Paeds · clinical-pharmacology-and-therapeutics
Adverse drug reactions and pharmacovigilance
Also known as Adverse drug reactions in children · ADR classification and causality · Drug allergy and hypersensitivity in children · Spontaneous reporting and VigiBase · Paediatric pharmacovigilance
A fellowship approach to adverse drug reactions and pharmacovigilance in children: Rawlins and Thompson Type A/B classification with DoTS and EIDOS extensions, paediatric epidemiology, immune and non-immune mechanisms, recognition, Naranjo causality and Hartwig severity assessment, management from stopping the drug through anaphylaxis and SJS/TEN, and the reporting pathway from TGA, MHRA Yellow Card and FDA MedWatch to WHO VigiBase across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old who, ten days into a course of an anticonvulsant for new epilepsy, develops a blistering rash with mouth ulcers and fever. That child is the reason adverse drug reactions and pharmacovigilance exist as a discipline. The reaction is not a side effect to shrug off, and it is not bad luck — it is a predictable, serious hazard of a medicine used at a normal dose, and recognising it fast is what separates a safe prescriber from a dangerous one. [1]
The World Health Organization defines an adverse drug reaction as a response to a medicine that is noxious and unintended, occurring at doses normally used in humans. The key phrase is "normally used" — it excludes deliberate overdose and error, which sit in the related but distinct territory of adverse drug events and medication errors. [1] An adverse drug event is broader: any injury from a medicine whether or not the dose was correct, so it captures both true ADRs and harm from mistakes. A medication error is the process failure itself — wrong drug, wrong dose, wrong route, wrong patient — that may or may not reach the child and may or may not cause harm.
This distinction matters at the bedside and in the exam. A child harmed by a ten-fold dosing error has suffered an adverse drug event caused by a medication error, not an ADR. A child who develops anaphylaxis to a correctly given first dose of an antibiotic has suffered an ADR. Both deserve reporting and prevention, but the mechanism, the learning, and the regulatory response differ. [1]
Pharmacovigilance is the science and the activities concerned with detecting, assessing, understanding and preventing adverse effects of medicines. It begins at the bedside with one clinician who suspects a reaction and reports it, and it ends in a global system that compares millions of reports to find signals no trial could ever detect. Children sit at the heart of the problem and the opportunity: they are rarely included in premarketing trials, so most medicines reach them with thin paediatric evidence, and the first signs of harm often appear only after the drug is in widespread use. [7] [8]
Classification
Once you suspect an ADR, the next question an examiner asks is "what type?" The oldest and most exam-friendly system is the Rawlins and Thompson division into Type A and Type B reactions, later extended into the alphabet of Types C through F. The contrast is the whole point, and it is worth holding as a clean pair. [1]
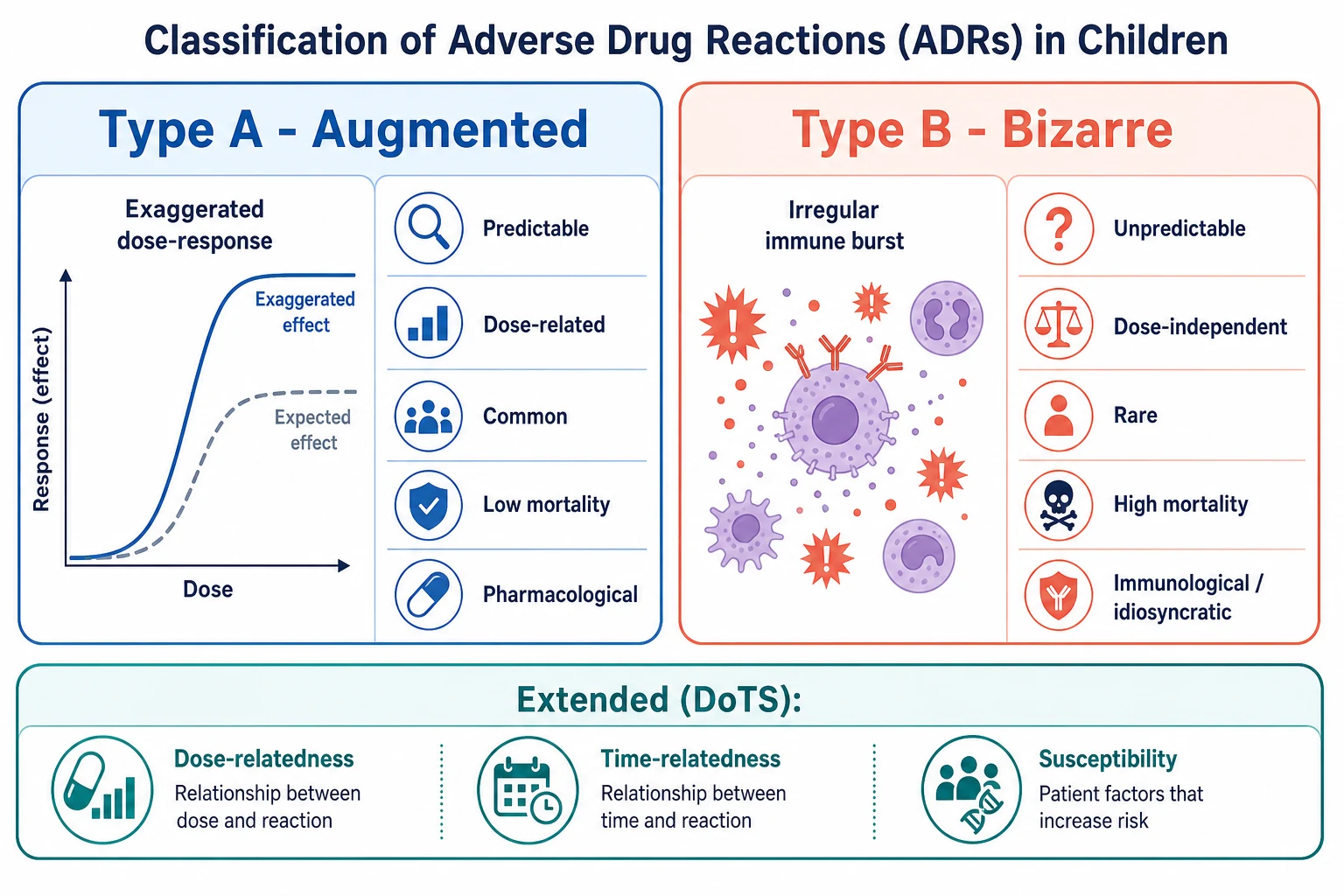
Type A stands for "augmented" — the drug does exactly what it is supposed to do, but too much. Think of opioid-induced respiratory depression, beta-agonist tachycardia, or the sedation that follows a benzodiazepine. These reactions are predictable from the pharmacology, dose-related, common, and usually carry low mortality. They are also the ones developmental pharmacokinetics makes more dangerous in infants, whose immature metabolism and clearance exaggerate the effect of a "normal" dose. [1]
Type B stands for "bizarre" — the reaction is qualitatively unlike the normal pharmacology and is not predicted by it. Anaphylaxis to a first dose of penicillin, the rash of carbamazepine-induced Stevens-Johnson syndrome, or the haemolysis of a G6PD-deficient child given oxidant drugs all belong here. These reactions are unpredictable, largely dose-independent, rare, and — when they are severe cutaneous or systemic reactions — carry high morbidity and mortality. [1]
Type A — Augmented
- Mechanism: exaggerated primary pharmacology
- Predictable from drug action
- Dose-related
- Common
- Usually low mortality
- Example: opioid respiratory depression, beta-agonist tachycardia
Type B — Bizarre
- Mechanism: immune-mediated or idiosyncratic
- Unpredictable
- Largely dose-independent
- Rare
- Potentially high mortality
- Example: anaphylaxis, SJS/TEN, DRESS, G6PD haemolysis
The alphabet extends further, and a candidate should recognise each letter. Type C (chronic or continuous) arises from long-term use — corticosteroid osteonecrosis or adrenal suppression. Type D (delayed) appears long after exposure, classically carcinogenesis or growth suppression. Type E (end-of-use) is the rebound or withdrawal that follows stopping a drug, such as opioid or benzodiazepine withdrawal in a neonate. Type F (failure of therapy) is unexpected therapeutic failure, often from a drug interaction or formulation problem. [1]
The modern mechanistic classification that examiners increasingly expect is DoTS, which reads each reaction across three axes rather than forcing it into a single letter. Dose-relatedness asks whether the reaction fits a standard, low, or high dose-response. Time-relatedness asks whether it is early, intermediate or late, or whether it depends on cumulative dose. Susceptibility asks what makes this child vulnerable — age, genotype, organ function, disease, and interacting drugs. DoTS does not replace Type A/B; it explains why a single reaction can be dose-related in one axis and time-dependent in another, which is exactly the nuance a viva probes. [1]
Epidemiology & Risk Factors
Ask how often ADRs really happen in children and the honest answer is "more often than most prescribers think." The most cited systematic review of prospective studies found an overall incidence around 9.5 percent of paediatric inpatients and a higher figure among the seriously ill. [3] A later review of prospective studies and safety alerts confirmed that ADRs are a leading source of iatrogenic harm in childhood and that the burden is concentrated in particular settings and particular children. [4]
The children most at risk share recognisable features. Neonates and young infants have immature hepatic metabolism (reduced glucuronidation), lower glomerular filtration, reduced protein binding, and a more permeable blood-brain barrier, so a dose that is safe at two years can be toxic at two weeks. Children who are seriously ill, in intensive care, or on chemotherapy are exposed to high-risk drugs at high intensity. Those on polypharmacy, particularly children with medical complexity and technology dependence, accumulate interactions and additive toxicity. And a consistent and important theme runs through the evidence: off-label and unlicensed medicines are over-represented among paediatric ADRs, a finding shown clearly in a nested case-control study of inpatients. [6] [5]
The drug classes that cause ADRs in children are familiar. Antibiotics (especially penicillins, cephalosporins and sulfonamides) dominate both community and hospital reports and are the commonest single cause of ADR-related admission. Anticonvulsants (notably lamotrigine, carbamazepine and phenytoin) account for a disproportionate share of severe cutaneous reactions. Non-steroidal anti-inflammatories, opioids, psychotropics, and chemotherapy agents each carry their own characteristic adverse-effect profile. VigiBase data show that worldwide, antibiotics, nervous-system drugs, and anti-inflammatory agents head the list of suspected paediatric reports. [7] [11]
Under-reporting is the hidden tax on all of this. A systematic review of under-reporting of ADRs found a median around 94 percent across settings — meaning that for every hundred ADRs that actually occur, only a handful reach a database. [9] This is why every clinician's report matters, and why the absence of a published signal is never proof of safety.
Pathophysiology
Why does a medicine that heals one child harm another? The mechanism splits cleanly along the same line as the classification. Type A reactions are pharmacology gone too far, and Type B reactions are biology gone wrong — usually an immune response, sometimes an idiosyncratic vulnerability. [1]
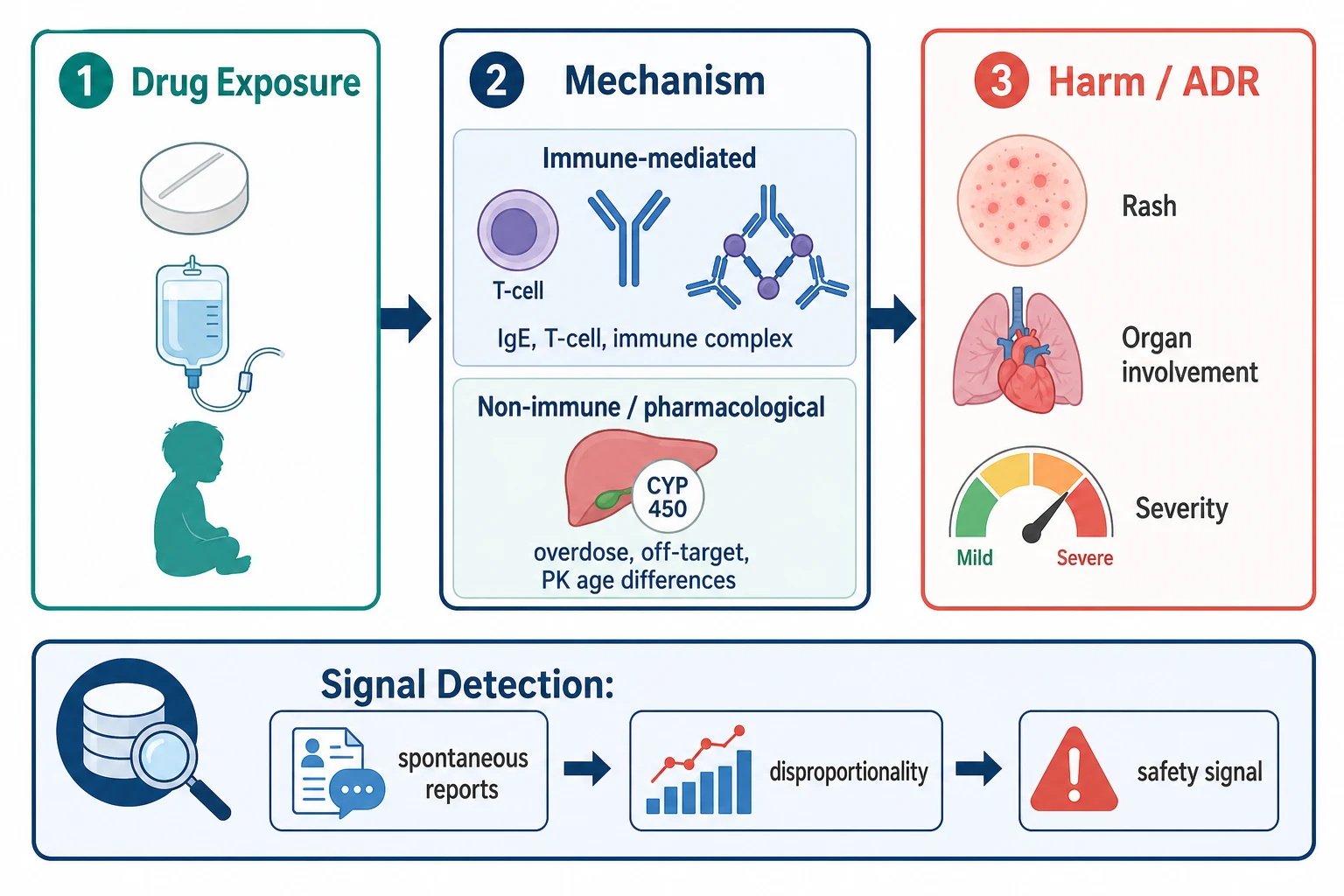
Type A reactions amplify the drug's known action. The dose-response curve is simply shifted into the harmful range, most often because exposure is higher than intended. In an infant whose cytochrome P450 enzymes are still maturing and whose renal clearance is low, a "normal" milligram-per-kilogram dose can accumulate until it behaves like a slow overdose. Drug-drug interactions amplify this: a CYP inhibitor raises exposure to a substrate, and the predictable pharmacology becomes predictable toxicity. The teaching point is that Type A harm is preventable with attention to weight, age, organ function and interactions. [1]
Type B reactions run through the immune system or through a fixed metabolic vulnerability. The Gell and Coombs framework still organises the immune types: Type I (IgE-mediated) gives anaphylaxis, urticaria and angioedema within minutes to hours; Type II (cytotoxic antibody) gives drug-induced cytopenias; Type III (immune complex) gives serum sickness-like reactions and vasculitis; and Type IV (T-cell mediated) underlies the delayed maculopapular exanthem and, more dangerously, the severe cutaneous adverse reactions. The idiosyncratic, non-immune Type B reactions include G6PD-deficiency haemolysis after an oxidant drug and the paradoxical reactions that some genotypes produce. [1]
The severe cutaneous adverse reactions deserve a paragraph of their own because they are the ones that kill or maim and because they cluster in identifiable children. Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are now understood as Type IVc and IVd T-cell reactions in which drug-specific cytotoxic T cells and their mediators (notably granulysin) drive keratinocyte apoptosis and skin detachment. DRESS (drug reaction with eosinophilia and systemic symptoms) is a Type IVb reaction that typically appears two to eight weeks after a new drug and can involve liver, kidney, lung and heart. The single best-known pharmacogenomic story in paediatric ADRs is carbamazepine-induced SJS/TEN, which is strongly associated with the HLA-B*15:02 allele carried at high frequency in Han Chinese and Southeast Asian populations — a finding that converted a "bizarre" reaction into a predictable and screenable one. [1]
How does a single child's reaction become a safety signal the world acts on? Each report enters a database where the frequency of the drug-event combination is compared with what would be expected by chance, using disproportionality measures such as the proportional reporting ratio or the reporting odds ratio. A reporting imbalance that is statistically robust and clinically plausible becomes a signal, which is then assessed, confirmed or refuted, and — if confirmed — translated into a label change, a contraindication, or a market withdrawal. Children generate signals that adult trials miss precisely because they were never studied, which is why paediatric reporting is not optional. [8]
Clinical Presentation
The first presentation of an ADR is rarely labelled as one. A febrile child on antibiotics is thought to have a "drug fever or a virus"; a drowsy child on opioids is thought to be "tired." The discipline of pharmacovigilance begins with a low threshold: any new symptom that follows the start of a medicine, and any worsening of an existing one, earns an ADR on the differential until you have actively excluded it. [1]
Cutaneous reactions are by far the commonest paediatric ADR and range from the trivial to the lethal. A simple exanthem is usually benign. Urticaria and angioedema suggest immediate hypersensitivity and raise the question of anaphylaxis. Fixed drug eruptions recur at the same site with each exposure. The red flags are blistering, mucosal involvement, skin pain, and skin detachment — the hallmarks of SJS and TEN. A rash that appears with fever, facial oedema, lymphadenopathy, eosinophilia or liver dysfunction two to eight weeks into a new anticonvulsant or antibiotic points to DRESS. [1]
Systemic ADRs present by organ. Anaphylaxis arrives within minutes to hours of a dose, with respiratory compromise (wheeze, stridor, hypoxia), hypotension or collapse, and skin change such as urticaria or angioedema. Drug-induced liver injury presents with nausea, jaundice and transaminitis. Haematologic ADRs present as neutropenia, thrombocytopenia or aplastic anaemia and are easily misattributed to infection. Neurologic ADRs — sedation, ataxia, tremor, extrapyramidal signs, or new seizures — are particularly common in infants because the blood-brain barrier and hepatic clearance are immature. [1]
Neonates present differently and dangerously. Chloramphenicol in a neonate with immature glucuronidation produces grey baby syndrome: grey discolouration, abdominal distension, cardiovascular collapse and death. Historical lessons such as kernicterus from sulphonamide displacement of bilirubin, and gasping syndrome from benzyl alcohol in flushes, shaped modern neonatal prescribing. The message is that a neonate's reaction may be systemic, delayed, and unlike anything seen in older children, so developmental pharmacokinetics must always be in mind. [10]
Type E (end-of-use) reactions present as withdrawal. An infant who has received opioids or benzodiazepines for prolonged intensive care may develop irritability, tremor, seizures and autonomic instability when the drug is stopped — neonatal abstinence syndrome. Recognising this as an ADR rather than new disease prevents a cascade of unnecessary investigation and points to a structured weaning plan. [10]
Differential Diagnosis
The central skill in the differential is separating drug-caused from disease-driven. A fever on day five of antibiotics may be the infection, may be the drug, or may be a new infection; a rising creatinine on a nephrotoxic combination may be the underlying illness or the regimen. The tools that separate them are temporal relationship, dechallenge (does it improve when the drug stops), rechallenge (does it recur when it restarts — never deliberate after a serious reaction), and whether an alternative cause explains the picture better. [1]
Drug rash
- Temporal link to a new drug
- Improves on dechallenge
- Eosinophilia or systemic features in DRESS
- Mucosal involvement and detachment in SJS/TEN
- Often polymorphous: morbilliform, urticarial, targetoid
Viral exanthem
- Prodrome of fever and coryza
- Typical distribution and evolution
- Concurrent viral illness in family
- No clear drug dechallenge relationship
- Often self-limited over days
Several specific distinctions earn their place in the differential because they are commonly confused. SJS and TEN must be separated from staphylococcal scalded skin syndrome (superficial peeling, no mucosal involvement, positive Nikolsky but intact deeper skin), Kawasaki disease (prolonged fever, conjunctivitis, strawberry tongue, coronary risk), and severe viral exanthem. Drug-induced liver injury must be distinguished from viral hepatitis and sepsis by serology, timing and the drug history. Anaphylaxis must be separated from an asthma exacerbation, a vasovagal episode (bradycardia and pallor rather than hypoxia and urticaria), and hereditary angioedema (often a family history, no urticaria, complement C4 low). [1]
A prescribing cascade is the pitfall in which the ADR of one drug is diagnosed as a new disease and treated with a second drug. The child who becomes constipated on an opioid receives a laxative, who then becomes dehydrated and receives fluids, all of which could have been avoided by anticipating the opioid effect. The differential question to hold is: "is this new symptom the disease, or is it the treatment?" [1]
Finally, avoid two opposite errors. Do not over-label a child as "allergic" on the basis of a non-immune side effect or a viral rash — a penicillin label persists for life and denies the child first-line antibiotics. And do not under-attribute a severe reaction to "disease progression" while continuing the causative drug. Both errors are common and both are preventable. [1]
Clinical & Bedside Assessment
Bedside assessment of a suspected ADR follows a tight sequence: stabilise, take a complete drug history, characterise the reaction, and grade its severity. The history is the single highest-yield step, because most ADRs are diagnosed by their temporal pattern rather than by any laboratory test. [1]
Build the drug history deliberately and do not stop at the prescription chart. Ask about every medicine the child actually takes — prescribed, over-the-counter, herbal, vitamin, and medicines shared in the household — and include recently stopped drugs, because a Type E reaction can follow withdrawal. Record each one with its dose, route, frequency, indication, start date and last dose. For liquids, confirm the concentration and the measuring device, because volume without concentration is a common source of error. Clarify any "allergy" with the actual reaction: a description of rash, timing, and severity, not a free-text label. [1]
For a cutaneous reaction, the examination looks for the features that separate a benign exanthem from SJS or TEN. Examine all skin and all mucous membranes — conjunctivae, oral cavity, genitals, and anal margin. Look for atypical target lesions, vesicles, bullae, skin tenderness or pain, and a positive Nikolsky sign (epidermal detachment on lateral pressure). Estimate the percentage of body surface area with skin detachment, because the detachment cut-offs define the diagnosis and prognosticate severity. [1]
For a systemic reaction, the examination is organised by organ. Assess airway, breathing and circulation first; a child with evolving anaphylaxis can deteriorate in minutes. Examine for hypoxia, wheeze, stridor, hypotension and altered consciousness. Then assess the liver (size, tenderness, jaundice), the kidneys (urine output, fluid status), and the blood (bruising, pallor, mucosal bleeding). A brief neurologic examination screens for the sedation, ataxia or extrapyramidal signs that point to neurotoxic drugs. [1]
Document the temporal sequence precisely. The three observations that anchor a causality judgement are the interval from first dose to onset, the response to withdrawal (dechallenge), and any prior rechallenge. Also record the most likely culprit when several drugs overlap, ranking them by timing, by the known reaction profile of each, and by the pattern of the presentation. These notes are what the Naranjo algorithm then turns into a probability rating, and they are also what a regulator needs in a report. [2]
Investigations
No single test confirms an ADR. The diagnosis rests on a structured causality assessment supported by targeted investigations that characterise the harm, exclude mimics, and occasionally identify the culprit. The validated scales — Naranjo for causality and Hartwig for severity — are the tools a fellowship candidate must be able to apply at the bedside. [1]
Routine bloods screen for organ involvement: a full blood count with differential (eosinophilia supports a hypersensitivity reaction, cytopenia a Type II reaction), liver function tests, creatinine and electrolytes, coagulation, and C-reactive protein. These do not prove an ADR, but they grade its severity and they exclude competing diagnoses. A serum tryptase drawn within one to two hours of a suspected anaphylactic reaction supports mast-cell degranulation and is one of the few investigations that meaningfully confirms an acute immune mechanism. [1]
Drug levels answer a narrow but important question: is this Type A toxicity from accumulation? A paracetamol level read against the treatment nomogram distinguishes toxic from non-toxic exposure and guides N-acetylcysteine. Anticonvulsant, digoxin and methotrexate levels, read against their therapeutic and toxic ranges, are essential when a child on these drugs presents with compatible symptoms. This is where therapeutic drug monitoring meets adverse drug reactions, and where the boundaries of the two topics overlap. [1]
Specialist testing is selective. Serum-specific IgE and skin testing have a role in confirming immediate beta-lactam allergy and guiding safe alternatives, but they are poor predictors of severe cutaneous reactions and should not be used after SJS or TEN. Drug provocation testing — the controlled reintroduction of a suspect drug under supervision — is the gold standard for some low-risk reactions but is contraindicated after any serious immune-mediated reaction. Skin biopsy confirms SJS or TEN and excludes mimics. Pharmacogenomic testing for HLA-B*15:02 before carbamazepine is standard of care in high-risk populations. [1]
The two scales that operationalise the assessment are Naranjo and Hartwig, and both are examinable as named tools. Naranjo scores ten items to rate causality. Hartwig grades severity from mild (no treatment needed) through moderate (treatment or prolonged admission) to severe and lethal (life-threatening or fatal). The Liverpool avoidability tool, developed and validated specifically for paediatric use, adds a third judgement: was this ADR avoidable? [2] [12]
Management — Resuscitation
A severe ADR is a time-critical emergency, and the first step does not depend on the classification. The priorities are airway, breathing and circulation, followed by stopping the suspected drug. Stopping the drug is both diagnostic and therapeutic — it is the dechallenge that every causality tool rewards — and in a deteriorating child it is never wrong to stop a non-essential medicine. [1]
Anaphylaxis is the prototypical resuscitation. The first-line treatment is intramuscular adrenaline (epinephrine) given without delay. The weight-based dose is 10 micrograms per kilogram of 1:1000 (1 mg per mL) solution, intramuscularly into the anterolateral thigh, repeated every five minutes as needed. For an adolescent or older child over about 12 years or over 20 kg, a 300 microgram autoinjector approximates the dose; for a young child from 7.5 to 20 kg the 150 microgram autoinjector is used; for an infant under 7.5 kg, draw up the weight-based dose from an ampoule rather than relying on an autoinjector. Lay the child flat with legs raised, give high-flow oxygen, establish intravenous access, and give a fluid bolus (10 to 20 mL per kg of isotonic crystalloid) for shock. Adjuncts — antihistamine, corticosteroid, bronchodilator — come after adrenaline, never instead of it. Observe for at least six hours because biphasic reactions occur. [1]
[1]Severe cutaneous reactions demand their own protocol. When SJS or TEN is suspected, stop the responsible drug immediately, admit to a high-dependency or PICU setting, and treat as a burn: fluids titrated to the surface area of detachment, meticulous wound care, eye review by ophthalmology within 24 hours (ocular adhesions cause lifelong blindness), nutritional support, pain relief, and surveillance for infection. Avoid prophylactic antibiotics. The benefit of immunomodulators such as intravenous immunoglobulin or ciclosporin is debated and should follow specialist advice. DRESS is managed by drug withdrawal, organ support, and — when severe — corticosteroid under specialist guidance, with screening for viral reactivation. [1]
Other emergencies follow the same logic of stop-the-drug-plus-specific-care. Opioid respiratory depression responds to naloxone (10 microgram per kg titrated to respiratory rate). Severe methaemoglobinaemia from oxidant drugs responds to methylene blue (1 to 2 mg per kg), but only after excluding G6PD deficiency because methylene blue can worsen haemolysis. Drug-induced torsades from a QT-prolonging agent is treated with intravenous magnesium and withdrawal of the drug. For any child who is unstable from a suspected ADR, escalate to PICU retrieval early. [1]
Management — Definitive & Stepwise
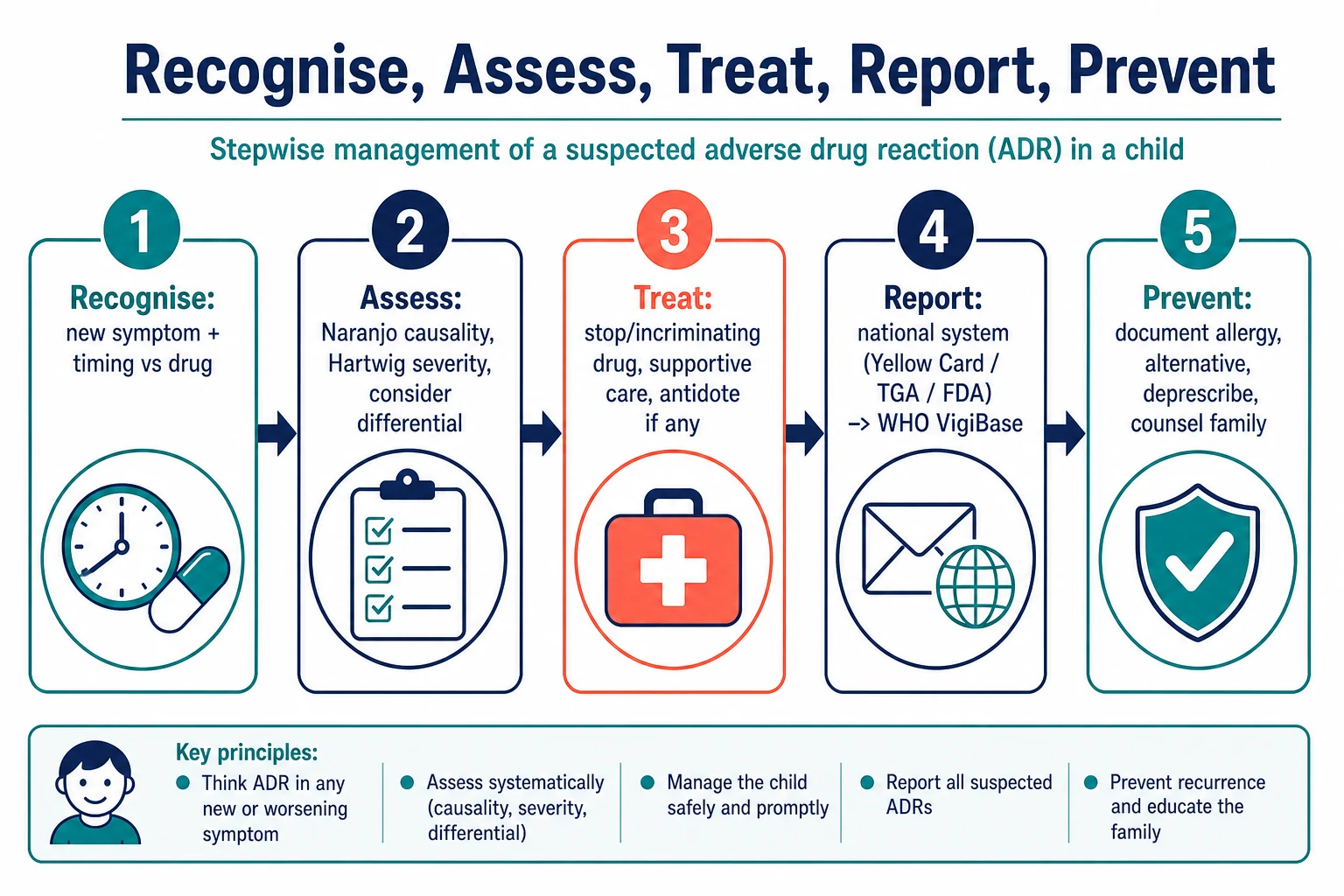
Once the child is stable, management becomes a sequence you can reproduce at the bedside and defend in a viva. The five steps — recognise, assess, treat, report, prevent — give the structure, and an emergency interrupt sits above them for any life-threatening reaction. [1] [10]
Recognise: place an ADR on the differential whenever a new or worsening symptom follows a medicine.
Assess: stop the suspected drug, apply Naranjo causality, grade Hartwig severity, and weigh the differential.
Treat: supportive care plus specific therapy — antihistamine for urticaria, adrenaline for anaphylaxis, antidote for reversible toxicity, withdrawal-plan for Type E reactions.
Report: file a report with your national system (TGA, MHRA Yellow Card, FDA MedWatch), and it reaches WHO VigiBase through the national centre.
Prevent: document the reaction, update the allergy record and MedicAlert, choose a non-cross-reactive alternative, simplify the regimen, and counsel the family.
Choosing the alternative drug is where pharmacology meets the individual child. After a true IgE-mediated beta-lactam allergy, select an agent from a different class; when a beta-lactam is essential, allergy review and, where appropriate, supervised drug provocation or desensitisation can recover first-line therapy. After carbamazepine-induced SJS/TEN, avoid oxcarbazepine and other aromatic anticonvulsants because of cross-reactivity, and screen the next family member who might be prescribed the drug. The principle is to match the alternative to the mechanism, not to default to "avoid everything." [1]
Graded reintroduction and desensitisation have narrow indications. They suit predictable, non-immune reactions where the drug is indispensable, such as chemotherapy or certain antibiotics in a child with limited options. They are contraindicated after any serious immune-mediated reaction — SJS, TEN, DRESS, or anaphylaxis — because re-exposure can be fatal. The decision belongs with a specialist drug allergy or immunology service. [1]
Reporting closes the loop between the bedside and the population. Every serious ADR, every ADR to a Black Triangle (newly marketed) medicine, and every paediatric ADR of note should be reported even when causality is uncertain — the regulator, not the reporter, makes the judgement on the signal. The professional duty to report is independent of certainty, and it is the mechanism by which the next child is protected. [9]
Specific Subtypes & Scenarios
Each high-yield subtype carries its own decision points. A beta-lactam allergy in a child who needs antibiotics is the everyday one: confirm whether the original reaction was truly immune-mediated (many penicillin labels originate in childhood viral rashes), use a non-cross-reactive agent when possible, and refer to an allergy service for delabelling when the history is low-risk. Cross-reactivity between penicillins and cephalosporins is lower than once feared for modern agents, but a severe reaction still mandates caution and specialist input. [1]
Anticonvulsant hypersensitivity is the subtype most likely to appear in a long case. Carbamazepine, lamotrigine, phenytoin and phenobarbitone can each cause a benign rash or a severe cutaneous reaction, and the latency is typically one to eight weeks. HLA-B*15:02 screening before carbamazepine is standard in Han Chinese and Southeast Asian populations, and the finding has reshaped prevention. The management is immediate withdrawal of the culprit and avoidance of cross-reactive aromatic anticonvulsants, with substitution of a structurally unrelated agent such as levetiracetam or valproate. [1]
NSAID-reactive airway disease presents in children with asthma who develop bronchospasm, urticaria or angioedema after ibuprofen or related drugs. Avoidance of non-selective NSAIDs is the mainstay, with paracetamol or a COX-2 selective agent when an anti-inflammatory is essential and the history permits. Opioid adverse effects — sedation, constipation, pruritus, respiratory depression, tolerance, and withdrawal — are managed by dose reduction, rotation, adjuvants, anticipatory laxatives, and structured weaning. Chemotherapy-related and corticosteroid-related ADRs each have their own topic and should be cross-referenced. [1]
Vaccine adverse events deserve a specific note because they are easily over-attributed. A fever or rash in the days after vaccination is most often coincidental with a community virus, and the task is to distinguish a true vaccine reaction from a vaccine-preventable disease or an unrelated event. Reporting of suspected vaccine ADRs is mandatory in many jurisdictions and feeds dedicated vaccine-safety surveillance, which is itself part of the wider pharmacovigilance system. [8]
Complications & Pitfalls
The complications of ADRs span the immediate and the long-term. Anaphylaxis can be fatal within minutes; SJS and TEN can cause blindness, strictures, and chronic skin and mucosal sequelae; DRESS can progress to multi-organ failure and reactivation of human herpesviruses. Drug-induced organ injury can leave residual hepatic, renal, or haematologic damage even after the drug is stopped. Beyond the physical harm, an inappropriate allergy label can deny a child first-line therapy for decades. [1]
The pitfalls that earn examination marks are the ones that recur. Confounding by indication — blaming the drug for an outcome caused by the disease — is the commonest error in causality judgement, and it is why a structured tool such as Naranjo exists. Under-reporting blinds the system: if no one reports the severe reaction to the Black Triangle drug, no signal is ever generated, and the next child receives it unknowingly. [9] Over-labelling a child allergic is the mirror error, restricting treatment for life on the basis of a viral rash. The prescribing cascade turns one ADR into two prescriptions. And deliberate rechallenge after a serious immune-mediated reaction is the error that can kill — it must never be done.
Look-alike and sound-alike drugs, and concentration errors in liquids, are system-level causes of paediatric ADRs that a careful prescriber can intercept. Ignoring the off-label or unlicensed status of a medicine is a subtler pitfall: these drugs are over-represented in paediatric ADR reports, so awareness of status should raise the threshold for vigilance rather than lower it. [6]
Prognosis & Disposition
Prognosis after an ADR is determined by severity, organ involvement, latency to stopping the drug, and the child's baseline health. A mild reaction resolves with drug withdrawal and simple symptomatic care, and the child can often be managed as an outpatient with clear safety-netting: return immediately if breathing, rash, or alertness worsen. A moderate reaction requires observation or short admission; a severe reaction mandates PICU and specialist input. [1]
The severe cutaneous reactions carry the most important long-term sequelae. SJS and TEN survivors need ophthalmology follow-up for months to years because ocular adhesions and corneal damage can appear late; urogenital and gastrointestinal strictures, chronic photosensitivity, and skin scarring all require structured surveillance. DRESS can relapse and can leave residual organ dysfunction, so liver, renal and cardiac monitoring continues after discharge. After anaphylaxis, prescribe an adrenaline autoinjector and an action plan, and refer to an allergy service; the dose of the autoinjector matches the weight band (150 microgram for 7.5 to 20 kg, 300 microgram for over 20 kg and over about 12 years). [1]
Disposition is never complete until the ADR is documented for life-long safety. Update the patient record, the allergy status, and where appropriate a MedicAlert, and communicate the reaction and the safe alternative to the medical home, the pharmacy, the school, and the family. A referral to a drug allergy or clinical immunology service is indicated for any serious immune-mediated reaction, for a child with multiple drug allergies, or when the label is uncertain and delabelling may restore first-line therapy. [1]
Special Populations
The risk profile of an ADR is never uniform across children, and the populations that concentrate risk are the ones a fellowship candidate must be able to name. Neonates and premature infants sit at the top of the list: immature glucuronidation and renal clearance, a larger volume of distribution, reduced protein binding, and a permeable blood-brain barrier all increase exposure to a "normal" dose, and off-label use is common. The lessons of grey baby syndrome and kernicterus are the historical proof that a neonate is not a small adult. [6]
Children with medical complexity and technology dependence carry polypharmacy, enteral tubes, and multiple prescribers, and they accumulate interactions and additive toxicity. Children with chronic kidney or liver disease need dose adjustment because reduced clearance converts a safe dose into accumulation toxicity — the bridge to the renal and hepatic dose-adjustment topic. Paediatric oncology and immunocompromised children face myelosuppression, drug interactions, and the consequences of off-label use, and their ADR burden is among the highest in medicine. [6]
Adolescents present a different set of risks: variable adherence, polypharmacy with mental health medicines, recreational substance interaction, and the privacy and consent considerations that shape what can be asked and documented. Pharmacogenomic variation cuts across every population: HLA-B*15:02 and carbamazepine SJS/TEN, G6PD deficiency and oxidant haemolysis, TPMT and thiopurine myelosuppression, and CYP2D6 and codeine metabolism all demonstrate that susceptibility is partly written in the genome. Indigenous, migrant and refugee children, and children with developmental disability or neurodiversity, may communicate and present atypically, and language discordance without a professional interpreter worsens every step from history to counselling. [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric ADRs rests on a small number of landmark contributions. Impicciatore and colleagues quantified the incidence of ADRs in paediatric inpatients and outpatients in a systematic review that still anchors teaching, and Clavenna and Bonati extended this with a review of prospective studies and safety alerts. [3] [4] Edwards and Aronson's framework for definitions, classification and diagnosis remains the conceptual backbone used worldwide, and the Naranjo algorithm, now over four decades old, is still the most widely taught causality tool. [1] [2]
The global infrastructure is the WHO Programme for International Drug Monitoring, which holds more than 20 million individual case reports in VigiBase, managed by the Uppsala Monitoring Centre in Sweden. VigiBase has been mined specifically for paediatric signals, and those analyses have shown that children generate distinctive signals that adult trials never surfaced. [7] [8] The Liverpool avoidability tool, developed for paediatric use, has shown that a meaningful proportion of childhood ADRs are potentially avoidable, which reframes prevention as a measurable target. [12]
Reporting systems at a glance
Comparative regional reference
Key finding
Reports flow from clinician or public to the national centre (ANZ: TGA; UK: MHRA Yellow Card; US: FDA MedWatch/FAERS), and the national centre contributes de-identified data to WHO VigiBase.
Practice change
The clinician reports once to the national system; the global signal emerges from pooled data. Every report contributes to paediatric safety.
The regional reporting systems differ in structure but share the same purpose. In ANZ the Therapeutic Goods Administration accepts reports through its online portal; reporting is voluntary for health professionals and the public, and feeds VigiBase through the Uppsala Monitoring Centre. In the UK the MHRA Yellow Card scheme accepts reports from clinicians and the public, with particular emphasis on Black Triangle medicines, serious reactions, and vaccines. In the US the FDA MedWatch programme accepts voluntary reports, while manufacturers must report serious ADRs within defined timeframes, and FAERS is the public database. Pharmacogenomic screening for HLA-B*15:02 before carbamazepine is embedded in FDA, CPIC and regional guidance but its uptake varies by health system and by population risk. [7]
The evidence has well-known limits. Spontaneous reporting captures signals, not proof — it carries no denominator of exposure, is distorted by under-reporting and notoriety, and a reporting imbalance is an association, not causation. Active surveillance, sentinel systems, electronic health-record-based monitoring, and paediatric investigation plans under paediatric regulations all extend the picture. Where the evidence remains thin is in children themselves: causality tools were built largely in adults, avoidability assessment is still maturing, and the long-term sequelae of severe cutaneous reactions in children are incompletely characterised. [8] [9]
Exam Pearls
The one-liners that earn marks in this topic are sharp and few. Type A is Augmented — predictable, dose-related, common, low mortality; Type B is Bizarre — unpredictable, dose-independent, rare, potentially lethal. The DoTS mnemonic reads Dose-relatedness, Time-relatedness, Susceptibility, and it is the modern mechanistic classification that sits on top of the alphabet. The Naranjo bands are a memorisation must: 0 to 4 doubtful, 5 to 6 possible, 7 to 13 probable, 14 to 18 definite. [2]
ADR-PV
The high-yield specifics reward precision. The first-line treatment of anaphylaxis is intramuscular adrenaline at roughly 10 microgram per kg of 1:1000 solution, repeated every five minutes; the autoinjector is 150 microgram for 7.5 to 20 kg and 300 microgram for over 20 kg and over about 12 years. SJS involves under 10 percent body surface area detachment, SJS-TEN overlap 10 to 30 percent, and TEN over 30 percent — a must-know for severity. Carbamazepine SJS/TEN is strongly associated with HLA-B*15:02 in Han Chinese and Southeast Asian ancestry. Under-reporting is the rule not the exception, with a systematic-review median around 94 percent. [9] And the single most important management step, asked in nearly every viva, is to stop the suspected drug first.
[8]References
- [1]Edwards IR, Aronson JK Adverse drug reactions: definitions, diagnosis, and management Lancet (London, England), 2000.PMID 11072960
- [2]Naranjo CA, Busto U, Sellers EM, et al A method for estimating the probability of adverse drug reactions Clinical pharmacology and therapeutics, 1981.PMID 7249508
- [3]Impicciatore P, Choonara I, Clarkson A, et al Incidence of adverse drug reactions in paediatric in/out-patients: a systematic review and meta-analysis of prospective studies British journal of clinical pharmacology, 2001.PMID 11453893
- [4]Clavenna A, Bonati M Adverse drug reactions in childhood: a review of prospective studies and safety alerts Archives of disease in childhood, 2009.PMID 19531524
- [5]Gallagher RM, Mason JR, Bird KA, et al Adverse drug reactions causing admission to a paediatric hospital PloS one, 2012.PMID 23226510
- [6]Bellis JR, Kirkham JJ, Nunn AJ, Pirmohamed M Adverse drug reactions and off-label and unlicensed medicines in children: a nested case-control study of inpatients in a pediatric hospital BMC medicine, 2013.PMID 24229060
- [7]Star K, Noren GN, Nordin K, Edwards IR Suspected adverse drug reactions reported for children worldwide: an exploratory study using VigiBase Drug safety, 2011.PMID 21513364
- [8]Star K, Chandler RE, Noren GN, Edwards IR Paediatric safety signals identified in VigiBase: Methods and results from Uppsala Monitoring Centre Pharmacoepidemiology and drug safety, 2019.PMID 30767342
- [9]Hazell L, Shakir SA Under-reporting of adverse drug reactions: a systematic review Drug safety, 2006.PMID 16689555
- [10]Sammons HM Learning lessons from adverse drug reactions in children Children (Basel, Switzerland), 2016.PMID 27417239
- [11]Cliff-Eribo KO, Sammons HM, Choonara I Systematic review of paediatric studies of adverse drug reactions from pharmacovigilance databases Expert opinion on drug safety, 2016.PMID 27501085
- [12]Bracken LE, Nunn AJ, Kirkham JJ, et al Development of the Liverpool Adverse Drug Reaction Avoidability Assessment Tool PloS one, 2017.PMID 28046035