moral lectures. [15] [34] [14]
Frenotomy counselling
If ankyloglossia is functionally limiting breastfeeding after skilled lactation assessment, discuss frenotomy using balanced evidence: Cochrane data and later meta-analysis suggest possible breastfeeding benefit in selected dyads, with method limitations. Do not use frenotomy to close a sepsis or cardiac differential. [7] [8] [6]
Specific Subtypes & Scenarios
Late-preterm inefficient feeder. Sleepy at the breast, long feeds, falling weights, mother in tears. Prioritise safety glucose and dehydration checks, then intensive lactation support, temporary supplementation strategy and early review. Address maternal mental health explicitly. [30] [25] [31]
Day 2–7 neonate with abrupt feed drop. Think sepsis and hypoglycaemia first, not “breastfeeding establishing.” Examine fully, measure glucose, use local sepsis pathways, and do not discharge on reassurance alone. [26] [25]
Sweaty, breathless feeder. Consider congenital heart disease and respiratory disease. Limit oral endurance demands, support breathing, and involve cardiology early when examination or saturation findings support it. [19]
Cough and desaturation with thin fluids. Stop high-risk oral trials, involve SLP, consider instrumental assessment when stable, and protect the chest. Absence of cough never excludes silent aspiration. [2] [32] [33]
Blood and mucus stools with feed refusal. CMPA enters the top tier. Trial elimination with dietetic cover rather than endless formula roulette without a plan. [9]
Toddler with three accepted foods and autism traits. Screen growth and safety, then map PFD domains and ARFID features. Multidisciplinary care beats a single “eat or else” lecture. [34] [14] [15]
Constipation, weak cry, poor suck, descending weakness. Infant botulism until proven otherwise. Stabilise airway, stop unsafe oral intake, escalate, follow diagnosis and antitoxin guidance. [20] [21] [22]
Complications & Pitfalls
Common pitfalls include premature closure and iatrogenic harm. [5]
- Closing as tongue-tie or reflux before threat assessment. [6] [23]
- Force-feeding that creates lifelong oral aversion. [1] [29]
- Starting long-term PPIs for normal regurgitation. [23]
- Leaving an NG tube without dietetic goals or review date. [35]
- Missing food insecurity and caregiver depression. [30] [1]
- Discharging without concrete volumes, red flags and early weight check. [3] [11]
- Assuming no cough means no aspiration. [32] [33]
Prognosis & Disposition
Prognosis tracks the driver. Acute infectious or technique problems often improve quickly with support. Medical complexity, neurodisability and entrenched aversion need longer multidisciplinary work. Early skilled intervention improves the odds of safe, adequate oral feeding. [31] [10] [13]
Admit or observe when there is dehydration, hypoglycaemia risk, suspected sepsis, unsafe swallow, failed outpatient plan, unreliable follow-up, or a caregiver who cannot safely feed at home. [26] [5] [27]
Ambulatory care can work for stable children with preserved growth when the plan is specific: volumes or fortification, therapy referrals, red flags, and a booked weight check. Safety-net in plain language and use teach-back. [3] [1]
Special Populations
NICU graduates and late-preterm infants need structured oral-feeding progression and family support, not a single discharge lecture. [31] [30]
Congenital heart disease requires energy-aware feeding plans and early dietetic/cardiology collaboration. [19]
Neurodisability and technology dependence need baseline-aware goals; “normal oral diet” may not be the right endpoint. [10] [35]
Down syndrome has high rates of feeding difficulty and occasional gastrostomy need; assess hypotonia, airway and cardiac comorbidity. [37]
Autism and sensory feeding restriction need PFD/ARFID-informed care without abandoning growth safety. [34] [15]
Indigenous, migrant and language-discordant families need professional interpreting, culturally safe lactation support and attention to access barriers. [1]
Out-of-home care and safeguarding contexts require careful collateral history; severe neglect can present as poor intake and growth failure. [11] [3]
Evidence, Guidelines & Regional Differences
Core evidence anchors for this page include the Goday PFD consensus and later characterisation work, dysphagia reviews, NICE faltering-growth summary guidance, NASPGHAN/ESPGHAN GERD recommendations, ABM neonatal hypoglycaemia protocol, CDC botulism guidelines, and WHO growth standards. [1] [2] [3] [23] [25] [22] [28]
Local practice commonly uses WHO growth standards in infancy, hospital clinical guidelines for growth faltering, strong lactation-consultant networks, and retrieval pathways for the unwell neonate. Always follow local sepsis and hypoglycaemia protocols. [28] [3]
NICE NG75-era faltering-growth guidance shapes community recognition and referral language; secondary care still applies threat-first assessment for acute poor feeding. [3]
PFD coding and ARFID pathways are more visible in US literature; NASPGHAN GERD guidance and AAP-adjacent nutrition practice influence primary care. Canadian case teaching often highlights rare but critical mimics such as infant botulism. [1] [23] [21]
Controversies to handle honestly in viva: frenotomy effectiveness and overuse; PPI over-prescription in infants; PFD versus ARFID boundary cases; and when instrumental swallow testing adds value versus risk. [7] [8] [23] [14] [32]
Exam Pearls
- Threat first: glucose, sepsis, airway, cardiac, metabolic. Technique later. [26] [25] [19]
- Watch a feed when safe. History alone misses coordination failure. [31] [17]
- Silent aspiration exists. No cough ≠ safe swallow. [32] [33]
- PFD has four domains; single-specialty care is incomplete. [1] [13]
- Normal regurgitation is not an automatic PPI script. [23]
- Tubes need goals and an exit plan. [35]
- Frenotomy is a targeted tool after skilled assessment, not a master key. [7] [8]
- Write concrete safety-nets: volumes, wet nappies, breathing, colour, lethargy, when to return. [3] [11]
FEED-SAFE triage
PFD vs ARFID lens
PFD emphasises medical, nutrition, skill and psychosocial dysfunction around oral intake and is built for multidisciplinary paediatric care. ARFID is a DSM feeding/eating disorder pattern of avoidance or restriction driven by sensory sensitivity, fear of aversive consequences or low interest, with impairment not explained by body-image goals. Overlap is real; consensus work exists to reduce misclassification. Use both lenses when a child has severe restriction. [1] [14] [15]
References
- [1]Goday, Praveen S Pediatric Feeding Disorder: Consensus Definition and Conceptual Framework. Journal of pediatric gastroenterology and nutrition, 2019.PMID 30358739
- [2]Lawlor, Claire M Diagnosis and Management of Pediatric Dysphagia: A Review. JAMA otolaryngology-- head & neck surgery, 2020.PMID 31774493
- [3]Gonzalez-Viana, Eva Faltering growth in children: summary of NICE guidance. BMJ (Clinical research ed.), 2017.PMID 28963099
- [4]Viswanathan, Sreekanth Feeding and Swallowing Difficulties in Neonates: Developmental Physiology and Pathophysiology. Clinics in perinatology, 2020.PMID 32439109
- [5]Gulati, Ish K Approach to Feeding Difficulties in Neonates and Infants: A Comprehensive Overview. Clinics in perinatology, 2020.PMID 32439111
- [6]Costa-Romero, Marta Ankyloglossia in breastfeeding infants. An update. Archivos argentinos de pediatria, 2021.PMID 34813240
- [7]O'Shea, Joyce E Frenotomy for tongue-tie in newborn infants. The Cochrane database of systematic reviews, 2017.PMID 28284020
- [8]Cordray, Holly Quantitative impact of frenotomy on breastfeeding: a systematic review and meta-analysis. Pediatric research, 2024.PMID 37608056
- [9]Malik, Rohan Cow's Milk Protein Allergy. Indian journal of pediatrics, 2024.PMID 37851326
- [10]Dodrill, Pamela Pediatric Dysphagia: Physiology, Assessment, and Management. Annals of nutrition & metabolism, 2015.PMID 26226994
- [11]Cole, Sarah Z Failure to thrive: an update. American family physician, 2011.PMID 21524049
- [12]Kovacic, Karlo Pediatric Feeding Disorder: A Nationwide Prevalence Study. The Journal of pediatrics, 2021.PMID 32702429
- [13]Sharp, William G Toward Better Understanding of Pediatric Feeding Disorder: A Proposed Framework for Patient Characterization. Journal of pediatric gastroenterology and nutrition, 2022.PMID 35687655
- [14]Estrem, Hayley H A US-Based Consensus on Diagnostic Overlap and Distinction for Pediatric Feeding Disorder and Avoidant/Restrictive Food Intake Disorder. The International journal of eating disorders, 2025.PMID 39679744
- [15]Kambanis, P Evelyna Assessment and Treatment of Avoidant/Restrictive Food Intake Disorder. Current psychiatry reports, 2023.PMID 36640211
- [16]Moroco, Annie E Pediatric Dysphagia. Pediatric clinics of North America, 2022.PMID 35337544
- [17]Jensen, D LATCH: a breastfeeding charting system and documentation tool. Journal of obstetric, gynecologic, and neonatal nursing : JOGNN, 1994.PMID 8176525
- [18]Riordan, J Predicting breastfeeding duration using the LATCH breastfeeding assessment tool. Journal of human lactation : official journal of International Lactation Consultant Association, 2001.PMID 11847847
- [19]Mills, Kimberly I Nutritional Considerations for the Neonate With Congenital Heart Disease. Pediatrics, 2022.PMID 36317972
- [20]Cox, Nadine Infant botulism. American family physician, 2002.PMID 11996423
- [21]Schwartz, Kevin L Constipation and poor feeding in an infant with botulism. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 2012.PMID 22988147
- [22]Rao, Agam K Clinical Guidelines for Diagnosis and Treatment of Botulism, 2021. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports, 2021.PMID 33956777
- [23]Rosen, Rachel Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Journal of pediatric gastroenterology and nutrition, 2018.PMID 29470322
- [24]Duncan, Daniel R Clinical Aspects of Thickeners for Pediatric Gastroesophageal Reflux and Oropharyngeal Dysphagia. Current gastroenterology reports, 2019.PMID 31098722
- [25]Wight, Nancy E ABM Clinical Protocol #1: Guidelines for Glucose Monitoring and Treatment of Hypoglycemia in Term and Late Preterm Neonates, Revised 2021. Breastfeeding medicine : the official journal of the Academy of Breastfeeding Medicine, 2021.PMID 33835840
- [26]Shane, Andi L Neonatal sepsis. Lancet (London, England), 2017.PMID 28434651
- [27]Jauregui, Joshua External validation and comparison of three pediatric clinical dehydration scales. PloS one, 2014.PMID 24788134
- [28]WHO Multicentre Growth Reference Study Group WHO Child Growth Standards based on length/height, weight and age. Acta paediatrica (Oslo, Norway : 1992). Supplement, 2006.PMID 16817681
- [29]Babik, Katarzyna Infant feeding practices and later parent-reported feeding difficulties: a systematic review. Nutrition reviews, 2021.PMID 33486523
- [30]Vizzari, Giulia Feeding Difficulties in Late Preterm Infants and Their Impact on Maternal Mental Health and the Mother-Infant Relationship: A Literature Review. Nutrients, 2023.PMID 37432319
- [31]Hasenstab, Kathryn A Evidence-Based Approaches to Successful Oral Feeding in Infants with Feeding Difficulties. Clinics in perinatology, 2022.PMID 35659100
- [32]Suterwala, M S Using fiberoptic endoscopic evaluation of swallowing to detect laryngeal penetration and aspiration in infants in the neonatal intensive care unit. Journal of perinatology : official journal of the California Perinatal Association, 2017.PMID 28055025
- [33]Imdad, Aamer Laryngeal Penetration and Risk of Aspiration Pneumonia in Children with Dysphagia-A Systematic Review. Journal of clinical medicine, 2023.PMID 37373780
- [34]Bourne, Laura Avoidant/restrictive food intake disorder and severe food selectivity in children and young people with autism: A scoping review. Developmental medicine and child neurology, 2022.PMID 35112345
- [35]Broekaert, Ilse J The Use of Jejunal Tube Feeding in Children: A Position Paper by the Gastroenterology and Nutrition Committees of the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition. Journal of pediatric gastroenterology and nutrition, 2019.PMID 31169666
- [36]Barton, C Pediatric Oral Motor Feeding Assessments: A Systematic Review. Physical & occupational therapy in pediatrics, 2018.PMID 28430014
- [37]Poskanzer, Sheri A Feeding difficulty and gastrostomy tube placement in infants with Down syndrome. European journal of pediatrics, 2020.PMID 31984440