Paeds · clinical-assessment-and-reasoning
Recognising the seriously ill child and paediatric assessment triangle
Also known as Seriously ill child · Sick child assessment · Paediatric Assessment Triangle · PAT · Paediatric deterioration recognition
An age- and baseline-aware fellowship approach to recognising serious paediatric illness, using the Paediatric Assessment Triangle for first impression, immediate ABCDE stabilisation, repeated reassessment, capability-based escalation or retrieval, communication, safeguarding and safe disposition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seriously ill child is one who may lose airway, effective breathing, circulation, neurological function or immediate safety unless the team acts promptly. You do not need a diagnosis before treating a life threat. Equally, a child who looks settled may still need urgent review because of age, history, a dangerous possible diagnosis, change from baseline or caregiver concern. One normal sign never settles the question. [4] [7] [15]
Keep four questions separate. How severe is the illness? Is an airway, breathing, circulation or neurological problem present now? Is the child getting worse? Could a dangerous diagnosis still be present despite a calm examination? PAT helps only with the first impression. Observations, history, examination, response to treatment, trend and caregiver concern answer the rest. [2] [3] [4]
The observable pathway from doorway to disposition
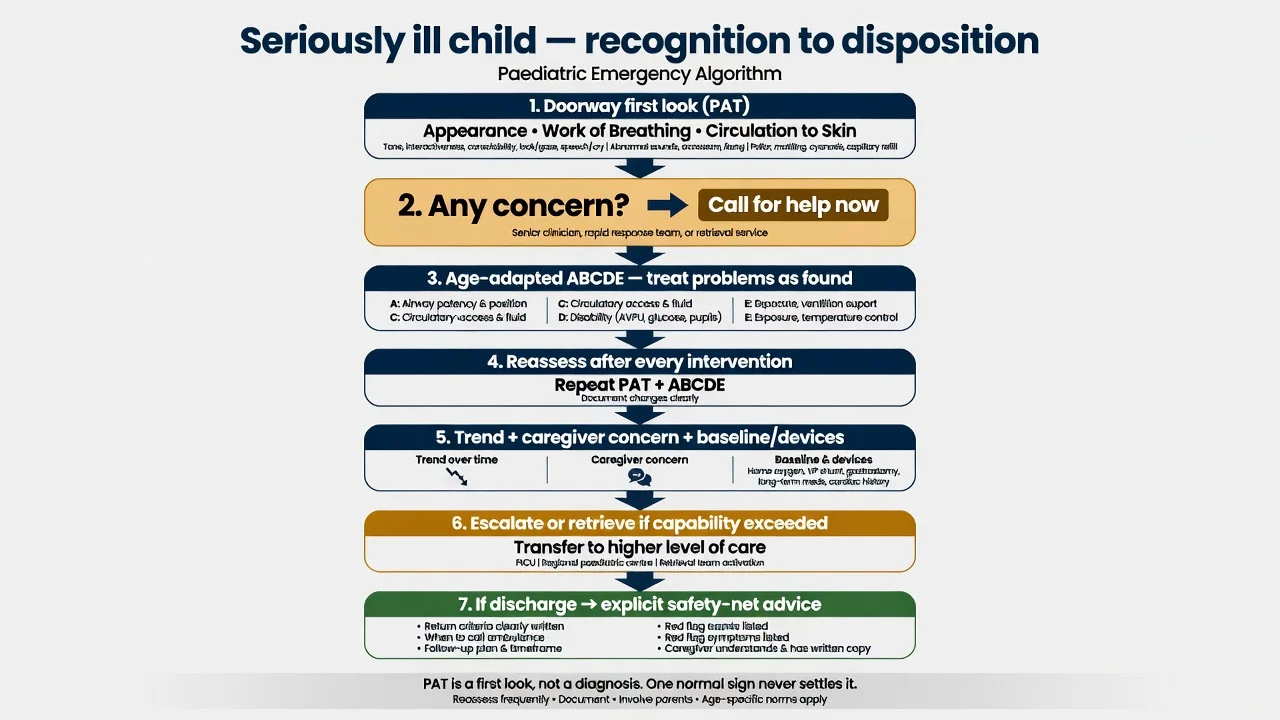
First 30 seconds
Look before touch. Describe Appearance, Work of Breathing and Circulation to Skin. If any finding worries you, call for help and start ABCDE immediately.
First 5 minutes
Name a leader, allocate roles, attach appropriate monitoring, prepare age- and weight-appropriate equipment, treat each ABCDE problem as found and reassess from A after every action.
Focused history and examination
Ask what is different from usual and what worries the caregiver most. Add age-specific observations, focused examination, baseline, devices, exposures and targeted tests without delaying treatment.
Reassess and escalate
Record the intended result, actual response, adverse effects and direction of change. Call senior, PICU or retrieval teams before the child needs support your service cannot provide.
Disposition and communication
Choose a destination that can provide the required monitoring and rescue. Hand over trend, timed treatment and response; explain the plan to the child and caregiver; continue safeguarding work in parallel.
Classification
The canonical PAT is the rapid visual and auditory assessment defined in the American Academy of Pediatrics PEPP framework. Appearance uses TICLS: Tone, Interactiveness, Consolability, Look or gaze, and Speech or cry. Work of Breathing includes visible or audible effort, abnormal sounds, retractions, nasal flaring and abnormal positioning. Circulation to Skin means pallor, mottling or cyanosis. Capillary refill, pulse, blood pressure, oxygen saturation, temperature and PEWS are measured afterwards; they are not PAT domains. [2] [3]
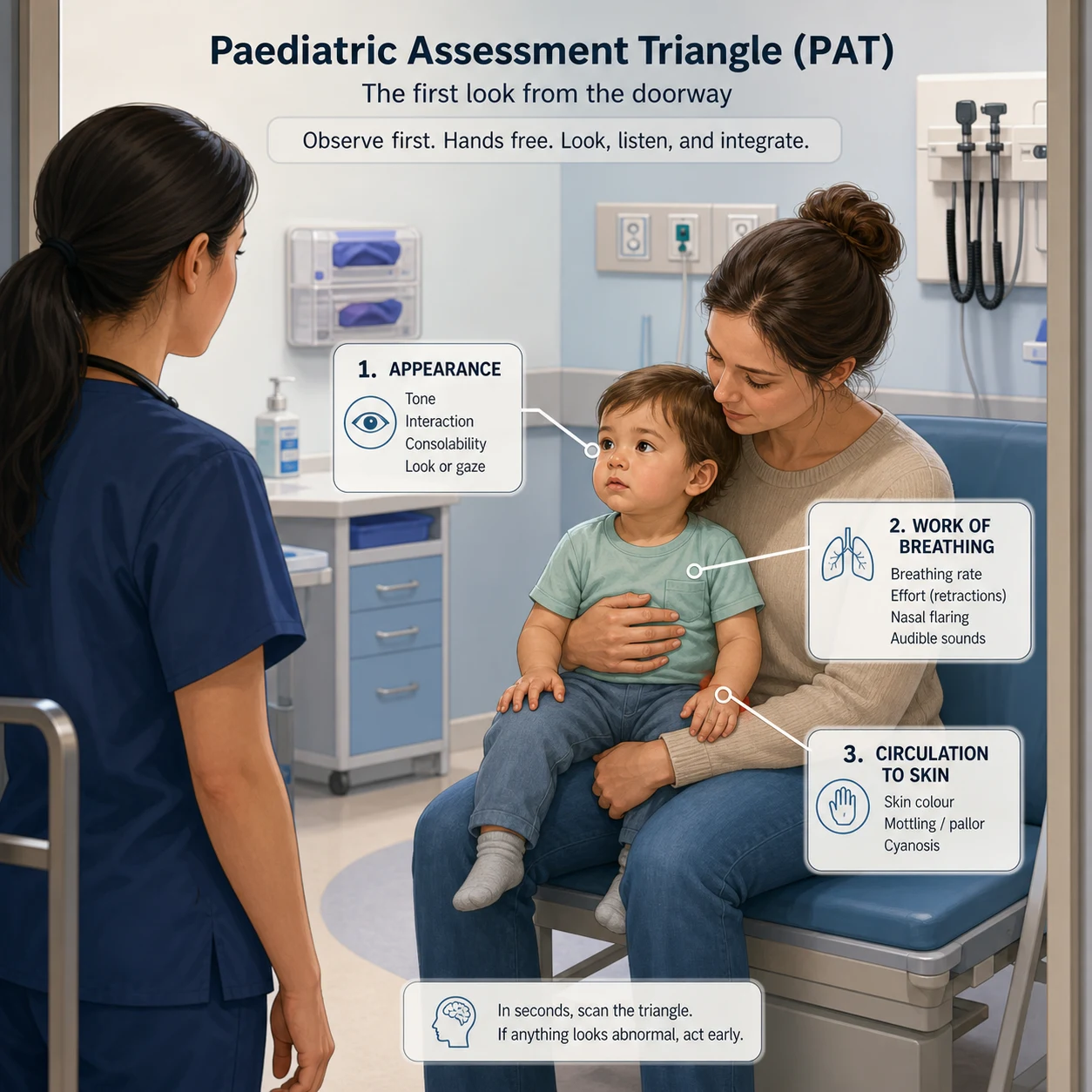
Read the figure like this: describe exactly what you see, say which ABCDE area may be failing, and act. PAT has no numeric total. Capillary refill is not part of canonical PAT. A normal PAT means only that the three domains look normal at that moment; it is not a discharge decision. [2] [4] [7]
PAT
Hands-off first impression
- Three observational domains
- Seconds; no equipment required
- Describes dominant pattern of possible organ-system failure
- Not a diagnosis, triage score, complete examination or disposition rule
ABCDE
Primary assessment and stabilisation
- Hands-on, prioritised life-threat survey
- Treat each threat when found
- Uses measurements, equipment and interventions
- Repeat from A after each intervention or deterioration
PEWS
Setting-bound recognition and response
- Age-banded measured observations
- Requires a validated chart and response system
- Trend, staffing and governance determine performance
- A low score never cancels clinician or caregiver concern
PAT combinations describe a pattern, not a diagnosis. All three domains normal means a stable first impression at that moment. Abnormal Appearance alone points toward brain or metabolic dysfunction. Work of Breathing alone suggests respiratory distress; Appearance plus Work of Breathing suggests respiratory failure. Circulation to Skin alone with preserved Appearance suggests compensated shock; Appearance plus Circulation to Skin suggests decompensated shock. All three abnormal suggests cardiopulmonary failure. Each pattern tells you where to focus ABCDE first, while history, examination, observations and response establish the cause. [2] [12]
| Observed pattern | Safe interpretation | What must follow |
|---|---|---|
| All three domains normal | Stable first impression now | Age-adjusted measurements, focused history and examination, risk assessment and reassessment |
| Appearance abnormal alone | Brain or metabolic dysfunction pattern | Disability assessment, airway and breathing check, glucose when clinically relevant and a neurological, metabolic or toxic differential |
| Work of Breathing abnormal alone | Respiratory-distress pattern | Assess effectiveness, air entry, oxygenation, fatigue and cause during ABCDE |
| Appearance plus Work of Breathing abnormal | Respiratory-failure pattern | Immediate help, airway and breathing support, disability assessment and escalation |
| Circulation to Skin abnormal with preserved Appearance | Compensated-shock pattern | Integrated circulation assessment, reversible threats, likely shock type and escalation based on available support |
| Appearance plus Circulation to Skin abnormal | Decompensated-shock pattern | Immediate resuscitation, cause-directed threat control and parallel critical-care or retrieval activation |
| All three domains abnormal | Cardiopulmonary-failure pattern | Full resuscitation response and parallel critical-care or retrieval activation |
Epidemiology & Risk Factors
Do not quote one incidence for “missed deterioration.” Emergency, ward, community, retrieval and low-resource studies include different children and outcomes. The practical lesson is that every recognition tool depends on where and in whom it is used. Children with bacteraemia have had a normal PAT; caregiver concern predicted critical illness in one Australian hospital cohort; and children with medical complexity are not well represented in many studies. These findings justify senior review and reassessment, but not a universal probability or trigger. [4] [15] [16]
Child and disease context
- Young infant or neonatal transition
- Prematurity, chronic or multisystem disease
- Immunocompromise or attenuated inflammatory presentation
- Congenital heart or pulmonary vascular physiology
- Technology dependence or personalised emergency plan
Presentation context
- Caregiver says the child is different from usual
- Recurrent presentation, recent discharge or prior healthcare contact
- Poor intake, altered behaviour, seizure, collapse or unexplained injury
- Medication exposure, ingestion, trauma or environmental risk
- A concerning diagnosis despite presently preserved physiology
Health-system context
- Rural distance, weather or delayed transport
- Limited access to monitoring, airway support, critical care or vasoactive rescue
- Telehealth constraints and poor connectivity
- Language or communication-access barriers
- Handover gaps, incomplete observations or unclear escalation ownership
Family and social context
- Caregiver expertise or repeated concern
- Health literacy, access or transport barriers
- Racism or prior adverse healthcare experience
- Safeguarding, family violence or uncertain caregiver authority
- Pending results or safety net that the family cannot enact
Season, outbreaks, travel, contacts and exposures change which causes are likely. They do not change the order of immediate care. Say, “The exposure makes infection more likely, but ineffective breathing is the problem I must treat first.” Use the same discipline with fever, pain, crying, dehydration or anxiety. These may alter observations, but they must not automatically explain deterioration. [4] [22]
Pathophysiology
Children can maintain interaction and blood pressure while faster heart rate, increased breathing effort and vascular tone compensate. The amount of reserve and the expected observations change with age. Compensation is therefore a collection of findings, not a fixed sequence. When demand exceeds reserve, air entry and gas exchange fail, interaction falls, pulses weaken, organs malfunction and blood pressure may fall. Hypotension is worrying, but waiting for hypotension misses earlier circulatory failure. [5] [12]
Oxygen delivery depends on effective ventilation and oxygenation, blood oxygen content, cardiac output, tissue perfusion and cellular use. Failure at any point can make the child seriously ill. [12]
Cardiac output depends on heart rate and stroke volume, while vascular tone directs blood flow. Neonates and young infants have limited stroke-volume reserve, so heart rate contributes more to maintaining output. Tachycardia and vasoconstriction may preserve pressure and interaction for a time, but also increase demand. In a child who is hypoxic or deteriorating, a falling or abnormally low heart rate is an ominous sign, not evidence of recovery. This context-specific warning does not make every isolated bradycardia pre-arrest, as stated in Resuscitation Council UK 2025 PLS guidance. [5] [12]
Young infants have smaller airways, different respiratory mechanics and less reserve for their metabolic demand. Greater effort may initially maintain air movement, but fatigue can make ventilation worse even while retractions or visible effort lessen. This is why a suddenly quiet breathless infant may be sicker. There is no universal age threshold: count the rate under stated conditions and interpret it for the child’s exact age and context. At birth, lung aeration and circulatory transition require Resuscitation Council UK 2025 NLS guidance, not an older-child pathway. [5] [12]
Read the figure like this: a quieter child after marked respiratory effort may be recovering or tiring. Recovery requires easier breathing with effective air entry, improving interaction and stable perfusion. Less effort with poorer air entry or interaction is failure until proved otherwise. The “inborn error” label in the figure means an inborn error of metabolism. [12] [22] [23]
Compensation
Reserve is being recruited
- Increasing rate or effort
- Tachycardia and vascular tone may preserve pressure
- Interaction may initially remain acceptable
- Signs must be interpreted against exact age, conditions and personal baseline
Failure
Reserve is being exhausted
- Reduced respiratory effort with poor air entry
- Falling interaction or altered consciousness
- Weak pulses, worsening skin perfusion or organ dysfunction
- Hypotension can occur late and is not a prerequisite
Response
A trend, not a diagnosis
- State the expected change before acting
- Reassess all affected ABCDE domains
- Record benefit, adverse effect and unresolved threat
- Improvement after an action does not prove one cause
Respiratory deterioration may start with faster breathing and more effort, then become ineffective as fatigue, limited air entry or impaired drive develops. Circulatory failure may be hypovolaemic, distributive, cardiogenic, obstructive or mixed; do not expect a fixed warm-to-cold sequence. Appearance may worsen because of hypoxia, altered ventilation, reduced perfusion, seizure, dangerous low glucose, toxin or systemic illness. Reassessment shows whether treatment helped; it does not prove one cause. [12] [13] [23]
Birth transition has different physiology and pathways from older-child resuscitation. Congenital heart disease, pulmonary hypertension, autonomic dysfunction, neuromuscular weakness and chronic respiratory support can also change the child’s usual observations and route to failure. Learn the personal baseline, communication method, device dependence and emergency plan before calling a finding “normal” or “improved.” [16] [21]
Clinical Presentation
Observe before touch unless treatment cannot wait. Describe interaction and arousability; tone and posture; cry or speech; consolability and gaze; visible and audible breathing effort; symmetry and apparent air entry; pallor, mottling or cyanosis; and caregiver-child interaction. Replace “looks sick” with what you can see and hear. If any finding is worrying, call for help and start ABCDE while someone else obtains the focused history. [1] [2] [22]
| Life stage | High-value change from usual | Assessment adaptation |
|---|---|---|
| Neonate and young infant | Feeding, behaviour, tone, breathing, colour or temperature change; serious illness may occur without fever | Clarify gestation, birth and maternal history; observe feeding and breathing; obtain prompt senior review and relevant bedside glucose |
| Older infant | Cry, gaze, consolability, tone, wet nappies, feeding or interaction | Observe with the caregiver before separation or handling; interpret limited reserve and rapid change |
| Toddler | Loss of play, mobility, speech, usual attachment behaviour or intake | Begin on the caregiver; use play and least-distressing steps first; reconsider ingestion, injury and safeguarding risks |
| Preschool child | Change in play, speech, gait, toileting, feeding or participation | Offer simple choices, explain before touch and ask the child directly without leading |
| School-age child | Exercise tolerance, school function, pain description, behaviour or hidden exposure | Take the child’s history directly while retaining caregiver observations and seeking assent |
| Adolescent | Collapse, chest symptoms, intake restriction, substance exposure, self-harm risk or pregnancy possibility | Create private time when safe, explain confidentiality and its limits, and avoid adult assumptions |
| Young-adult transition | Change in personal plan, device support, capacity or caregiver role | Transfer baseline, emergency plan and decision-making arrangements across paediatric and adult teams |
For the neonate and young infant, the named Victorian source is the Royal Children’s Hospital Melbourne seriously unwell neonate and young infant guideline. It supports prompt senior review, risk-directed assessment and bedside glucose, and warns that serious illness may be afebrile or non-specific. The caregiver’s account of change from baseline remains important. [15] [16]
Respiratory distress means increased effort while breathing remains effective. Respiratory failure means oxygenation or ventilation is ineffective and Appearance is often abnormal. A quieter child may be improving, but less effort with poor air entry, reduced interaction or worse perfusion suggests fatigue. Pulse oximetry can overestimate oxygenation, including in children with darker skin, and it does not measure ventilation. Trust the number only when the signal is credible and agrees with the child. [2] [11] [22]
Assess circulation as a whole: pulse rate and quality, skin temperature and colour, capillary-refill technique and result, mental state, urine output, blood pressure, device function and trend. Normal blood pressure or capillary refill alone does not exclude shock. [7] [12]
Serious neurological illness may appear as irritability, poor feeding, reduced interaction, abnormal tone or posture, seizure or altered behaviour rather than a verbal complaint. [23]
Differential Diagnosis
Build the differential in this order: what can kill the child now, what is most likely, what is reversible, and what is most harmful to miss. PAT tells you which part of the child may be failing. It does not tell you why. Keep the important cause groups open until focused history, examination, targeted tests and response to treatment make them less likely. [1] [12] [23]
Airway and respiratory
- Upper-airway obstruction: abnormal upper-airway sound, position or rapid worsening with agitation
- Lower-airway disease: wheeze or prolonged expiration with variable air entry
- Parenchymal disease: increased effort with hypoxaemia or focal findings
- Disordered drive or neuromuscular weakness: low effort despite ineffective breathing
- Do not infer cause from one respiratory sign
Circulatory
- Hypovolaemic: loss history and low-volume pattern
- Distributive: infection or allergic context with vascular-tone failure
- Cardiogenic: cardiac history, dysrhythmia, congestion or poor response to empiric fluid
- Obstructive: mechanical impediment with abrupt compromise
- Mixed physiology is possible; response and overload risk matter
Neurological and metabolic
- Seizure, post-ictal state or central infection
- Hypoxia or altered ventilation
- Clinically dangerous low glucose
- Endocrine, electrolyte or inborn metabolic disorder
- Toxin, medication effect or withdrawal
Infection and inflammation
- Serious infection may be occult or afebrile
- Young infant and immunocompromised presentations may be subtle
- Non-blanching or rapidly evolving skin findings require urgent synthesis
- Sepsis pathway timing depends on risk group and shock, not fever alone
Cardiac and collapse
- Congenital heart or pulmonary vascular physiology
- Dysrhythmia or myocardial dysfunction
- Syncope and exertional symptoms
- Individual saturation and circulation baseline may differ
- Do not label primary respiratory disease before checking circulation
Trauma, toxicology and environment
- Occult injury despite initial compensation
- Unknown substance, dose or time
- Medication error or device-related exposure
- Temperature or environmental insult
- Stabilise first while obtaining collateral history
Mimics and modifiers
- Pain, fever, crying, fear, separation or recent exertion
- Reassess after comfort without dismissing persistent abnormalities
- Functional or behavioural distress remains a diagnosis of exclusion when physiology is concerning
- A response to comfort does not prove a benign cause
Safeguarding
- Non-accidental injury, neglect, poisoning or induced illness
- Inconsistent or developmentally implausible history
- Unexplained recurrent deterioration or delayed presentation
- Immediate ABCDE treatment and safety planning proceed in parallel
A clear synthesis sounds like this: “This child has abnormal Appearance and Work of Breathing, so I am treating respiratory failure. Air entry and interaction are worsening. Airway, lower-airway, parenchymal, impaired-drive, cardiac and toxic causes remain possible. I will support breathing, check reversible causes, reassess the effect and call for senior airway or critical-care help before the exact diagnosis is settled.” [1] [11] [22]
Clinical & Bedside Assessment
Observe, engage, then examine
Keep the child with the caregiver when possible. Observe breathing and interaction before handling, use play or feeding when safe, and examine the least distressing parts first. Distress can change rate, effort and behaviour and can worsen an unstable airway. These steps improve the examination; they must not delay ABCDE in an unstable child. [1] [22]
Age-adapted ABCDE at the bedside
A — Airway
Listen for abnormal sound or silence; assess patency, position, secretion or blood, ability to vocalise and ability to maintain or protect the airway. Avoid upsetting a potentially threatened airway and summon airway expertise early.
B — Breathing
Count rate under stated conditions; assess work, effectiveness, symmetry, air entry, fatigue and credible oxygen-saturation trend. Support breathing and reassess; a saturation does not measure ventilation.
C — Circulation
Integrate pulse rate and quality, skin colour and temperature, technique-stated capillary refill, blood pressure, mental state, urine output, bleeding, access and device function. Do not diagnose a shock type from one sign.
D — Disability
Assess interaction, age-appropriate consciousness, pupils, posture, tone and movement; time seizure activity and check bedside glucose when relevant. Protect airway, breathing and safety while the local pathway is activated.
E — Exposure
Look for rash, injury, bleeding, swelling, device problems and safeguarding evidence while preserving temperature and dignity. Record objective findings and spontaneous words accurately.
D — Disability: exact AVPU and RCH age-adapted pGCS
Use AVPU for a rapid screen: A = Alert; V = Responds to voice; P = Responds to pain; U = Unresponsive. The Royal Children’s Hospital Melbourne altered-conscious-state guideline directs any V, P or U finding to formal Glasgow Coma Scale assessment. Record AVPU and reassess after immediate ABCDE care. Also perform age-adapted pGCS when baseline concern persists despite an apparently Alert screen. Never convert an AVPU letter into an assumed pGCS number. [24] [25]
| Component | Score | RCH child 4 years or older | RCH child under 4 years |
|---|---|---|---|
| Eye opening (E) | 4 | Spontaneously | Spontaneously |
| 3 | To verbal stimuli | To verbal stimuli | |
| 2 | To painful stimuli | To pain | |
| 1 | No response to pain | No response to pain | |
| Best verbal response (V) | 5 | Orientated and converses | Alert; babbles, coos words to usual ability |
| 4 | Confused and converses | Less than usual words, spontaneous irritable cry | |
| 3 | Inappropriate words | Cries only to pain | |
| 2 | Incomprehensible sounds | Moans to pain | |
| 1 | No response to pain | No response to pain | |
| Best motor response (M) | 6 | Obeys verbal commands | Spontaneous or obeys verbal commands |
| 5 | Localises to stimuli | Localises to pain or withdraws to touch | |
| 4 | Withdraws to stimuli | Withdraws from pain | |
| 3 | Abnormal flexion to pain (decorticate) | Abnormal flexion to pain (decorticate) | |
| 2 | Abnormal extension to pain (decerebrate) | Abnormal extension to pain (decerebrate) | |
| 1 | No response to pain | No response to pain | |
| The linked RCH guideline is the source for every descriptor in this table. The cited paediatric comparison studies support only the warning that AVPU categories do not convert exactly to pGCS totals; they do not define these RCH descriptors. [24] [25] |
This is the exact RCH under-4 and 4-or-older implementation, not a universal developmental boundary. Add E, V and M for a total out of 15, but record each component, the total, time and trend because the same total can hide different patterns. Document the child’s usual developmental, communication and neurological baseline. If a component cannot be tested, record why rather than scoring “no response.” Use the locally endorsed chart if it differs. AVPU and pGCS do not replace pupils, posture, tone, movement, glucose assessment or the rest of the neurological examination. [24] [25]
Capillary refill: methods and cut-offs must remain separate
Capillary refill is not a PAT domain. Use it later during C of ABCDE. Record the site, compression time, ambient conditions and local chart, then interpret it with pulse, skin, mental state, urine output and blood pressure. A normal result cannot rule out serious illness. [6] [7]
| Source and purpose | Source-specific rule | Safe use |
|---|---|---|
| Children’s Health Queensland CHQ-NSS-51027 version 2.0, a local Queensland PAT adaptation | Central capillary refill greater than 2 seconds is a local addition | Do not import this into canonical PAT or call it an Australian national rule |
| Fleming measurement review | A specified finger technique uses at least 3 seconds as abnormal under defined conditions | Keep the stated site, compression and environment |
| NHS England National PEWS, general children’s inpatient wards | Records capillary refill at least 3 seconds | Use only within that chart and its response system |
| WHO ETAT, mainly low-resource hospitals | Capillary refill greater than 3 seconds is one of three required shock signs | Do not treat one sign as the complete ETAT shock definition |
Focused history while stabilisation proceeds
Start with the caregiver: “What is different from usual, and what worries you most?” Ask about onset, pace, breathing, feeding, urine output, interaction, sleep and mobility. Then ask about pain, temperature change, rash, collapse, seizure, exposure, trauma, ingestion, medicines, allergies, immunisation and recent healthcare. When relevant, ask privately about pregnancy, substance use, eating restriction and self-harm. Use the child, ambulance staff, records, personal plans and devices as additional sources. Do this in parallel without interrupting life-saving care. [15] [16] [18]
For a child with complex needs, first establish usual communication, behaviour, mobility and pain expression. Then establish usual heart rate, respiratory rate, saturation, respiratory support, feeding, urine output and device function. Ask about recent changes, the emergency plan, limits of treatment and what has worked before. A chronically abnormal observation is not automatically safe; compare it with the personal baseline and trend. [16] [21]
Measurement and synthesis
Heart and respiratory rates change continuously with age. Published ranges differ because studies of healthy children, low-acuity emergency patients and hospitalised children answer different questions. The Royal Children’s Hospital Melbourne acceptable ranges for physiological variables are ranges for unwell children in that setting, not universal normal values. Say whether a number is a reference range, local escalation trigger, disease-risk threshold, treatment target or the child’s baseline. Do not merge them into one universal table. [5]
Use the correct pulse-oximetry probe and site. Check that the waveform or signal is credible, the displayed pulse matches the child and perfusion is adequate. Pulse oximetry may overestimate oxygenation in darker skin. Temperature, lighting and pigmentation also affect visual recognition of pallor, cyanosis and mottling, so examine in good light and combine several sites and signs. [11]
Three time anchors that are safe only with their source attached
After each assessment or treatment, say and document: Is the child stable now? Which ABCDE problem is most urgent? Are they improving or worsening? What differs from baseline? Which reversible causes remain? What did the last action change? Can this service provide the next likely support? Where should the child go? Record the time, conditions and who raised concern. [15] [18] [21]
Investigations
Stabilise first, then order a test for a named question. A useful test finds an immediately reversible cause, measures failing physiology, separates urgent pathways or changes the destination. A normal panel cannot overrule a child who is worsening or remains high risk. [10] [11] [23]
Immediate bedside questions
- Is glucose clinically dangerous in altered consciousness, seizure, shock, poor intake or toxic or metabolic concern?
- Is the oxygen-saturation signal technically credible and concordant?
- Does an ECG identify a rhythm branch?
- Will a gas or lactate quantify failing physiology without delaying support?
- Is a device malfunction creating the deterioration?
Conditional sampling
- Cultures before antimicrobials only when this does not substantially delay time-critical treatment
- Electrolytes, renal or hepatic indices, blood count, inflammatory markers and coagulation only for a defined question
- Targeted toxicology, endocrine or metabolic sampling where the result changes the branch
- Use minimum necessary volume and pain-reduction measures
Targeted imaging
- Chest imaging only if it changes management beyond the clinical assessment
- Ultrasound or echocardiography only within operator and interpretation competence
- Neuroimaging or lumbar puncture only after stability and procedure risk are assessed
- Never move an unstable child to imaging without monitoring, staff, equipment and a rescue plan
Investigation harms
- Delay to airway, breathing or circulation support
- Repeated pain, restraint or blood loss
- Unsafe transport or sedation
- Avoidable radiation
- False-positive and incidental findings that cause low-value treatment
| Test group | Question it can answer | Unsafe inference to avoid |
|---|---|---|
| Blood gas | Whether acid-base state and ventilation are failing, and whether the pattern changes respiratory, circulatory, metabolic or toxic priorities | One gas does not replace the child, serial clinical assessment or a technically appropriate oxygenation measure |
| Lactate | Whether a concerning metabolic or perfusion signal is present and how it changes after treatment | A normal value cannot exclude shock or serious illness; an elevated value does not identify the cause by itself |
| Glucose and electrolytes | Whether an immediately reversible metabolic threat or a cause-specific branch is present | An unexpected point-of-care glucose should be confirmed when feasible, but dangerous-low correction must not wait |
| Blood count and inflammatory markers | Whether the pattern contributes to infection, inflammation, bleeding or marrow questions | Normal or mildly abnormal results cannot independently rule out serious infection in a high-risk or deteriorating child |
| Renal, hepatic and coagulation indices | Whether organ dysfunction, treatment risk or a cause-specific complication is emerging | An early normal result does not cancel worsening physiology; compare age, baseline and trend |
| Cultures and microbiology | Whether a suspected infection can be identified and later therapy refined | Sampling must not substantially delay time-critical antimicrobial treatment |
| Imaging and point-of-care ultrasound | Whether a specific question about structure or organ function changes the immediate branch or destination | Operator limits, transport, radiation, restraint and sedation can outweigh low-probability information |
Glucose: a reversible threat without a universal threshold
Check bedside glucose promptly when the child has altered consciousness, seizure, shock, poor intake, or possible toxic or metabolic illness. If feasible, confirm an unexpected point-of-care result with a blood gas or laboratory sample because meters may be inaccurate at low levels. Do not delay correction of a clinically dangerous low. Use the current age- and context-specific pathway, recheck the glucose and escalate if it does not correct. The named Victorian source is the Royal Children’s Hospital Melbourne hypoglycaemia guideline. This page deliberately gives no universal threshold, agent, dose or infusion. [23]
Imaging and procedures
In typical bronchiolitis, chest radiography rarely changed the clinical diagnosis and was followed by more antibiotic use. NICE NG9 bronchiolitis guidance also advises against routine chest radiography because changes can mimic pneumonia and should not determine antibiotic treatment. This is a bronchiolitis-specific warning, not a ban on targeted imaging in another child. Lumbar puncture, transport-dependent imaging or a sedated procedure is premature when instability makes the procedure or movement unsafe; stabilise and seek senior or specialist input first. [10] [22]
Management — Resuscitation
A worrying doorway assessment starts age-adapted ABCDE immediately. Say that you are concerned, call the appropriate team, name a leader, assign roles, use closed-loop communication, prepare age- and weight-appropriate equipment, and monitor continuously where possible. Treat each problem when found, then reassess from A. History, sampling and cause-specific treatment can proceed in parallel only when they do not delay resuscitation. [1] [13] [18]
Read the figure like this: the child, caregiver and personal baseline stay at the centre. The loop is constant, but exact rules depend on the disease, phase, location and available support. [13] [21]
Check glucose when altered consciousness, seizure, shock, poor intake or toxic or metabolic concern makes it relevant; correct a dangerous low through the local pathway and recheck. Under RCUK 2025 PLS guidance, an ongoing convulsive seizure activates status treatment at 5 minutes. Fluid and vasoactive decisions depend on shock type, available rescue and the local pathway. Resuscitation at birth follows RCUK 2025 NLS guidance. [13] [23]
The first five minutes when the diagnosis is uncertain
Call and organise
State what you see, call senior, resuscitation, airway, critical-care or retrieval help as needed, identify the leader and allocate tasks.
A — Keep the airway open
Position the airway, clear an immediately removable obstruction or secretions, avoid agitating a threatened airway and call airway expertise before failure.
B — Make breathing effective
Use oxygenation or ventilation support from the active pathway. Recheck air entry, work, interaction, credible saturation and fatigue; declare failure early.
C — Support circulation safely
Control obvious loss, gain vascular access without repeated attempts delaying care, consider the likely shock type and risk from fluid, and reassess after every aliquot or action.
D — Protect the brain
Assess consciousness, protect airway and breathing, time any seizure, check glucose when relevant, correct a dangerous low through the local pathway, recheck and escalate non-response.
E — Expose with care
Look for rash, injury and device problems while preventing heat loss, preserving dignity and starting immediate safeguarding actions in parallel.
Reassess from A
Compare the child with the result you expected. Record benefit or harm, revise the differential and move to the next pathway or destination without waiting for a fixed interval.
Emergency working weight when immediate weighing is unsafe
Use a measured weight if it can be obtained immediately without delaying life-saving care. Otherwise announce and document one temporary working weight in kilograms, including its source, method and time. [26]
Follow the local protocol: a recent reliable measured weight or credible caregiver estimate, or the service’s trained length-and-habitus method. RCUK 2025 PLS guidance uses parent or person-with-parental-responsibility report before a habitus-corrected length method in its UK hierarchy. ANZCOR Guideline 12.2 directs clinicians to local charts. Published methods vary in accuracy and are not interchangeable. [26]
Use the declared working weight with the current local paediatric cognitive aid for medicines, fluid, energy and weight-linked equipment. Still check the drug-specific body-size measure and maximum, and confirm equipment fit and function. [26]
Caregiver estimates may be stale, guessed or in the wrong units. Length-and-habitus tools depend on the population, body habitus, device version, technique and training. Total body weight is not correct for every drug or device. Age-only equations are a last local fallback, not an improvised universal formula. Re-weigh at the first safe opportunity, announce the measured value, replace the estimate and recalculate ongoing treatment. [26]
Oxygen: phase, population and jurisdiction must stay attached
RCUK 2025 PLS guidance states that respiratory, circulatory or neurological failure receives 100% oxygen initially, followed by titration. For a previously healthy child it gives a 94–98% target, using the lowest inspired oxygen fraction that achieves at least 94%. These are UK acute-rescue facts. They are not universal targets for post-resuscitation care, ventilation, chronic respiratory support or cyanotic congenital heart disease. Confirm a credible oximeter signal and follow the personal emergency plan and local pathway. [11]
Convulsive seizure: activation begins at 5 minutes
Time the seizure, protect airway and breathing, monitor, check glucose and prevent injury. RCUK 2025 PLS guidance defines a seizure continuing for at least 5 minutes as status epilepticus requiring first-line benzodiazepine treatment. Activate status treatment at 5 minutes; do not wait for two doses to fail. [23]
Circulatory support: source-specific rules are not interchangeable
First decide whether the child has shock using the whole circulation assessment. Consider the likely shock type, whether hypotension is present, whether malnutrition or fluid intolerance increases risk, and whether ventilation, critical care and vasoactive rescue are available. Decide what improvement you expect before giving fluid, reassess after each aliquot, and stop for overload or no benefit. A maximum first-hour volume is a ceiling, not a target. [12] [13] [14]
| Source, population and available critical care | Exact source-specific fluid statement | Boundary that must accompany it |
|---|---|---|
| Surviving Sepsis Campaign 2026, septic shock with intensive-care availability | Up to 40–60 mL/kg in 10–20 mL/kg first-hour boluses | Conditional ceiling; reassess and stop for resolution or overload |
| Surviving Sepsis Campaign 2026, no intensive-care availability | No bolus for sepsis without hypotension; up to 40 mL/kg for hypotensive septic shock | Available critical care and hypotension change the pathway |
| NICE NG254, England and Wales high-risk suspected sepsis | Glucose-free crystalloid 10 mL/kg over less than 10 minutes, maximum 250 mL per bolus; newborn under 28 days 10–20 mL/kg | High-risk pathway only; do not merge with RCUK, SSC, WHO or a local chart |
| WHO ETAT, mainly low-resource hospitals | Shock requires cold extremities, capillary refill greater than 3 seconds and a weak fast pulse; 10–20 mL/kg isotonic crystalloid over 30–60 minutes with reassessment | One or two signs do not trigger rapid infusion; malnutrition differs |
FEAST found increased early mortality with saline or albumin bolus versus no bolus in its African severe-febrile-illness population. It does not prove that all boluses are harmful everywhere; it proves that a high-resource algorithm cannot be exported without regard to population and available rescue resources. If vasoactive support may be needed, activate critical-care or retrieval help in parallel. There is no audit-approved universal timing or first agent for this page; selection, concentration, preparation, access and titration belong to the dedicated shock pathway and local drug chart. [13] [14]
NLS and PLS apply at different times
Use Newborn Life Support (NLS) for resuscitation at birth and support of transition. RCUK 2025 NLS guidance is the official source for that period. During the first hospital stay, local policy defines the NLS-to-PLS boundary while experienced help is called. RCUK 2025 PLS guidance is the corresponding older-child source. [12]
Management — Definitive & Stepwise
After immediate resuscitation, move into the pathway for the likely cause without stopping reassessment. This page does not reproduce full shock, ventilation, status, antimicrobial, toxicology or glucose algorithms. Treat the most reversible dangerous problem first while keeping other serious causes open. [12] [13] [23]
From immediate treatment to the right ongoing plan
Name the expected result
Before acting, state the change you expect in airway patency, breathing effectiveness, interaction, perfusion, urine output or device function.
Measure what happened
Repeat the affected ABCDE areas and observations. Distinguish sustained improvement, brief improvement, no response and harm.
Choose the cause-specific pathway
Move to respiratory support, shock, sepsis, status, toxicology, metabolic, trauma, cardiac or safeguarding care as the evidence becomes clearer.
Stop harmful repetition
Do not repeat treatment because the initial label feels right. Reconsider the cause, fluid overload, access problems and whether more support is needed.
Agree monitoring and contingency
Specify the location, staff, observation intensity, response owner, next sign of failure and what to do if transfer is delayed.
Handover and disposition
Transfer baseline, trend, timed actions, response, unresolved risks, tests, devices, family and safeguarding information, and the next action.
Improvement must make sense across several findings. An open airway must also remain open. Less work of breathing is reassuring only when air entry and interaction improve. Better blood pressure does not prove adequate perfusion. A corrected glucose needs a documented recheck and a plan for the cause. A low PEWS does not cancel concern. Reassess after each action and meaningful change rather than waiting for a universal interval. [7] [8] [12] [23]
Early PICU and retrieval consultation
Call PICU or retrieval when the child may need support your service cannot reliably provide, not after every local option has failed. Discuss the likely support, present monitoring and access, equipment and staff limits, transport time and weather, safest destination, escort, expected deterioration and what to do if transfer is delayed. Exact referral thresholds, escort arrangements, transport mode and accepting service remain local or regional. [21]
| Domain | Content that must cross the boundary |
|---|---|
| Identity and baseline | Age, measured or estimated weight, development, usual observations, communication, function, devices and emergency plan |
| First impression and physiology | PAT pattern, current ABCDE findings, age-adjusted observations and direction of change |
| Actions and response | Intervention, time, route, expected result, actual response and adverse effect |
| Reasoning | Prioritised threat-based differential, key tests, pending results and unresolved risks |
| Local limits | Access, equipment, staff, airway or critical-care limits, transport constraints and requested destination or support |
| Child and family | Caregiver concern, child’s communication needs, professional interpreter, family understanding and preferences |
| Safety | Safeguarding information, objective documentation, immediate safety plan and jurisdictional pathway already activated |
| Contingency | Next failure marker, action if deterioration occurs and named ownership until transfer is complete |
Keep the caregiver present when safe and assign someone to explain what is wrong, what is happening next and what remains uncertain. Speak directly to the child at their developmental level. Use a professional interpreter or communication aid when needed and check understanding. The caregiver’s knowledge of the child is clinical information. [15] [16] [17]
Specific Subtypes & Scenarios
The recognition loop stays the same, but age, presentation, baseline and setting change what you look for and how early you escalate. In each scenario: stabilise first, identify what is failing, activate the correct pathway and state which facts are specific to that source or setting. [1] [12] [16]
Neonate or young infant
- Treat feeding, behaviour, tone, breathing or temperature change as potentially significant even without fever
- Clarify gestation, birth, maternal and transition history
- Seek prompt senior review and check relevant bedside glucose
- Use NLS for resuscitation at birth; keep the first-stay NLS/PLS boundary local
Threatened airway
- Observe sound, position, voice or cry and effort before provoking distress
- Keep the child and caregiver in the position of comfort when safe
- Call airway expertise early
- Do not delay support for diagnostic examination
Breathless child becomes quiet
- Consider fatigue, poorer air entry and falling interaction before assuming improvement
- Reassess effectiveness, not rate alone
- Support breathing and activate the respiratory-support pathway
- Escalate before complete failure
Poor perfusion, cause uncertain
- Keep dehydration, sepsis, cardiac, obstructive, haemorrhagic and mixed physiology open
- Integrate pulses, skin, mental state, urine, blood pressure and technique-stated refill
- Use circulatory support suited to the likely shock type and available rescue
- Do not repeat fluid blindly when response is absent or overload appears
Subtle immunocompromised presentation
- Absence of fever or dramatic inflammatory signs does not close serious infection
- Compare with baseline and recent treatment
- Use targeted sampling without delaying treatment for instability
- Escalate on physiology and risk context
Non-blanching or evolving rash
- Assess ABCDE before completing lesion classification
- Document distribution and evolution objectively
- Keep infection, haematological, inflammatory, traumatic and safeguarding causes open
- Use the active time-critical pathway
Altered behaviour or first seizure
- Protect airway, breathing and safety; time seizure
- Check relevant glucose and correct a clinically dangerous low through the local pathway
- Activate local status care at 5 minutes if convulsions continue
- Keep infection, toxin, metabolic, traumatic and neurological causes open
Trauma with apparent compensation
- Do not wait for hypotension
- Control immediate threats and preserve temperature
- Reassess repeatedly because transport or handling can change physiology
- Consider non-accidental injury when the history or findings require it
Adolescent collapse
- Stabilise first, then create private history time when safe
- Ask directly about substance exposure, self-harm, eating restriction and pregnancy possibility
- Explain confidentiality and its safety limits
- Do not use adult appearance to bypass paediatric baseline, consent or services
Congenital heart disease
- Obtain the individual saturation and circulation baseline
- Use the personal emergency plan and early subspecialty input
- Do not apply a universal oxygen or fluid target
- Consider cardiac and obstructive physiology when the presentation appears respiratory
Technology-dependent child
- Assess the child and the device in parallel
- Ask what normal device function looks and sounds like
- Use the personal emergency and manufacturer or specialty pathway
- Bring caregiver expertise into the escalation and handover
Severe neurodisability
- Establish usual interaction, tone, movement, pain and autonomic signs
- Adapt sensory input and communication
- Treat caregiver-described change as evidence
- Do not claim that adaptation has validated diagnostic sensitivity
Possible poisoning
- Stabilise physiology while substance, dose and time remain uncertain
- Seek containers, medication lists and collateral information
- Use targeted ECG, glucose or toxicology questions when they change the branch
- Activate the local toxicology pathway
Rural or remote clinic
- Call retrieval before the child needs support unavailable locally
- State equipment, staff, weather, distance and communication limits
- Agree a delayed-transfer contingency and reassessment schedule driven by acuity
- Package monitoring, access and handover for transport
Telehealth
- PAT evidence is sparse in remote assessment
- Video cannot reliably replace palpation, air entry, perfusion measurements or device verification
- A poor connection or uncertain examination lowers the threshold for in-person review
- Give a specific access route and contingency, not a generic reassurance
Repeated caregiver concern
- Restart assessment rather than defending the previous decision
- Ask what has changed and what was missed
- Escalate despite a low score when concern and direction of change remain discordant
- Review safeguarding and the feasibility of the safety net
Complications & Pitfalls
Most harm begins when assessment stops too early. A normal number, convenient explanation or brief response is accepted as the answer, so the child is not reassessed. Prevent this by recording the current problem, serious alternatives, intended result, actual response and next escalation action. [7] [8] [18]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Normal PAT or low PEWS ends assessment | Occult or evolving illness and baseline exceptions are missed | Continue age- and risk-specific assessment; respond to concern and trend |
| Blood pressure or capillary refill used alone | Compensation and poor sensitivity create false reassurance | Integrate multiple perfusion signs, technique and direction of change |
| Quieter breathing labelled recovery | Fatigue and falling air entry may be misread | Seek concordant improvement in effectiveness and interaction |
| Abnormal observations attributed to fever, crying, pain or anxiety | A plausible modifier becomes premature closure | Reassess after comfort and explain persistent abnormalities |
| Adult norms, equipment or assumptions | Age, weight, reserve and consent are ignored | Use exact age, weight estimate, local paediatric charts and trained support |
| Repeated distressing examination or access attempts | Physiology and assessment validity worsen while treatment is delayed | Observe first, sequence least-distressing steps and escalate access expertise |
| Oxygen, fluid or vasoactive rule transferred between contexts | Disease phase, shock type, available rescue and baseline differ | Name source, population, phase and stop rule beside every rule |
| Imaging or procedure before stability | Transport, sedation, restraint or delay can destabilise | Ask whether the result changes the immediate branch and whether movement is safe |
| Caregiver or nursing concern discounted | Baseline change and early deterioration information are lost | Elicit, document and provide escalation irrespective of score |
| Poor referral or shift handover | Timed actions, response and contingencies disappear | Use structured transfer with read-back and named ownership |
| Safeguarding postponed until diagnosis | Immediate safety and evidence may be lost | Stabilise first while objective documentation and the local pathway proceed in parallel |
| Transient response accepted as diagnosis | Mixed or alternative causes remain hidden | Treat response as a trend; repeat full synthesis |
At handover, watch for anchoring on the previous diagnosis, choosing tests only to confirm it, carrying forward the referral label and hierarchy that silences bedside concern. PAT followed by ABCDE and reassessment helps only if the team is willing to revise its view when the child or trend does not fit. [8] [18]
After stabilisation, look actively for harm from treatment. Check airway or access complications, fluid overload, heat loss, repeated sampling, medication or device error, and pressure or restraint injury. Also look for deterioration during movement. The fact that the child did not arrest does not prove an intervention or transfer was harmless. [14] [21]
Prognosis & Disposition
Disposition follows the trend and response, not one reassuring observation. Consider the child’s age, reserve, underlying disease and the duration and severity of organ dysfunction. Then consider reversibility, treatment harm, local support, transport risk and whether the family can carry out the plan. There is no universal observation time or PICU threshold on this page. [12] [19] [21]
Critical care or retrieval
- Unresolved or worsening ABCDE threat
- Need for support, monitoring or expertise unavailable locally
- Repeated or transient response with likely further deterioration
- Transport risk that requires early specialist planning
Ward, high-dependency or observation
- Physiology currently supported but trend, age, diagnosis or baseline needs close reassessment
- Monitoring and staffing can detect and respond to failure
- Pending tests or treatment response still change disposition
- A named escalation pathway exists
Discharge only when defensible
- Sustained improvement or stability after appropriate reassessment
- No unresolved immediate threat or high-harm diagnostic concern
- Caregiver concern addressed and understanding confirmed
- Specific warning changes, access route, follow-up and pending-result ownership agreed
A useful safety net says what change to watch for, how urgently to act, and exactly where or how to get help. It also states when review will occur, who owns pending results and what to do if access is difficult. NICE fever-in-under-5s guidance provides an England-and-Wales example. “Return if worried” alone is not enough. No leaflet, video, call-back interval or follow-up time is best for every child. Check understanding with teach-back or another method and document it. [19]
Before the child leaves your care
Reassess the direction of change
Repeat the relevant PAT and ABCDE domains under stated conditions and compare with baseline and the expected result.
Close unresolved loops
Name residual diagnostic risk, pending results, medication or device changes and who will act on each.
Make access executable
Give warning changes, urgency, destination or contact route and a contingency for transport, language or cost barriers.
Check understanding
Speak to the child at the appropriate level, use professional language access when needed and confirm caregiver understanding.
Connect follow-up
Involve the medical home, primary care, community nursing or subspecialty team according to the child’s needs and personal plan.
After a critical event, explain what happened and what remains uncertain. Invite questions and caregiver observations, and consider debriefing for the child, family and team when appropriate. [18]
Recurrent presentation or unexplained deterioration needs senior diagnostic review and may need safeguarding reassessment. [20]
For young people moving to adult services, transfer the baseline, devices, emergency plan, capacity and caregiver roles instead of rebuilding them during the next crisis. [16]
Special Populations
Adapt how you observe, communicate and examine, but do not lower the standard for recognising deterioration. Evidence is sparse for recognition tools in disability, neurodiversity, technology dependence, telehealth and many low-resource settings. Present these adaptations as safer communication and assessment practices, not as proven improvements in diagnostic accuracy. [3] [16]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Premature, ex-premature, neonate | Use gestation, birth and transition history; compare feeding, tone, temperature, breathing and personal baseline; keep NLS birth-transition rules distinct | Do not import older-child pathways into birth transition |
| Immunocompromised | Lower threshold for senior assessment when physiology or baseline changes despite attenuated signs; use treatment history and targeted testing | Absence of fever cannot independently reassure |
| Congenital heart disease, pulmonary hypertension or palliative plan | Use individual saturation, circulation, device and escalation plan; involve the usual team early | No universal oxygen, fluid or disposition target |
| Complex chronic or technology-dependent child | Assess child and device together; use caregiver expertise, baseline and emergency plan; hand over device details | Do not label chronic abnormal observations either normal or acute without trend |
| Disability, neurodiversity or sensory difference | Adapt environment, sequence, pain cues and communication; use assistive methods and usual behaviour | Adaptation is required, but validated sensitivity gain is not established |
| Aboriginal and Torres Strait Islander child and family | Ask what culturally safe communication, family participation and connection to Country require; address distance and access without stereotype | Culture never replaces individual history or physiology |
| Māori child and whānau | Support whānau participation and relevant local tikanga as defined by the child and whānau; verify Aotearoa service pathways | Do not treat Māori children and whānau as homogeneous |
| Migrant, refugee or asylum-seeking family | Use a professional interpreter, clarify records, immunisation and exposure history, and acknowledge trust and access barriers | A family member should not interpret a safeguarding conversation |
| Out-of-home care or youth justice | Verify caregiver authority, consent route, records and safeguarding coordination while urgent care proceeds | Legal and agency routes are jurisdiction-specific |
| Gender or sexual diversity and confidential adolescent care | Address the young person directly, offer privacy when safe and explain confidentiality and safety limits | Do not let social history distract from urgent ABCDE problems |
| Maltreatment or family violence | Stabilise first; use non-leading necessary questions, objective documentation and the active safeguarding pathway | Reporting thresholds and agencies vary by jurisdiction |
| Socioeconomic disadvantage or housing and transport insecurity | Design a safety net and follow-up the family can enact; state a contingency when access fails | A theoretically correct plan is unsafe if it is inaccessible |
Professional interpreters improve included outcomes compared with ad hoc or no interpretation, although the evidence covers limited populations and delivery methods. Speak directly to the child in developmentally appropriate language, state the immediate concern and next action, acknowledge uncertainty and check understanding. An interpreter or communication aid is a safety measure, not a courtesy. [17]
Safeguarding runs in parallel with medical care, but immediate stabilisation and safety come first. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words accurately, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [20]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
PAT gives a consistent rapid first impression, and trained staff can use it. Its reliability and validity still vary with the domain, rater, training, setting, exclusions and outcome studied. There is no justified single pooled sensitivity, specificity, area under the curve or kappa for all settings. Neonates, older adolescents, remote and low-resource care, and children with complex baselines remain under-represented. A normal PAT cannot exclude serious infection or evolving disease. [2] [3] [4]
PEWS tools differ and depend on the chart, complete observations, training, staffing, response system and governance. Positive predictive value may be low. The EPOCH cluster randomised trial found no reduction in all-cause hospital mortality after BedsidePEWS implementation. Teach the full recognition-and-response system, not the score alone. Clinician or caregiver concern can justify escalation despite the number. [8] [9] [15]
There is no justified universal vital-sign range, PEWS chart, capillary-refill method, oxygen target, glucose threshold, fluid strategy, vasoactive timing, retrieval trigger, safeguarding route, handover mnemonic, observation interval or safety-net medium. Attach each rule to its population, purpose, conditions, jurisdiction and available support. Where evidence is weak, say so rather than inventing precision. [5] [6] [8] [13] [19] [21] [23]
EPOCH
JAMA
Cluster randomised trial of BedsidePEWS implementation in hospitalised children
Key finding
The intervention did not reduce all-cause hospital mortality.
Practice change
Do not equate prediction or implementation with proven mortality benefit; evaluate the complete local response system.
FEAST
New England Journal of Medicine
Randomised fluid-bolus trial in African children with severe febrile illness
Key finding
Saline or albumin bolus increased 48-hour mortality compared with no bolus in that population.
Practice change
Fluid strategy must remain specific to the population, shock type and available rescue; do not transplant protocols uncritically.
Caregiver concern has a strong recent signal, but it comes from one Australian hospital cohort and does not establish a universal likelihood ratio or response tier. Evidence supports professional interpretation but remains limited. Adaptations for complex children and disability are clinically necessary, although direct diagnostic-accuracy evidence is sparse. Pulse-oximetry disparity across skin colour is credible; this page offers no correction factor. [11] [15] [16] [17]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Australian national deterioration standard requires individual monitoring and graphical trends. Locally agreed criteria must include worry and direct patient or family escalation. The standard does not mandate one national paediatric score. [8] [15]
ANZCOR Guideline 12.2 is the 2026 regional PALS source. Retrieval, observation charts, mandatory reporting, consent and exact escalation routes remain state-, territory-, district- or service-specific. In Aotearoa New Zealand, verify the active local deterioration, retrieval and safeguarding system rather than borrowing an Australian threshold. [8] [15] [21]
Global and low-resource settings: WHO ETAT is designed mainly for low-resource hospitals and non-specialists. [14]
The WHO ETAT three-sign shock definition and slower fluid approach must remain attached to that population. FEAST explains why apparently familiar interventions can change effect when population and available rescue resources change. [14]
Board and assessment distinctions
RACP current PREP curriculum candidates in 2026 must keep those learning objectives separate from the renewed curriculum for new first-year trainees from 2027. [1]
RCPCH Progress+ outcomes are curriculum expectations; MRCPCH FOP, TAS and AKP are theory classifications, while Clinical History, Communication, Video and short clinical stations are assessment formats. [15] [17]
The 2024 public MRCPCH face-to-face normal circuit describes two Communication and two Video stations of 9 minutes each; do not invent marks, pass standards or confidential station content. The clinical reason to preserve these distinctions is that concern, communication access and family escalation are evaluated in different instruments, not interchangeable scores. [15] [17]
The RACP General Paediatrics specialty-development page is the implementation source for that 2026-to-2027 transition; the RCPCH Generic Syllabus for Specialty Paediatric Training provides the specialty-level board mapping used alongside Progress+. [18]
The ABP General Pediatrics Content Outline classifies written examinations; ABP Core EPAs are workplace activities. [18]
ACGME Pediatrics Milestones and the 2026 Program Requirements govern residency development and accreditation, not ABP certification. Milestone Level 4 is a goal, not an automatic graduation or certification requirement. [18]
RCPSC Transition to Discipline EPA 1 and Foundations EPA 1 separate the basic history, examination and presentation task from deterioration recognition and initial stabilisation. Structured handover and transfer planning based on available support remain clinically important across these frameworks. [18] [21]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Interpret an age-adapted vignette and trend, identify the dominant threat and choose the safest next action without waiting for a diagnosis |
| RACP DCE long case | Integrate baseline, physiology, comorbidity, development, devices, family impact, psychosocial context and immediate plus longitudinal plan |
| RACP DCE or MRCPCH short clinical | Observe and examine breathing, perfusion and interaction, describe technique and summarise severity plus differential |
| MRCPCH History and Communication | Elicit caregiver concern and age-specific risk; explain urgent escalation and uncertainty using developmentally appropriate language |
| MRCPCH Video | Describe PAT observations, state what video cannot assess and give the next in-person action |
| ABP | Apply content domains and universal tasks in written assessment; distinguish these from workplace EPAs |
| ACGME | Demonstrate developmental milestones in clinical reasoning, patient management, safety, transitions and communication |
| RCPSC structured oral | Recognise evolving instability, stabilise, seek assistance, reassess and hand over across tertiary or rural contexts |
Exam Pearls
Doorway
- Observe before touch
- Name PAT domains objectively
- Declare whether help is needed now
- Do not diagnose from PAT
Primary survey
- ABCDE and treat threats as found
- Use age, weight and personal baseline
- Check immediately reversible threats
- Repeat from A after intervention
Reasoning
- Prioritise threat, likelihood, reversibility and harm from delay
- Keep PAT pattern and cause separate
- Use targeted tests only if they change the branch
- Treat response as trend, not proof
Escalation
- Call PICU or retrieval before the child needs support unavailable locally
- State failure markers and contingency
- Give structured handover
- Preserve family and safeguarding information
Boundaries
- No harmonised CRT
- No blended oxygen or fluid rule
- Status pathway at 5 minutes
- No universal glucose threshold
- NLS at birth
Disposition
- Require sustained improvement or stability
- Resolve pending-result ownership
- Give warning, urgency, access and follow-up
- Check understanding
“PAT first impression → help if threatened → age-adapted ABCDE with treatment → targeted reversible-threat checks → immediate reassessment → escalation based on available local support, structured handover and safe disposition.”
Viva: the tachypnoeic child becomes quiet
Do not say “improved” until breathing effectiveness is reassessed. Recheck Appearance and full ABCDE, including air entry, work, respiratory rate under stated conditions, credible saturation, interaction, perfusion and glucose when relevant. Less effort with poorer air entry or interaction means fatigue and impending failure. Call airway or critical-care help, support breathing through the active pathway, state the improvement you expect and reassess from A. [11] [12] [22] [23]
Viva: concern exceeds the PEWS
Say: “The score is one input. I am concerned because interaction, breathing or perfusion and the direction of change differ from baseline, and the caregiver reports deterioration. I am escalating now through the clinician- or family-concern route while I repeat ABCDE and verify the observations.” A low score cannot cancel a high-risk presentation, worsening trend or baseline exception. [8] [9] [15]
Structured oral: rural retrieval
State the current ABCDE problem and treatment already under way. Ask what monitoring, airway, vascular-access, staff and transport resources are available. Call retrieval early, agree the destination, treatment to continue, expected response, deterioration plan and handover, and explain uncertainty and transport delay to the family. Do not invent a universal threshold or wait until all local options have failed. [18] [21]
References
- [1]Dieckmann, Ronald A The pediatric assessment triangle: a novel approach for the rapid evaluation of children. Pediatric emergency care, 2010.PMID 20386420
- [2]Horeczko, Timothy The Pediatric Assessment Triangle: accuracy of its application by nurses in the triage of children. Journal of emergency nursing, 2013.PMID 22831826
- [3]Tørisen, Tore A G Emergency pediatric patients and use of the pediatric assessment triangle tool (PAT): a scoping review. BMC emergency medicine, 2024.PMID 39227775
- [4]Gomez, B Bacteremia in previously healthy children in emergency departments: clinical and microbiological characteristics and outcome. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology, 2015.PMID 25252630
- [5]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [6]Fleming, Susannah Validity and reliability of measurement of capillary refill time in children: a systematic review. Archives of disease in childhood, 2015.PMID 25260515
- [7]Fleming, Susannah The Diagnostic Value of Capillary Refill Time for Detecting Serious Illness in Children: A Systematic Review and Meta-Analysis. PloS one, 2015.PMID 26375953
- [8]Trubey, Rob Validity and effectiveness of paediatric early warning systems and track and trigger tools for identifying and reducing clinical deterioration in hospitalised children: a systematic review. BMJ open, 2019.PMID 31061010
- [9]Parshuram, Christopher S Effect of a Pediatric Early Warning System on All-Cause Mortality in Hospitalized Pediatric Patients: The EPOCH Randomized Clinical Trial. JAMA, 2018.PMID 29486493
- [10]Schuh, Suzanne Evaluation of the utility of radiography in acute bronchiolitis. The Journal of pediatrics, 2007.PMID 17382126
- [11]Sharma, Megha Racial and skin color mediated disparities in pulse oximetry in infants and young children. Paediatric respiratory reviews, 2024.PMID 38233229
- [12]Bjorklund, Ashley Pediatric Shock Review. Pediatrics in review, 2023.PMID 37777656
- [13]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844
- [14]Maitland, Kathryn Mortality after fluid bolus in African children with severe infection. The New England journal of medicine, 2011.PMID 21615299
- [15]Mills, Erin Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [16]Kuo, Dennis Z Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [17]Boylen, Susan Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [18]Starmer, Amy J Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [19]Burvenich, Ruben Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [20]Bragança-Souza, Kátia Kely Health Professionals: Identifying and Reporting Child Physical Abuse-a Scoping Review. Trauma, violence & abuse, 2024.PMID 36747372
- [21]Chaichotjinda, Krittiya Assessment of interhospital transport care for pediatric patients. Clinical and experimental pediatrics, 2020.PMID 31477679
- [22]Shah, Sonal N Does This Child Have Pneumonia?: The Rational Clinical Examination Systematic Review. JAMA, 2017.PMID 28763554
- [23]Faustino, E Vincent S Hypoglycemia in critically ill children. Journal of diabetes science and technology, 2012.PMID 22401322
- [24]Hoffmann, Florian Comparison of the AVPU Scale and the Pediatric GCS in Prehospital Setting. Prehospital emergency care, 2016.PMID 26954262
- [25]Ramgopal, Sriram Comparing AVPU and Glasgow Coma Scales Among Children Seen by Emergency Medical Services. Pediatrics, 2024.PMID 38993159
- [26]Young, Kelly D Weight Estimation Methods in Children: A Systematic Review. Annals of emergency medicine, 2016.PMID 27105839
- [27]McIntyre, John Safety and efficacy of buccal midazolam versus rectal diazepam for emergency treatment of seizures in children: a randomised controlled trial. Lancet (London, England), 2005.PMID 16023510