Paeds · clinical-pharmacology-and-therapeutics
Developmental pharmacology and age-related pharmacokinetics
Also known as Paediatric pharmacokinetics · ADME ontogeny · Neonatal drug handling · Developmental clinical pharmacology
Fellowship guide to how absorption, distribution, metabolism and excretion of medicines change across paediatric development, and the dosing and monitoring consequences from preterm neonate to adolescent.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Quote the developmental stage before you argue the dose. Postmenstrual age, postnatal age, weight in kilograms and the maturational trajectory of the relevant organ together set the safe exposure window. [1] [5]
A.D.M.E. — four phases, four maturation traps
Overview & Definition
Developmental pharmacology is the study of how drug handling and drug action change across the developmental continuum — from fetal life, through preterm and term neonate, infancy, childhood, adolescence and into adult transition. [1] The reason it deserves its own topic is that pharmacokinetics in children is not a scaled-down version of adult pharmacokinetics. The same dose per kilogram that is curative in a teenager can be lethal in a preterm neonate, because the gut, the body water compartments, the hepatic enzymes and the kidney all mature at different rates over the first months and years of life. [1] [5]
The working definition a fellowship candidate should hold is operational. Pharmacokinetics (PK) describes what the body does to the drug — absorption, distribution, metabolism and excretion, summarised by the apparent volume of distribution (Vd), clearance (CL) and half-life (t½). Pharmacodynamics (PD) describes what the drug does to the body. In paediatrics, PK is the dominant variable that changes with age, and the change is steepest in the first month of life. [1] [4]
The age variables that matter for prescribing are gestational age at birth, postmenstrual age (gestational plus postnatal, used as the covariate for renal maturation), postnatal age, corrected age, and weight in kilograms. [5] [7] The next sections walk through how each ADME phase matures, and how that should change what you write on the chart.
Classification
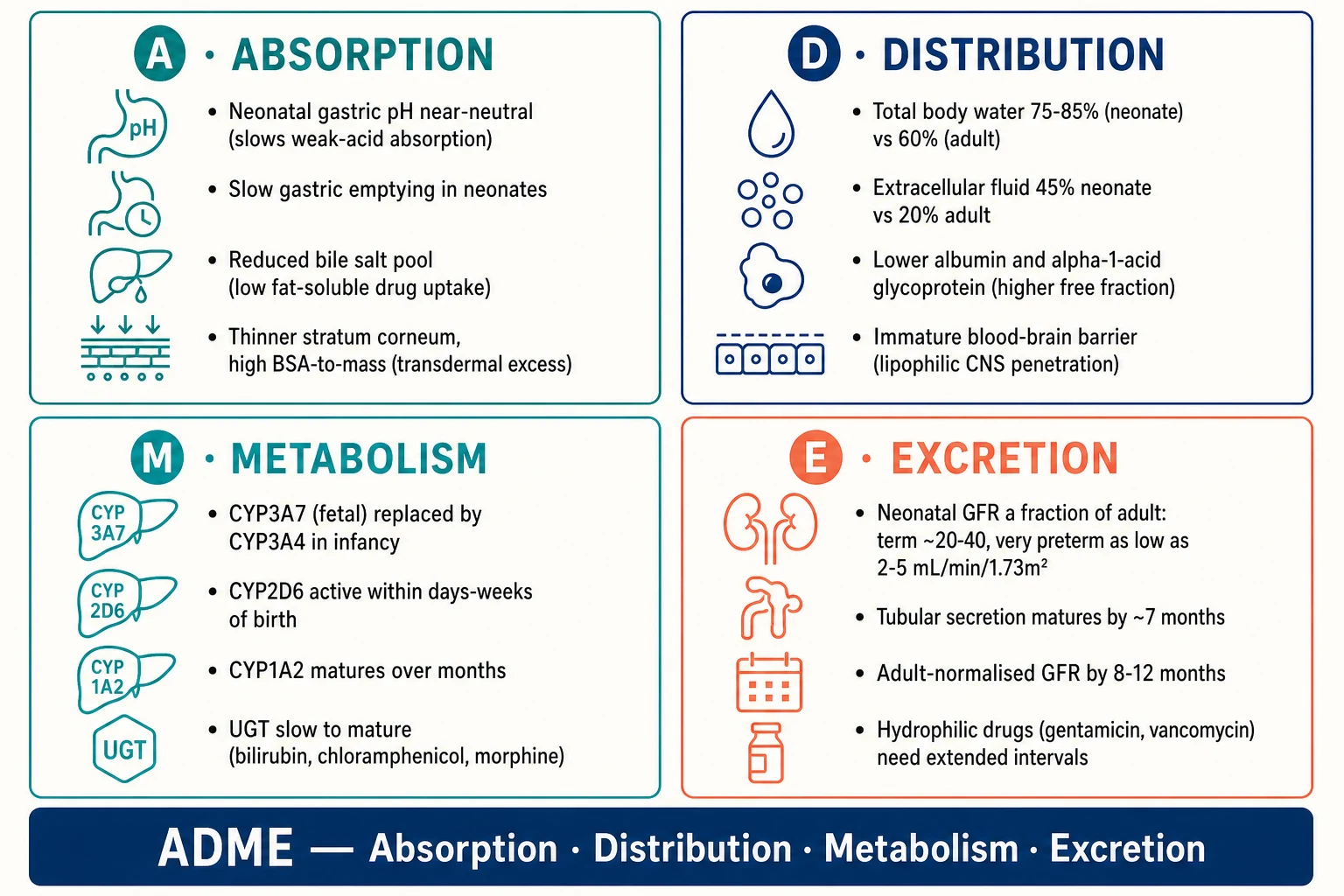
The four ADME phases — Absorption, Distribution, Metabolism and Excretion — are the scaffold every developmental pharmacology answer hangs on. Each phase has one or two maturational changes that have a clinically important dosing consequence. [1] [2]
Headline paediatric pharmacology numbers
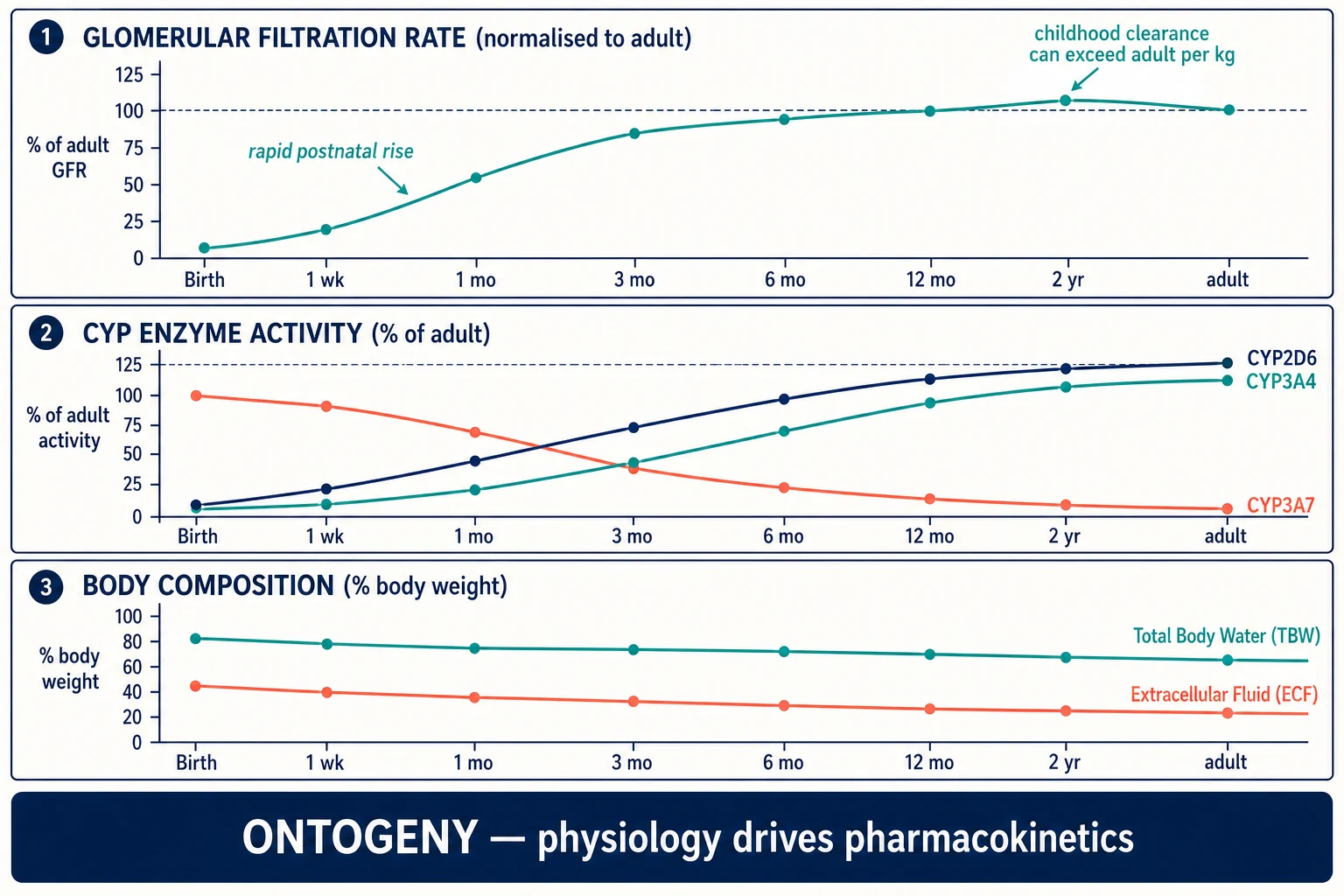
Two further dimensions complete the classification. Ontogeny is the time-dependent maturation of an enzyme, transporter or organ function — CYP3A7 falling as CYP3A4 rises, or GFR climbing from birth. Pharmacogenomics is the genetically determined variation in drug handling. The two interact: a CYP2D6 poor metaboliser genotype has different consequences in a neonate (whose enzyme is barely active anyway) versus a school-age child (whose enzyme is mature and now genetically constrained). [3] [10]
Epidemiology & Risk Factors
Neonates and infants under two months carry the highest risk of therapeutic failure and adverse drug reaction from adult-style dosing, because every ADME compartment is still maturing at once. Preterm birth amplifies each risk further: the gut is more permeable, the skin thinner, the body water fraction higher, the hepatic enzyme reserve smaller, and the glomerular filtration rate lower still. [5] [9]
Children are also disproportionately exposed to off-label and unlicensed medicines, because most drugs were historically studied in adults and never formally approved for paediatric use. [1] [9] This removes the safety net of an established reference dose and compounds the developmental vulnerability. Legislative change — the U.S. Pediatric Research Equity Act (PREA) and Best Pharmaceuticals for Children Act (BPCA), and the European Paediatric Regulation with its Paediatric Investigation Plans — has narrowed the evidence gap, but the legacy of the therapeutic orphan is still visible in everyday prescribing. [9]
Risk is compounded in specific populations: the complex chronically ill child on polypharmacy, the technology-dependent child whose fluid balance shifts constantly, the child with chronic kidney or liver disease whose clearance is already minimal, and the asphyxiated neonate under therapeutic hypothermia whose enzyme and renal clearance fall further still. Weight extremes matter too — obesity changes Vd of lipophilic drugs and confounds weight-based dosing, while failure to thrive lowers the body fat that buffers lipophilic exposure. [9] [11]
Pathophysiology
Developmental pharmacology is a story of organs maturing at different speeds. Walking through each ADME phase in turn shows why the same drug behaves differently at each age band. [1] [4]
Absorption. At birth the gastric pH is near-neutral (around 6 to 8), because acid secretion is immature. Weak acids such as phenytoin and phenobarbitone are poorly ionised in a near-neutral stomach and absorb erratically; adult gastric pH of around 1 to 3 develops over the first two years. [4] Gastric emptying is slower in neonates, the bile salt pool is reduced (limiting absorption of fat-soluble drugs such as vitamin K or diazepam), and the intestinal surface and transporter expression are immature. [6] The preterm skin is itself a route of systemic toxicity: the stratum corneum is thin and the ratio of body surface area to mass is high, so topical antiseptics (hexachlorophene, iodine), lignocaine-prilocaine (which can cause methaemoglobinaemia), and corticosteroids can produce clinically significant systemic exposure. [1] [5]
Distribution. Total body water and extracellular fluid are far higher in neonates than in adults. Total body water falls from about 75 to 85 per cent of body weight in the term neonate (and higher still in the preterm) to about 60 per cent in the adult; extracellular fluid falls from about 45 per cent to about 20 per cent. [4] The practical consequence is that water-soluble drugs such as gentamicin and vancomycin distribute into a larger volume, so a weight-based mg/kg dose produces a lower peak — which is why neonatal aminoglycoside dosing uses extended intervals and higher per-kg amounts than adult dosing. The opposite is true for lipophilic drugs (diazepam, phenytoin), whose Vd is smaller per kilogram in the neonate. [1] [4]
Plasma protein binding is also reduced in the neonate. Both albumin and alpha-1-acid glycoprotein are lower, and the available binding sites are occupied by endogenous competitors (bilirubin, free fatty acids). The free fraction of highly-bound drugs is therefore higher — phenytoin, furosemide and certain antibiotics behave as if a larger active dose has been given. [1] [4] This is also the mechanism by which sulphonamides, ceftriaxone and other highly-bound anions displace bilirubin from albumin and precipitate kernicterus. [1] The blood-brain barrier is functionally immature in the neonate, so opioids, barbiturates and bilirubin itself penetrate the central nervous system more readily. [5]
Metabolism. Hepatic drug metabolism occurs in two phases. Phase I is dominated by the cytochrome P450 family, whose isoforms mature at different rates — the classic maturational story. CYP3A7 is the fetal form and dominates at birth; it is progressively replaced by the adult form CYP3A4 over the first weeks to months of life, which is why midazolam, ciclosporin, tacrolimus and other 3A substrates behave differently in a neonate versus an older infant. [2] [6] CYP2D6 is active within days to weeks of birth; CYP1A2 matures over months; CYP2C9 and CYP2C19 follow intermediate trajectories. [3] [12] The first month of life is an ontogeny bottleneck: many phase I pathways are simultaneously under-expressed, narrowing the safe therapeutic window. [2]
Phase II conjugation matures more slowly than phase I. The uridine diphosphate glucuronosyltransferase (UGT) family is the clinically important example. UGT1A1, which conjugates bilirubin, is markedly deficient in the neonate — the biochemical basis of physiological jaundice. UGT2B7, which conjugates morphine, is slow to mature, prolonging opioid effect. The classic grey-baby syndrome of chloramphenicol — grey cyanosis, cardiovascular collapse and abdominal distension in neonates receiving adult-style cumulative exposure — is the textbook example of UGT immaturity producing a fatal adverse drug reaction. [1] [4]
Excretion. Renal elimination is the rate-limiting step for many water-soluble drugs. Glomerular filtration rate at birth is a fraction of adult values — around 20 to 40 mL per minute per 1.73 m² in the term neonate, lower in the preterm infant and as low as 2 to 5 mL per minute per 1.73 m² in the very premature baby — then rises sharply over the first two weeks of life as renal vascular resistance falls, and reaches adult-normalised values by about 8 to 12 months of age. [5] Tubular secretion matures a little later, approaching adult capacity by about 7 months. [6] The clinical consequence is that hydrophilic drugs cleared by the kidney — gentamicin, vancomycin, many beta-lactams, furosemide — must be dosed at extended intervals in the neonate and young infant, and the interval is widened further in the preterm baby. [5]
A counter-intuitive but high-yield fact is that per-kilogram clearance in mid-childhood can exceed adult clearance. [7] [8] Hepatic capacity and renal tubular secretion, normalised to body size, peak around early-to-mid childhood. A child on standard mg/kg dosing of an anti-epileptic (carbamazepine, phenytoin, valproate) or an antibiotic can therefore run subtherapeutic levels — a common reason for treatment failure that the fellowship examiner rewards. [7]
Clinical Presentation
Developmental pharmacology reveals itself clinically when a child responds unexpectedly to a 'standard' dose. The neonate who becomes apnoeic shortly after an opiate infusion is started, the preterm baby who turns grey on chloramphenicol, the jaundiced newborn whose bilirubin climbs after a sulphonamide, and the school-age child whose seizures break through on a textbook mg/kg dose of an anti-epileptic are all presentations of maturational pharmacology. [1] [4]
In a non-verbal infant the early signs of toxicity are subtle. Look for reduced suck and tone, a high-pitched or absent cry, excessive sedation that does not match the dose given, abnormal movements that could be seizure or drug effect, and a respiratory pattern that has changed since the last dose. In the neonate, apnoea, bradycardia and temperature instability are non-specific but should always prompt a medication review alongside sepsis and metabolic causes. [5]
Adverse drug reactions in children differ in pattern from adults. Skin reactions, behavioural change, growth and weight effects, and changes in developmental trajectory are common; attribution is harder because the child cannot describe symptoms and because many drugs are used off-label without a well-described paediatric safety profile. [9] Always suspect a drug when the temporal pattern fits, even if the listed adverse reaction is rare.
Differential Diagnosis
When a child responds unexpectedly to a drug, the developmental differentials should be exhausted before reaching for disease progression or non-adherence. [1] [9]
For unexpected toxicity in a neonate on a 'standard' weight-based dose, consider low clearance (renal or hepatic immaturity), low plasma protein binding raising the free fraction, immature blood-brain barrier allowing CNS penetration, a formulation excipient effect (ethanol, benzyl alcohol, propylene glycol), and a tenfold dosing error — each of which is common, and any of which can coexist. [5]
For subtherapeutic drug levels in a mid-childhood patient, the developmental differential is that per-kilogram clearance has overshot adult rates, so the standard mg/kg dose produces a sub-therapeutic peak. Other causes include adherence (ask before re-dosing), malabsorption, a drug interaction that induces clearance (for example rifampicin on oral contraceptives or anti-epileptics), and a formulation change (switching brands of an anti-epileptic with narrow therapeutic index). [7] [10]
For apnoea in a preterm neonate after an opiate or caffeine, distinguish true drug effect from disease progression (sepsis, intraventricular haemorrhage), anaemia, patent ductus arteriosus, and temperature instability. For hyperbilirubinaemia worsening on therapy, distinguish UGT immaturity, drug-albumin displacement, haemolysis, sepsis and biliary obstruction. For nephrotoxicity during aminoglycoside therapy, distinguish developmental immaturity, hypovolaemia, a co-administered nephrotoxin (non-steroidal anti-inflammatory, contrast) and an underlying renal anomaly. [4] [5]
Clinical & Bedside Assessment
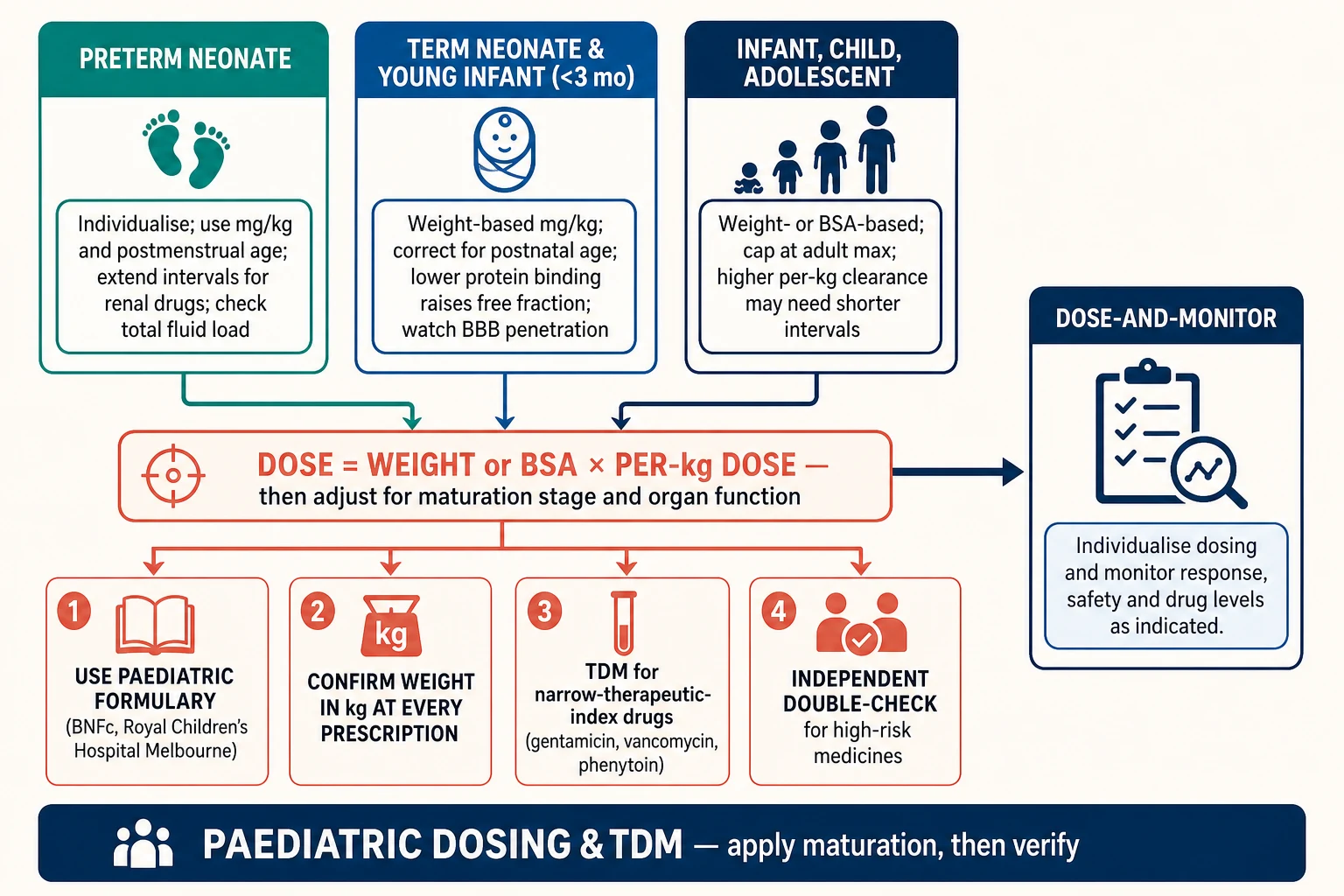
The bedside assessment of developmental pharmacology starts with the right age variables. Document gestational age at birth, postmenstrual age, postnatal age, corrected age, weight in kilograms (measured, never estimated), length, and where relevant body surface area. [5] [7] Confirming weight in kilograms at every prescription is the single highest-yield error-prevention step — pounds-and-kilograms confusion and estimated weights underpin a large fraction of paediatric tenfold errors. [1]
Assess hydration, perfusion and organ function before prescribing renally or hepatically cleared drugs. In the neonate this means capillary refill, colour, urine output, the most recent creatinine and bilirubin, and the overall trajectory. In the older child, add a focused hydration and abdominal exam and the most recent renal and liver function tests. [5]
Recognise the signs of drug effect, adverse effect and withdrawal in a non-verbal infant. Suck, tone, cry, sedation state and seizure activity are the relevant observations. Counsel caregivers on liquid medicine measurement — an oral syringe, never a household spoon — on storage, and on the specific return triggers (worsening breathing, reduced feeding, abnormal drowsiness, rash) that should bring them back. [9]
Always check a paediatric formulary before prescribing. In Australia and New Zealand this means the Royal Children's Hospital Melbourne guidelines; in the UK and many Commonwealth settings, the BNF for Children; for neonatal dosing in many units, Neofax; and globally, the WHO Model List of Essential Medicines for Children. [1] [9] These formularies have already translated the developmental science into age-banded doses; do not reproduce adult doses from memory.
Investigations
Therapeutic drug monitoring (TDM) is indicated for narrow-therapeutic-index drugs, when pharmacokinetics are unpredictable, in serious infection, in renal or hepatic impairment, and in critical illness. The high-yield paediatric TDM drugs are gentamicin (extended-interval peak and trough, or area-under-curve-based dosing), vancomycin (area-under-curve to minimum inhibitory concentration ratio target 400 to 600), and phenytoin (total 10 to 20 mg/L and free 1 to 2 mg/L). [4] The detailed sampling schedules and dosing adjustment formulas belong to the dedicated therapeutic-drug-monitoring topic; the developmental point here is that neonatal hypoalbuminaemia invalidates a total phenytoin level — measure the free level when albumin is low. [4]
Creatinine-based estimation of glomerular filtration rate (the Schwartz formula in children) is useful for renally cleared drugs but has limits in neonates and during acute kidney injury, where the creatinine reflects maternal transfer and a non-steady state. [5] Bilirubin, albumin and liver function tests inform dose adjustment for highly-bound or hepatically cleared drugs. Pharmacogenomic testing — CYP2D6 before codeine (avoid in children), TPMT before thiopurines, HLA-B*15:02 before carbamazepine in susceptible populations — is increasingly available, but developmental status can override genotype: a neonate's CYP2D6 is barely active regardless of genotype, so the pharmacogenomic result changes management mainly once the enzyme has matured. [3] [10]
Management — Resuscitation
When a neonate or infant shows unexpected toxicity from a 'standard' weight-based dose, the immediate priority is the child, not the analysis. Stop the suspected drug. Run an ABCDE assessment. Give the specific antidote where one exists — naloxone for opioid toxicity (titrated to respiratory effort, not full alertness, to avoid precipitating withdrawal), flumazenil for benzodiazepine toxicity only when the risk-benefit is clear, and supportive care for the rest. Escalate early to senior paediatric and PICU or neonatal help. [5]
For specific syndromes, the resuscitation is syndrome-tailored. Grey-baby syndrome from chloramphenicol requires immediate drug cessation, cardiovascular support and exchange transfusion in severe cases. Kernicterus from bilirubin displacement requires intensive phototherapy and, in severe cases, exchange transfusion. Methaemoglobinaemia from topical lignocaine-prilocaine requires methylthioninium chloride (methylene blue) when symptomatic. [1] [4]
Preserve the order, the pump settings, the syringe and the original drug chart for investigation after a suspected tenfold or concentration error. Open disclosure to the family begins once the child is stable and follows the local open-disclosure policy; the developmental pharmacology framing helps explain that a 'normal' adult dose produced toxicity because the child's clearance was immature, but it does not excuse the error. [1]
Management — Definitive & Stepwise
The canonical paediatric prescribing sequence applies maturation at every step. [1] [9]
- Confirm age and weight. Gestational and postmenstrual age for neonates; weight in kilograms, measured, for every prescription.
- Confirm the indication and that the drug is appropriate for that age band (check for contraindications, excipient safety, and off-label status).
- Look up the paediatric dose in the formulary — do not reproduce adult doses from memory.
- Apply maturation adjustment. Use postmenstrual and postnatal age to extend intervals for renally cleared drugs in neonates and young infants; cap weight-based doses at the adult maximum for older or larger children.
- Choose the formulation. Liquid for infants, soluble or small solid for young children, standard forms for adolescents. Check excipient safety (ethanol, propylene glycol, benzyl alcohol) in premature neonates.
- Specify route, frequency, duration and monitoring plan — including TDM sampling times for narrow-therapeutic-index drugs.
- Independent double-check for high-risk medicines (insulin, opioids, infusions, chemotherapy, anticoagulants).
- Document and communicate — to nursing staff, to the family, and to primary care at discharge. [1] [9]
Choose between weight-based (mg/kg) and body-surface-area (mg/m²) dosing deliberately. Weight-based dosing covers most paediatric medicines; BSA-based dosing is preferred for cancer chemotherapy, high-dose corticosteroids and certain fluids because it scales more accurately across the body composition changes of childhood. The BSA formula (Mosteller: square root of [height in cm × weight in kg divided by 3600]) and its derivation are covered in the dedicated weight-based-dosing topic; the developmental point is that BSA remains the better scaler for cytotoxics because it tracks organ blood flow better than weight alone. [7]
For renally cleared drugs in neonates, apply maturation adjustment using both postmenstrual and postnatal age — a preterm baby at 32 weeks postmenstrual age clears gentamicin at roughly half the rate of a term baby at the same postnatal age. [5] As the child grows, watch for the per-kilogram clearance overshoot: anti-epileptic and antibiotic levels in school-age children sometimes need higher mg/kg doses or shorter intervals than the textbook states. [7] [8]
TDM-based dose revision is a cycle, not a one-off. Sample at steady state (around five half-lives after a dose change), interpret the level against the age-appropriate target and the child's organ function, adjust using population pharmacokinetic principles, and re-sample to confirm. The detailed target ranges belong to the therapeutic-drug-monitoring topic; the developmental point is that the target itself is stable across ages but the dosing needed to reach it is not. [4]
Specific Subtypes & Scenarios
Each age band has its own pharmacological signature. [1] [5]
Preterm neonate. Every compartment is immature at once — gut, skin, liver and kidney — and fluid shifts are large. Doses are highly individualised; high-risk medicines are usually discussed with neonatal pharmacy. Watch formulation excipients closely: benzyl alcohol, propylene glycol and ethanol (even in small amounts) can accumulate in the very preterm baby. [5]
Term neonate (first month). CYP3A7 is still active, protein binding is low, the blood-brain barrier is immature, and GFR is rising sharply but still low. This is the age band of the classic toxicities: grey-baby syndrome from chloramphenicol, kernicterus from bilirubin displacement, opioid over-sedation, and local-anaesthetic methaemoglobinaemia. [1] [4]
Young infant (1 to 3 months). GFR is approaching adult-normalised values but UGT is still rising. Gentamicin intervals begin to shorten and paracetamol weight bands apply (the 2 to 3 month infant can receive a larger per-kg dose than the neonate). [4]
Older infant and toddler (3 months to 2 years). Many drugs clear more rapidly per kilogram than in adults; higher mg/kg doses and shorter intervals may be needed to maintain exposure. [7]
School-age child. Per-kilogram clearance can exceed adult, so weight-based dosing alone can under-treat. Anti-epileptics, antibiotics and certain anaesthetics are the common culprits. [7] [8]
Adolescent. Physiology is approaching adult; consider the body composition changes of puberty, adherence (which often worsens), substance use that may interact with prescribed drugs, and the formal transition of care to adult services. [9]
Child with obesity. Weight-based dosing can overdose lipophilic drugs. Ideal or adjusted body weight is used for induction agents and certain anaesthetics; the dedicated weight-based-dosing topic covers the detail. [11]
Child with hepatic or renal impairment. Combine maturation with the organ dysfunction to derive an individualised dose and a TDM plan. [5]
Child on extracorporeal circuits (ECMO, continuous renal replacement therapy, cardiopulmonary bypass). Volume of distribution and clearance are altered, drugs are sequestered in the circuit, and sampling artefacts are common; specialist pharmacy input is essential. [9]
Asphyxiated neonate under therapeutic hypothermia. Hypothermia reduces clearance of morphine, phenobarbital and anti-epileptics; dosing intervals are extended and TDM is used where available. [5]
Complications & Pitfalls
The classic mistakes in paediatric prescribing are predictable, and the fellowship examiner probes them deliberately. [1]
Applying adult doses or adult normal ranges to neonates and infants without maturation adjustment is the cardinal error. Confusing pounds and kilograms, or using an estimated weight for a high-risk medicine, is the highest-yield error-prevention failure. Missing the CYP3A7-to-CYP3A4 switch and interpreting a neonate's poor midazolam response as 'tolerance' rather than ontogeny is a subtle trap. Using a total rather than free phenytoin level in a hypoalbuminaemic neonate or child produces dangerous under-treatment of toxicity. [4]
Prescribing chloramphenicol, sulfonamides or ceftriaxone to neonates at risk of grey-baby or bilirubin displacement is now rare but still tested. Extending gentamicin intervals without confirming that renal maturation has caught up risks under-treatment of sepsis in young infants. Ignoring formulation excipients (ethanol, benzyl alcohol, propylene glycol) in premature neonates can produce toxicity that mimics sepsis. Assuming a school-age child with a normal creatinine clears drugs at adult per-kilogram rates leads to under-dosing of anti-epileptics and antibiotics. Forgetting to counsel caregivers on liquid medicine measurement with an oral syringe produces household-spoon dosing errors. [5] [9]
Prognosis & Disposition
Developmental stage predicts how long special monitoring is needed after an adverse drug event. A preterm neonate who has had an opiate over-sedation needs close observation until renal and hepatic clearance catch up with the drug burden; an adolescent on the same drug may clear it within hours. [5]
Transition from paediatric weight-based dosing to adult dosing is individualised rather than calendar-driven. The cut-point is usually late adolescence, when body composition, hepatic capacity and renal clearance approach adult values, and when transition-of-care planning is in place. [9]
After neonatal nephrotoxic or ototoxic drug exposure, follow-up should include renal function and audiology surveillance as the child grows, because the full consequence of an early insult may not be apparent until later development. [5]
Developmental pharmacology must be communicated to families and to primary care at discharge so that future prescriptions stay safe. A simple explanation — "this baby clears the drug more slowly because their liver and kidney are still maturing" — is usually enough; the key safety-netting points are the weight, the formulary dose, the return triggers, and the named contact. [9]
Special Populations
Preterm and extremely preterm neonates are the highest-risk group: multi-compartment immaturity, large fluid shifts, and minimal hepatic reserve. [5] Term neonates in the first month of life carry the classic neonatal pharmacology toxicities (grey-baby, kernicterus, opioid over-sedation). Infants with failure to thrive and low body fat have an altered Vd for lipophilic drugs. Children with cerebral palsy, neurodisability or autonomic dysfunction have altered gut motility, secretion and tone that change absorption and clearance. [9]
Children with chronic kidney disease or end-stage renal failure already have minimal GFR; dialysis pharmacokinetics add another layer (drugs are cleared by the dialysate as well as residual renal function), and the dedicated renal-and-hepatic-dose-adjustment topic covers the detail. [5] Children with chronic liver disease or post-hepatic transplant have altered first-pass metabolism and protein binding. Children with medical complexity on multiple concurrent medications experience polypharmacy and drug interactions amplified by maturational status. [9]
Asphyxiated neonates under therapeutic hypothermia have reduced clearance across both enzyme and renal pathways. Adolescents may be on hormonal therapies, gender-affirming care, or transitioning to adult services. Indigenous, migrant and refugee families need equitable access to formularies, language-appropriate communication for safe dosing, and equity of monitoring — the science is the same, but the access is not. [9]
Evidence, Guidelines & Regional Differences
The evidence base for developmental pharmacology rests on a small number of landmark reviews that a fellowship candidate should be able to name. [1]
Kearns and colleagues established the modern framework in their 2003 New England Journal of Medicine review, which defined the ADME-based developmental approach and remains the foundational reference. [1] Hines mapped the ontogeny of the cytochrome P450 family in 2008 and detailed the developmental expression of drug-metabolising enzymes in 2013 — these are the references for the CYP3A7-to-CYP3A4 switch and the isoform-specific maturation timelines. [2] [3] van Groen and colleagues provided the comprehensive 2021 Pharmacological Reviews synthesis of hepatic transporter and drug-metabolising enzyme ontogeny across species. [6]
de Wildt wrote the accessible 2014 Drug metabolism for the paediatrician in Archives of Disease in Childhood — the bedside-friendly summary of phase I and II maturation. [4] van den Anker set out the considerations for drug dosing in premature infants in 2021, including the renal maturation timeline. [5] Chapron and colleagues reviewed recent advances in the ontogeny of drug disposition in 2022, including the per-kilogram clearance overshoot. [8]
Anderson established the mechanistic basis of using body size and maturation to predict clearance in humans — the allometric and maturation modelling that underlies modern population pharmacokinetics in children. [7] Smits and colleagues, in the 2022 conect4children and European Society for Developmental, Perinatal and Paediatric Pharmacology White Paper, set out current knowledge, challenges and innovations. [9] Leeder reviewed the ontogeny of paediatric pharmacogenetics in 2022, showing how genotype and developmental stage interact. [10] Morse contributed pharmacokinetic-pharmacodynamic modelling contributions to paediatric anaesthesia practice in 2022. [11] Thakur summarised the ontogeny of drug-metabolising enzymes as a methodology reference in 2021. [12]
Landmark evidence to quote
Narrative reviews and consensus white papers
Population: Paediatric developmental pharmacology evidence base
Key finding
The corpus converges on a single framework: PK is the dominant paediatric variable, ADME each matures at a different rate, and weight- or BSA-based dosing alone is insufficient without maturation adjustment.
The main controversies are about how to operationalise the science. Extrapolation of adult pharmacokinetics to children remains common where paediatric data are missing, and population pharmacokinetic and physiologically-based pharmacokinetic (PBPK) modelling increasingly substitute for clinical studies in younger children. Whether childhood clearance overshoots adult or simply plateaus at the same per-kilogram rate is an area of active research with implications for dose selection in school-age children. [7] [8]
Exam Pearls
- Lead with ADME — name the phase and the maturational change before you argue the dose. [1]
- Grey-baby syndrome is UGT immaturity (chloramphenicol); kernicterus is UGT1A1 deficiency plus drug-albumin displacement. [4]
- Neonatal gastric pH is near-neutral; weak acids (phenytoin, phenobarbitone) absorb poorly; adult pH by about 2 years. [4]
- Total body water falls from about 75 to 85 per cent (neonate) to about 60 per cent (adult); extracellular fluid from about 45 per cent to about 20 per cent. [4]
- GFR is a fraction of adult at birth (term ~20-40 mL/min/1.73 m², very preterm as low as 2-5), rises sharply in the first two weeks, and is adult-normalised by 8 to 12 months. [5]
- Per-kilogram clearance can exceed adult in mid-childhood — a common reason for subtherapeutic anti-epileptic and antibiotic levels. [7]
- Always cap weight-based doses at the adult maximum for larger or older children. [9]
- Confirm weight in kilograms at every prescription — the single highest-yield error-prevention step. [1]
- The classic teaching: aminoglycoside intervals are extended in neonates and shortened as the child matures; vancomycin targets AUC/MIC 400 to 600; phenytoin uses total 10 to 20 mg/L unless albumin is low, when the free level is needed. [4]
- Boards reward: ADME phase + age band + maturational mechanism + dose consequence + TDM + one named classic toxicity. [1] [2]
References
- [1]Kearns GL Developmental pharmacology--drug disposition, action, and therapy in infants and children. N Engl J Med, 2003.PMID 13679531
- [2]Hines RN The ontogeny of drug metabolism enzymes and implications for adverse drug events. Pharmacol Ther, 2008.PMID 18406467
- [3]Hines RN Developmental expression of drug metabolizing enzymes: impact on disposition in neonates and young children. Int J Pharm, 2013.PMID 22766445
- [4]de Wildt SN Drug metabolism for the paediatrician. Arch Dis Child, 2014.PMID 25187498
- [5]van den Anker J Considerations for Drug Dosing in Premature Infants. J Clin Pharmacol, 2021.PMID 34185893
- [6]van Groen BD Ontogeny of Hepatic Transporters and Drug-Metabolizing Enzymes in Humans and in Nonclinical Species. Pharmacol Rev, 2021.PMID 33608409
- [7]Anderson BJ Mechanistic basis of using body size and maturation to predict clearance in humans. Drug Metab Pharmacokinet, 2009.PMID 19252334
- [8]Chapron BD Recent advances in the ontogeny of drug disposition. Br J Clin Pharmacol, 2022.PMID 33733546
- [9]Smits A Current knowledge, challenges and innovations in developmental pharmacology: A combined conect4children Expert Group and European Society for Developmental, Perinatal and Paediatric Pharmacology White Paper. Br J Clin Pharmacol, 2022.PMID 34180088
- [10]Leeder JS Ontogeny of Pediatric Pharmacogenetics: Celebrating the Past and Vision for the Future. J Pediatr Pharmacol Ther, 2022.PMID 35002553
- [11]Morse JD Pharmacokinetic Pharmacodynamic Modelling Contributions to Improve Paediatric Anaesthesia Practice. J Clin Med, 2022.PMID 35683399
- [12]Thakur A Ontogeny of Drug-Metabolizing Enzymes. Methods Mol Biol, 2021.PMID 34272706