Paeds · clinical-pharmacology-and-therapeutics
Corticosteroid therapy and adverse effects
Also known as Glucocorticoid therapy in children · Prednisolone dosing and weaning · Adrenal suppression from steroids · Stress-dose hydrocortisone · Corticosteroid adverse effects
A fellowship approach to corticosteroid therapy in children covering glucocorticoid versus mineralocorticoid potency and the equivalent-dose ladder (hydrocortisone, prednisolone, methylprednisolone, dexamethasone), weight-based prednisolone and dexamethasone dosing for asthma and croup, the hypothalamic-pituitary-adrenal axis and how exogenous steroids suppress it, the recognition and emergency management of adrenal crisis with age-banded stress-dose hydrocortisone, the safe weaning of longer courses, and the full spectrum of adverse effects from growth suppression to osteopenia.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a five-year-old gasping with an asthma exacerbation who improves within hours of a single dose of oral prednisolone, a toddler with croup whose stridor melts after dexamethasone, and a teenager on long-term prednisolone for nephrotic syndrome who arrives in the emergency department collapsed and hypoglycaemic with a fever. These three children sit on the two edges of the same medicine: its capacity to switch off inflammation, and its capacity to switch off the adrenal cortex. Corticosteroid therapy is the prescribing discipline that uses the first while defending against the second. [11] [7]
A corticosteroid earns its place when inflammation, immune activation, or hormone deficiency is the disease. Three properties decide which agent you reach for. Glucocorticoid potency measures anti-inflammatory strength relative to hydrocortisone. Mineralocorticoid activity measures the tendency to retain sodium and water and waste potassium. Duration of action measures how long the drug suppresses the hypothalamic-pituitary-adrenal (HPA) axis after a single dose — short-acting agents allow the axis to recover between doses, long-acting agents suppress it continuously. Hydrocortisone is the physiological replacement; prednisolone is the workhorse anti-inflammatory; dexamethasone is the high-potency, minimal-mineralocorticoid option. Choosing well means matching the property to the job. [7] [8]
Classification
The corticosteroids a general paediatrician uses fall into a potency ladder ordered around glucocorticoid strength, and the ladder is also an equivalent-dose table. Hydrocortisone sits at the bottom: potency 1, with moderate mineralocorticoid activity, which is why it replaces both the glucocorticoid and the mineralocorticoid lost in adrenal insufficiency. Prednisolone is four times more potent as a glucocorticoid, with slight mineralocorticoid effect, and is the standard oral anti-inflammatory for asthma, nephrotic syndrome, and rheumatological disease. Methylprednisolone is about five times hydrocortisone, with minimal salt retention, and is given intravenously for acute severe disease. Dexamethasone sits at the top, twenty-five to thirty times the glucocorticoid potency of hydrocortisone, with negligible mineralocorticoid activity and a long duration of action that suppresses the axis around the clock. [7] [8]
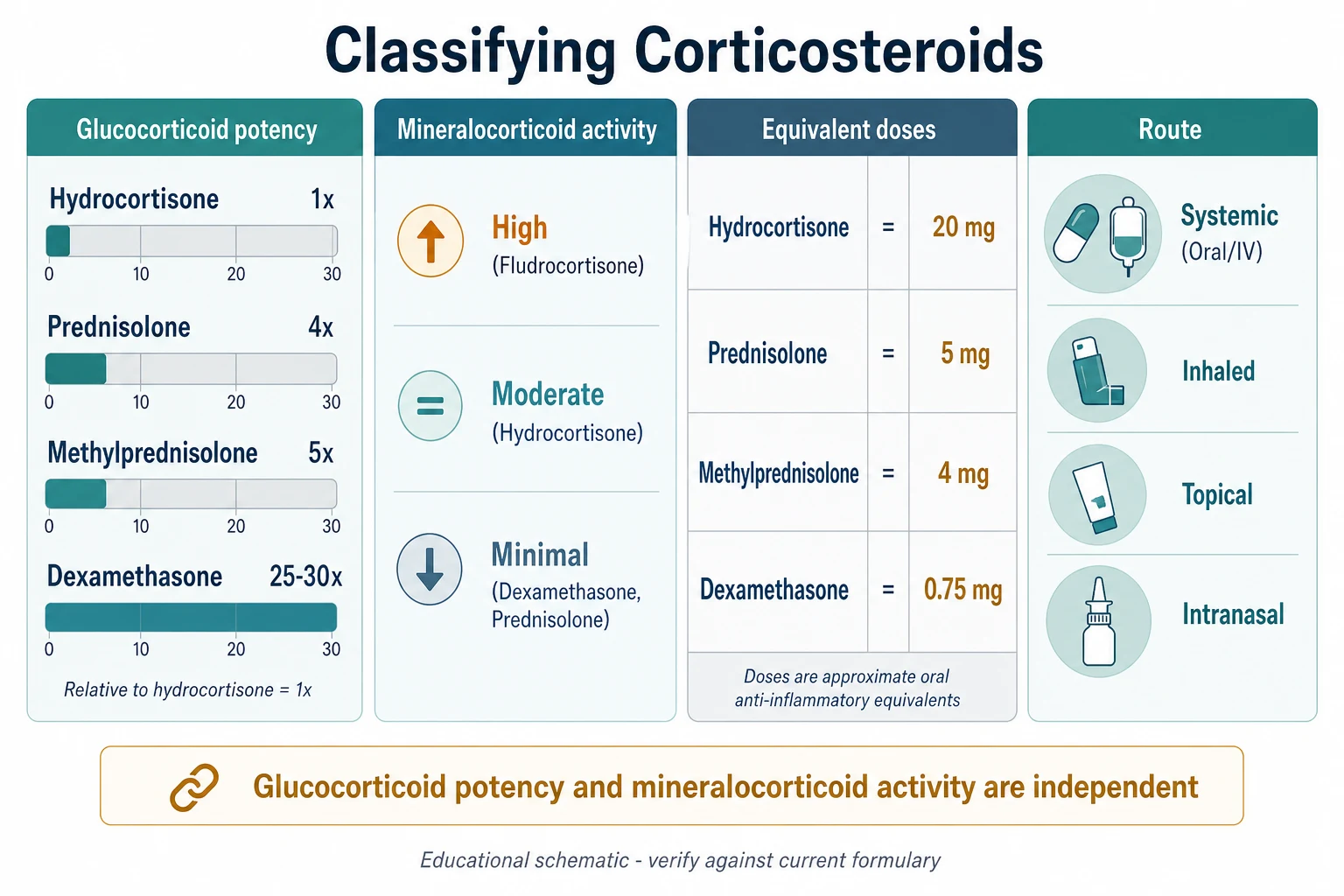
| Agent | Glucocorticoid potency | Mineralocorticoid activity | Typical paediatric use |
|---|---|---|---|
| Hydrocortisone | 1x (reference) | Moderate | Physiological replacement; adrenal crisis; perioperative stress cover |
| Prednisolone | 4x | Slight | Asthma exacerbation; nephrotic syndrome; inflammatory disease (oral workhorse) |
| Methylprednisolone | 5x | Minimal | Acute severe asthma; acute demyelination; transplant rejection (intravenous) |
| Dexamethasone | 25-30x | Negligible | Croup; cerebral oedema; airway oedema; congenital adrenal hyperplasia |
| Fluticasone, budesonide, beclometasone (inhaled) | High, topical | Systemic trace | Asthma and allergic rhinitis prophylaxis — adrenal suppression at very high doses |
Epidemiology & Risk Factors
Corticosteroids are everyday paediatric prescribing. On a single acute-taking ward round you will see prednisolone for an asthma exacerbation, dexamethasone for croup, and hydrocortisone for a child with known adrenal insufficiency; in the outpatient clinic you will see long-term prednisolone for nephrotic syndrome, juvenile idiopathic arthritis, inflammatory bowel disease, and the immunosuppression that follows transplant. The medicines are common; the discipline of choosing the agent, the dose, and the weaning plan is what separates safe from unsafe practice. [11]
Several factors raise the chance that a corticosteroid course harms the child. Duration is the most powerful: courses longer than two to three weeks of pharmacologic dosing reliably suppress the HPA axis, while short three-to-five day bursts for asthma or croup generally do not. Cumulative exposure matters in chronic disease, where years of daily prednisolone stack growth suppression, osteopenia, and cataracts on top of adrenal suppression. Route changes the profile — very-high-dose inhaled corticosteroids, particularly fluticasone in young children, can cause clinically significant adrenal suppression even though they were designed to act topically. Age matters: the neonate is both more sensitive and more likely to receive steroids for chronic lung disease, and the growing child shows growth suppression earliest. And interactions raise risk — enzyme inducers such as rifampicin and phenytoin lower steroid levels and can unmask adrenal insufficiency in a child on replacement. [5] [11]
Short-course child
Asthma, croup
- Prednisolone 1-2 mg/kg for 3-5 days, or single-dose dexamethasone
- HPA suppression generally clinically insignificant
- Can stop abruptly after a short burst
- No routine weaning needed
Long-term child
Nephrotic, IBD, JIA
- Daily or alternate-day prednisolone for weeks to months
- HPA suppression, growth and bone effects accumulate
- Must wean slowly with a written plan
- Sick-day rules and MedicAlert essential
Inhaled high-dose child
Severe asthma
- Very-high-dose fluticasone a particular risk
- Adrenal suppression can be clinically silent
- Check growth and consider cortisol testing
- Step down to lowest effective dose
Neonate
Chronic lung disease
- Dexamethasone for evolving BPD, timed and short
- Hydrocortisone for hydrocortisone-responsive hypotension
- Neurodevelopmental risk informs timing
- Specialist neonatal protocol only
Pathophysiology
The reason corticosteroids work, and the reason they harm, lies in the hypothalamic-pituitary-adrenal axis — a negative-feedback loop that normally keeps cortisol flowing at the rate the body needs. Corticotropin-releasing hormone from the hypothalamus drives adrenocorticotropic hormone (ACTH) from the pituitary, and ACTH drives cortisol from the adrenal cortex. Cortisol then feeds back to quiet the hypothalamus and pituitary. The loop is dynamic: it raises cortisol several-fold in response to surgery, sepsis, hypoglycaemia, and fear. [7]
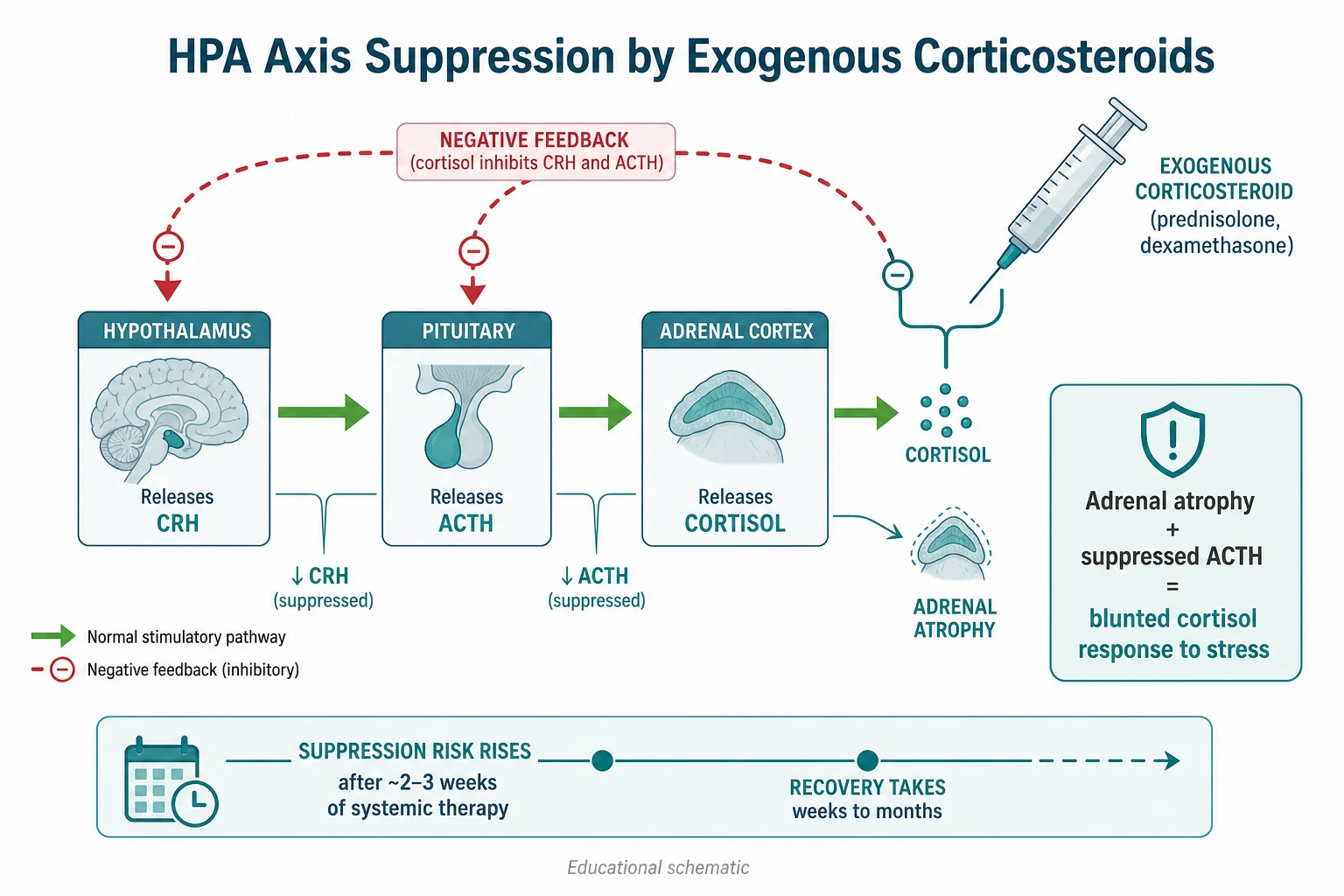
Give an exogenous corticosteroid and you place a fake cortisol signal into that loop. The hypothalamus and pituitary read the signal as plenty, and they switch off their own CRH and ACTH. With the trophic drive withdrawn, the adrenal cortex shrinks. The suppression begins within days of a pharmacologic dose, but it becomes clinically important after about two to three weeks of continuous therapy — especially with long-acting agents like dexamethasone, which occupy the receptor around the clock and give the axis no window to recover. The atrophied cortex can take weeks to months to recover full responsiveness, and during that window the child cannot mount the cortisol surge that stress demands. [7] [9]
The adverse effects flow from the same receptor. Glucocorticoid receptors sit in nearly every tissue, so a systemic corticosteroid reads as a global signal to catabolise protein, lay down visceral fat, raise glucose, weaken bone, and suppress immunity. Growth slows because corticosteroid suppresses the pulsatile release of growth hormone and the action of insulin-like growth factor at the growth plate. Bone thins because formation falls and resorption rises. The child becomes Cushingoid — moon face, buffalo hump, striae — because the drug redistributes fat. Recognising these as the expected, dose-dependent pharmacology — not mysterious side effects — is the first step in preventing them. [8] [11]
Clinical Presentation
The clinical presentation of a corticosteroid problem arrives in two shapes: the disease you are treating, and the harm the drug is doing. The child who wheezes less and breathes easier after prednisolone is showing you the therapeutic face. The child who, after weeks of daily prednisolone, stops growing, bruises easily, complains of back pain, or becomes emotionally labile is showing you the adverse-effect face. The child who was steroid-dependent and now presents with vomiting, abdominal pain, hypotension, and a low glucose under the stress of a fever is showing you the most dangerous face of all — adrenal crisis. [11] [12]
Adrenal crisis declares itself along a steepening curve. The earliest signs are non-specific — lethargy, anorexia, nausea, abdominal pain, and muscle aching — and they are easy to attribute to the intercurrent illness that precipitated the crisis. As cortisol falls further, vomiting becomes intractable, the child becomes hypotensive and tachycardic, and hypoglycaemia appears, particularly in infants and young children whose glycogen reserves are small. Hyponatraemia with hyperkalaemia is the classic biochemical signature of primary adrenal failure, but in corticosteroid-suppressed secondary adrenal insufficiency the mineralocorticoid axis is often preserved (the renin-angiotensin-aldosterone system does not depend on ACTH), so potassium may be normal. The child can decompensate within hours. [7] [12]
Differential Diagnosis
When a steroid-dependent child presents unwell, your first job is to decide whether the child is in adrenal crisis, has an intercurrent illness, or both — because the wrong assumption in either direction is dangerous. The under-diagnosis error is to call the collapse "just a virus" and miss the cortisol deficit. The over-diagnosis error is to attribute everything to adrenal failure and miss sepsis, because the steroid-dependent child is also immunosuppressed and vulnerable to overwhelming infection. The correct reflex is to treat for both at once. [7] [11]
The differential of collapse in a steroid-dependent child runs through septic shock, hypovolaemic shock from gastroenteritis, hypoglycaemia from poor intake, and adrenal crisis. Several features steer toward the adrenal. The timing relative to stress matters: collapse during a febrile illness, after surgery, or after a missed or reduced steroid dose raises adrenal crisis. The biochemistry helps: hyponatraemia, hypoglycaemia, and a relatively normal or only mildly raised potassium, with metabolic acidosis, fit cortisol deficiency. The response to treatment is diagnostic in practice: a child who brightens and whose blood pressure climbs within hours of hydrocortisone was cortisol-deficient. When sepsis is also possible — and in a steroid-dependent child it usually must be assumed — send cultures and start broad-spectrum antibiotics alongside the steroid, without waiting for confirmation. [9] [12]
The differential of the chronic adverse effects is wider but less urgent. Growth failure in a child on long-term steroids may be the drug, the underlying disease, or both; back pain may be steroid osteopenia with vertebral compression, or unrelated. In each case the drug is the first suspect until the evaluation shows otherwise, and the management is to reduce the steroid exposure to the lowest effective regimen — alternate-day dosing, steroid-sparing agents, or step-down of an inhaled dose. [5] [8]
Clinical & Bedside Assessment
Bedside assessment of a corticosteroid patient means asking three questions in order. What is the drug, the dose, and the duration? A child on prednisolone 2 mg/kg daily for four months is a different proposition from one on a three-day asthma burst. Has the axis been suppressed? Courses longer than two to three weeks, very-high-dose inhaled steroids, and any child on long-term replacement are at risk. Is the child under stress right now? Fever, surgery, trauma, vomiting, and poor intake all raise the cortisol demand. A child who fits all three needs stress dosing before you do anything else. [10] [11]
In the well child on chronic steroids, assess for the cumulative adverse effects at every visit. Measure height and plot it — growth suppression is often the earliest and most reversible sign, and a child whose height velocity is falling needs the dose revisited, not reassurance. Ask about mood, sleep, and behavioural change, which parents notice before clinicians do. Examine the back for tenderness, the skin for easy bruising and striae, and the blood pressure, because steroid-induced hypertension is common and often silent. Review bone health with a low threshold for a vitamin D level and, in heavily exposed children, a bone density assessment. [5] [8]
In the acutely unwell steroid-dependent child, the assessment is resuscitation, not diagnosis. Take the history while you treat: confirm the steroid history and any missed or reduced doses, the precipitating illness, and the time of collapse. Examine for hypotension, capillary refill, level of consciousness, and signs of the precipitant. Take blood for glucose at the bedside — a low glucose confirms a dangerous state and demands immediate treatment — and for sodium, potassium, urea, creatinine, and a cortisol level before you give the first hydrocortisone dose if it can be done without delay. Do not let blood tests delay the steroid. [7] [12]
Investigations
The investigation of corticosteroid therapy has two purposes: to confirm adrenal suppression in the at-risk child, and to chase the precipitant and the complications in the acute child. The morning serum cortisol is the screening test for the ambulatory child at risk of suppression. A reliably collected early-morning cortisol above the laboratory cut-off for adequate response (commonly around 400 to 500 nmol/L) makes clinically significant adrenal insufficiency unlikely; a low value (below roughly 100 to 150 nmol/L) is concerning and warrants specialist endocrine evaluation and a dynamic test. The cut-offs are assay- and age-dependent, so always interpret against your local laboratory reference and involve endocrinology for borderline values. [7] [11]
| Test | What it measures | Interpretation |
|---|---|---|
| Early-morning cortisol | Basal HPA output (screening) | Normal cut-off lab-dependent (approx 400-500 nmol/L excludes in most units); low value needs dynamic testing |
| Short Synacthen test (250 mcg) | Adrenal cortisol reserve | Peak cortisol above the local cut-off (approx 500 nmol/L) indicates an adequate reserve; gold standard for diagnosing adrenal insufficiency |
| Low-dose (1 mcg) Synacthen test | Mild or recent suppression | More sensitive for partial secondary adrenal insufficiency; specialist setting |
| ACTH (plasma) | Distinguishes primary from secondary | High ACTH with low cortisol indicates primary; low/normal ACTH with low cortisol indicates secondary (steroid-suppressed) |
The short Synacthen test is the standard dynamic confirmation: 250 micrograms of synthetic ACTH is given, and cortisol is measured at baseline and at 30 and 60 minutes. A peak cortisol above the local response cut-off indicates an adequate adrenal reserve; a blunted response confirms adrenal insufficiency. In the acute collapse, you do not wait for any of these — you draw a single cortisol and ACTH sample for later interpretation, give empirical hydrocortisone, and resuscitate. For the child on long-term inhaled steroids with declining growth or suggestive symptoms, a morning cortisol is a reasonable first screen, with referral for a Synacthen test if it is low or the clinical suspicion is high. [5] [6]
STRESS — the six questions for a steroid-dependent child
Management — Resuscitation
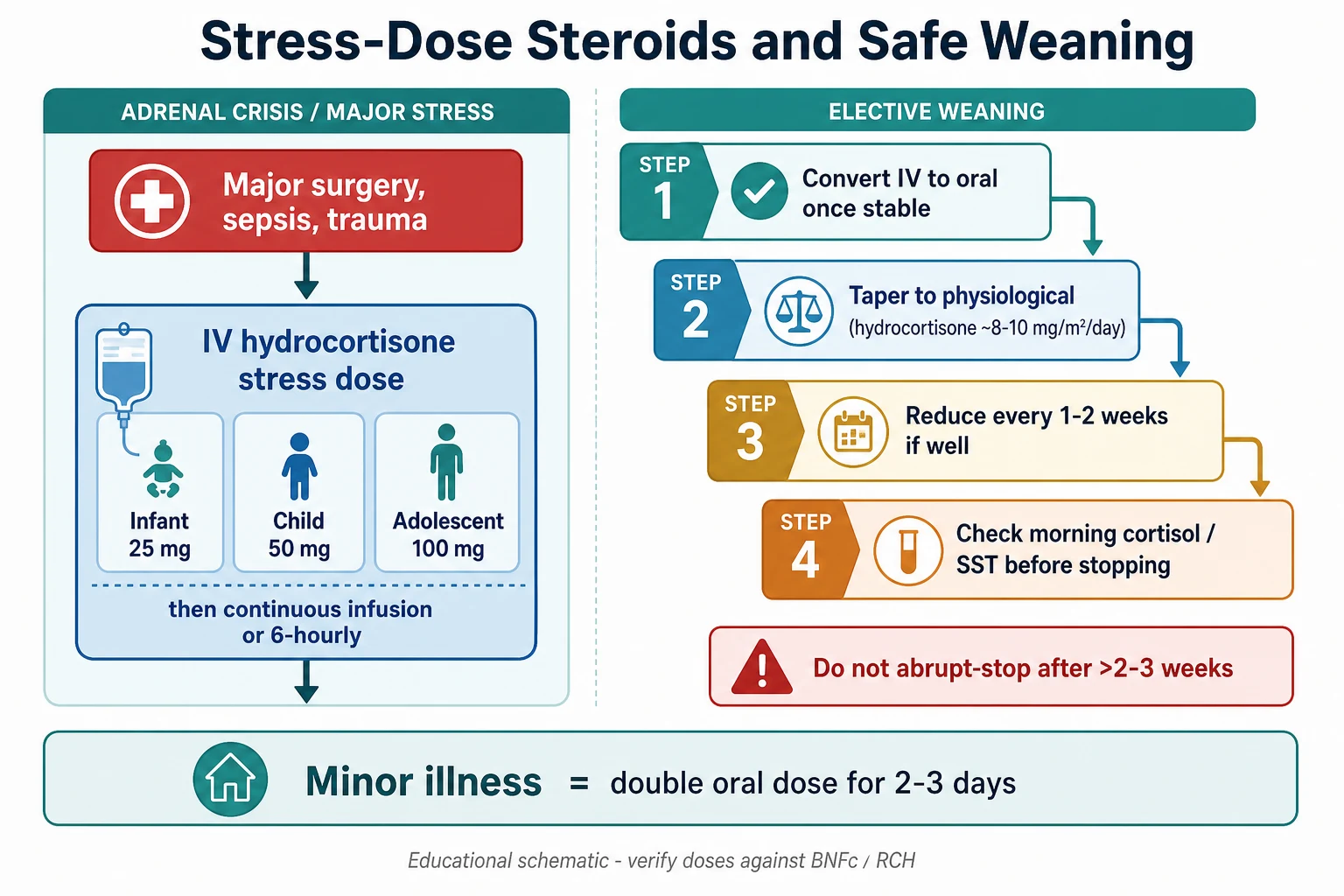
The resuscitation moment in corticosteroid therapy is adrenal crisis, and the first action is to replace the cortisol the child cannot make. Give intravenous or intramuscular hydrocortisone immediately at the age-banded stress dose — 25 mg in an infant, 50 mg in a young child (commonly 1 to 5 years), and 100 mg in an older child or adolescent — followed by a continuous infusion (commonly hydrocortisone around 2 to 3 mg/kg per 24 hours in PICU) or repeated intravenous doses every six hours. Hydrocortisone, not dexamethasone, is the crisis drug, because at stress doses it carries the mineralocorticoid activity the child also needs. [8] [9]
Resuscitation runs in parallel with the steroid. Give intravenous fluid — a 10 to 20 mL/kg bolus of isotonic saline, repeated as needed for shock — because the cortisol-deficient child is hypovolaemic from salt-wasting and vomiting. Correct hypoglycaemia with intravenous dextrose, and monitor glucose closely because it can rebound. Give broad-spectrum antibiotics after cultures, because sepsis is both a precipitant and a differential, and the steroid-dependent child is immunosuppressed. Identify and treat the precipitant — an infection, a missed dose, surgery, or trauma. Reassess blood pressure, capillary refill, and glucose within the first hour; the child who does not improve needs escalation to PICU. [8] [12]
Management — Definitive & Stepwise
The definitive management has three arms — the acute course, the chronic course, and the weaning bridge between them. For the acute therapeutic course you give a weight-based dose for a defined, short time and stop. For an asthma exacerbation that is oral prednisolone 1 to 2 mg/kg once daily (maximum commonly 40 to 60 mg) for three to five days, supported by trials that show equivalence or non-inferiority between prednisolone and a short dexamethasone course; single-dose or two-dose oral dexamethasone at 0.6 mg/kg is an evidence-supported alternative when adherence to a multi-day course is uncertain. For croup it is a single oral dose of dexamethasone 0.15 mg/kg, with nebulised budesonide an alternative. These short courses generally do not need weaning. [1] [2] [3]
Prednisolone (oral)
Dose
1-2 mg/kg once daily
For the chronic course the aim is the lowest dose that controls the disease, given on alternate days where possible to spare the axis and growth, with steroid-sparing agents introduced early. The long-term child needs a written plan for intercurrent illness — the sick-day rules: double the oral dose for two to three days during a febrile illness, and never miss a dose because of vomiting, switching to parenteral hydrocortisone if the child cannot absorb orally. The child should carry a steroid card and wear a MedicAlert identifier, and the family must know the crisis warning signs. [9] [11]
The weaning bridge is where most prescribing errors happen. After any course longer than two to three weeks of pharmacologic dosing, do not stop abruptly — taper to a physiological dose and then step down. A practical approach is to reduce the prednisolone to a physiological equivalent (around hydrocortisone 8 to 10 mg per square metre per day), reduce every one to two weeks while the child remains well, and test the axis with a morning cortisol or a Synacthen test before declaring recovery and stopping. Recovery of full adrenal responsiveness can take months, so the family must keep the sick-day rules and emergency hydrocortisone through that window. [7] [10]
The safe-weaning staircase after a long corticosteroid course
1 · Convert to oral
Once the child is stable, switch intravenous therapy to an equivalent oral dose.
2 · Taper to physiological
Reduce to a physiological equivalent (about hydrocortisone 8-10 mg/m2 per day) over days to weeks.
3 · Step down weekly
Reduce every 1-2 weeks if the child stays well, watching for fatigue, hypotension, and hypoglycaemia.
4 · Test the axis
Check a morning cortisol or perform a Synacthen test before declaring recovery.
5 · Keep sick-day cover
Maintain emergency hydrocortisone and sick-day rules for weeks to months, because full recovery is slow.
Specific Subtypes & Scenarios
Three paediatric scenarios recur in examinations and at the bedside, and each turns the general principles into a specific prescription. Acute asthma is the commonest reason a child receives a corticosteroid: oral prednisolone 1 to 2 mg/kg once daily for three to five days is standard, with the Paniagua trial showing that a short dexamethasone course (0.6 mg/kg per day for two days) is non-inferior and better tolerated when adherence to a multi-day course is doubtful. The choice often comes down to whether the family will reliably give a five-day course. [1] [2]
Croup turns the dose down to dexamethasone 0.15 mg/kg as a single oral dose, with the comparison trials showing oral, intramuscular, and nebulised routes are effective and that nebulised budesonide is an alternative. The single-dose convenience and the clear benefit even in mild croup have made oral dexamethasone the default in most paediatric emergency settings. [3]
The preterm neonate is the scenario where the risk-benefit balance is finest. Systemic dexamethasone for evolving bronchopulmonary dysplasia improves lung function and allows earlier extubation, but high cumulative doses carry neurodevelopmental harm, so modern protocols use hydrocortisone, lower dexamethasone doses, and treat only the baby who cannot wean from the ventilator. The Watterberg trial showed that prophylactic hydrocortisone in extremely preterm infants improved survival without bronchopulmonary dysplasia in the subgroup that needed it, refining the neonatal use toward hydrocortisone. This prescribing belongs to the neonatal specialist, not the generalist — but the generalist must know the principle that neonatal corticosteroid use is a measured, protocolised decision. [4]
Complications & Pitfalls
The complications of corticosteroid therapy are the expected pharmacology of a catabolic, immunosuppressive hormone given in pharmacologic doses, and the pitfalls in prescribing are the predictable ways clinicians get them wrong. The complications fall into systems. Growth suppression is often the earliest and most reversible, and it can occur with both systemic and very-high-dose inhaled steroids. Bone effects — osteopenia and vertebral compression fractures — appear with higher cumulative exposure. Metabolic effects include hyperglycaemia, hypertension, and the Cushingoid redistribution of fat. Gastrointestinal effects include gastritis and, rarely, perforation. Immune effects raise susceptibility to infection, including severe varicella in a non-immune child. Behavioural effects range from irritability to steroid psychosis. Ocular effects include cataracts and raised intraocular pressure with chronic use. [5] [8]
The pitfall examiners test is the abrupt cessation of a long course, which can precipitate adrenal crisis. The safe practice is to wean any course beyond about two to three weeks. A second pitfall is the under-recognition of inhaled-steroid adrenal suppression — symptomatic suppression has been reported at moderate doses of inhaled corticosteroid, particularly fluticasone, so a child on very high doses who develops fatigue, hypoglycaemia, or poor growth needs the axis tested rather than reassured. A third is the failure to give stress doses perioperatively: the Association of Anaesthetists and Society for Endocrinology guidance is clear that patients with known adrenal insufficiency need additional parenteral hydrocortisone around surgery. A fourth is the mineralocorticoid gap — treating crisis with dexamethasone alone leaves the child salt-wasting. [5] [6] [10]
Prognosis & Disposition
The prognosis of corticosteroid therapy depends almost entirely on whether the prescribing was disciplined. A short course for asthma or croup resolves the exacerbation with negligible axis effect, and the child goes home well. A long course that is weaned carefully leaves a child whose axis recovers over weeks to months, during which the family carries the sick-day rules and emergency hydrocortisone and the child wears a MedicAlert identifier. A long course stopped abruptly, or a steroid-dependent child whose stress cover is missed, can end in adrenal crisis and death. [9] [11]
Disposition follows the axis. The child treated and weaned well is discharged with primary care follow-up and advice to seek review during serious illness. The child with proven adrenal suppression is discharged under endocrinology with a written emergency plan, parent education on hydrocortisone injection, and school or daycare notification. The child who presented in crisis is admitted to PICU until stable, then stepped down to a ward for education and an endocrinology review before discharge, because the risk of recurrence is high without a robust plan. [7] [12]
Special Populations
Several groups need a modified approach. The preterm neonate receives corticosteroids only under a specialist protocol that balances bronchopulmonary dysplasia prevention against neurodevelopmental risk, and hydrocortisone has largely replaced dexamethasone for routine use. The child with complex chronic disease often needs long-term steroids for transplant, rheumatological, or gut disease, and these children carry the heaviest cumulative exposure; they need a coordinated steroid-sparing strategy, bone health monitoring, and a shared emergency plan with their subspecialty team. [4] [8]
The Indigenous and remotely living child with severe or recurrent disease may be far from acute services, which makes the sick-day rules and emergency hydrocortisone even more critical — a remote family must be able to give the first dose before retrieval arrives. The migrant or refugee child may have received steroids elsewhere without documentation, so a careful exposure history and a low threshold for axis testing guide the plan. The immunocompromised child on steroids is doubly vulnerable to infection, and live vaccines and varicella exposure need proactive management. In each group the principles are the same — right agent, right dose, right duration, and a plan for stress — but the execution bends to the child's circumstance and geography. [11]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric corticosteroid therapy is broad and mature, but the dose thresholds and weaning schedules remain regionally variable, so verify against your local formulary. Randomised trials underpin the acute-dose choices: Paniagua and colleagues showed that a short dexamethasone course is non-inferior to a five-day prednisolone course for childhood asthma, and the Egyptian comparison trial confirmed equivalence, which has shifted many emergency departments toward single or two-dose dexamethasone when adherence is uncertain. Croup dosing rests on a body of trials showing oral dexamethasone 0.15 mg/kg and nebulised budesonide are effective. Neonatal hydrocortisone for bronchopulmonary dysplasia was refined by the Watterberg trial, which shaped the move from dexamethasone toward hydrocortisone. [1] [2] [3] [4]
The adrenal suppression and crisis management guidance comes from endocrine consensus. The Hahner and Husebye reviews, and the Nowotny consensus on adrenal crisis management, set the age-banded stress-dose hydrocortisone and the principle of empirical treatment. The Association of Anaesthetists, Royal College of Physicians and Society for Endocrinology perioperative guideline sets the surgical stress cover, though the historical practice of large perioperative doses has been questioned and modern guidance is more restrained. The inhaled-steroid suppression literature — the Patel case series and the Schwartz review — established that clinically significant adrenal suppression occurs at moderate-to-high inhaled doses, prompting the regulatory warnings on fluticasone in particular. [5] [7] [9] [10]
[5] [10]Exam Pearls
Examiners reward three things in this topic. First, the equivalent-dose ladder — know that hydrocortisone 20 mg equals prednisolone 5 mg equals methylprednisolone 4 mg equals dexamethasone 0.75 mg, and know that dexamethasone is twenty-five to thirty times as potent as hydrocortisone. Second, the age-banded stress hydrocortisone — 25 mg infant, 50 mg young child, 100 mg adolescent — given empirically in crisis, not after the cortisol result. Third, the two-to-three-week rule — any course of pharmacologic systemic dosing longer than this needs weaning, and the suppressed axis takes weeks to months to recover. [8] [9]
State the agent, the dose, the duration, and the weaning plan in one breath, and you have told the examiner you understand corticosteroid therapy. Never say "it is recommended" — say what you will give, to whom, and why. Remember that the mineralocorticoid activity is independent of the glucocorticoid potency, that hydrocortisone is the crisis drug, and that the weaning plan is what separates a course that heals from one that harms. [8] [11]
References
- [1]Paniagua N, Lopez R, Munoz N, Tames M, et al. Randomized Trial of Dexamethasone Versus Prednisone for Children with Acute Asthma Exacerbations. The Journal of pediatrics, 2017.PMID 29173304
- [2]Elkharwili DA, Ibrahim OM, Elazab GA, Elrifaey SM Two regimens of dexamethasone versus prednisolone for acute exacerbations in asthmatic Egyptian children. European journal of hospital pharmacy, 2020.PMID 32419935
- [3]Cetinkaya F, Tufekci BS, Kutluk G A comparison of nebulized budesonide, and intramuscular, and oral dexamethasone for treatment of croup. International journal of pediatric otorhinolaryngology, 2004.PMID 15013613
- [4]Watterberg KL, Walsh MC, Li L, Chawla S, et al. Hydrocortisone to Improve Survival without Bronchopulmonary Dysplasia. The New England journal of medicine, 2022.PMID 35320643
- [5]Patel L, Wales JK, Kibirige MS, Massarano AA, et al. Symptomatic adrenal insufficiency during inhaled corticosteroid treatment. Archives of disease in childhood, 2001.PMID 11567945
- [6]Schwartz RH, Neacsu O, Ascher DP, Alpan O Moderate dose inhaled corticosteroid-induced symptomatic adrenal suppression: case report and review of the literature. Clinical pediatrics, 2012.PMID 23043135
- [7]Husebye ES, Pearce SH, Krone NP, Kampe O Adrenal insufficiency. Lancet, 2021.PMID 33484633
- [8]Hahner S, Ross RJ, Arlt W, Bancos I, et al. Adrenal insufficiency. Nature reviews. Disease primers, 2021.PMID 33707469
- [9]Nowotny H, Ahmed SF, Bensing S, Beun JG, et al. Therapy options for adrenal insufficiency and recommendations for the management of adrenal crisis. Endocrine, 2021.PMID 33661460
- [10]Woodcock T, Barker P, Daniel S, Fletcher S, et al. Guidelines for the management of glucocorticoids during the peri-operative period for patients with adrenal insufficiency. Anaesthesia, 2020.PMID 32017012
- [11]Auron M, Raissouni N Adrenal insufficiency. Pediatrics in review, 2015.PMID 25733761
- [12]Lee SC, Baranowski ES, Sakremath R, Saraff V, et al. Hypoglycaemia in adrenal insufficiency. Frontiers in endocrinology, 2023.PMID 38053731