Paeds · clinical-pharmacology-and-therapeutics
Analgesics and antipyretics
Also known as Paediatric analgesia · Paracetamol and ibuprofen dosing in children · Antipyretic use in the febrile child · WHO analgesic ladder for children · Paediatric opioid safety and codeine restriction
A fellowship approach to choosing and dosing an analgesic or antipyretic in a child: weigh the child, calculate the dose from a current paediatric formulary, cap it at the adult maximum, and combine the drug with age-appropriate comfort. Paracetamol 15 mg per kg per dose (maximum 60 mg per kg per day, adult maximum 1 g per dose and 4 g per day) and ibuprofen 5 to 10 mg per kg per dose (maximum 30 mg per kg per day, from three months and over 5 kg) cover most fever and mild-to-moderate pain. Morphine 0.1 to 0.2 mg per kg intravenously treats severe pain. Aspirin is avoided in under-16s with viral illness because of Reye syndrome, and codeine and tramadol are contraindicated in children under 12 and after tonsillectomy because CYP2D6 ultrarapid metabolisers convert a therapeutic prodrug dose into a fatal morphine overdose. Alternating paracetamol and ibuprofen is not routine: use one effective agent with a clear plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
An analgesic relieves pain, and an antipyretic lowers fever. The two jobs overlap because the same drug often does both: paracetamol and the non-steroidal anti-inflammatory drugs (NSAIDs) reduce fever by resetting the hypothalamic thermostat and ease pain by blocking prostaglandin-driven inflammation, so a single dose given for a febrile, uncomfortable child is doing two jobs at once. Morphine, by contrast, is a pure analgesic with no antipyretic action, because it works on the opioid receptor rather than on the prostaglandin pathway. The prescriber's question is therefore not "pain or fever" but "what is the problem, how heavy is it, and which agent at which dose will relieve the child safely." [2] [3]
The discipline of the topic lives in four facts. First, every dose is calculated from a measured weight in kilograms, because a child is not a fraction of an adult. Second, the calculation always stops at the adult maximum, so a large adolescent never receives more than an adult would. Third, the choice is governed by the child's age, hydration, renal and liver function, asthma and bleeding risk, and by what the drug is for. Fourth, the response is judged on the child — comfort, activity, hydration and a pain score — and not on a number on the thermometer, because a falling temperature in a toxic child can mask serious illness. [2] [9]
The unifying principle is the right drug, at the right weight-based dose, capped at the adult maximum, combined with comfort, and judged on the child. A fever that distresses a well child is treated for comfort; a fever in a toxic child is treated while the septic work-up proceeds. Pain is treated in its own right and reassessed, because undertreated pain in a pre-verbal or cognitively impaired child is a failure of care, not a kindness. The exam answer is the workflow and the safety boundaries, not the arithmetic of a single dose: weigh, calculate, cap, give, comfort, reassess. [11] [12]
Classification
The single most useful classification is by drug class and the clinical job it does, because the class decides the dose, the cap, the age cut-off and the principal danger. Look at the problem — fever, mild pain, inflammatory pain, severe pain, procedural discomfort — and the class follows: a simple analgesic covers most fever and mild pain, an NSAID adds anti-inflammatory action, an opioid is reserved for severe pain, and non-pharmacological measures anchor every step, especially in the neonate. [2] [11]
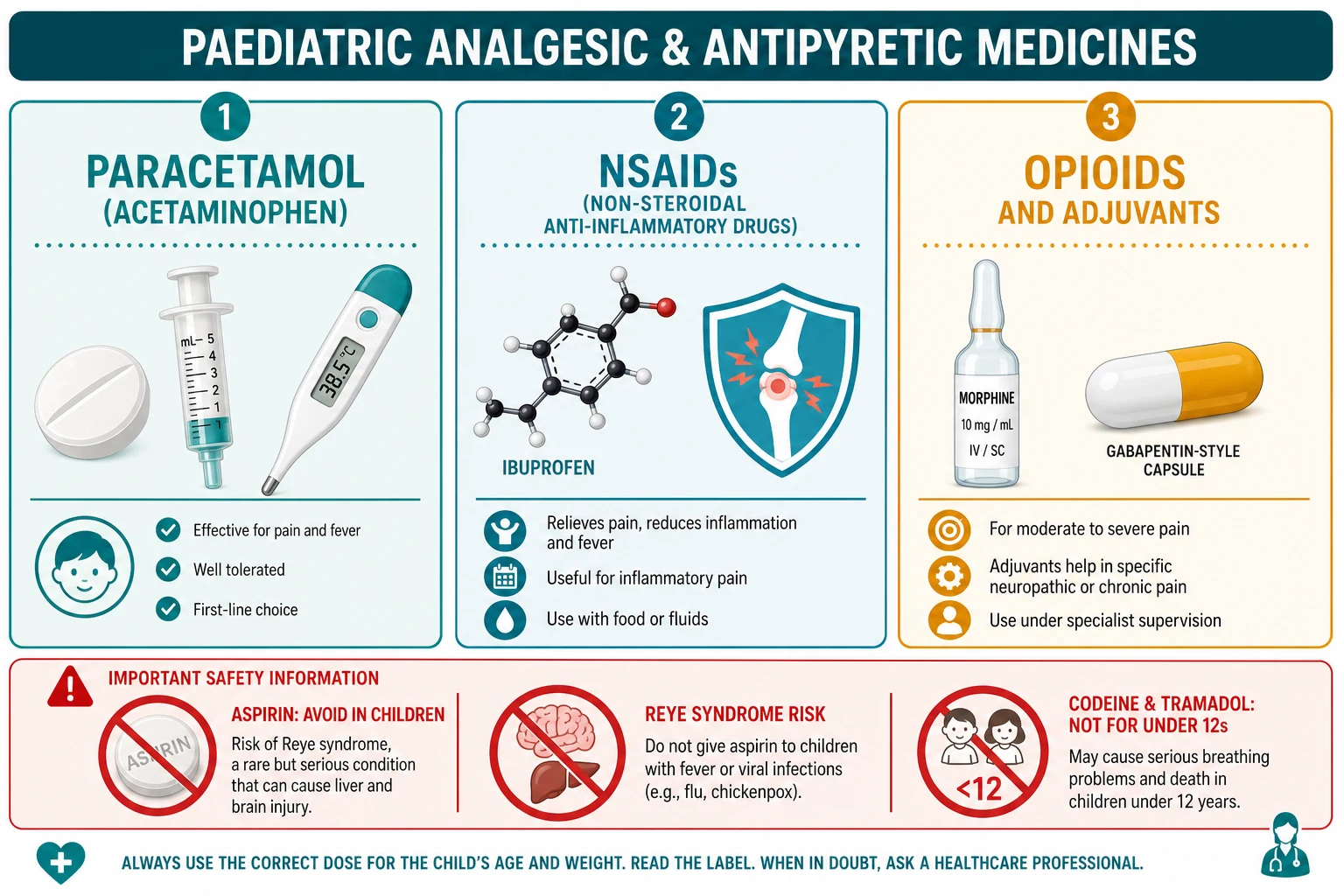
Simple analgesic
Paracetamol (acetaminophen)
- Analgesic and antipyretic, weak anti-inflammatory
- 15 mg per kg per dose, every 4–6 h, max 60 mg per kg per day; adult max 1 g per dose and 4 g per day
- Safe in most children; hepatotoxic in overdose
- First-line for fever and mild-to-moderate pain; usable at all ages including neonates with care
NSAID
Ibuprofen, naproxen, diclofenac
- Analgesic, antipyretic and anti-inflammatory via COX inhibition
- Ibuprofen 5–10 mg per kg per dose, every 6–8 h, max 30 mg per kg per day, from 3 months and over 5 kg
- Avoid in dehydration, renal impairment, bleeding risk and aspirin-sensitive asthma
- First-line when inflammation is a feature (e.g. juvenile arthritis, soft-tissue injury)
Opioid
Morphine; restricted codeine and tramadol
- Pure analgesic, no antipyretic action; mu-opioid receptor
- Morphine 0.1–0.2 mg per kg IV or 0.2–0.5 mg per kg orally; titrate and monitor
- Codeine and tramadol contraindicated under 12 and after tonsillectomy
- Reserved for moderate-to-severe pain, usually postoperative or in critical care
Adjuvant and topical
Gabapentinoids, ketamine; amethocaine, EMLA
- Add-on for neuropathic or persistent pain (gabapentin, amitriptyline), or perioperative opioid-sparing (ketamine)
- Topical amethocaine or EMLA for needle procedures; sucrose for neonatal procedures
- Reduce total opioid exposure as part of multimodal analgesia
- Specialist pain team guidance for chronic or cancer pain
Classification by age and developmental stage frames why the choice changes across childhood. The neonate has an immature liver and a low glomerular filtration rate, so paracetamol doses are weight-banded with a lower daily ceiling and opioids are given cautiously with monitoring. The infant and preschool child can take paracetamol and, from three months and over 5 kg, ibuprofen, but they cannot describe their pain, so a behavioural score (FLACC) stands in for words. The school-age child begins to use a numerical rating scale, and the adolescent is dosed as an adult once the weight-based calculation reaches the adult cap. The class is constant across age; the dose, the formulation and the assessment tool change. [11] [12]
Epidemiology & Risk Factors
Fever and pain are among the most common reasons a child presents to care, and analgesics and antipyretics are among the most commonly used medicines in childhood. The risk lies less in the drugs themselves, which are remarkably safe when dosed correctly, than in the errors that surround them: an under-dose that leaves a child in pain, an over-dose that exceeds a ceiling, an agent given to a child who should not have it, and a formulation whose strength is misread. The child who is harmed is usually the one whose weight was estimated, whose paracetamol came from more than one preparation, or who received an opioid metabolised unpredictably. [2] [4]
Child factors
- Pre-verbal or cognitively impaired children carry the highest risk of under-recognised, undertreated pain
- Dehydration or renal impairment turns a safe NSAID into a nephrotoxin
- Asthma and aspirin sensitivity increase NSAID bronchospasm risk
- Liver disease, malnutrition and the neonate lower the safe paracetamol ceiling
Drug and process factors
- Combining cold preparations hides paracetamol and breaches the daily ceiling
- A concentrated infant drop dosed as a children's suspension overdoses the child
- Estimating weight rather than measuring it invites a dosing error
- Alternating two agents without a plan confuses carers and doubles doses
System factors
- Post-tonsillectomy children historically received codeine despite the black-box restriction
- Out-of-hours and remote prescribing with limited pharmacist review
- Care transitions where a dose is not re-checked or re-written in mg
- Discharge with a liquid medicine and no dosing syringe or mg instruction
Paracetamol hepatotoxicity remains the leading cause of acute liver failure in children in many high-income settings, and almost every case is preventable. The mechanism is dose-stacking: a carer gives a cold preparation and a separate paracetamol, or repeats a dose ahead of schedule, or doses on an estimated weight, and the daily ceiling is breached over hours. The risk is concentrated in the under-five child receiving an oral liquid, in the child with fasting or intercurrent illness that depletes glutathione, and in the deliberate or accidental large ingestion. Codeine and tramadol carry a different and rarer risk concentrated in a single pharmacogenetic subgroup, but that subgroup cannot be identified at the bedside, which is exactly why the drugs are restricted outright rather than dosed around. [4] [7]
Pathophysiology
Fever and inflammatory pain share a final common pathway — prostaglandins — and that is why paracetamol and the NSAIDs do both jobs. A pyrogen (from infection, inflammation or tissue injury) stimulates the hypothalamus to produce prostaglandin E2, which resets the thermoregulatory set-point upward: the body behaves as if its normal temperature were 39 or 40 degrees, generates heat by shivering and conserves it by vasoconstriction, and the child feels cold and looks unwell. Paracetamol and the NSAIDs lower the set-point back toward normal by inhibiting prostaglandin synthesis; the child then vasodilates, sweats, and the fever falls. The antipyretic does not cool a hot child directly, it switches off the instruction to be hot. [2] [3]
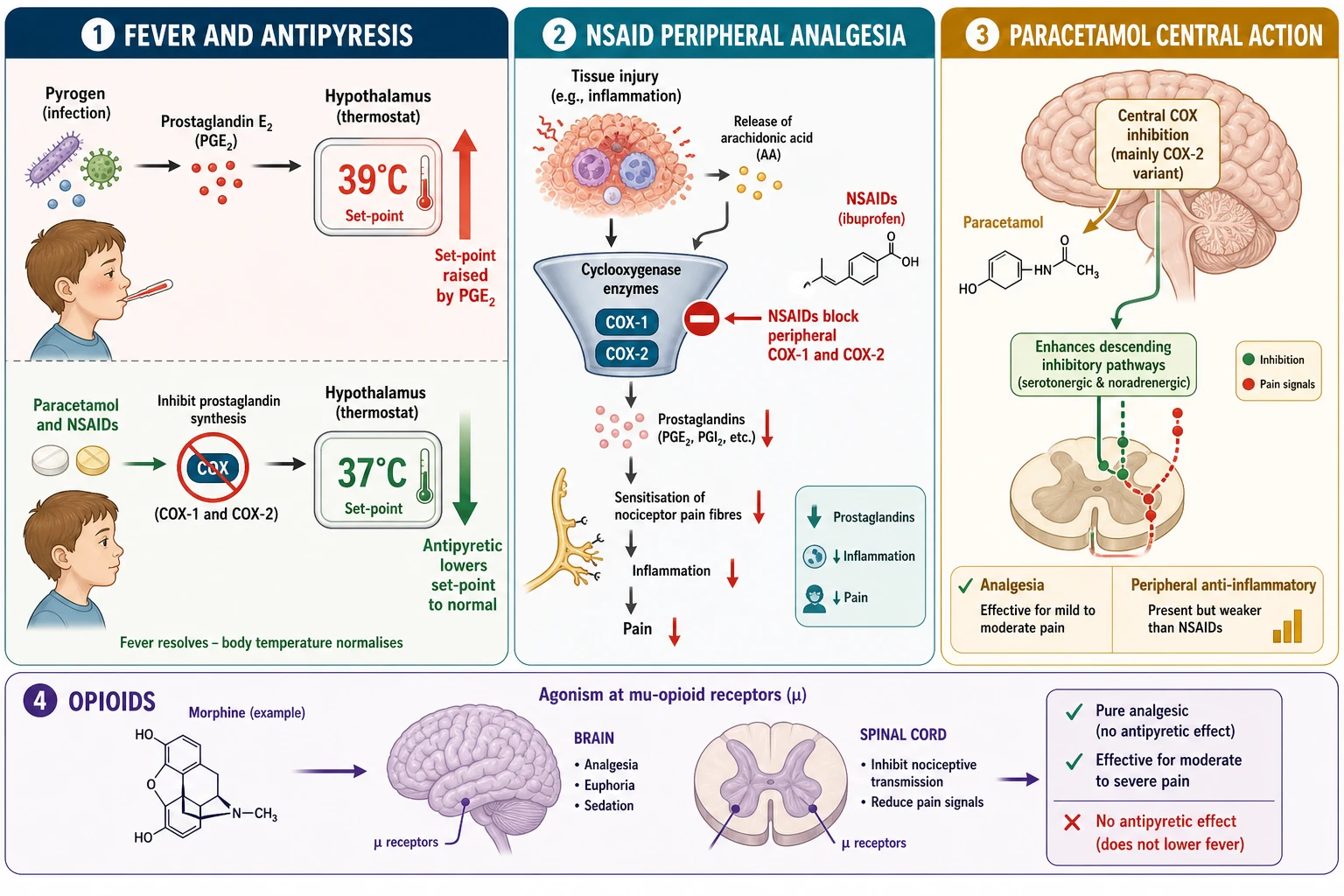
At the tissue, injury releases arachidonic acid from damaged cell membranes, and the cyclooxygenase enzymes COX-1 and COX-2 convert it to prostaglandins that sensitise nociceptors to bradykinin and other pain mediators. The NSAIDs reduce peripheral pain by blocking this step, which is why they are preferred when inflammation is part of the picture — a soft-tissue injury, juvenile arthritis, dysmenorrhoea. Paracetamol is a weaker anti-inflammatory than the NSAIDs despite acting on the prostaglandin pathway, because its principal action is central: it is thought to inhibit a COX variant in the brain and to enhance the endocannabinoid and serotonergic descending inhibitory pathways. That central bias is also why paracetamol is the safer choice in a child who should not have an NSAID — the dehydrated or renally impaired child, the child with a bleeding risk, the aspirin-sensitive asthmatic. [3] [9]
The opioids act at a different site altogether. Morphine agonises the mu-opioid receptor in the brain and spinal cord, dampening the perception of pain and the affective response to it, and (unhelpfully) also the respiratory centre in a dose-related way. Codeine and tramadol are prodrugs: codeine is O-demethylated by the cytochrome P450 enzyme CYP2D6 into morphine, and tramadol is converted by the same enzyme to its more active opioid metabolite. In a CYP2D6 ultrarapid metaboliser — roughly 5 to 10 per cent of people, varying by ancestry — a standard codeine or tramadol dose generates a flood of morphine, and the child develops opioid respiratory depression and apnoea. Because the genotype cannot be known at the bedside, the regulator treats the whole population as at risk and restricts the drug. [7] [8]
The paracetamol overdose mechanism closes the pathophysiology. At therapeutic dose, paracetamol is cleared by conjugation to glucuronide and sulphate, with a small fraction oxidised by CYP2E1 to the reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI), which is immediately detoxified by glutathione. In overdose, the conjugation pathways saturate, NAPQI accumulates, glutathione is depleted, and NAPQI binds hepatocyte proteins and causes centrilobular necrosis. N-acetylcysteine works by replenishing glutathione and by directly detoxifying NAPQI, and it is highly effective when given early — which is why the time of ingestion and a four-hour level drive the whole treatment decision. [4] [5]
Clinical Presentation
A child who needs an analgesic or antipyretic presents in one of three ways, and the prescriber's first move is to recognise which. The first is the febrile child: hot to touch, irritable or clingy, often refusing fluids, sometimes with a clear source (a runny ear, a cough, a rash) and sometimes without. The second is the child in pain: the postoperative child guarding a wound, the child with a fracture holding the limb still, the toddler with otitis media pulling at an ear, the infant with colicky, drawing-up legs. The third is the child who needs a procedure: a cannula, a venepuncture, a urethral catheter, a lumbar puncture, where the pain is brief but real and anticipatory anxiety amplifies it. [2] [11]
The crucial clinical skill is to tell, within each presentation, the child who is merely uncomfortable from the child who is seriously ill. A febrile child who is alert, playing and drinking is managed with comfort and an antipyretic at home with a safety-net; a febrile child who is toxic — tachycardic beyond the fever's expectation, tachypnoeic, mottled, limp, or non-responsive — needs urgent assessment, a septic work-up and antibiotics regardless of the temperature response. Pain has the same divide: most pain is managed with a simple analgesic, but severe pain, pain with a serious cause (a torsion, an appendicitis, a sickle crisis), or pain that does not respond as expected escalates the child up the ladder and up the service. [2] [12]
Febrile, well child
- Alert, interacting, playing, drinking
- Normal perfusion and work of breathing for age
- Manage with comfort and paracetamol or ibuprofen, safety-net for deterioration
- Antipyretic response does not exclude serious infection — judge the child
Febrile, toxic child
- Tachycardic beyond fever expectation, tachypnoeic, mottled, limp, non-responsive
- Urgent septic work-up and empiric antibiotics alongside the antipyretic
- Do not wait for the temperature to fall before acting
- Escalate to senior, intensive care and retrieval as indicated
Child in pain
- Score pain with an age-appropriate tool (FLACC, numeric, revised FLACC)
- Give the weight-based dose of the right class; reassess at the expected onset
- Severe pain or a serious cause escalates the ladder and the service
- Untreated pain in a pre-verbal child is a failure of care
Procedural discomfort
- Brief but real pain; anxiety amplifies it
- Combine non-pharmacological measures (sucrose, breastfeeding, distraction, positioning) with topical local anaesthetic
- Amethocaine or EMLA for cannulation 30–60 min beforehand
- Plan the procedure, the analgesia and the child's position together
Paracetamol hepatotoxicity is the presentation the prescriber must never miss, because it is silent when it is treatable. The child who has taken a supra-therapeutic or large dose may look entirely well for the first 24 hours, then develop right-upper-quadrant pain, vomiting and tenderness as hepatocyte necrosis begins, and over the next days coagulopathy, encephalopathy and acute liver failure. The early window — the first hours to a day — is when N-acetylcysteine prevents the injury; the late window is when it can only limit it. Opioid respiratory depression, by contrast, declares itself at the bedside: the child on a postoperative opioid who becomes progressively sedated, with a falling respiratory rate and a small or unreactive pupil, needs naloxone titrated to the respiratory rate, not to full reversal. [4] [12]
Differential Diagnosis
When a febrile child fails to respond to an antipyretic, the prescriber's instinct should be systematic, not reflexive. Build the differential in a fixed order. First, is the dose adequate for the weight — an under-dose given on an estimated weight is the commonest reason a fever "does not respond." Second, is the measurement real and the technique correct, or is the child simply overdressed? Third, is the fever driven by a serious bacterial infection needing source control rather than another milligram of paracetamol? Fourth, is the child genuinely non-responsive, which itself is a red flag for serious illness? A fever that fails to fall after a correct dose does not by itself diagnose anything, but it raises the index of suspicion and shifts the focus to the child and the cause. [2] [9]
Dose or technique
- Under-dose for weight (estimated weight, or a cap applied too early)
- Thermometer or route error; overdressed child
- Wrong formulation strength dosed as another
- Dose given but not yet absorbed — onset is 30–60 min for oral paracetamol
Serious infection
- Bacteraemia, meningitis, pyelonephritis, pneumonia, septic arthritis
- A toxic child needs a septic work-up regardless of the antipyretic response
- Failure to respond raises suspicion but does not confirm or exclude
- Source control (antibiotics, drainage) is the definitive treatment, not the antipyretic
Unrecognised pain
- The postoperative, cognitively impaired or pre-verbal child in unrecognised pain
- Agitation mistaken for delirium or anxiety
- Score with FLACC or revised FLACC; treat and reassess
- A full bladder, a tight cast, a blocked catheter — look before dosing
Other
- Drug fever, Kawasaki disease, malignancy, autoimmune in the prolonged fever
- Heat illness in the overdressed or entrapped child
- Hypoglycaemia in the unwell child — check bedside glucose
- Constipation, otitis, pharyngitis as reversible sources of distress
The discriminator that separates paracetamol hepatotoxicity from viral hepatitis is the history of intake: a single large ingestion (the child who drank the bottle), a staggered repeated supra-therapeutic dosing over a day or two, or the covert repeated dose in a child with fasting and intercurrent illness. A paracetamol level taken at or after four hours, plotted against the time of ingestion on the treatment nomogram, is the decision tool, and the time of ingestion is the linchpin — without it the level is uninterpretable and the clinician errs toward treating. Non-analgesic causes of a child's distress must be kept open alongside the pain diagnosis, because hypoglycaemia, hypoxia, infection and a full bladder each masquerade as agitation until they are looked for. [4] [5]
Clinical & Bedside Assessment
The bedside assessment has two parts: score the problem, and weigh the child. Pain is scored with an age-appropriate, validated tool, because the carer's and clinician's estimates systematically under-rate a child's pain. The FLACC scale (Face, Legs, Activity, Cry, Consolability), each domain scored 0 to 2 for a total of 0 to 10, is the standard for infants and pre-verbal children; the revised FLACC extends the same framework to children with cognitive impairment by adding observed behaviours specific to that child. The school-age child uses a 0-to-10 numerical rating scale or a faces scale, and the adolescent a numeric or verbal rating as an adult would. Fever is measured accurately by age: axillary for the well older infant, tympanic for the cooperative child, oral for the older child, and a rectal temperature as the reference standard in the small or seriously ill infant where under-reading is dangerous. [11] [12]
The focused history frames the choice. Ask the age and the weight; the source and severity of the pain or fever; the hydration status and urine output; any renal or liver disease; asthma and aspirin sensitivity; bleeding risk; concurrent medicines (especially other paracetamol-containing preparations, anticoagulants, and other central nervous system depressants); a paracetamol intake history when toxicity is possible; and any allergy. The synthesis the candidate should speak and document is the problem representation: the child's age and weight, the pain or fever problem and its score, the chosen drug, the calculated dose, the cap, the frequency, and the plan to reassess. Every dose is written with a leading zero (0.5 mg, never .5 mg) and never a trailing zero (5 mg, never 5.0 mg), and every calculation is capped at the adult maximum before it is signed. [2] [12]
Investigations
Most febrile and painful children are managed without investigations beyond the bedside, because the analgesic and antipyretic decision is clinical. Investigations serve two purposes: to identify the cause of the fever, and to frame the safety of the drug. The risk-stratified septic work-up is driven by age and immune status — a febrile infant under one month, or a toxic child of any age, is investigated and treated for sepsis until proven otherwise — and the response to an antipyretic is one input into that decision, never a replacement for it. A child whose fever falls after paracetamol can still have bacteraemia; a child who remains toxic needs the work-up regardless of the temperature. [2] [9]
For suspected paracetamol toxicity, the time of ingestion and a paracetamol level taken at or after four hours are the decision tools: the level is plotted on the treatment nomogram, and treatment with N-acetylcysteine is started if the level is on or above the treatment line, if the ingestion is staggered or the time is unknown, or if there is any evidence of hepatotoxicity. Renal function and electrolytes frame the NSAID decision — an NSAID given to a dehydrated child can precipitate acute kidney injury — and liver function and coagulation frame both the paracetamol safety question and the severity of an established toxicity. A bedside glucose is taken early in any child with altered behaviour or a reduced conscious level, because hypoglycaemia mimics and compounds opioid sedation and the unwell febrile state. [4] [12]
Management — Resuscitation
Resuscitation in this topic is the recognition and immediate management of the toxic febrile child, the paracetamol-overdosed child, and the opioid-over-sedated child. The general approach is constant: assess the airway, breathing and circulation; treat the pain and the fever; identify the source; and escalate to senior help, intensive care and retrieval when the child is seriously ill. For the toxic febrile child, the antipyretic is given alongside, not instead of, the septic work-up and empiric antibiotics — the fever is one sign, and source control is the definitive treatment. [2] [9]
For suspected opioid-induced respiratory depression, the action is airway and breathing support and naloxone titrated to the respiratory rate, not to full reversal. A child who is bradypnoeic or apnoeic on a postoperative opioid is stimulated, given bag-valve-mask support if needed, and naloxone is dosed incrementally until the respiratory rate recovers — the goal is a breathing child who is still comfortable, not an awake, howling, in-pain child who will need re-dosing as the opioid outlasts the antidote. Because naloxone's half-life is shorter than the opioid's, a child who has received naloxone is monitored for recurrence, with repeat boluses or an infusion as required. After any dosing error or adverse drug event, the child is made safe first, the event is reported, and the family is communicated with honestly — in that order. [12]
Management — Definitive & Stepwise
Definitive management is the WHO analgesic ladder adapted for children, anchored by the weight-based doses and capped at the adult maximum. The ladder is climbed stepwise, by the clock (regular dosing, not as-needed for established pain), by the child (the weight-based dose), and by the ladder (move up when the current step is inadequate). The paediatric version places non-pharmacological comfort at the first step alongside the simple analgesic, because comfort, sucrose, breastfeeding, distraction and positioning are analgesic in their own right and reduce the total drug load — a point the adult ladder underplays and the paediatric prescriber must not. [2] [11]
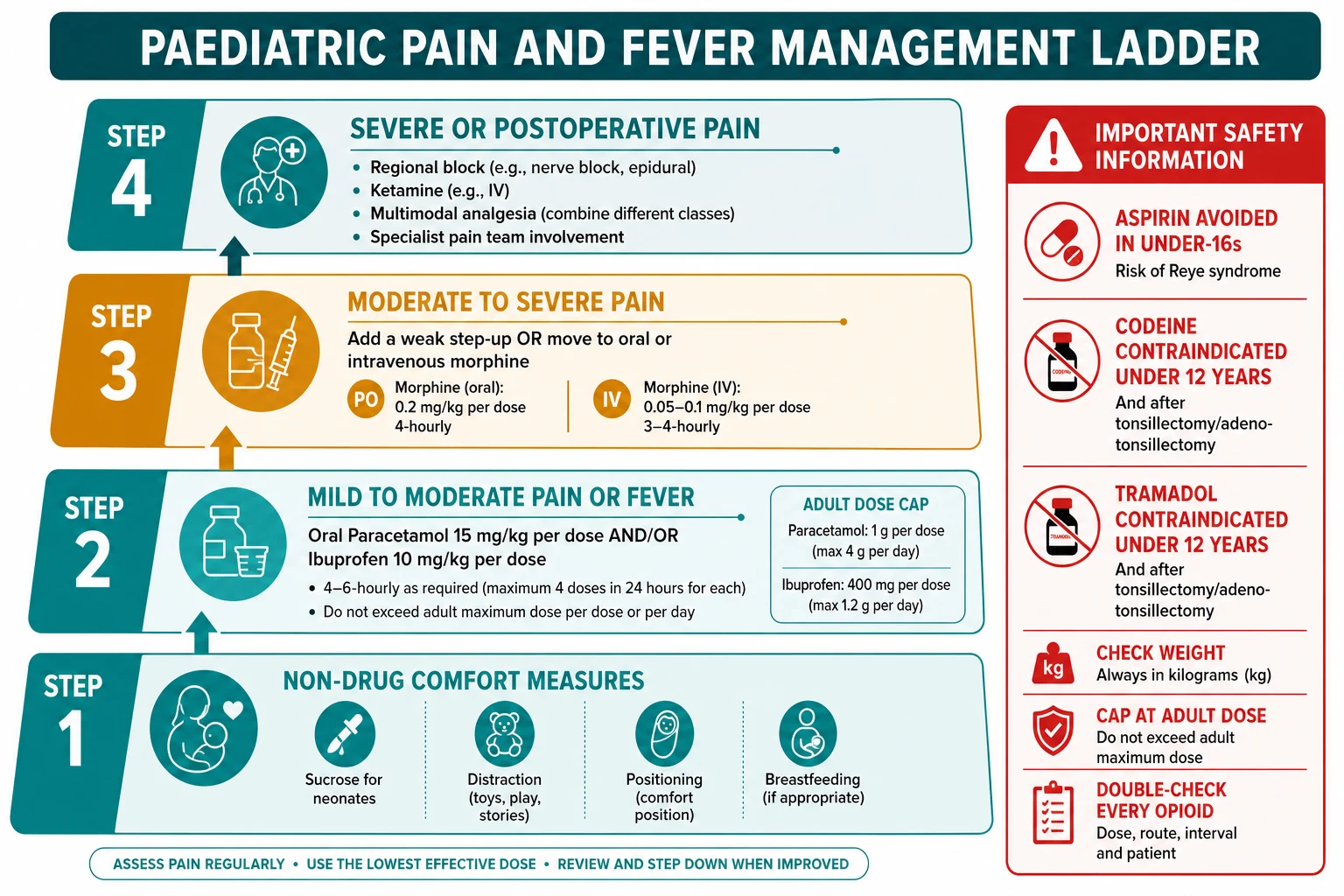
Step 1 — Comfort and a simple analgesic
Non-drug measures (sucrose, breastfeeding, distraction, positioning) plus paracetamol 15 mg per kg per dose every 4–6 h (max 60 mg per kg per day, adult max 4 g per day) or ibuprofen 5–10 mg per kg per dose every 6–8 h (max 30 mg per kg per day, from 3 months and over 5 kg). First-line for fever and mild-to-moderate pain.
Step 2 — Add a low-dose opioid
For moderate pain not controlled by step 1, add low-dose morphine 0.1–0.2 mg per kg intravenously or 0.2–0.5 mg per kg orally, titrated to the pain score and monitored for sedation and respiratory rate. The historical weak-opioid step (codeine, tramadol) is replaced by low-dose morphine because codeine and tramadol are restricted.
Step 3 — Strong opioid, regional, multimodal
For severe or postoperative pain, titrated morphine (or another strong opioid), a regional or local anaesthetic block, ketamine as an opioid-sparing adjuvant, and regular paracetamol and an NSAID as the multimodal backbone. Involve the specialist acute or chronic pain team for persistent, cancer or neuropathic pain.
Safety boundaries at every step
Weigh in kg, cap at the adult maximum, write a leading zero and no trailing zero, double-check every opioid, avoid aspirin in under-16s, and do not use codeine or tramadol in under-12s or after tonsillectomy. Reassess the pain score after each step at the expected onset of action.
The doses are the anchor facts. Paracetamol is 15 mg per kg per dose every four to six hours, maximum 60 mg per kg per day in a child and an adult ceiling of 1 g per dose and 4 g per day. Ibuprofen is 5 to 10 mg per kg per dose every six to eight hours, maximum 30 mg per kg per day, from three months of age and over 5 kg (some formularies, including the BNFc, set the lower age at three months; others prefer six months — state the source). Morphine is 0.1 to 0.2 mg per kg intravenously or 0.2 to 0.5 mg per kg orally, titrated and monitored. Every one of these is calculated from a measured weight, capped at the adult maximum, and rounded to an available formulation. The dose-pressing pitfall is the paracetamol ceiling breached by a second preparation — always ask what the carer has already given. [2] [3]
The alternating question deserves its own sentence, because it is a common exam and a common practice trap. The 2024 network meta-analysis found that short-term dual therapy (paracetamol plus ibuprofen) can lower temperature faster and for longer than either agent alone in the febrile child, but the effect is modest, and routine alternating is not recommended because it increases dosing error, parental confusion and the risk of doubled or exceeded doses. The defensible position is to use a single effective agent with a clear plan, and to reserve dual therapy for a distressed child who has not responded to monotherapy, with a written dosing schedule and a dosing syringe for the family. [1] [2]
In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne guidelines and the AMH Children's Dosing Companion are the bedside references: paracetamol 15 mg per kg per dose (max 60 mg per kg per day, adult max 4 g per day) and ibuprofen 5 to 10 mg per kg per dose (max 30 mg per kg per day) from three months and over 5 kg. The ANZ paracetamol poisoning guideline drives the N-acetylcysteine decision; the TGA restricts codeine and tramadol in children under 12 and after tonsillectomy. [4] [2]
Specific Subtypes & Scenarios
The neonate is the scenario where non-pharmacological measures carry most of the weight. Oral sucrose, given as small absolute volumes (commonly 0.1 to 2 mL of 24 per cent sucrose) by mouth or on a pacifier two minutes before a procedure, with non-nutritive sucking and breastfeeding, reduces the behavioural pain response to heel lancing, venepuncture and other minor procedures, and is the procedural analgesia of first resort on the neonatal unit. Repeated dosing within a short window is avoided where evidence is thin, and sucrose does not substitute for effective analgesia in a sustained painful procedure. Paracetamol is used in the neonate at weight-banded doses with a lower daily ceiling, reflecting hepatic immaturity; opioids are given cautiously with monitoring for apnoea. [11] [4]
The postoperative child is managed with multimodal, opioid-sparing analgesia, and this is the modern standard. Regular paracetamol and an NSAID (where not contraindicated) form the backbone, a regional or local anaesthetic technique (a wound infiltration, a peripheral block, a caudal) targets the surgical site, and a low-dose opioid such as morphine or oxycodone is reserved for breakthrough or moderate-to-severe pain, titrated and monitored with a sedation score. The explicit goal is to minimise total opioid exposure, which both improves recovery and reduces opioid-related adverse effects, and the historical weak-opioid step (codeine, tramadol) is replaced by low-dose morphine because the prodrug opioids are restricted. [12] [11]
The post-tonsillectomy child is the archetype of why codeine was restricted. Children after tonsillectomy or adenoidectomy frequently have obstructive sleep apnoea and a compromised airway, and codeine given to a CYP2D6 ultrarapid metaboliser produced fatal respiratory depression and deaths that led to the FDA and MHRA contraindications. The modern regimen is regular paracetamol, ibuprofen where not contraindicated (the bleeding-risk question is balanced against the analgesic benefit in current guidance), and morphine or oxycodone only when needed, with overnight monitoring for the child at airway risk. Codeine and tramadol are simply not given to these children. [7] [8]
Child with asthma
- Paracetamol is first-line and safe
- NSAIDs avoided if aspirin-sensitive or NSAID-exacerbated respiratory disease; otherwise used with caution after specialist input
- Estimate risk from prior NSAID reaction, not from asthma alone
- Modern evidence is reassuring on ibuprofen in most children with asthma
Child with renal impairment or dehydration
- NSAIDs avoided — restore circulating volume first
- Paracetamol dose-adjusted for severe impairment
- Morphine titrated carefully, metabolites accumulate in renal failure
- Monitor urine output and electrolytes
Child with liver disease
- Lower paracetamol daily ceiling; avoid in decompensated disease
- NSAIDs avoided with coagulopathy or portal hypertension (bleeding, renal injury)
- Opioids titrated cautiously; consider non-opioid multimodal first
- Specialist pain and hepatology input
Child with cognitive impairment
- Use the revised FLACC to score pain reliably
- Low threshold to treat; assume pain before behaviour
- Structured, written pain plan across carers and settings
- Beware altered opioid sensitivity in some syndromes
The child with persistent or chronic pain — juvenile idiopathic arthritis, cancer pain, neuropathic pain, complex regional pain syndrome — extends the ladder upward and sideways rather than simply increasing the opioid. Adjuvant analgesics come into their own: gabapentinoids and antidepressants for neuropathic pain, ketamine as an opioid-sparing infusion in the perioperative and critical-care setting, and disease-modifying therapy for the underlying cause. A specialist paediatric pain team coordinates the pharmacological, physical and psychological components, because chronic pain in a child is a biopsychosocial problem and the opioid is rarely the whole answer. The principle that unifies all four scenarios is the same: the right class, the right weight-based dose, the cap, and the reassessment, adjusted for the child in front of you. [11] [12]
Complications & Pitfalls
The preventable errors cluster at predictable points, and naming them is half of avoiding them. The first is under-dosing for weight, which leaves a child in pain and is most often the result of an estimated weight or an adult cap applied too early. The second is exceeding the paracetamol daily ceiling, almost always by combining preparations — a cold medicine and a separate paracetamol, or a fixed-dose combination whose paracetamol content is hidden — and it is prevented by asking, every time, what the carer has already given. The third is giving an NSAID to a dehydrated child, which precipitates acute kidney injury and is prevented by restoring volume first. The fourth is giving codeine or tramadol to a young or post-tonsillectomy child, which is now a regulatory contraindication and is prevented by replacing the prodrug opioids with low-dose morphine. The fifth is aspirin in a febrile child, avoided in under-16s because of Reye syndrome. [4] [7]
PAINS
The alternating pitfall deserves restating, because it is the commonest safe-looking practice that is not. Alternating paracetamol and ibuprofen without a clear plan confuses carers, blurs the dosing schedule, and invites a doubled dose or an exceeded ceiling; if dual therapy is used at all, it is for a distressed child who has not responded to monotherapy, with a written schedule and a dosing syringe. The formulation pitfall is the concentrated infant drop dosed as the children's suspension, or the fixed-dose combination tablet hiding the paracetamol content — both are prevented by checking the concentration and the active ingredients before the dose leaves the hand. The discharge pitfall is the child sent home with an opioid or a liquid paracetamol and no written mg-per-dose instruction and no dosing syringe; the defence is a written dose in mg, a dosing syringe, the maximum daily dose stated, and teach-back to the carer. [1] [12]
Prognosis & Disposition
Outcome in paracetamol hepatotoxicity is driven almost entirely by the time to N-acetylcysteine and the pattern of ingestion. A child who receives N-acetylcysteine within the early window, on the basis of a nomogram-positive level or a clear history, does well — the treatment is highly effective and the injury is prevented. Delay, a staggered ingestion that exhausts glutathione before the level is interpretable, or late presentation with established coagulopathy and encephalopathy, shift the prognosis toward acute liver failure and, in a small minority, transplant or death. The disposition of the paracetamol-exposed child is therefore conservative: treat when the criteria are met, observe the child who does not yet meet them, and seek the liver-transplant service early if the child deteriorates. [4] [5]
For the febrile child, the underlying cause drives the disposition, and the antipyretic response is one input among many. A well child who responds to comfort and an antipyretic, with a clear source and a safety-net, goes home. A toxic or non-responsive child, an infant in the high-risk age band, or a child with a serious source is admitted, investigated and treated. The safety-net written for the family names the features that should bring the child back — reduced feeding, reduced wet nappies, lethargy, a fever that does not settle, a non-blanching rash — and is the link between the disposition and the outcome. For the opioid adverse event, prognosis is driven by the speed of naloxone and the availability of monitoring, and a child who has received naloxone is observed for recurrence because the opioid outlasts the antidote. [2] [12]
Special Populations
The neonate is dosed with weight-band figures from a neonatal formulary, a lower paracetamol daily ceiling reflecting hepatic immaturity, and opioids given cautiously with monitoring for apnoea; procedural pain is anchored in non-pharmacological measures, especially oral sucrose, breastfeeding and non-nutritive sucking. The child with cognitive impairment or communication difficulty is assessed with the revised FLACC, carries a low threshold to treat pain, and benefits from a written pain plan shared across carers and settings, because under-treated pain is the failure mode and a structured plan is the defence. [11] [12]
The child with renal impairment is managed without NSAIDs, with paracetamol dose-adjusted for severe impairment and morphine titrated carefully and monitored, because the morphine metabolites accumulate in renal failure and the NSAID is nephrotoxic in the under-perfused kidney. The child with liver disease or malnutrition carries a lower paracetamol ceiling, an NSAID caution, and careful opioid titration. The Indigenous, remote, migrant or socioeconomically disadvantaged family is supported with clear dosing instructions, a dosing syringe, accessible language and teach-back, follow-up that the family can reach, and culturally safe communication — because the safety-net only closes if the family can act on it, and the home dosing error is concentrated where the instructions are least clear. The principle that unifies these populations is the same: the class is constant, the number changes with the child, and the check is never optional. [2] [4]
Evidence, Guidelines & Regional Differences
The evidence base is strongest where the stakes are highest. The alternating question was addressed by the 2024 network meta-analysis, which found that short-term dual therapy with paracetamol and ibuprofen lowered temperature faster and for longer than either agent alone, but with a modest effect size and an increased risk of dosing error — supporting a single-agent-first position with selective dual therapy rather than routine alternating. The codeine and tramadol restriction rests on the post-marketing reports of deaths in children, particularly after tonsillectomy, and on the pharmacogenetic understanding of CYP2D6 ultrarapid metabolism; the FDA and MHRA contraindications in children under 12 and after tonsillectomy are the regulatory consequence, and the observation that over-prescribing nonetheless persists is the ongoing quality problem. [1] [7]
Paracetamol poisoning management (Chiew 2020; Chiew 2018)
Key finding
The ANZ guideline and the Cochrane review support an N-acetylcysteine regimen (a 150 mg per kg intravenous loading dose, then weight-banded maintenance) guided by a four-hour paracetamol level on the treatment nomogram, and a low threshold to treat when ingestion is staggered or the time unknown. N-acetylcysteine is effective and the early window is the treatable window.
Codeine and tramadol after tonsillectomy (Robb 2013; Kohler 2020)
Key finding
Post-marketing reports of codeine-related deaths in children after tonsillectomy, particularly in CYP2D6 ultrarapid metabolisers with obstructive sleep apnoea, led to the FDA and MHRA contraindications. Continued periprocedural prescribing nonetheless persisted after the black-box warning.
Regional formularies converge on the doses but differ slightly at the edges. The BNFc, the AMH Children's Dosing Companion and the Royal Children's Hospital Melbourne guidelines agree on paracetamol 15 mg per kg per dose with a 60 mg per kg per day ceiling and a 4 g per day adult cap. They differ on the ibuprofen lower age cut-off — three months (and over 5 kg) in the ANZ and many formularies, with some preferring six months — and the prescriber states the source. The WHO analgesic ladder, adapted for children, is the unifying framework, and the single-source discipline (one current formulary, checked each time) prevents the mixed-figure error. Where the evidence is genuinely thin — antipyretics to prevent febrile seizure recurrence, sucrose for sustained procedures, the weight scalar for the obese child on an opioid — the position is stated honestly and the uncertainty named rather than filled from memory. [2] [6]
Exam Pearls
Self-test — the alternating trap
A worried parent asks whether they should "just alternate paracetamol and ibuprofen every two hours" for their febrile toddler. What is the correct position? [1]
Routine alternating is not recommended. Although short-term dual therapy can lower temperature modestly faster than either agent alone, it increases dosing error, parental confusion and the risk of doubled or exceeded doses. Use a single effective agent with a clear written plan first; reserve dual therapy for a distressed child who has not responded to monotherapy, with a written dosing schedule, a maximum daily dose stated, and a dosing syringe for the family. Ask what the child has already been given, because the commonest ceiling breach is a second preparation the carer did not realise contained paracetamol. [1] [2]
The high-yield one-liners: paracetamol is analgesic and antipyretic but a weak anti-inflammatory; the NSAIDs add a true anti-inflammatory action through peripheral COX inhibition; morphine is a pure analgesic with no antipyretic effect and no analgesic ceiling, which is why it is titrated and monitored. The antipyretic response never excludes serious bacterial infection. The neonate's procedural analgesia of first resort is oral sucrose with non-nutritive sucking and breastfeeding. The post-tonsillectomy child receives no codeine and no tramadol. The discharge defence is a written dose in mg, a dosing syringe, the daily maximum stated, and teach-back. And the single question that prevents most paracetamol disasters is the one the prescriber asks every time: what has the child already been given? [2] [11]
References
- [1]De la Cruz-Mena, J E; López-González, E; López-López, M J; et al. Short-term Dual Therapy or Mono Therapy With Acetaminophen and Ibuprofen for Fever: A Network Meta-Analysis Pediatrics, 2024.PMID 39318339
- [2]Paul, I M; Yestraan, J; McGuire, K; et al. Acetaminophen and ibuprofen in the treatment of pediatric fever: a narrative review Curr Med Res Opin, 2021.PMID 33966545
- [3]Rainsford, K D Ibuprofen: pharmacology, efficacy and safety Inflammopharmacology, 2009.PMID 19949916
- [4]Chiew, A L; Fountain, J S; Greig, R; et al. Updated guidelines for the management of paracetamol poisoning in Australia and New Zealand Med J Aust, 2020.PMID 31786822
- [5]Chiew, A L; Gluud, C; Brok, J; Buckley, N A Interventions for paracetamol (acetaminophen) overdose Cochrane Database Syst Rev, 2018.PMID 29473717
- [6]Schrör, K Aspirin and Reye syndrome: a review of the evidence Paediatr Drugs, 2007.PMID 17523700
- [7]Kohler, J E; Downard, C D; Heiss, K F; et al. Continued Prescribing of Periprocedural Codeine and Tramadol to Children after a Black Box Warning J Surg Res, 2020.PMID 32693330
- [8]Robb, P J More codeine fatalities after tonsillectomy in North American children. Time to revise prescribing practice! Clin Otolaryngol, 2013.PMID 24165486
- [9]Kauffman, R E; Sawyer, L A; Scheinbaum, M L Ibuprofen and increased morbidity in children with asthma: fact or fiction? Paediatr Drugs, 2004.PMID 15449966
- [10]Pywell, A; Cashin, P; Dyer, J; Mills, A C Does topical Amethocaine cream increase first-time successful cannulation in children compared with a eutectic mixture of local anaesthetics (EMLA) cream? A systematic review and meta-analysis of randomised controlled trials Emerg Med J, 2015.PMID 25351196
- [11]Pillai Riddell, R; Yamada, J; Harrison, D; et al. Non-pharmacological management of infant and young child procedural pain Cochrane Database Syst Rev, 2023.PMID 37314064
- [12]Parikh, J M; Turner, R; Tang, A; Baehner, F An update on the safety of prescribing opioids in pediatrics Expert Opin Drug Saf, 2019.PMID 30650988