Paeds · clinical-pharmacology-and-therapeutics
Cardiovascular medicines in children
Also known as Paediatric cardiovascular drugs · Cardiac medications in children · Antihypertensives in children · Paediatric antiarrhythmics · Ductal and inotropic therapy in children
A fellowship approach to prescribing cardiovascular medicines in children, covering the diuretics, ACE inhibitors and beta-blockers used in heart failure, the inotropes digoxin and milrinone, the antiarrhythmics adenosine, amiodarone, flecainide and sotalol, the vasodilator antihypertensives amlodipine, labetalol, hydralazine and sodium nitroprusside, prostaglandin E1 for duct-dependent congenital heart disease, and the pulmonary vasodilators such as sildenafil — with weight-based doses, developmental pharmacokinetics, monitoring and the high-risk adverse effects that shape every prescription.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a two-month-old turning grey on the postnatal ward, a five-year-old with a racing narrow-complex tachycardia, and a teenager in the emergency department with a blood pressure of 180 over 110. Each child needs a cardiovascular medicine, and in each case the medicine is powerful enough to rescue or to harm. The discipline of prescribing these drugs in childhood is built on one idea: the dose is matched to the child's weight and developmental physiology, and then watched for the effect the drug is meant to produce and the harm it is capable of causing. [1] [4]
A cardiovascular medicine in paediatric practice is any drug whose primary action is on the heart, the circulation, or the vascular tone. That includes the drugs used for heart failure, arrhythmia, hypertension, duct-dependent congenital heart disease and pulmonary hypertension. What sets these drugs apart is how narrow the gap is between the dose that helps and the dose that harms, and how much that gap moves with age. A neonate clears digoxin slowly and tolerates prostaglandin E1 apnoea; a school-age child clears a beta-blocker faster than an adult per kilogram; a teenager on an ACE inhibitor needs pregnancy counselling. The same mg-per-kilogram dose is never assumed to behave the same way at two ages. [1]
From the prescription to a safe, on-target cardiovascular drug
1 · Confirm the current weight
Weigh the child and recheck at intervals; every cardiovascular dose is calculated per kilogram against a current weight.
2 · Correct for age and organs
Adjust for developmental clearance (neonate, infant, adolescent) and for renal or hepatic function before the first dose.
3 · Give the loading or starting dose
Start low where the drug is high-risk (ACE inhibitor, beta-blocker, vasodilator); load where a rapid effect is needed (adenosine, digoxin, prostaglandin E1).
4 · Monitor the effect and the harm
Watch the heart rate, blood pressure, saturation, QTc, renal function and potassium, and the drug level where indicated.
5 · Titrate and review
Up-titrate over days to weeks for chronic drugs; set a stop or wean date for high-risk acute drugs; review interactions at every change.
Classification
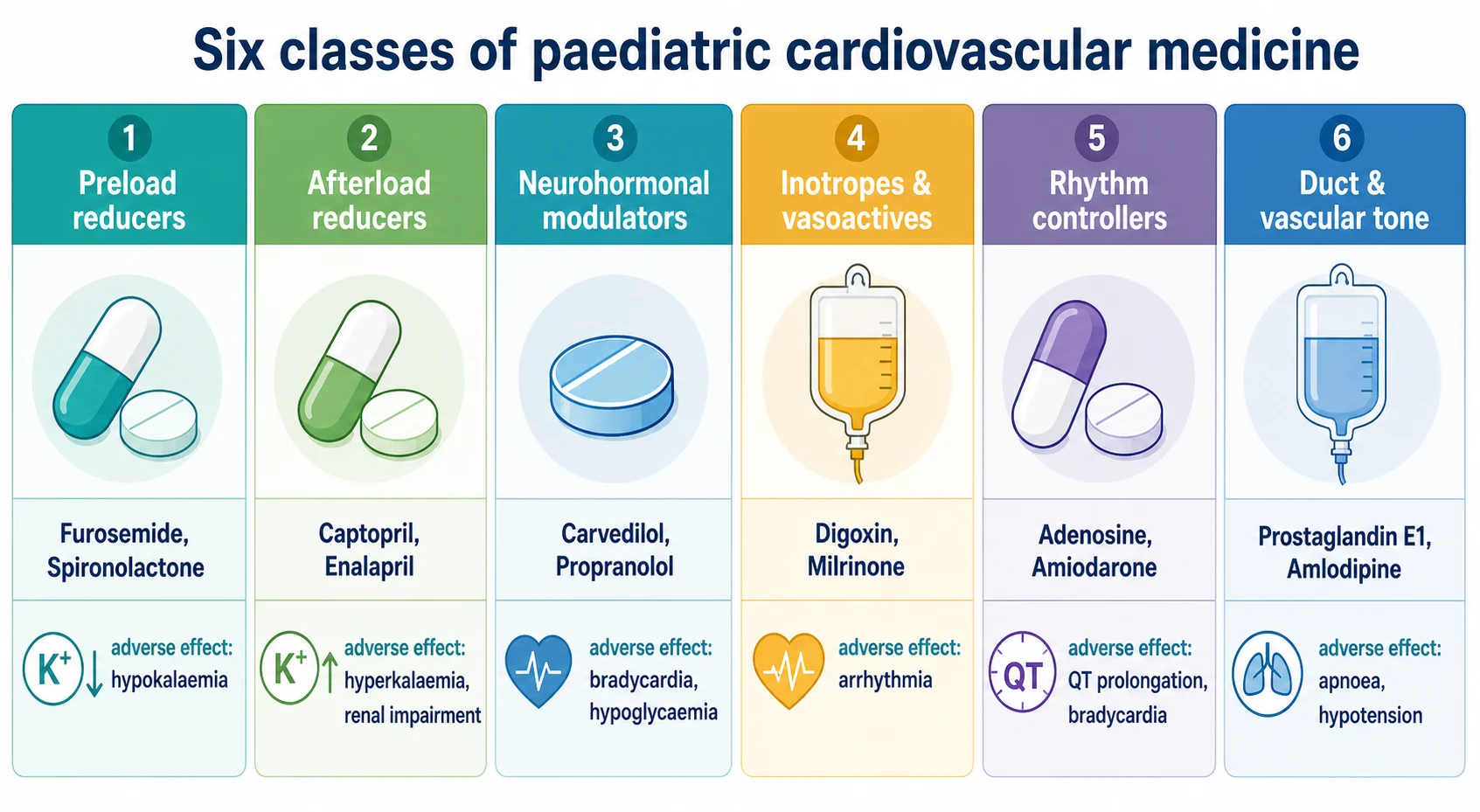
The cardiovascular medicines a general paediatrician prescribes sort into six practical groups, and the group tells you which problem the drug is solving. Preload reducers — the loop diuretics furosemide and the potassium-sparing spironolactone — pull fluid off the overloaded circulation. Afterload reducers — the ACE inhibitors captopril and enalapril and the angiotensin receptor blockers — widen the vessels so the failing ventricle ejects against less resistance. Neurohormonal modulators — the beta-blockers carvedilol and propranolol — dampen the sympathetic and renin-angiotensin overdrive that worsens chronic heart failure. Inotropes and vasoactives — digoxin, milrinone, dopamine and dobutamine — strengthen contractility or support blood pressure. Rhythm controllers — adenosine, amiodarone, flecainide and sotalol — terminate or prevent arrhythmia. Ductal and vascular tone agents — prostaglandin E1 to keep a duct open, the vasodilator antihypertensives, and the pulmonary vasodilators — set the tone of a single vessel or vascular bed. [4] [5]
| Class | Representative drugs | Problem solved | Key adverse effect |
|---|---|---|---|
| Preload reducers | Furosemide, spironolactone, amiloride | Volume overload, oedema | Hypokalaemia, hyponatraemia, dehydration |
| Afterload reducers | Captopril, enalapril, losartan | Heart failure, hypertension | Hyperkalaemia, renal impairment, cough |
| Neurohormonal modulators | Carvedilol, propranolol, metoprolol | Chronic heart failure, arrhythmia, haemangioma | Bradycardia, hypotension, hypoglycaemia in infants |
| Inotropes and vasoactives | Digoxin, milrinone, dopamine, dobutamine | Low cardiac output, poor perfusion | Arrhythmia, digoxin toxicity, tachyarrhythmia |
| Rhythm controllers | Adenosine, amiodarone, flecainide, sotalol | Supraventricular and ventricular arrhythmia | Pro-arrhythmia, QT prolongation, bradycardia |
| Ductal and vascular tone agents | Prostaglandin E1, amlodipine, labetalol, hydralazine, sodium nitroprusside, sildenafil | Duct-dependent disease, hypertension, pulmonary hypertension | Apnoea and fever (PGE1), hypotension, cyanide toxicity |
Epidemiology & Risk Factors
Cardiovascular drugs are everyday paediatric prescribing. On a single ward round a general paediatrician will meet furosemide in the child with bronchopulmonary dysplasia or heart failure, captopril or carvedilol in the child with a cardiomyopathy, amlodipine in the child with chronic kidney disease, and adenosine in the child who is brought in tachycardic. In tertiary practice the list grows to milrinone after cardiac surgery, prostaglandin E1 for the duct-dependent neonate, and sildenafil for pulmonary hypertension. The drugs are common; what separates safe from unsafe practice is the discipline of dosing by weight and watching for the specific harm. [4]
Several factors push a cardiovascular drug toward failure or harm. Young age is the most powerful, because the renal and hepatic machinery that clears a drug is still maturing, and because an infant's high total body water and low albumin change both the distribution and the free fraction of a drug. Congenital and structural heart disease multiplies the number of cardiac drugs a child takes, and with it the risk of interaction. Renal impairment slows the clearance of digoxin, the ACE inhibitors and milrinone. Critical illness changes the volume of distribution and the response to vasoactives. And drug interactions — amiodarone raising the digoxin level, a potassium-sparing diuretic compounding ACE-inhibitor hyperkalaemia, sildenafil and nitrate together causing profound hypotension — perturb the effect of a dose that looked safe on paper. [1]
Neonate
Immature clearance
- Low GFR slows digoxin and milrinone clearance
- High total body water changes distribution of water-soluble drugs
- Low albumin raises the free fraction of bound drugs
- Prostaglandin E1 apnoea is common and anticipated
Infant
Rapid maturation
- Hepatic enzyme activity rises fast and changes beta-blocker clearance
- Risk of hypoglycaemia with propranolol and beta-blockers
- Verapamil can cause cardiovascular collapse — avoid in infancy
- Single-ventricle infants need staged drug adjustment
Child with organ impairment
Reduced clearance
- Renal disease slows digoxin, ACE inhibitor and milrinone clearance
- Hepatic disease slows amiodarone metabolism
- Reduce dose or extend the interval
- Monitor potassium, creatinine and the drug level
Child on interacting drugs
Additive or competing effects
- Amiodarone raises the digoxin level
- ACE inhibitor plus potassium-sparing diuretic risks hyperkalaemia
- Sildenafil plus nitrate risks profound hypotension
- Recheck after starting or stopping the interacting drug
Pathophysiology
The reason cardiovascular drugs behave so differently in children is that the dose a weight carries to the bloodstream is shaped by four developmental processes, and each one changes with age. [1]
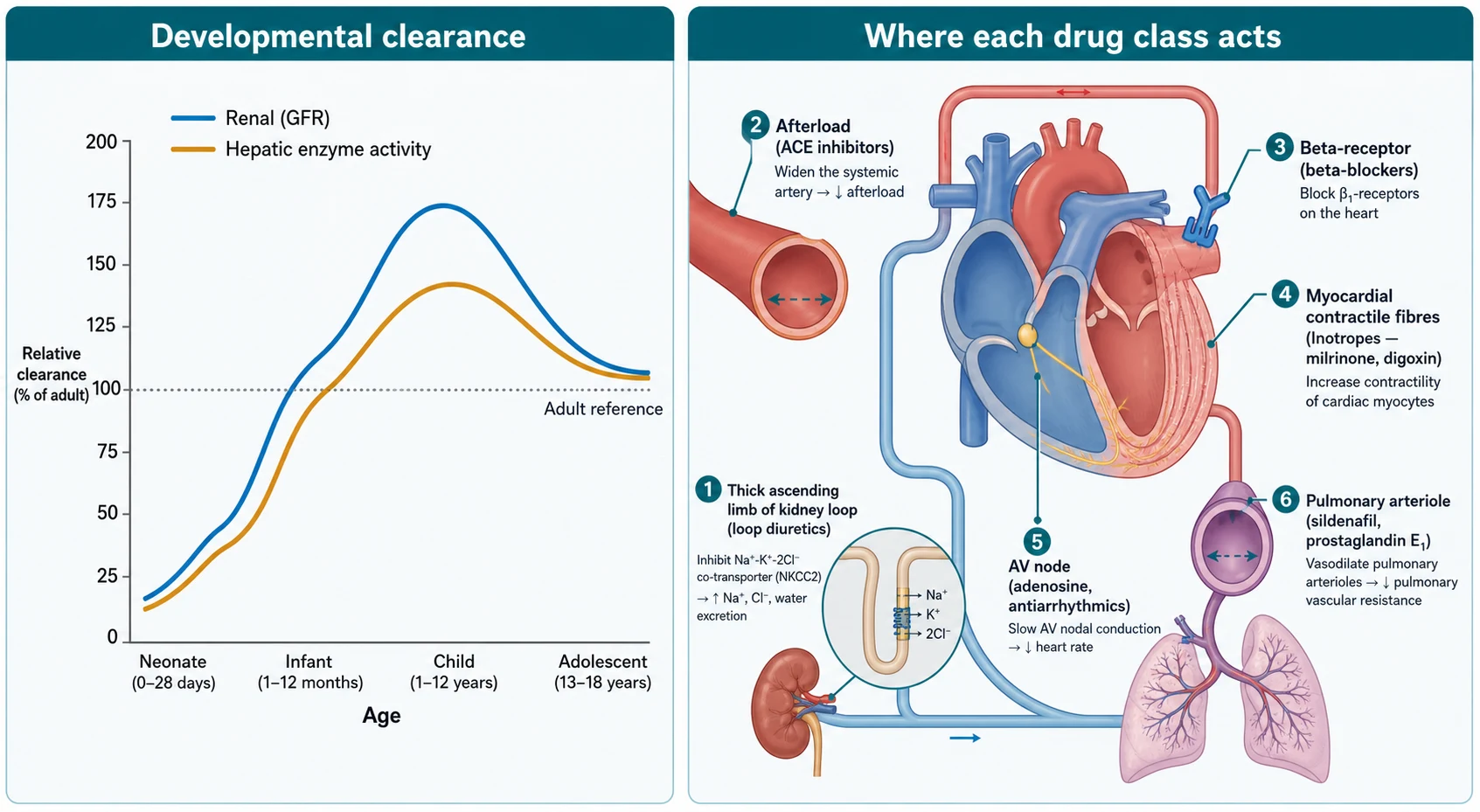
Absorption of oral cardiovascular drugs is more variable in the neonate because gastric acidity is low and emptying is irregular, but it approaches adult patterns by infancy. Distribution changes with body composition: the neonate's high total body water enlarges the volume of distribution of water-soluble drugs such as digoxin and lidocaine, so the same mg-per-kilogram dose reaches a lower peak. Metabolism follows a biphasic curve — hepatic enzyme activity is slow at birth, then overshoots adult per-kilogram rates in early childhood, before settling. Elimination mirrors that pattern: glomerular filtration is low at birth, reaches adult values by around eight to twelve months, and exceeds adult per-kilogram values during childhood. The practical consequence is that a neonate needs a lower per-kilogram dose or a longer interval for renally cleared drugs, and a young child may need a higher per-kilogram dose to hold a level. [1]
The mechanism of each class then predicts both the effect and the harm. A loop diuretic blocks sodium-potassium-chloride reabsorption in the thick ascending limb, so it pulls off fluid and, with it, potassium. An ACE inhibitor blocks the conversion of angiotensin I to angiotensin II, so it lowers afterload and aldosterone — and risks hyperkalaemia and a rise in creatinine. A beta-blocker antagonises adrenergic stimulation of the heart, so it slows the rate and unloads the failing ventricle — and risks bradycardia, hypotension and, in the infant, hypoglycaemia. Milrinone inhibits phosphodiesterase-3, raising intracellular cyclic adenosine monophosphate and contractility while vasodilating — so it improves low cardiac output, and risks hypotension and arrhythmia. Adenosine blocks conduction through the atrioventricular node, terminating a re-entry supraventricular tachycardia — and it briefly asystoles, so it is given fast and watched on a monitor. [4] [6]
Clinical Presentation
The clinical presentation of a cardiovascular drug problem is usually a change in the child rather than a change in the chart. The tired, slow-to-feed infant on a beta-blocker may be bradycardic or hypoglycaemic. The vomiting child on digoxin whose rate has slowed may be digoxin-toxic. The hypotensive child on a recently up-titrated ACE inhibitor may simply be over-vasodilated. The cyanotic neonate whose saturation is falling may have a duct closing, and the same neonate on prostaglandin E1 who becomes febrile, hypotensive or apnoeic is showing you the drug rather than the disease. [4]
Adverse effects declare themselves along a recognisable ladder for each drug. With digoxin, anorexia and nausea come first, then bradycardia and arrhythmia; toxicity is precipitated by hypokalaemia, renal impairment, and the interaction with amiodarone. With amiodarone, the immediate risks are bradycardia and QT prolongation, and the delayed risks are thyroid dysfunction, hepatic injury, pulmonary fibrosis and corneal microdeposits. With furosemide, the signs are electrolyte loss — hypokalaemia, hyponatraemia, and a contracted volume — and the renal consequence of long-term use. With the ACE inhibitors, the acute signal is hypotension and the subacute signal is a rising creatinine and potassium. With sodium nitroprusside, the late signal of cyanide toxicity is a rising lactate and a falling responsiveness despite a controlled blood pressure. [4] [5]
The child who is not responding as expected is another presentation. The heart failure child whose oedema is worsening despite furosemide may need a higher dose, a second diuretic, or investigation of a cause. The tachycardic child whose rate has not broken with two adenosine doses may have an incorrect diagnosis (a junctional or ventricular rhythm rather than re-entry), a technical failure of administration, or a need for a higher dose or cardioversion. The hypertensive child whose pressure is not falling may need a different agent or an evaluation for a secondary cause. [4]
Differential Diagnosis
When a child deteriorates on a cardiovascular drug, your first job is to decide whether the drug is the cause, the disease is progressing, or both. A bradycardic child on a beta-blocker may simply be over-medicated, but the same heart rate in a septic or hypoxic child means something very different. A hypotensive child on a vasodilator may be over-dosed, or may be bleeding, septic, or dehydrated. A rising creatinine on an ACE inhibitor may be drug effect, volume depletion, or intrinsic renal disease. [4]
The discriminating principle is to hold the suspect drug, re-examine the child, and re-test. If the child improves when the drug is held, the drug is the likely cause. If the child does not improve, the disease is progressing and the drug is bystander. Two specific traps deserve naming. In the digoxin-toxic child with vomiting and bradycardia, the differential includes any cause of bradycardia, but a digoxin level, a potassium, and the history of a recent dose change or interaction make the diagnosis. In the apnoeic neonate on prostaglandin E1, the differential includes sepsis, metabolic disease and intracranial pathology, but a prostaglandin-effect apnoea is common and expected — the response is supportive airway care and, where possible, a small dose reduction, not an infection work-up alone. [4] [10]
Clinical & Bedside Assessment
Bedside assessment of a cardiovascular drug means checking the child and the chart together. Before you prescribe, weigh the child and confirm the weight is current — a cardiovascular dose calculated against a weight from last month is a common and dangerous error. Examine the heart rate, the blood pressure, the perfusion, the hydration, and the oxygen saturation. Read the renal function, the electrolytes, and the magnesium. Look at the ECG for the QTc if you are about to start an antiarrhythmic. Only then write the dose. [1]
After the dose is given, the monitoring is drug-specific. For the ACE inhibitors and ARBs, recheck the urea, electrolytes and creatinine within one to two weeks of starting and after each dose change, because the harm is hyperkalaemia and a rising creatinine. For the beta-blockers, watch the heart rate and blood pressure and, in the infant, the glucose. For digoxin, watch the heart rate and request a level when toxicity is suspected or at steady state. For amiodarone and sotalol, check the QTc before and during therapy. For the vasoactive infusions in intensive care, titrate to a haemodynamic target and re-examine with each change. [4] [7]
When a child is on a cardiovascular drug and becomes unwell, examine them for the toxicity that fits the drug. For digoxin, look for bradycardia and a slow atrioventricular rhythm. For a beta-blocker, look for bradycardia, hypotension and hypoglycaemia. For an ACE inhibitor, look for hypotension and a rising creatinine. For prostaglandin E1, look for apnoea, fever and hypotension. For sodium nitroprusside, look for a rising lactate and falling responsiveness. The drug a child is taking is always a candidate cause of any new presentation, and naming the fit between drug and sign is the bedside skill. [4] [10]
Investigations
The investigations that govern cardiovascular prescribing are simple and repeatable. Urea, electrolytes and creatinine are mandatory before and during ACE inhibitor, ARB, diuretic and digoxin therapy, because these drugs touch the kidney and the potassium. Magnesium matters for the child on a diuretic or an antiarrhythmic, because hypomagnesaemia both accompanies diuretic use and prolongs the QT. The ECG and QTc are mandatory before and during amiodarone, sotalol, flecainide and digoxin therapy, because each can prolong conduction or repolarisation. A drug level is indicated for digoxin when toxicity is suspected or to confirm a steady-state level, and for amiodarone or flecainide in selected chronic arrhythmia care. [4]
| Drug | Baseline tests | Ongoing monitoring | Trigger to act |
|---|---|---|---|
| ACE inhibitors and ARBs (captopril, enalapril, losartan) | Urea, electrolytes, creatinine; blood pressure | Urea, electrolytes, creatinine and blood pressure within 1–2 weeks and after each change | Rising creatinine or potassium; symptomatic hypotension |
| Beta-blockers (carvedilol, propranolol) | Heart rate, blood pressure; glucose in infants | Heart rate and blood pressure at each change; glucose in the infant | Symptomatic bradycardia or hypotension; hypoglycaemia |
| Digoxin | ECG, renal function, potassium | Heart rate; digoxin level at steady state or if toxicity suspected | Bradycardia or arrhythmia; digoxin level above range; hypokalaemia |
| Amiodarone, sotalol | ECG with QTc; thyroid and liver function | QTc; thyroid, liver and (long term) pulmonary and ocular surveillance | QTc prolongation; bradycardia; thyroid or liver dysfunction |
| Prostaglandin E1 | Airway and ventilation plan; blood pressure | Continuous saturation and respiratory rate; temperature and blood pressure | Apnoea, fever or hypotension; inadequate ductal response |
| Sodium nitroprusside | Continuous arterial blood pressure; lactate | Blood pressure titrated; lactate and mental state if prolonged | Excess hypotension; rising lactate (cyanide toxicity) |
The interpretation of these tests is what guides titration. A creatinine that rises by more than around thirty per cent after an ACE inhibitor is started usually means the dose should be held or reduced and the child reassessed for volume depletion or renal artery disease. A QTc that exceeds four hundred and fifty milliseconds, or that lengthens after an antiarrhythmic, is a signal to reduce the dose or reconsider the drug. A digoxin level above the therapeutic range with bradycardia is toxicity until proven otherwise. The number is only ever interpreted in the child. [4] [7]
Management — Resuscitation
The resuscitation moments in cardiovascular prescribing are the duct-dependent neonate, the tachycardic compromised child, and the hypertensive emergency. Each is time-critical, and each hinges on a single drug given at the right dose and watched for the right effect. [10]
The duct-dependent neonate — a child whose circulation depends on an open ductus arteriosus — turns cyanotic, breathes fast, and collapses as the duct closes in the first days of life. The resuscitative drug is prostaglandin E1 (alprostadil), started at 0.01 to 0.05 microgram per kilogram per minute intravenously and titrated upward to a typical maximum around 0.1 microgram per kilogram per minute until the duct reopens and the saturation rises toward a target of seventy-five to eighty-five per cent. Three adverse effects are expected and prepared for: apnoea (have a plan for intubation), fever, and hypotension. The prostaglandin is a bridge to definitive anatomy repair, not a treatment itself. [10]
The haemodynamically compromised child in supraventricular tachycardia needs the rhythm terminated. Vagal manoeuvres are tried first in a stable child. If they fail or the child is compromised, adenosine is given as a rapid intravenous bolus of 0.1 milligram per kilogram (maximum 6 mg for the first dose), followed immediately by a saline flush, escalating to 0.2 milligram per kilogram (maximum 12 mg) if the first dose fails. Adenosine must be given fast, through a proximal line, with a flush chasing it, because it is metabolised within seconds. If the tachycardia is broad-complex or the child is severely compromised, synchronised cardioversion is the safer path. Adenosine is diagnostic as well as therapeutic — it blocks the atrioventricular node, so a re-entry tachycardia breaks, while an atrial tachycardia may reveal its atrial origin. [7]
The child with a hypertensive emergency — a blood pressure well above the ninety-fifth percentile with end-organ signs such as encephalopathy, cardiac failure or seizures — needs a controlled reduction, not a rapid one. A reduction of around twenty-five per cent in the first eight hours is the aim, using a titratable agent. Labetalol is given as an intravenous bolus of 0.2 to 0.5 milligram per kilogram followed by an infusion of 0.25 to 3 milligrams per kilogram per hour, or hydralazine as 0.1 to 0.2 milligram per kilogram per dose every four to six hours. Sodium nitroprusside, at 0.3 to 1 microgram per kilogram per minute titrated (short-term maximum around 8 micrograms per kilogram per minute), is reserved for the most tightly monitored child because of the risk of cyanide toxicity with prolonged use. [4]
Management — Definitive & Stepwise
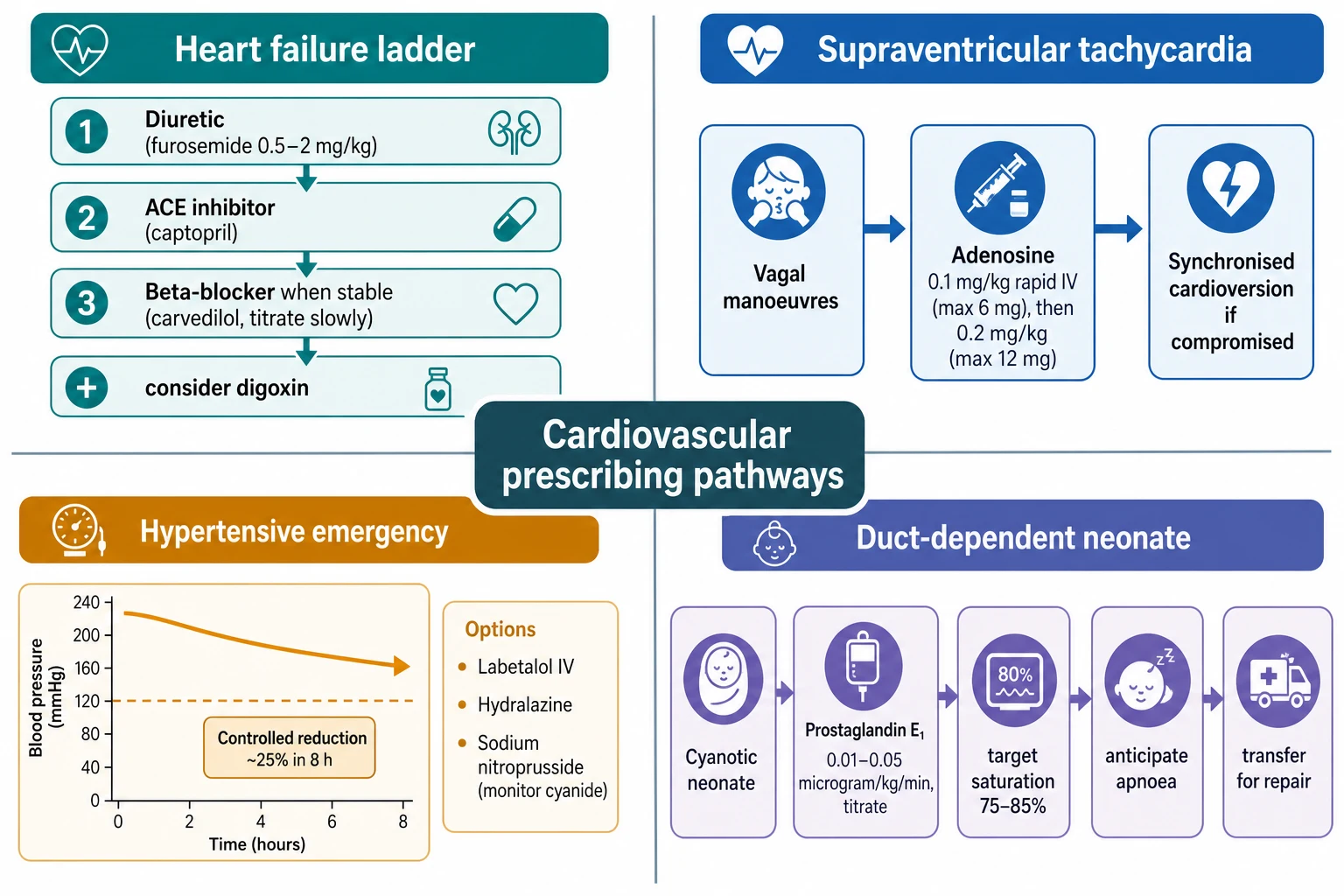
The definitive management of paediatric heart failure is a stepwise neurohormonal and symptomatic ladder. Diuretics relieve congestion first: furosemide at 0.5 to 2 milligrams per kilogram per dose orally or intravenously, one to four times daily, with spironolactone at 1 to 3 milligrams per kilogram per day for potassium-sparing and aldosterone antagonism. ACE inhibitors are then added to reduce afterload and the neurohormonal burden — captopril in the infant at an initial 0.15 to 0.3 milligram per kilogram per dose every eight hours, or enalapril at 0.1 milligram per kilogram once daily titrated upward. Beta-blockers are added once the child is stable, carvedilol started at 0.05 to 0.1 milligram per kilogram twice daily and titrated over weeks to 0.3 to 0.5 milligram per kilogram twice daily. Digoxin may be added for symptomatic benefit, with an oral maintenance dose of 5 to 10 micrograms per kilogram per day in divided doses. [4] [5]
Weight-based doses for common paediatric cardiovascular drugs (verify against the current local formulary)
The beta-blocker and ACE inhibitor evidence in children deserves a clear-eyed summary, because it is the part of paediatric heart failure pharmacology that examiners test for nuance. The landmark carvedilol randomised trial of Shaddy and colleagues in children and adolescents with heart failure did not show a significant benefit of carvedilol over placebo on the primary composite outcome — a result that differs sharply from adult heart failure, where beta-blockers reduce mortality. The lesson is that paediatric heart failure is not adult heart failure, and that beta-blockers are still used in carefully selected, stable children under cardiology guidance, titrated slowly. The single-ventricle enalapril trial of Hsu and colleagues likewise showed no improvement in the primary growth and haemodynamic outcomes for infants with a single ventricle after stage-one palliation. These trials explain why paediatric heart failure prescribing is extrapolated and specialist-supervised rather than evidence-rigid. [2] [3]
For the child in low cardiac output syndrome after cardiac surgery, the vasoactive of evidence is milrinone. The PRIMACORP trial of Hoffman and colleagues showed that prophylactic high-dose milrinone — a loading dose of 50 micrograms per kilogram over thirty to sixty minutes followed by an infusion of 0.75 microgram per kilogram per minute — reduced the composite outcome of low cardiac output syndrome or death compared with placebo in infants and young children after corrective congenital heart surgery. Milrinone improves inotropy and lusitropy while reducing afterload, and its main adverse effect is hypotension, often managed with a fluid bolus or a low-dose vasopressor. Dopamine (2 to 20 micrograms per kilogram per minute) and dobutamine (2 to 20 micrograms per kilogram per minute) remain the catecholamine inotropes for the child who needs both contractility and pressure. [6]
Specific Subtypes & Scenarios
The duct-dependent neonate is the child where one drug, given early, changes the outcome. A duct-dependent lesion — hypoplastic left heart syndrome, critical aortic stenosis, coarctation, interrupted aortic arch, pulmonary atresia, severe tetralogy or transposition — relies on the ductus arteriosus to carry blood to the lungs or the body. As the duct closes in the first hours to days of life, the child turns cyanotic, breathes fast, becomes acidotic, and collapses. Prostaglandin E1 reopens and keeps the duct patent while the child is transferred and repaired. Start at 0.01 to 0.05 microgram per kilogram per minute, titrate to the response (a rising saturation, a warming perfusion, a falling lactate), and prepare for the adverse effects — apnoea (with an intubation plan), fever, and hypotension. The target saturation in most duct-dependent cyanotic disease is around seventy-five to eighty-five per cent, not a normal saturation, because too much pulmonary flow steals from the systemic circulation. [10]
The child with a single-ventricle circulation moving through staged palliation needs careful drug adjustment between stages. Diuretics manage the volume load; ACE inhibitors are sometimes used to modulate afterload, though the single-ventricle enalapril trial showed no benefit on the primary outcome for infants after stage one. Between stages the balance of pulmonary and systemic flow is fragile, and every cardiovascular drug — diuretic, afterload reducer, vasoactive — is titrated against that balance. [3] [4]
The child in low cardiac output syndrome after cardiac surgery is managed with milrinone prophylaxis and the catecholamine inotropes. The child with pulmonary arterial hypertension is managed with pulmonary vasodilators: sildenafil at 0.5 milligram per kilogram per dose three times daily orally, bosentan (an endothelin antagonist under specialist supervision), and in the acute setting inhaled nitric oxide. A critical caution is that sildenafil must never be combined with nitrate, because the combination can cause profound and life-threatening hypotension. The infant with a severe infantile haemangioma treated with oral propranolol at 1 milligram per kilogram per day in divided doses (titrated to around 3 milligrams per kilogram per day) needs cardiovascular monitoring at initiation — heart rate, blood pressure, and glucose — because propranolol is a beta-blocker and carries the bradycardia, hypotension and hypoglycaemia risks of its class. [8] [9]
The first day of a duct-dependent neonate on prostaglandin E1
Complications & Pitfalls
The complications of cardiovascular drugs are the harms the drugs are capable of, and most are avoidable with the right dose and the right monitoring. Prostaglandin E1 causes apnoea, fever and hypotonia or hypotension — anticipated and prepared for. Digoxin causes anorexia, nausea, bradycardia and arrhythmia, precipitated by hypokalaemia, renal impairment, and the amiodarone interaction. Amiodarone causes immediate bradycardia and QT prolongation, and delayed thyroid, hepatic, pulmonary and ocular effects. Furosemide causes hypokalaemia, hyponatraemia, contraction alkalosis and, with long-term use, electrolyte and renal consequences. ACE inhibitors cause hyperkalaemia, a rising creatinine, and cough. Sodium nitroprusside causes cyanide and thiocyanate toxicity with prolonged or high-dose use, signalled by a rising lactate. [4] [5]
The dangerous dose errors in paediatric cardiovascular prescribing are the tenfold and the decimal-point errors — a prostaglandin E1 or digoxin dose written at ten times the intended value, or a milligram-per-kilogram dose misplaced by a decimal. The safeguards are a current weight, an independent check of high-risk drugs (digoxin, prostaglandin E1, infusions), and a unit check at every step. The classic interaction errors are giving amiodarone without reducing the digoxin dose (amiodarone raises the digoxin level), starting an ACE inhibitor with a potassium-sparing diuretic without checking the potassium, and combining sildenafil with nitrate. [4]
Principle
- Prescribe by current weight, correct for age and organs, titrate to effect
- Name the drug, dose, route, target and adverse effect in one breath
- Monitor the organ the drug endangers
Classes
- Diuretics: furosemide, spironolactone
- Afterload: captopril, enalapril
- Beta-blockers: carvedilol, propranolol
- Inotropes: digoxin, milrinone, dopamine, dobutamine
- Rhythm: adenosine, amiodarone, flecainide, sotalol
- Tone: prostaglandin E1, amlodipine, labetalol, hydralazine, sodium nitroprusside, sildenafil
Resuscitation doses
- Prostaglandin E1: 0.01–0.05 microgram/kg/min, titrate; anticipate apnoea
- Adenosine: 0.1 mg/kg rapid IV (max 6 mg), then 0.2 mg/kg (max 12 mg)
- Hypertensive emergency: controlled reduction ~25% in 8 h with labetalol or hydralazine
Heart failure
- Diuretic first, add ACE inhibitor, add beta-blocker when stable
- Carvedilol 0.05–0.1 mg/kg twice daily, titrate to 0.3–0.5 mg/kg twice daily
- Carvedilol and single-ventricle enalapril trials were negative on primary outcome
Inotropes
- Milrinone: load 50 micrograms/kg, then 0.25–0.75 microgram/kg/min (PRIMACORP)
- Dopamine and dobutamine: 2–20 micrograms/kg/min
- Digoxin maintenance: 5–10 micrograms/kg/day
Pitfalls
- Verapamil avoided in infants
- Amiodarone raises digoxin; reduce digoxin dose
- ACE inhibitor plus potassium-sparing diuretic: hyperkalaemia
- Sildenafil plus nitrate: profound hypotension
- Sodium nitroprusside: cyanide toxicity if prolonged
“Right drug by class → right weight-based dose → right correction for age and organs → right target (rate, pressure, saturation, QTc, potassium) → right monitoring of the organ the drug endangers → anticipate the named adverse effect for every drug.”
Prognosis & Disposition
The prognosis of a child on cardiovascular drugs depends on whether the right drug reaches the right target and whether the harms are caught early. For heart failure, the response to the diuretic, ACE inhibitor and beta-blocker ladder — falling filling pressures, improving perfusion, stabilising weight and renal function — predicts a child who can be managed as an outpatient under cardiology. For the duct-dependent neonate, prostaglandin E1 is a bridge: the prognosis is set by the anatomy and the definitive repair, not by the drug. For the child in supraventricular tachycardia, adenosine terminates the acute episode in most, and the decision to start a maintenance antiarrhythmic depends on the frequency, the mechanism, and the Wolff-Parkinson-White substrate. [4] [7]
Disposition is shaped by the drug, the target, and the monitoring burden. A child on an ACE inhibitor or beta-blocker whose heart failure is controlled and whose renal function and blood pressure are stable can be managed as an outpatient with structured review. A child on a high-risk infusion — milrinone, sodium nitroprusside, prostaglandin E1, a catecholamine — needs a high-dependency or intensive care bed and continuous monitoring. A child on long-term amiodarone needs an organised surveillance plan — thyroid, liver, eye, pulmonary, and QTc — and a clear weaning strategy, because amiodarone is not a forever drug. [4] [7]
Special Populations
The neonate needs age-adjusted cardiovascular dosing as a core safety measure, not a refinement. Low glomerular filtration slows the clearance of digoxin, the ACE inhibitors and milrinone; high total body water enlarges the volume of distribution of water-soluble drugs; and low albumin raises the free fraction of bound drugs. The neonate is also the patient for whom prostaglandin E1 is life-saving, and the patient most likely to be harmed by verapamil — which is why verapamil is avoided in infancy. The child with single-ventricle physiology or after Fontan requires careful diuretic, ACE inhibitor and vasodilator titration against the fragile balance of pulmonary and systemic flow. [1] [3]
The child with renal impairment needs dose adjustment of the renally cleared drugs — digoxin, the ACE inhibitors, milrinone and several diuretics — with interval extension or dose reduction and close monitoring. The adolescent girl on an ACE inhibitor or ARB needs pregnancy counselling and reliable contraception, because these drugs are teratogenic. For Aboriginal and Torres Strait Islander and Māori children, and children from remote settings, the burden of multiple cardiovascular medicines and repeated blood tests is real, and a coordinated plan with trusted venous access, clear communication, and a single responsible team reduces both missed doses and the distress of repeated needles. [1]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne Cardiology guidelines and Therapeutic Guidelines (eTG) are the primary references for paediatric cardiovascular drug doses, routes and monitoring, with state and institutional formularies operationalising them. For Aboriginal and Torres Strait Islander and Māori children, repeated blood sampling and multiple cardiac medicines carry a real burden, particularly for families travelling from remote settings, and a coordinated plan with trusted venous access and clear communication reduces both sampling failures and the distress of repeated needles. [4]
Global and low-resource settings: where paediatric cardiology and intensive care are distant, the principles — dose by weight, anticipate the named adverse effect, monitor the heart rate, blood pressure, saturation and potassium, and prepare for the prostaglandin E1 apnoea — hold even where a drug level cannot be measured. A coordinated transfer plan to a cardiac centre, with prostaglandin E1 running and the airway secured, is the single most important resuscitative action for the duct-dependent neonate in any setting. [10]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric cardiovascular pharmacology is strong in some places and conspicuously thin in others, and naming that distinction is part of safe prescribing. The strongest evidence is for milrinone in low cardiac output syndrome: the PRIMACORP randomised trial of Hoffman and colleagues showed that prophylactic high-dose milrinone reduced the composite outcome of low cardiac output syndrome or death after corrective congenital heart surgery in infants and children. The strongest caution comes from the negative paediatric heart failure trials: the carvedilol trial of Shaddy and colleagues did not meet its primary composite endpoint in children, and the single-ventricle enalapril trial of Hsu and colleagues did not improve the primary outcomes for infants after stage-one palliation. These trials explain why paediatric heart failure prescribing extrapolates from adult evidence and physiology, and why every prescription is specialist-supervised. [2] [3] [6]
The 2024 American Heart Association scientific statement on the pharmacological management of fetal and neonatal arrhythmias consolidates the modern approach to adenosine, amiodarone, flecainide, sotalol and digoxin in the youngest patients, and is the authoritative reference for paediatric antiarrhythmic prescribing. The pulmonary arterial hypertension pharmacology is summarised in the JAMA review of Ruopp and Cockrill and the comprehensive pharmacological review of Berman Rosenzweig and Barst, covering the calcium-sensitising, endothelin, phosphodiesterase-5 and prostacyclin pathways that now shape paediatric pulmonary hypertension care. [7] [8] [9]
The evidence is weaker where dosing rests on formulary tradition rather than trials — many paediatric cardiovascular doses are derived from pharmacokinetic studies, expert consensus, and the BNF for Children and RCH formularies rather than randomised outcome trials. Where the evidence is weak, state the dose, cite the formulary, and communicate the uncertainty rather than implying a precision the data do not support. [4]
Board and assessment distinctions
RACP current PREP curriculum candidates must apply safe prescribing, weight-based dosing and the pharmacological management of cardiac and haemodynamic disorders within the acute-illness and medication-safety learning objectives; first-year trainees from 2027 encounter it under quality-and-safety goals. RCPCH Progress+ embeds cardiovascular prescribing as a core patient-safety and cardiology outcome. The ABP General Pediatrics Content Outline covers pharmacology and medication management alongside cardiology. [1]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Given a clinical scenario, choose the correct cardiovascular drug, dose, adverse effect or first-line agent for heart failure, SVT, hypertensive emergency or duct-dependent disease |
| RACP DCE long case | Build a stepwise heart-failure or post-operative vasoactive regimen for a complex cardiac child, integrating pharmacology, interactions and monitoring |
| MRCPCH clinical | Explain a cardiovascular medicine plan to a family and demonstrate safe prescribing reasoning |
| ABP | Apply pharmacology and cardiology domain knowledge to select, dose, monitor and adjust a cardiovascular drug |
| RCPSC structured oral | Defend a prostaglandin E1, adenosine, milrinone or hypertensive-emergency plan across age groups |
Exam Pearls
Viva: why is prostaglandin E1 the first drug in a cyanotic neonate, and what adverse effects do you prepare for?
A cyanotic neonate in the first days of life with a duct-dependent lesion collapses as the ductus arteriosus closes. Prostaglandin E1 (alprostadil) reopens and keeps the duct patent, restoring pulmonary or systemic flow while definitive anatomy-specific repair is arranged. I start at 0.01 to 0.05 microgram per kilogram per minute and titrate upward to a typical maximum around 0.1 microgram per kilogram per minute, watching for a rising saturation toward a target of seventy-five to eighty-five per cent and a falling lactate. Three adverse effects are expected and prepared for: apnoea, for which I have an intubation plan; fever; and hypotension. Prostaglandin E1 is a bridge, not a treatment. [10]
Structured oral: a five-year-old has a narrow-complex tachycardia at 220 per minute and is compromised — walk me through adenosine
In a compromised child I prepare for synchronised cardioversion while I try to terminate the rhythm with adenosine. Vagal manoeuvres are reasonable only if they do not delay definitive care. Adenosine is given as a rapid intravenous bolus of 0.1 milligram per kilogram, maximum 6 milligrams, chased immediately by a saline flush through a proximal line, because the drug is metabolised within seconds. If the first dose fails, I give 0.2 milligram per kilogram, maximum 12 milligrams. I watch on a monitor, because adenosine briefly asystoles and I need a continuous trace. Adenosine blocks the atrioventricular node, so it terminates a re-entry tachycardia and may reveal the atrial origin of a focal tachycardia — it is diagnostic as well as therapeutic. If the rhythm is broad-complex or the child is severely compromised, I move to synchronised cardioversion. [7]
References
- [1]Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL Developmental pharmacology--drug disposition, action, and therapy in infants and children. The New England journal of medicine, 2003.PMID 13679531
- [2]Shaddy RE, Boucek MM, Hsu DT, Boucek RJ Carvedilol for children and adolescents with heart failure: a randomized controlled trial. JAMA, 2007.PMID 17848651
- [3]Hsu DT, Zak V, Mahony L, Sleeper LA Enalapril in infants with single ventricle: results of a multicenter randomized trial. Circulation, 2010.PMID 20625111
- [4]Hsu DT, Pearson GD Heart failure in children: part II: diagnosis, treatment, and future directions. Circulation Heart failure, 2009.PMID 19808380
- [5]Loss KL, Shaddy RE, Kantor PF Recent and Upcoming Drug Therapies for Pediatric Heart Failure. Frontiers in pediatrics, 2021.PMID 34858897
- [6]Hoffman TM, Wernovsky G, Atz AM, Kulik TJ Efficacy and safety of milrinone in preventing low cardiac output syndrome in infants and children after corrective surgery for congenital heart disease. Circulation, 2003.PMID 12600913
- [7]Batra AS, Silka MJ, Borquez A, Cuneo B Pharmacological Management of Cardiac Arrhythmias in the Fetal and Neonatal Periods: A Scientific Statement From the American Heart Association: Endorsed by the Pediatric and Congenital Electrophysiology Society (PACES). Circulation, 2024.PMID 38314551
- [8]Ruopp NF, Cockrill BA Diagnosis and Treatment of Pulmonary Arterial Hypertension: A Review. JAMA, 2022.PMID 35412560
- [9]Berman Rosenzweig E, Barst RJ Pulmonary arterial hypertension : a comprehensive review of pharmacological treatment. Treatments in respiratory medicine, 2006.PMID 16512692
- [10]Taksande A, Jameel PZ Critical Congenital Heart Disease in Neonates: A Review Article. Current pediatric reviews, 2021.PMID 33605861
- [11]Eades SK, Christensen ML The clinical pharmacology of loop diuretics in the pediatric patient. Pediatric nephrology (Berlin, Germany), 1998.PMID 9761364