Paeds · clinical-pharmacology-and-therapeutics
Chemotherapy and supportive pharmacology
Also known as Cytotoxic chemotherapy in children · Antiemetics in paediatric oncology · G-CSF and pegfilgrastim in children · Dexrazoxane cardioprotection · Palifermin for mucositis · Anthracycline extravasation management
A fellowship approach to chemotherapy and supportive pharmacology in children covering the cytotoxic drug classes and their organ-specific toxicities, the antiemetic ladder built on 5-HT3 antagonists (ondansetron), the NK1 antagonist aprepitant and dexamethasone for chemotherapy-induced nausea and vomiting, the colony-stimulating factors filgrastim and pegfilgrastim for febrile neutropenia prophylaxis, palifermin (keratinocyte growth factor) for oral mucositis after stem-cell transplant conditioning, dexrazoxane for anthracycline cardioprotection and extravasation, and the non-negotiable rule that vincristine is given intravenously and never by the intrathecal route.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture an eight-year-old receiving doxorubicin for acute lymphoblastic leukaemia whose echocardiogram is tracked cycle by cycle, a six-year-old on cisplatin who vomits for three days after each infusion, and a ten-year-old the morning after stem-cell transplant conditioning whose mouth is so sore he cannot swallow his own saliva. Each child is living a cytotoxic toxicity, and each one has a supportive medicine built to prevent or treat it. The general paediatrician rarely prescribes the cytotoxic agent, but shares the surveillance, the febrile-neutropenia front door, and the safety culture that keeps the routes right. [1] [11]
Two ideas carry the whole topic. The first is the toxicity-to-antidote pairing: every cytotoxic class has a predictable organ injury, and modern paediatric oncology pairs each one with a supportive drug that blunts the injury without abolishing the anti-cancer effect. The second is the route-safety culture: the cytotoxics are among the most dangerous drugs to administer, and the vincristine-intrathecal catastrophe is the cautionary tale that drives minibag dilution, separate intrathecal preparation times, and double-independent checks. [9] [11]
From the cytotoxic plan to the supported child
1 · Know the drug and its toxicity
Identify the cytotoxic class and the organ it injures — anthracycline to the heart, vinca to nerves, platinum to ears and kidneys, antimetabolite to marrow.
2 · Match the supportive medicine
Pair the toxicity with its antidote — dexrazoxane, antiemetics, colony-stimulating factors, palifermin, hydration and rasburicase as indicated.
3 · Protect the route
Confirm vincristine is intravenous only and never prepared with intrathecal drugs; apply independent checks and minibag dilution.
4 · Plan the surveillance
Track cumulative anthracycline dose with echocardiography and troponin, blood counts for neutropenia, and growth and development throughout.
5 · Hold the front door
Treat the febrile neutropenic child as a medical emergency: cultures and empirical antibiotics within the hour, never as a routine viral illness.
Classification
The cytotoxic drugs sort into families by the cellular machinery they break, and each family carries its own signature toxicity. The alkylating agents — cyclophosphamide, ifosfamide, cisplatin and carboplatin — damage DNA directly and burden the kidneys, the bladder (haemorrhagic cystitis with cyclophosphamide and ifosfamide) and the ears (platinum ototoxicity). The antimetabolites — methotrexate at high dose, cytarabine, mercaptopurine — disrupt nucleic acid synthesis and suppress the bone marrow most of all. [10]
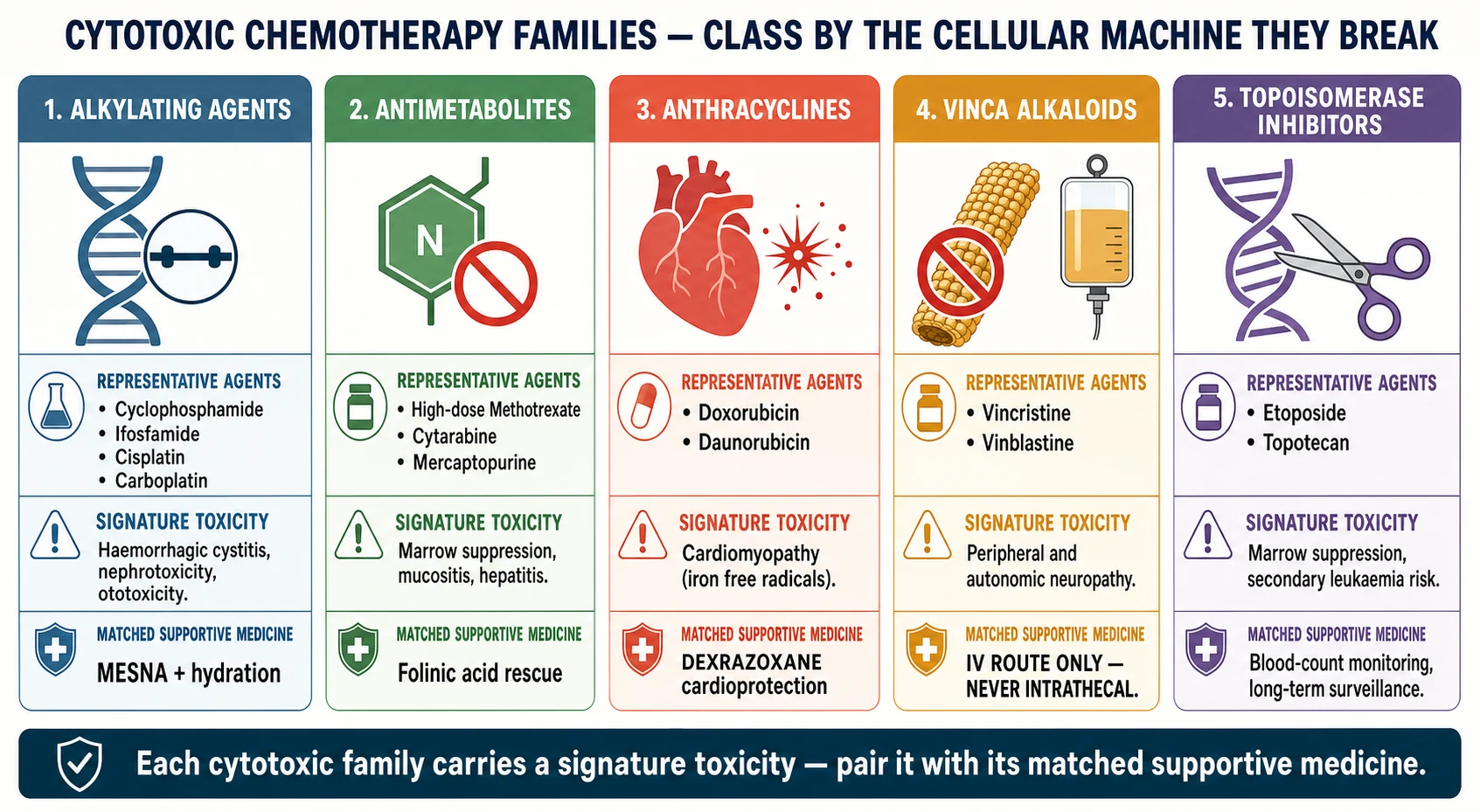
The anthracyclines — doxorubicin and daunorubicin — intercalate DNA and generate free radicals, and their free-radical injury to the myocardium is the cardiotoxicity that dexrazoxane exists to prevent. The vinca alkaloids — vincristine and vinblastine — block microtubule assembly, arresting dividing cells but also the axonal transport that nerves depend on, causing peripheral and autonomic neuropathy. The topoisomerase inhibitors — etoposide and the camptothecins — freeze the DNA-unwinding enzymes and carry a risk of treatment-related leukaemia. Across all of these, the dose-limiting toxicity is often myelosuppression, which is where the colony-stimulating factors enter. [1] [7]
| Drug family | Representative agents | Signature toxicity | Supportive medicine |
|---|---|---|---|
| Alkylating agents | Cyclophosphamide, ifosfamide, cisplatin, carboplatin | Haemorrhagic cystitis, nephrotoxicity, ototoxicity | Mesna, aggressive hydration, magnesium replacement |
| Antimetabolites | High-dose methotrexate, cytarabine, mercaptopurine | Marrow suppression, mucositis, hepatitis | Folinic acid rescue, hydration, alkalinisation |
| Anthracyclines | Doxorubicin, daunorubicin | Cardiomyopathy (free-radical myocardial injury) | Dexrazoxane cardioprotection, cardiac surveillance |
| Vinca alkaloids | Vincristine, vinblastine | Peripheral and autonomic neuropathy, jaw pain | Intravenous route only — never intrathecal; warmth for extravasation |
| Topoisomerase inhibitors | Etoposide, topotecan | Marrow suppression, secondary leukaemia risk | Blood-count monitoring, long-term surveillance |
| Highly emetogenic agents (any class) | Cisplatin, cyclophosphamide, doxorubicin | Chemotherapy-induced nausea and vomiting | Ondansetron plus aprepitant plus dexamethasone |
Epidemiology & Risk Factors
Cancer is the second commonest cause of death in children beyond infancy in high-income settings, and survival now exceeds eighty per cent in many paediatric malignancies — a success bought at the price of cumulative toxicity that the survivor carries for life. The Children's Oncology Group long-term follow-up guidelines exist precisely because the supportive medicines on this page determine not only whether the child survives the treatment, but how their heart, hearing, fertility and second-cancer risk read decades later. [11]
Several factors push a child toward the worst of these toxicities. A high cumulative anthracycline dose — classically above 300 mg per square metre of doxorubicin equivalent — raises the lifetime risk of cardiomyopathy, and dexrazoxane is reserved for the child crossing into that territory. Young age at exposure magnifies the cardiac and ototoxic burden because the organ is still developing. Concurrent chest radiotherapy compounds the anthracycline cardiac injury. And the emetogenic potential of the regimen — cisplatin at the top of the ladder, vincristine near the bottom — decides whether the child needs a single antiemetic or the full ondansetron–aprepitant–dexamethasone combination. [1] [3]
Child on cisplatin
Highly emetogenic
- Top of the emetogenic ladder
- Triple antiemetic: ondansetron, aprepitant, dexamethasone
- Mandatory hydration with mannitol or saline diuresis
- Audiometry and renal monitoring each cycle
Child on doxorubicin
Cardiotoxicity risk
- Cumulative anthracycline dose tracked precisely
- Echocardiography and troponin surveillance
- Dexrazoxane for high cumulative doses
- Avoid concomitant cardiotoxic drugs and chest radiotherapy where possible
Child on vincristine
Route-critical
- Intravenous only, never intrathecal
- Minibag dilution and independent checks
- Jaw pain, constipation, foot drop as neurotoxicity
- Extravasation managed with warmth, not cold
Child after HSCT
Mucositis and neutropenia
- Palifermin before and after conditioning
- Severe oral mucositis for one to two weeks
- Filgrastim to shorten neutropenia
- Febrile neutropenia is an emergency, not a viral illness
Pathophysiology
The cytotoxic drugs kill cancer cells by breaking the machinery of cell division, and the supportive drugs work by intercepting the specific injury that the cytotoxic causes in healthy tissue. Understanding the split tells you why dexrazoxane protects the heart without shielding the leukaemia, and why ondansetron stops the vomit without blunting the chemotherapy. [1] [10]
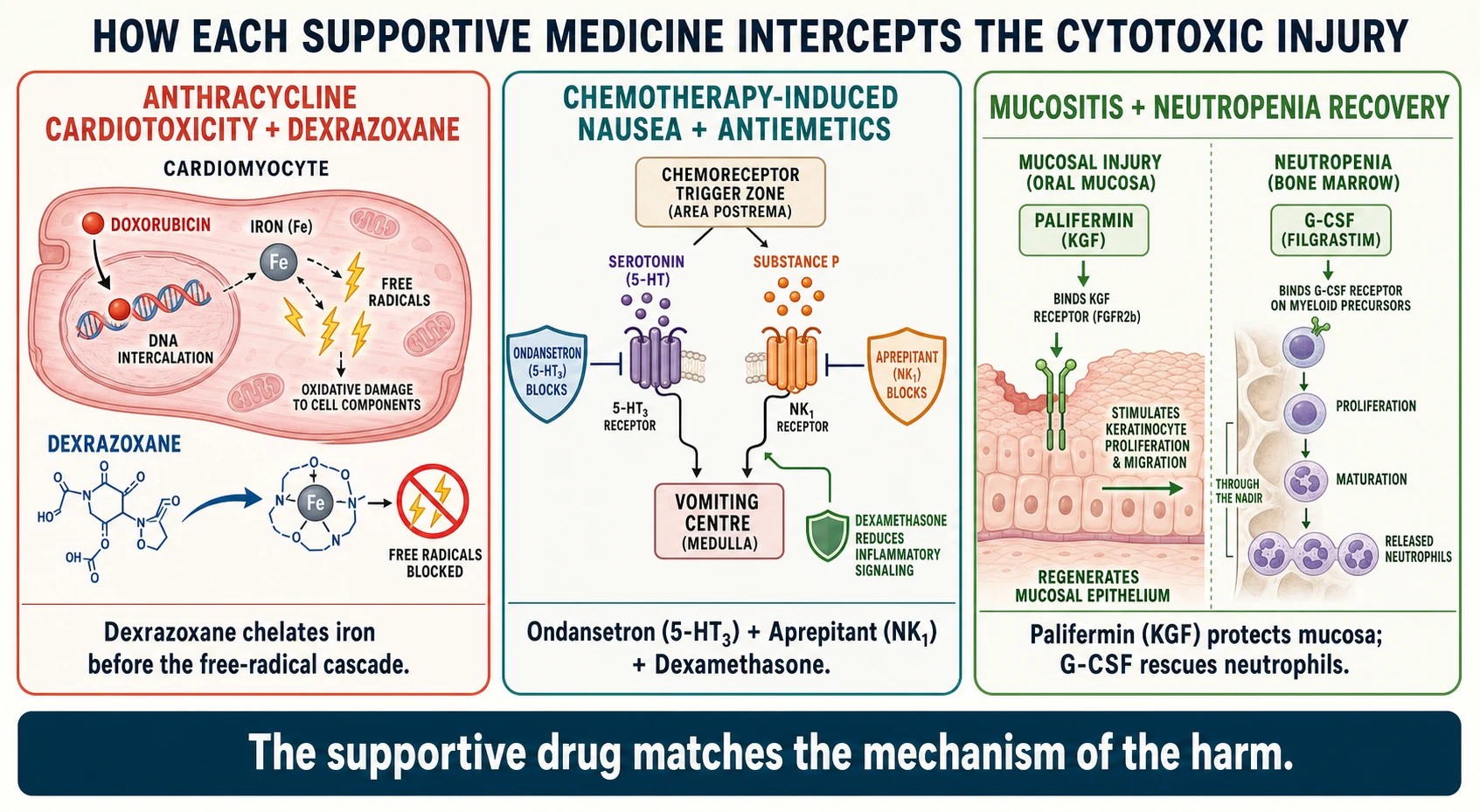
The anthracyclines intercalate DNA and poison topoisomerase, but the cardiotoxicity comes from a second action: the drug binds iron in the cardiomyocyte and the iron catalyses a runaway free-radical cascade that destroys cardiac cells, which regenerate poorly. Dexrazoxane is a cyclic derivative that chelates intracellular iron before the radical cascade begins, which is why it is given ahead of the anthracycline, and why the Lipshultz trial in children with acute lymphoblastic leukaemia showed less myocardial injury with dexrazoxane without compromising leukaemia control. The same chelating action, applied at high dose, neutralises the free anthracycline after an extravasation, which is why dexrazoxane rescues anthracycline spill into tissue. [1] [9]
The vomiting reflex is driven by serotonin released from enterochromaffin cells binding 5-HT3 receptors on the vagus, and by substance P binding NK1 receptors in the brainstem. Ondansetron blocks the 5-HT3 receptor and aprepitant blocks the NK1 receptor, so combining them with dexamethasone covers the acute, the delayed and the inflammatory arms of chemotherapy-induced nausea and vomiting. The colony-stimulating factors are glycoproteins that bind receptors on marrow neutrophil precursors and drive them through the nadir; filgrastim does this daily, and pegfilgrastim does it once per cycle because a polyethylene glycol moiety extends its half-life. Palifermin is recombinant keratinocyte growth factor that binds receptors on oral epithelium and accelerates the mucosal repair that the cytotoxic has stalled. [6] [7]
Clinical Presentation
You meet these drugs across the whole arc of a child's treatment. In the outpatient infusion suite a child receives cisplatin with the antiemetic ladder already running. On the ward a child the week after chemotherapy is neutropenic and the question is whether the fever is the nadir's first warning. In the emergency department the febrile neutropenic child arrives and the clock for empirical antibiotics starts on triage. And in the survivor clinic a teenager years off treatment meets the cardiologist because the cumulative doxorubicin dose crossed the threshold that dexrazoxane was meant to soften. [7] [11]
Toxicity declares itself along recognisable lines. The cardiotoxic child develops a falling ejection fraction or, acutely, a troponin rise during the anthracycline course. The emetogenic child retches through the cisplatin infusion and again in the delayed window of forty-eight to ninety-six hours. The neutropenic child becomes febrile with no obvious source, and the source, when found, is often a mucosal translocation from the mouth or gut that the depleted neutrophil pool could not contain. The mucositis child drools, cannot eat, and loses the oral mucosal barrier at exactly the moment the neutrophil count is at its lowest — a combination that turns minor flora into bacteraemia. [4] [7]
Differential Diagnosis
When a child on chemotherapy becomes unwell, the first question is whether the symptom is the cancer, the cytotoxic, an infection unmasked by myelosuppression, or a supportive drug in its own right. A fever in a neutropenic child is bacterial sepsis from mucosal translocation until proven otherwise, and the differential of a chest-positive source sits alongside line infection, perianal sepsis and typhlitis. [7]
A rising troponin or falling ejection fraction raises anthracycline cardiotoxicity against viral myocarditis and anaemia, and the cumulative-dose record resolves it. New jaw pain, constipation or foot drop in a child on vincristine is vinca neurotoxicity, and abdominal pain on vincristine raises vinca-induced ileus against neutropenic colitis. Severe mouth pain in the second week after transplant is mucositis, but the fever that accompanies it is infection until cultures say otherwise. The safeguard in every case is to draw the cumulative-dose record, check the relevant counts and markers, and treat the febrile neutropenic child empirically before the source is found. [3] [7]
Clinical & Bedside Assessment
Bedside assessment of a child on chemotherapy means weighing the disease control and the drug toxicity at every visit. For the anthracycline child, plot the cumulative dose against the cardiac surveillance schedule and ask about exercise tolerance, palpitations and breathlessness — the early signs of a falling ejection fraction. For the cisplatin child, ask about nausea in the acute and the delayed window, check the hearing, and review the renal function and magnesium each cycle. [3] [11]
Then turn to the supportive drugs. On filgrastim or pegfilgrastim, ask about bone pain — the marrow is expanding and the long bones ache — and confirm the neutrophil count is recovering as expected. On ondansetron, ask whether the vomiting broke through despite the scheduled dose, because an under-controlled emetogenic regimen dehydrates the child and erodes adherence. On vincristine, ask about constipation, jaw pain and tingling, and examine for foot drop and abdominal distension, because vinca neurotoxicity is dose-cumulative and often dose-limiting. [5] [6]
Adherence and supportive-care concordance matter at the bedside. A child who vomits the oral mercaptopurine at home runs a higher relapse risk; a family who waits out a fever because they fear the hospital loses the window for empirical antibiotics. Ask about the home emesis, the thermometer, the central-line care, and the plan the oncology team gave them for a fever. The general paediatrician's job is to know that plan and to enact it without delay. [7] [11]
Investigations
The investigations divide into the cycle surveillance and the emergency panel. Cycle surveillance tracks the cumulative toxicities: echocardiography and troponin for the anthracycline child, audiometry and renal function with magnesium for the cisplatin child, blood counts and liver enzymes for the antimetabolite child, and growth and endocrine panels for the long-term survivor. The cadence is set by the regimen and the cumulative thresholds, and the oncology team holds the schedule. [3] [11]
| Test | When | What it tells you | Action if abnormal |
|---|---|---|---|
| Echocardiography and troponin | Baseline and across the anthracycline course | Anthracycline cardiotoxicity — falling ejection fraction | Cardiology review; consider dexrazoxane; cumulative-dose check; dose or agent review with oncology |
| Audiometry | Baseline and per cisplatin cycle | Platinum ototoxicity — high-frequency hearing loss | Audiology review; dose or agent review; hearing support |
| Blood count, liver enzymes, creatinine | Each cycle and at nadir | Marrow suppression, hepatotoxicity, nephrotoxicity | Dose holds; filgrastim for neutropenia; supportive care |
| Blood culture, full blood count, CRP | At febrile neutropenia presentation | Source and depth of the neutropenic sepsis | Empirical broad-spectrum antibiotics within the hour; admit |
| Cumulative anthracycline dose record | Throughout treatment | Cardiotoxicity threshold crossing | Dexrazoxane and intensified cardiac surveillance above 300 mg/m² |
The emergency panel is the febrile neutropenia workup: blood cultures from every lumen of the central line, a peripheral culture, a full blood count with differential, and a CRP, together with a chest radiograph and a focused examination of the mouth, perianal area and line site. Urine is cultured when the child can provide it, and a chest or abdominal scan follows the clinical lead. The key is that the empirical antibiotics do not wait for the cultures — they go in within the hour, broad-spectrum and antipseudomonal, and narrow once the organism and sensitivity return. [7]
CAN-DO — the supportive pharmacology you match to each cytotoxic harm
Management — Resuscitation
The resuscitation moment in this topic is the febrile neutropenic child. A child with an absolute neutrophil count under 0.5 × 10⁹ per litre and a fever is in medical emergency, and the source is almost always mucosal translocation that the depleted neutrophils could not contain. The immediate actions are to assess for sepsis on the standard paediatric pathway, take cultures from every central-line lumen and a peripheral site, and begin empirical broad-spectrum antipseudomonal antibiotics within the hour — not after the cultures grow, but at the moment the fever and neutropenia are confirmed. [7]
For anthracycline extravasation, the resuscitation is dexrazoxane: it is given intravenously within six hours of the spill, on three consecutive days, with the dose banded to body surface area as set out in the Mouridsen multicentre studies. Cold compresses are not applied — cold worsens vinca injury and is not the standard for anthracycline. For the vincristine extravasation, warmth and hyaluronidase are the supportive measures, and the difference in thermal management between the two drug classes is a favourite examination point. For suspected anaphylaxis to a cytotoxic infusion, stop the infusion, treat the reaction, and reconsider the rate and premedication with the oncology team. [9]
Management — Definitive & Stepwise
Cardioprotection with dexrazoxane is built on the Lipshultz trial in children with acute lymphoblastic leukaemia, which showed that dexrazoxane given before each doxorubicin dose reduced myocardial injury measured by troponin T without compromising leukaemia control. It is dosed at a ratio of about ten parts dexrazoxane to one part doxorubicin, given ahead of the anthracycline, and reserved for the child crossing a high cumulative threshold. The Cochrane review of cardioprotective interventions for anthracyclines confirms the cardioprotective signal across trials, and the long-term biomarker follow-up ties the early troponin changes to later echocardiographic outcomes. [1] [3] [10]
Supportive pharmacology principles (verify against the current oncology formulary)
The antiemetic ladder is set by the emetogenic potential of the regimen. For the highly emetogenic cisplatin-containing courses, the MASCC/ESMO paediatric consensus supports combining a 5-HT3 antagonist (ondansetron), an NK1 antagonist (aprepitant) and dexamethasone to cover the acute and delayed phases. The Kang phase three trial established aprepitant as effective and tolerable in children when added to ondansetron and dexamethasone, and the principle is to match the antiemetic strength to the emetogenic challenge rather than to wait for breakthrough vomiting. [5] [6]
The colony-stimulating factors prevent or shorten the febrile neutropenic nadir. The ASCO guideline recommends primary prophylaxis with a colony-stimulating factor when the regimen carries a febrile neutropenia risk of about twenty per cent or higher, or when the child carries factors that raise that risk. Filgrastim is given daily at about 5 µg per kilogram subcutaneously after the chemotherapy, and pegfilgrastim is given once per cycle at about 100 µg per kilogram subcutaneously, with paediatric sarcoma trials confirming it supports dose-intensive regimens. Mucositis prevention with palifermin, at about 60 µg per kilogram daily for three days before and three days after stem-cell transplant conditioning, reduces the severe oral mucositis that the Spielberger trial defined in the autologous transplant population. [7] [8] [4]
Specific Subtypes & Scenarios
The child on a cisplatin regimen is the archetype of the highly emetogenic course. Cisplatin sits at the top of the emetogenic ladder, so the antiemetic plan is the full ondansetron–aprepitant–dexamethasone combination, and the delayed nausea window of forty-eight to ninety-six hours is the one families are warned about. Cisplatin also demands hydration with saline diuresis and magnesium surveillance, and audiometry each cycle because the high-frequency hearing loss is permanent. [5] [6]
The child on a doxorubicin-containing regimen for leukaemia or sarcoma is the cardiotoxicity archetype. The cumulative anthracycline dose is tracked precisely, the echocardiography and troponin are run across the course, and dexrazoxane is reserved for the child whose cumulative dose crosses into the high-risk threshold. The Lipshultz biomarker data tie the early troponin rise to the later echocardiographic decline, so the surveillance is not just a checkbox — it is the signal that drives the dexrazoxane decision. [1] [3]
The first year of a child on doxorubicin for acute lymphoblastic leukaemia
The child undergoing stem-cell transplant is the mucositis and neutropenia archetype. Palifermin runs for three days before and three days after the conditioning regimen, and filgrastim shortens the post-transplant neutropenia. The severe oral mucositis of the second week is managed with pain control, mouth care and nutritional support, and the fever that accompanies it is treated as febrile neutropenia regardless, because the broken mucosa is the gateway for bacteraemia. The child who extravasates an anthracycline into the tissue is the resuscitation archetype — dexrazoxane within six hours for three days, no cold, and surgical review for the necrosis that a delayed rescue allows. [4] [9]
Complications & Pitfalls
The complications of these drugs are the harms that the supportive medicines and the surveillance exist to prevent. The anthracyclines cause cardiomyopathy; the vinca alkaloids cause neuropathy and, given intrathecally, death; the platinum agents cause ototoxicity and nephrotoxicity; the myelosuppressive regimens cause febrile neutropenia; and the conditioning regimens cause mucositis. Most are avoidable or mitigable when the supportive drug and the surveillance are applied correctly. [1] [10]
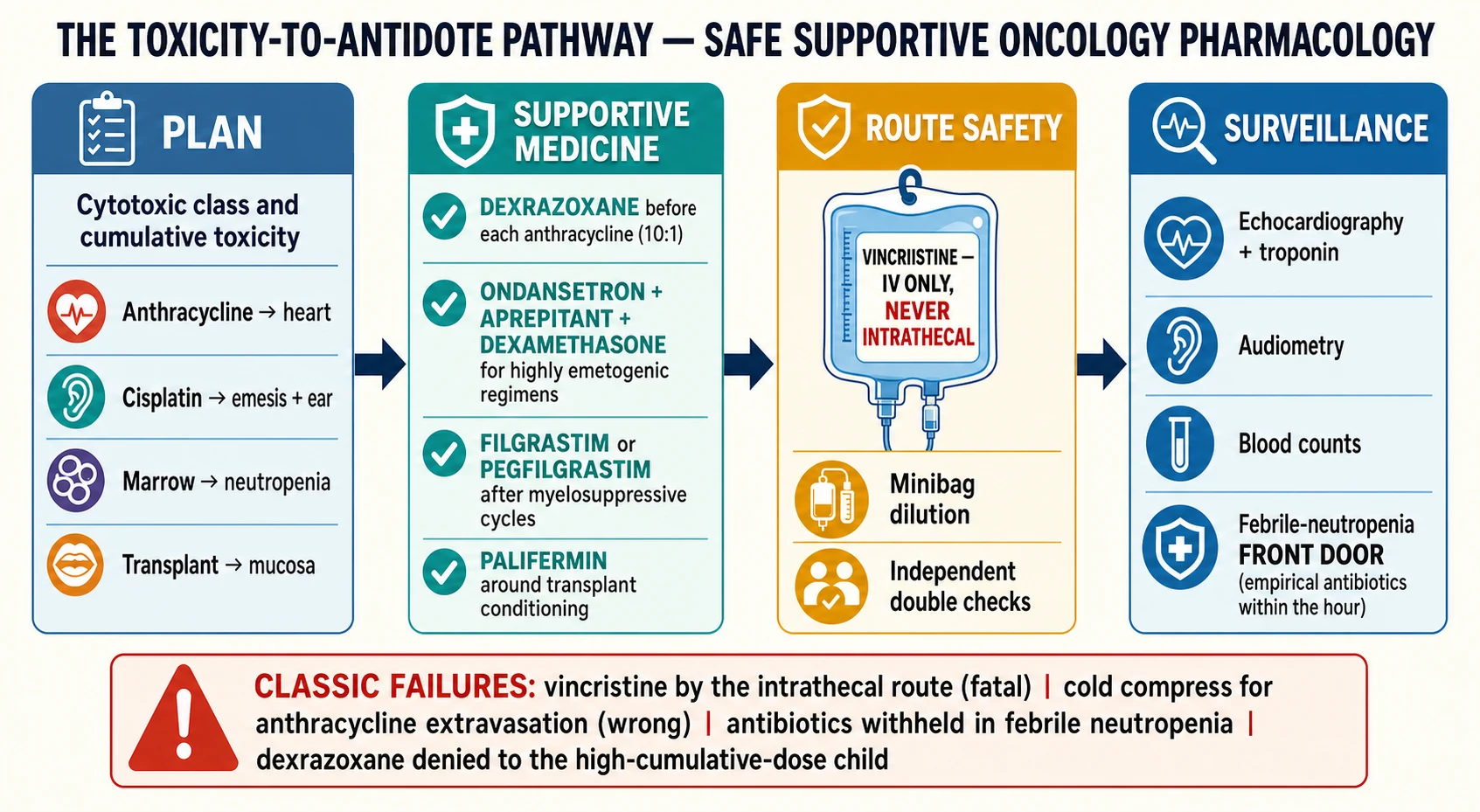
Four pitfalls recur at the bedside. The first is the vincristine-intrathecal error: vincristine drawn into a syringe and delivered with the intrathecal drugs, with catastrophic and fatal consequence. The second is the withheld empirical antibiotic: the febrile neutropenic child assessed as a viral illness and sent home, losing the hour that the sepsis needed. The third is the cold compress for anthracycline extravasation: the wrong thermal management that delays the dexrazoxane rescue. The fourth is the dexrazoxane denied on outdated fear: the child crossing a high cumulative anthracycline threshold denied cardioprotection because of an early concern about secondary malignancy that the Barry study in high-risk acute lymphoblastic leukaemia did not bear out. [2] [9]
Principle
- Each cytotoxic class has a matched supportive drug — pair the harm with its antidote
- Anthracycline → dexrazoxane; emesis → ondansetron + aprepitant + dexamethasone; neutropenia → G-CSF; mucositis → palifermin
- Route safety is absolute: vincristine intravenous only, never intrathecal
Anthracycline cardioprotection
- Doxorubicin, daunorubicin injure myocardium via iron free radicals
- Dexrazoxane chelates iron; about 10 : 1 ratio before each dose
- Surveillance: echocardiography and troponin; cumulative dose tracked
- Dexrazoxane for cumulative dose crossing about 300 mg/m²
Antiemetics
- 5-HT3: ondansetron; NK1: aprepitant; plus dexamethasone
- Triple for highly emetogenic (cisplatin)
- Mind ondansetron QT prolongation at high IV doses
- Cover the delayed 48–96 hour window
Colony-stimulating factors
- Filgrastim about 5 µg/kg/day SC
- Pegfilgrastim about 100 µg/kg SC once per cycle
- ASCO primary prophylaxis at about 20% febrile neutropenia risk
- Bone pain is expected as the marrow expands
Mucositis and extravasation
- Palifermin about 60 µg/kg/day around HSCT conditioning
- Anthracycline extravasation: dexrazoxane within 6 h for 3 days, NO cold
- Vinca extravasation: warmth and hyaluronidase
Pitfalls
- Vincristine by intrathecal route (fatal)
- Withheld antibiotics in febrile neutropenia
- Cold for anthracycline extravasation
- Dexrazoxane denied on outdated secondary-malignancy fear
“Toxicity → antidote → route → surveillance. Dexrazoxane for the anthracycline heart, ondansetron-aprepitant-dexamethasone for the emesis, filgrastim or pegfilgrastim for the neutropenia, palifermin for the mucositis, dexrazoxane within six hours for the extravasation — and vincristine intravenous only, never intrathecal, with the febrile neutropenic child given empirical antibiotics within the hour.”
Prognosis & Disposition
The prognosis for childhood cancer has transformed: survival now exceeds eighty per cent in many malignancies, and the supportive medicines on this page are part of the reason the child survives the treatment as well as the disease. Dexrazoxane protects the heart through the anthracycline course; the antiemetic ladder keeps the child fed and adherent; the colony-stimulating factors shorten the dangerous nadir; palifermin protects the mucosa. Each one moves a child from survival to survival with less long-term harm. [1] [11]
Disposition is shared between the oncology team and the general paediatrician. The oncology team prescribes and adjusts the cytotoxic and the supportive regimen; the general paediatrician and primary care hold the surveillance, the immunisation record, and the febrile-neutropenia front door. The survivor follows the Children's Oncology Group long-term follow-up guidelines, with cardiac, audiological, endocrine and second-malignancy surveillance calibrated to the cumulative exposures. A clear handover that names the cumulative anthracycline dose, the ototoxic exposure, and the febrile-neutropenia plan is the safeguard. [7] [11]
The long-term cardiac risk is the one the survivor carries furthest. The biomarker and echocardiographic follow-up of the anthracycline cohort ties early myocardial injury to late cardiomyopathy, and the dexrazoxane decision made during treatment reads decades later in the adult cardiology clinic. This is why the cumulative-dose record and the surveillance schedule are not paperwork but the foundation of the survivor's future. [3] [10]
Special Populations
The young child on these regimens is the patient where weight and surface-area dosing, taste intolerance and route safety matter most. The cytotoxics are surface-area calculations, and the supportive drugs are weight-banded; the liquid formulations taste bitter, and adherence to oral mercaptopurine and antiemetics falls when the child cannot tolerate them. The vincristine-intrathecal risk is highest in the smallest children where central-line lumens and intrathecal drugs are delivered close together, which is why the independent-check culture is reinforced at every administration. [9] [11]
The adolescent is the patient where adherence, transition and reproductive risk converge. A young person who vomits the oral chemotherapy loses disease control; the transfer to adult survivorship care is a moment to lose the patient; and the gonadotoxic burden of alkylating agents and platinum raises the fertility-counselling question that must be addressed before, not after, the cumulative exposure. The transition should name the cumulative doses, the surveillance schedule, and the reproductive risks in a documented handover. [11]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical guidelines and the Australian Medicines Handbook Children's Dosing Companion are the primary references for cytotoxic and supportive dosing, with the Australian and New Zealand Children's Haematology and Oncology Group coordinating care. For Aboriginal and Torres Strait Islander and Māori children, the febrile-neutropenia front door and the cold-chain for supportive medicines in remote settings matter, and a single coordinator with cultural support closes the gap. The vincristine-intrathecal safety standard is enforced at every administering unit. [7] [11]
Global and low-resource settings: where access to dexrazoxane, pegfilgrastim and palifermin is limited, the principles still hold — protect the vincristine route, give empirical antibiotics within the hour for febrile neutropenia, hydrate the platinum child, and track the cumulative anthracycline dose even when the cardioprotective drug is unavailable. The single largest preventable harm worldwide is the vincristine-intrathecal error, and the minibag-dilution and independent-check standard is achievable in every setting. [9] [11]
Evidence, Guidelines & Regional Differences
The evidence for dexrazoxane cardioprotection rests on the Lipshultz trial in children with acute lymphoblastic leukaemia, which showed reduced myocardial injury without compromising leukaemia control, the long-term biomarker follow-up tying early troponin changes to later echocardiographic outcomes, and the Cochrane review of cardioprotective interventions confirming the signal across trials. The concern that dexrazoxane might raise the risk of secondary malignancy was addressed by the Barry study, which found no excess secondary neoplasms in high-risk acute lymphoblastic leukaemia treated with dexrazoxane — a finding that supports its use in the high-cumulative-dose child. [1] [2] [3] [10]
The antiemetic evidence is anchored by the Kang phase three trial of aprepitant in children, the MASCC/ESMO paediatric consensus on chemotherapy-induced nausea and vomiting prevention, and the broader adult guideline literature carried into paediatric practice. The colony-stimulating factor evidence rests on the ASCO guideline recommending primary prophylaxis at the high-risk threshold, and the Spunt phase two trial of pegfilgrastim-supported dose-intensive chemotherapy in paediatric sarcoma. The mucositis evidence is the Spielberger trial of palifermin in autologous stem-cell transplant, and the extravasation evidence is the Mouridsen multicentre studies of dexrazoxane (Savene) for anthracycline spill. The long-term survivorship framework is the Children's Oncology Group long-term follow-up guidelines. [4] [5] [6] [7] [8] [9] [11]
The evidence is weaker where it rests on guideline consensus rather than paediatric trial — the exact paediatric ondansetron and aprepitant weight bands, the precise dexrazoxane threshold, and the pegfilgrastim role in regimens other than sarcoma are practice-derived in part. Where the evidence is weaker, state the principle, cite the guideline or trial, and verify the dose against the current local oncology formulary rather than implying a precision the data do not support. [6] [7]
Board and assessment distinctions
RACP current PREP curriculum candidates must apply safe prescribing of cytotoxic and supportive medicines within the medication-safety and acute-illness learning objectives, and first-year trainees from 2027 encounter it under quality-and-safety goals. RCPCH Progress+ embeds safe prescribing and the vincristine-intrathecal safety standard as core patient-safety outcomes. The ABP General Pediatrics Content Outline applies pharmacology-domain knowledge to supportive oncology care.
[3]| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Identify the matched supportive drug for a given cytotoxic toxicity, or the vincristine route rule, in a clinical vignette |
| RACP DCE long case | Build a toxicity-to-antidote plan for a child on an anthracycline and cisplatin regimen, with cumulative-dose surveillance |
| MRCPCH clinical | Counsel a family on chemotherapy-induced nausea and vomiting prevention and the febrile-neutropenia front-door plan |
| ABP | Apply pharmacology-domain knowledge to select and justify a colony-stimulating factor, antiemetic or cardioprotectant |
| RCPSC structured oral | Defend the dexrazoxane decision for the high-cumulative-dose child and the extravasation rescue |
Exam Pearls
Viva: why is dexrazoxane given before each doxorubicin dose in the high-cumulative-dose child?
Doxorubicin injures the cardiomyocyte through an iron-catalysed free-radical cascade that the slowly regenerating cardiac cell cannot repair, and the injury accumulates as the cumulative dose rises. Dexrazoxane is an intracellular iron chelator: given before the anthracycline it binds the iron before the radical cascade begins, protecting the heart without shielding the leukaemia, as the Lipshultz trial showed with reduced troponin injury and preserved leukaemia control. It is reserved for the child crossing a high cumulative threshold — classically above about 300 milligrams per square metre of doxorubicin equivalent — and the surveillance that drives the decision is the echocardiography and troponin that the biomarker follow-up ties to later cardiac outcomes. The earlier fear of secondary malignancy was not borne out in the high-risk acute lymphoblastic leukaemia cohort studied by Barry. [1] [2] [3]
Structured oral: vincristine is to be given — what is the non-negotiable route rule, and how is the catastrophe prevented?
Vincristine is given by the intravenous route only, and into the cerebrospinal fluid it is uniformly fatal — the microtubule blockade ascends the neuraxis and the child dies of ascending paralysis and brainstem failure within days. The catastrophe is prevented by a system, not a memory: vincristine is diluted in a minibag rather than a syringe, so it cannot be physically confused with the small-volume intrathecal drugs; intrathecal drugs are prepared and delivered at a separate time, often the only procedure in the room; and two clinicians check the drug, the route and the patient independently. The general paediatrician states the rule plainly — vincristine is intravenous, never intrathecal — and refuses to sign a check that is not independent. [9] [11]
References
- [1]Lipshultz SE; Rifai N; Dalton VM; Levy DE; Silverman LB; Lipsitz SR The effect of dexrazoxane on myocardial injury in doxorubicin-treated children with acute lymphoblastic leukemia The New England journal of medicine, 2004.PMID 15247354
- [2]Barry EV; Vrooman LM; Dahlberg SE; Neuberg DS; Asselin BL; Athale UH Absence of secondary malignant neoplasms in children with high-risk acute lymphoblastic leukemia treated with dexrazoxane Journal of clinical oncology, 2008.PMID 18309945
- [3]Lipshultz SE; Miller TL; Scully RE; Lipsitz SR; Rifai N; Silverman LB Changes in cardiac biomarkers during doxorubicin treatment of pediatric patients with high-risk acute lymphoblastic leukemia: associations with long-term echocardiographic outcomes Journal of clinical oncology, 2012.PMID 22370326
- [4]Spielberger R; Stiff P; Bensinger W; Gentile T; Weisdorf D; Kewalramani T Palifermin for oral mucositis after intensive therapy for hematologic cancers The New England journal of medicine, 2004.PMID 15602019
- [5]Kang HJ; Loftus S; Taylor A; DiCristina C; Green S; Zwaan CM Aprepitant for the prevention of chemotherapy-induced nausea and vomiting in children: a randomised, double-blind, phase 3 trial The Lancet. Oncology, 2015.PMID 25770814
- [6]Dupuis LL; Sung L; Molassiotis A; Orsey AD; Tissing W; van de Wetering M 2016 updated MASCC/ESMO consensus recommendations: Prevention of acute chemotherapy-induced nausea and vomiting in children Supportive care in cancer, 2017.PMID 27565788
- [7]Smith TJ; Khatcheressian J; Lyman GH; Ozer H; Armitage JO; Balducci L 2006 update of recommendations for the use of white blood cell growth factors: an evidence-based clinical practice guideline Journal of clinical oncology, 2006.PMID 16682719
- [8]Spunt SL; Irving H; Frost J; Sender L; Guo M; Yang BB Phase II, randomized, open-label study of pegfilgrastim-supported VDC/IE chemotherapy in pediatric sarcoma patients Journal of clinical oncology, 2010.PMID 20142595
- [9]Mouridsen HT; Langer SW; Buter J; Eidtmann H; Rosti G; de Wit M Treatment of anthracycline extravasation with Savene (dexrazoxane): results from two prospective clinical multicentre studies Annals of oncology, 2007.PMID 17185744
- [10]van Dalen EC; Caron HN; Dickinson HO; Kremer LC Cardioprotective interventions for cancer patients receiving anthracyclines Cochrane database of systematic reviews, 2011.PMID 21678342
- [11]DeVine A; Landier W; Hudson MM; Constine LS; Bhatia S; Armenian SH The Children's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers: A Review JAMA oncology, 2025.PMID 39976936