Paeds · clinical-pharmacology-and-therapeutics
Drug interactions and medication reconciliation
Also known as Drug-drug interactions in children · Cytochrome P450 interactions · Medication reconciliation · Best Possible Medication History · Polypharmacy in children
A fellowship approach to drug interactions and medication reconciliation in children covering cytochrome P450 induction and inhibition, pharmacodynamic additive toxicity, developmental changes in drug handling that shift interaction risk by age, the Best Possible Medication History, and the structured reconciliation of every medicine across admission, transfer and discharge.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A teenager on long-term tacrolimus after a liver transplant who is prescribed fluconosal for oral thrush and presents a week later with tremor and rising tacrolimus levels; a preschool child whose theophylline toxicity is unmasked by a five-day course of erythromycin; a complex child discharged on twelve medicines of which three are unintentionally duplicated — these are the faces of drug interactions and failed reconciliation at the bedside. A drug interaction is a clinically meaningful change in the effect or concentration of one drug caused by another drug, food, or substance, and most clinically important interactions are predictable from a knowledge of drug metabolism and pharmacodynamics. [1] [5]
Medication reconciliation is the formal process of creating the most accurate possible list of everything a child actually takes and comparing that list against every new prescription at each transition of care. The list is called the Best Possible Medication History, and it is built from at least two sources: the family interview, the community pharmacy record, the general practitioner summary, and any transfer letter or prior discharge summary. Reconciliation is not a clerical task; it is the structured check that catches the interacting medicine, the omitted medicine, the duplicated medicine, and the wrong dose before they reach the child. [7] [8]
From first prescription to safe transition
1 · Anticipate
Before prescribing, ask which enzyme metabolises each drug, and whether the new drug induces or inhibits it. Check the interaction against the child's age and organ function.
2 · Collect the BPMH
At admission, build the Best Possible Medication History from at least two sources, including name, dose, route, frequency, last dose, and adherence for every medicine, including over-the-counter and herbal products.
3 · Compare
Reconcile the BPMH against every new order. Flag omissions, duplications, wrong doses, wrong frequencies, and interactions for resolution with the prescriber.
4 · Communicate
At transfer and discharge, produce a verified, reconciled list. Explain changes to the family in plain language and confirm the community pharmacy and GP receive the updated plan.
5 · Monitor and review
For high-risk combinations, plan therapeutic drug monitoring and clinical review. Set the point at which the interaction will be reassessed.
Classification
Drug interactions fall into three families, and a candidate should hold all three at once: pharmacokinetic interactions that change drug concentration through absorption, distribution, metabolism, or excretion; pharmacodynamic interactions that change drug effect at the same receptor or physiological pathway without changing concentration; and pharmaceutical interactions that occur before the drug reaches the child, such as incompatibility in an intravenous line. The pharmacokinetic interactions driven by cytochrome P450 metabolism are the largest and most clinically important group in children. [1] [3]
Pharmacokinetic interactions act at four points. Absorption changes: drugs that chelate or bind in the gut reduce the availability of another, as when phosphate binders or calcium-containing antacids reduce ciprofloxacin absorption, or when continuous enteral feeds bind phenytoin. Distribution changes through displacement from plasma proteins, which matters mainly for highly bound drugs such as warfarin and phenytoin. Metabolism changes through cytochrome P450 induction or inhibition are the most consequential and the most predictable. Excretion changes when one drug alters the renal clearance of another, as when probenecid reduces penicillin excretion. [2] [4]
The pharmacodynamic interactions are the additive and antagonistic effects at the target. Two sedatives given together produce more sedation than either alone; two QT-prolonging drugs given together raise the risk of torsades de pointes; a non-steroidal anti-inflammatory drug added to an angiotensin-converting-enzyme inhibitor and a loop diuretic in a volume-depleted child produces the well-described triple-whammy acute kidney injury. These interactions do not change the concentration of either drug; they change the physiological effect when two drugs act on the same system. [1] [5]
| Feature | Pharmacokinetic | Pharmacodynamic |
|---|---|---|
| What changes | Drug concentration | Drug effect at the target |
| Mechanism | Absorption, distribution, metabolism, excretion | Receptor synergy, antagonism, shared pathway |
| Typical paediatric example | Erythromycin inhibits CYP3A4 and raises tacrolimus | SSRI plus tramadol causes serotonin syndrome |
| Detection | Drug levels, enzyme knowledge | Shared physiological effect recognition |
| Resolution | Dose adjust, substitute, monitor | Avoid combination or reduce combined effect |
Epidemiology & Risk Factors
Drug interactions are common in hospitalised children and the risk rises steeply with the number of medicines a child takes. A study of cytochrome P450-mediated interactions in children admitted to intensive care found that a substantial proportion of patients were exposed to at least one potentially clinically significant interaction, and that the probability rose with polypharmacy, organ failure, and the use of enzyme inhibitors or inducers. The child with a complex chronic condition on many drugs is therefore the child at greatest risk, and that child is increasingly common in modern paediatric practice. [1] [6]
Polypharmacy is the single strongest driver of interaction and reconciliation risk. A large United States inpatient study defined polypharmacy as exposure to five or more medications and found that it affected a significant and growing share of hospitalised children, concentrated among those with complex chronic conditions, technology dependence, and prolonged admissions. Every additional medicine on a child's list multiplies the possible drug pairs that can interact, so the complex child on twelve medicines is not simply twelve times the risk of the child on one — the combinatorial exposure is far greater. [6]
Previously well child
Short admission, few drugs
- Few concurrent drugs and few pairs
- Lower baseline interaction risk
- Reconciliation still needed at discharge
- Focus on acute prescriptions
Complex chronic child
Polypharmacy, technology
- Many concurrent drugs and many pairs
- High interaction and omission risk
- Pharmacist-led reconciliation essential
- Therapeutic drug monitoring common
Transplant or oncology
Calcineurin inhibitors
- Tacrolimus or ciclosporin substrates of CYP3A4
- Azoles and macrolides raise levels dangerously
- Close TDM and immunology liaison
- Adjust dose preemptively
Neonate
Immature CYP and renal function
- Slower metabolism prolongs half-lives
- Interaction magnitude differs by age
- Renal excretion immature
- Age-adjusted dosing essential
Transition points are where reconciliation errors concentrate. Admission, transfer between wards or units, and discharge each create a handover of the medicines list, and each is a moment where an omission, duplication, or wrong dose can be introduced. Prescribing errors, including those arising from incomplete reconciliation, are documented across paediatric inpatient settings and are more frequent in critically ill children where drug load and acuity are highest. Recognising these transitions as high-risk moments is the first step in preventing the errors they generate. [11] [12]
Pathophysiology
The cytochrome P450 enzyme family in the liver and intestinal wall metabolises the majority of clinically used drugs, and most clinically important pharmacokinetic interactions act through it. A small number of isoenzymes do most of the work: CYP3A4 handles the largest share of commonly used drugs, while CYP2D6, CYP2C9, CYP2C19, and CYP1A2 each metabolise specific groups. An interaction occurs when one drug either inhibits an enzyme — slowing the metabolism of a second drug that depends on it — or induces the enzyme — increasing its synthesis and accelerating the clearance of the substrate drug. [2] [3]
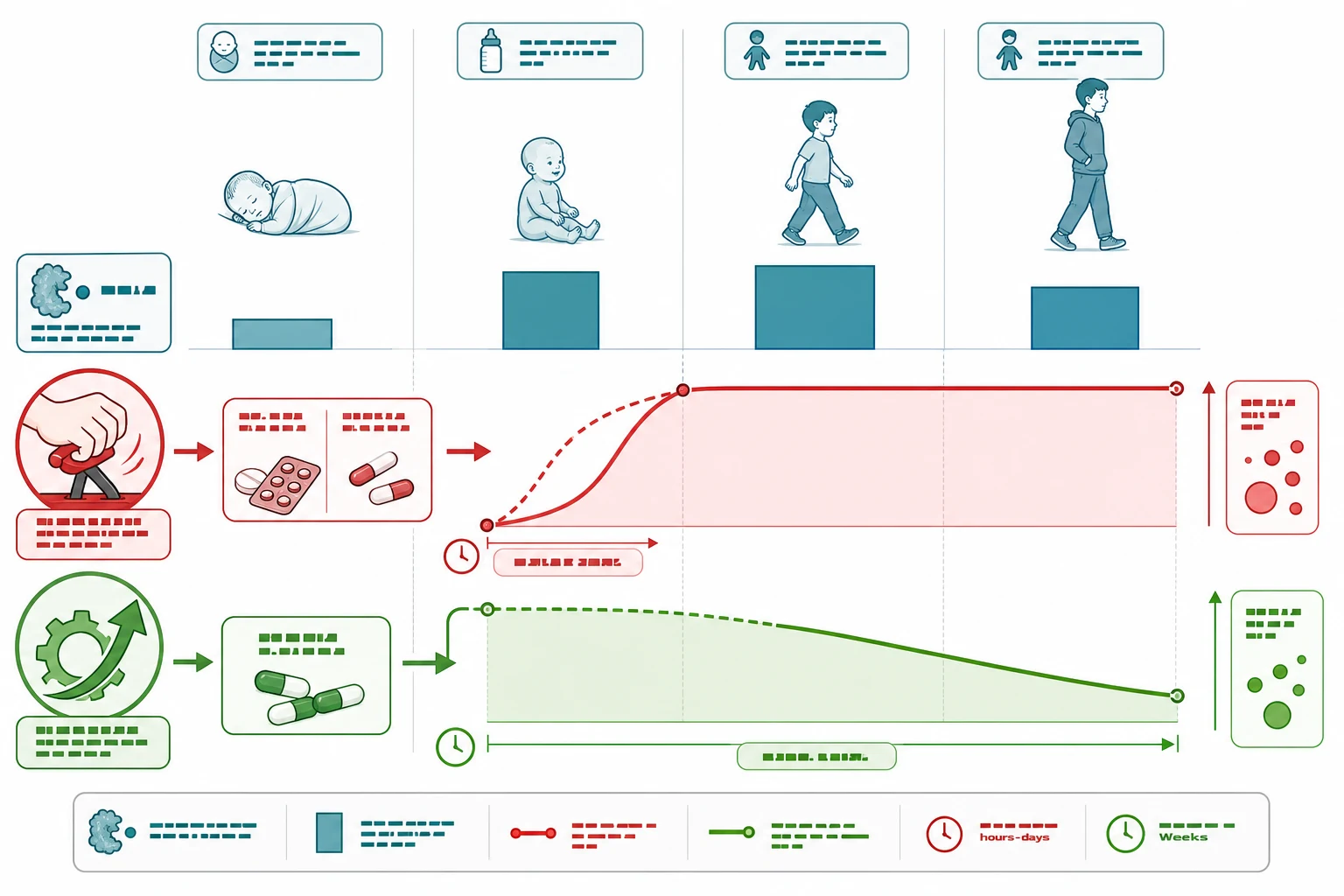
The direction and speed of the effect differ between inhibitors and inducers, and this timing matters clinically. Inhibition begins within hours to days of starting the inhibitor, so the substrate drug accumulates and toxicity can appear quickly — a child on a stable tacrolimus dose who starts fluconazole for thrush may develop tremor and rising levels within a week. Induction takes longer because it requires new enzyme protein synthesis; rifampicin lowers oral contraceptive, warfarin, and anticonvulsant levels over one to two weeks, so the loss of efficacy is delayed and may be missed unless the interaction is anticipated. [1] [2]
Developmental pharmacokinetics shift both the baseline handling of every drug and the magnitude of any interaction. At birth, hepatic cytochrome P450 activity — particularly CYP3A4 and CYP2D6 — is immature, so many drugs are cleared slowly and half-lives are prolonged; this is why neonates tolerate less and need lower or less frequent dosing. During infancy and early childhood, enzyme activity per kilogram often exceeds adult values, so clearance is faster and some children need higher weight-adjusted doses. The neonate exposed to a CYP3A4 inhibitor therefore experiences a larger proportional rise in substrate concentration than an older child on the same combination. [2] [4]
Renal maturation runs in parallel with hepatic maturation and matters for renally cleared drugs and their interactions. Glomerular filtration is low at birth, approaches adult values during the first year of life, and exceeds adult per-kilogram values during childhood before settling. A renally cleared substrate drug therefore behaves differently in a neonate than in a school-age child, and a drug that reduces renal clearance will have a greater effect when filtration is immature. Developmental changes are the reason the same interaction can be trivial in an adolescent and dangerous in a neonate. [4]
Clinical Presentation
The clinical presentation of a drug interaction is the presentation of the effect: toxicity when a substrate drug accumulates, or loss of disease control when an inducer lowers its level. There is no single interaction syndrome, so the examiner is testing whether the candidate connects an unexpected clinical change to a recent prescription change. A child with new tremor and rising tacrolimus levels after starting an azole; a child with breakthrough seizures after rifampicin is added for tuberculosis; a child with serotonin syndrome after tramadol is added to a selective serotonin reuptake inhibitor — each presents through the downstream effect. [1] [5]
Several bedside cues flag an interaction worth considering. Any unexpected clinical change that follows a recent prescription addition or dose change is an interaction until proved otherwise. A child on a narrow-therapeutic-index drug such as phenytoin, tacrolimus, ciclosporin, digoxin, or theophylline who develops new symptoms is a priority for a level check and an interaction review. A child whose previously controlled chronic disease suddenly destabilises after a new prescription may have lost efficacy through induction rather than disease progression. [5] [12]
The unreconciled medicines list is itself a clinical presentation. A child admitted with a medicines list built from one source, with no verification against the family or the community pharmacy, carries an elevated risk of omission and duplication errors that will surface as either missed essential therapy or unintended double dosing. Recognising an unverified list at the bedside — and acting on it by completing the reconciliation — is a clinical skill the fellowship candidate must demonstrate. [7] [8]
Differential Diagnosis
The differential in this topic is the set of questions that separates a true interaction from a competing explanation for the child's change. When a child deteriorates after a new prescription, the clinician asks: is this an interaction, a dose error, disease progression, an adverse drug reaction, or an unrelated new problem? Each explanation leads to a different action, and conflating them leads to harm. [11] [12]
When the change points toward an interaction, the clinician narrows the question: which two drugs, which shared enzyme or pathway, and what is the direction and timing? A child on tacrolimus who becomes tremulous a week after fluconazole was started has a classic CYP3A4 inhibition interaction; a child with new seizures a month after tuberculosis treatment began has a probable induction interaction lowering anticonvulsant levels. Naming the enzyme, the direction, and the timing converts a vague concern into an actionable diagnosis. [1] [2]
The prescribing error is a differential that sits beside the interaction and overlaps with it. A tenfold dose error from a misplaced decimal point, a wrong-frequency error, or an omission error may present identically to an interaction. A structured approach — check the level, check the dose, check the frequency, check the list against the Best Possible Medication History — resolves the cause rather than treating only the symptom. Prescribing errors are documented across paediatric inpatient care and are a leading contributor to medication-related harm. [11] [12]
Clinical & Bedside Assessment
Bedside assessment of an interaction means examining the prescription list, not the child alone. The clinician asks five questions of every new prescription: Which enzyme metabolises this drug? Does the new drug inhibit or induce that enzyme? What is the likely effect on every concurrent substrate? How does the child's age and organ function change the magnitude? What monitoring will confirm or refute the interaction? A prescription that cannot answer these questions needs an interaction check before it is signed. [1] [4]
Recognising the high-risk enzyme pairs is a core clinical skill. CYP3A4 is inhibited by erythromycin, clarithromycin, fluconazole, itraconazole, voriconazole, diltiazem, and grapefruit juice, and induced by rifampicin, phenytoin, and carbamazepine; its substrates include tacrolimus, ciclosporin, theophylline, many statins, and some benzodiazepines. Note that azithromycin is a weak CYP3A4 inhibitor and is a safer macrolide choice when an interaction is a concern. CYP2C9 is inhibited by fluconazole and amiodarone and metabolises warfarin and phenytoin, so a child starting fluconazole while on warfarin needs closer international normalised ratio monitoring. [2] [3]
| Enzyme | Key inhibitors | Key inducers | Representative substrates |
|---|---|---|---|
| CYP3A4 | Erythromycin, clarithromycin, fluconazole, itraconazole, grapefruit | Rifampicin, phenytoin, carbamazepine | Tacrolimus, ciclosporin, theophylline, many statins, midazolam |
| CYP2D6 | Fluoxetine, paroxetine, quinidine | None of clinical consequence | Codeine activation, many antidepressants, atomoxetine |
| CYP2C9 | Fluconazole, amiodarone | Rifampicin, carbamazepine | Warfarin, phenytoin, NSAIDs |
| CYP2C19 | Fluconazole, omeprazole | Rifampicin, carbamazepine | Clopidogrel activation, proton pump inhibitors, phenytoin |
| CYP1A2 | Fluvoxamine, ciprofloxacin | Tobacco smoke, phenytoin | Theophylline, caffeine, clozapine |
The pharmacodynamic additive interactions are assessed by looking at shared physiology, not enzyme tables. Two or more QT-prolonging drugs — macrolides, fluoroquinolones, ondansetron, antipsychotics — given together raise torsades risk. Two sedatives — an opioid with a benzodiazepine — raise respiratory depression risk. A non-steroidal anti-inflammatory drug with an angiotensin-converting-enzyme inhibitor and a loop diuretic in a dehydrated child causes the triple-whammy acute kidney injury. The selective serotonin reuptake inhibitor combined with tramadol, linezolid, or a monoamine oxidase inhibitor causes serotonin syndrome. Recognising the shared target is the assessment skill. [1] [5]
Investigations
Therapeutic drug monitoring is both the investigation that confirms an interaction and the safety tool that guides dose adjustment when an interacting combination cannot be avoided. For narrow-therapeutic-index drugs such as phenytoin, tacrolimus, ciclosporin, digoxin, and theophylline, a level measured after a new interacting drug is started will show the direction and magnitude of the effect. A rising tacrolimus level after fluconazole confirms CYP3A4 inhibition; a falling phenytoin level after rifampicin confirms induction. The level alone does not make the diagnosis, but it confirms the interaction the clinician predicted from the enzyme knowledge. [5] [12]
MINTS — the narrow-index drugs to monitor
Phenytoin illustrates how monitoring guides safe dosing, with a target therapeutic range typically cited around 10 to 20 mg per litre. Because phenytoin follows saturable, Michaelis-Menten kinetics, small dose increases can produce disproportionately large rises in level, and a CYP2C9 or CYP2C19 inhibitor such as fluconazole amplifies this further. A child on phenytoin who starts fluconazole needs a level check, dose review, and clinical review for toxicity — not a reflex dose continuation. The same principle applies to every narrow-index substrate. [5] [12]
The medication list is itself an investigation. Reconciling the admission list against the community pharmacy record and the family account frequently uncovers medicines the inpatient team did not know about, doses that have drifted, and over-the-counter or herbal products that interact. A child who takes St John's wort — a potent CYP3A4 inducer — that no one recorded will have unexpectedly low levels of co-prescribed substrates. The reconciliation interview is an investigation that prevents harm. [7] [10]
Management — Resuscitation
The resuscitation priority in a severe drug interaction is to stop the offending combination and treat the toxicity. A child with serotonin syndrome from a selective serotonin reuptake inhibitor and tramadol needs cessation of both, supportive care with cooling and benzodiazepines for agitation, and escalation if autonomic instability develops. A child with QT prolongation and torsades from interacting macrolide and antiemetic therapy needs cessation of both drugs, electrolyte correction, and cardiac monitoring. A child with opioid respiratory depression from combined sedatives needs airway support and naloxone. [1] [5]
Management principles for the interacting pair (verify against current local guidance)
The principle that governs resuscitation is the same one that governs every subsequent step: predict the interaction before it causes harm, and act on the prediction. A child on tacrolimus who needs antifungal therapy should either receive a non-azole such as nystatin, or have the tacrolimus dose reduced and levels checked before toxicity develops. Treating the interaction after it has caused harm is a failure of anticipation. [1] [4]
Management — Definitive & Stepwise

The definitive management of drug interactions is anticipation, substitution, and monitoring. When an interacting pair is identified, the clinician chooses among four options: avoid the combination entirely; substitute a non-interacting alternative, such as azithromycin for erythromycin or nystatin for fluconazole; adjust the dose of the substrate and monitor the level; or accept the combination with enhanced monitoring when no alternative exists. The choice depends on the severity of the potential interaction, the availability of alternatives, and the child's clinical context. [1] [4]
Medication reconciliation is the definitive process that catches the interactions, omissions, and duplications that no individual prescriber will foresee. The structured cycle — collect the Best Possible Medication History, compare it against every new order, resolve discrepancies, communicate the reconciled list, and monitor — is applied at every transition of care: admission, transfer between wards or units, and discharge. Each transition is a documented high-risk point where reconciliation reduces error rates, and pharmacist-led reconciliation is the model with the strongest evidence. [7] [9]
The discharge reconciliation deserves particular emphasis because it is where harm most often follows the child home. A randomised trial of health-literacy-informed communication at discharge reduced medication errors in hospitalised children, demonstrating that how the list is communicated matters as much as its accuracy. The reconciled discharge list should be explained to the family in plain language, written down, and confirmed to have reached the general practitioner and the community pharmacy before the child leaves. [10]
The reconciliation timeline across a hospital episode
Specific Subtypes & Scenarios
The transplant or oncology child on a calcineurin inhibitor is the paradigm of predictable, high-consequence interaction. Tacrolimus and ciclosporin are both CYP3A4 substrates with narrow therapeutic windows, and the azole antifungals and macrolide antibiotics are among the most powerful CYP3A4 inhibitors in paediatric use. A child who develops mucositis and starts fluconazole or who needs erythromycin for a chest infection will accumulate the calcineurin inhibitor and develop nephrotoxicity, neurotoxicity, or both. The management is anticipation: use a non-azole antifungal such as nystatin where possible, reduce the tacrolimus dose preemptively when an azole cannot be avoided, and check the level within days. [1] [5]
The child on anticonvulsants presents the interaction challenge from both directions. Enzyme-inducing anticonvulsants — phenytoin, carbamazepine, phenobarbitone — lower the levels of co-prescribed substrates such as oral contraceptives, warfarin, and many antimicrobials, while themselves being substrates affected by inhibitors. A girl on carbamazepine who starts a combined oral contraceptive at adolescence needs a higher oestrogen dose or an alternative method, because induction will reduce contraceptive efficacy. Phenytoin, a CYP2C9 and CYP2C19 substrate, is particularly vulnerable to fluconazole, which can push levels into the toxic range. [2] [5]
The neonate is the population where developmental pharmacokinetics change the interaction landscape most. Immature CYP3A4 and CYP2D6 activity means substrate drugs are cleared slowly, and an inhibitor produces a proportionally greater accumulation than in an older child. Renal immaturity compounds this for renally cleared drugs. Doses, intervals, and interaction checks must all be age-adjusted, and neonatal pharmacology reference sources — not adult values scaled by weight — are mandatory. The same macrolide-theophylline interaction that requires monitoring in a school-age child may be contraindicated or demand far closer surveillance in a neonate. [2] [4]
The complex, technology-dependent child is the population where reconciliation earns its place. These children take many medicines, are managed across multiple specialties, and move through frequent admissions and discharges. Each transition is an opportunity for omission or duplication, and each additional medicine is an opportunity for a new interaction pair. Pharmacist-led reconciliation, a single shared medicines list, and a dedicated complex-care coordinator are the structures that protect these children from medication-related harm. [6] [9]
Complications & Pitfalls
The complications of drug interactions are the toxicities and treatment failures they produce. A raised tacrolimus level causes nephrotoxicity and neurotoxicity; theophylline toxicity causes seizures and arrhythmia; QT prolongation causes syncope or sudden death; serotonin syndrome causes hyperthermia, rigidity, and autonomic instability; warfarin over-anticoagulation causes bleeding. On the other side, induction causes treatment failure — a pregnancy on an inducer-reduced contraceptive, a breakthrough seizure on a lowered anticonvulsant, a thrombosis on an under-anticoagulated warfarin regimen. Each complication is the downstream effect of an interaction that was not anticipated. [1] [5]
Three pitfalls undermine interaction safety at the bedside. Prescribing without an interaction check is the foundational failure — a new drug added to a complex list with no enzyme analysis or checker run. Failing to reconcile at transition leaves the team working from an incomplete or outdated list, so omissions and duplications propagate. Ignoring developmental pharmacokinetics — dosing or assessing interaction risk in a neonate as if the child were a small adult — produces both underdosing and toxicity. Each pitfall is preventable by a structured habit. [7] [11]
Anticipate
- Name the enzyme for every drug
- CYP3A4 inhibitors: macrolides, azoles, grapefruit
- Inducers: rifampicin, phenytoin, carbamazepine
- Azithromycin is the safer macrolide
Timing
- Inhibition: hours to days → toxicity
- Induction: one to two weeks → loss of efficacy
- Check levels after any new interacting drug
- Set a monitoring review point
High-risk pairs
- Azole/macrolide plus tacrolimus or ciclosporin
- Rifampicin plus contraceptive, warfarin, anticonvulsant
- Two serotonergic agents
- QT-prolonging combinations
- Triple-whammy NSAID plus ACE inhibitor plus diuretic
Reconcile
- Best Possible Medication History from two sources
- Reconcile at admission, transfer, discharge
- Pharmacist-led model has strongest evidence
- Plain-language discharge communication
Pitfalls
- No interaction check before prescribing
- Unreconciled list at transition
- Dosing a neonate like a small adult
- Forgetting over-the-counter and herbal products
“Anticipate the interaction (name the enzyme and the direction) → reconcile every medicine at every transition (collect, compare, communicate, monitor) → substitute, dose-adjust, or monitor the high-risk pair → developmental pharmacokinetics change everything for the neonate.”
A communication pitfall is the unverified discharge list. A child sent home on a list that the family does not understand, that the general practitioner has not received, and that the community pharmacy has not confirmed will accumulate discrepancies within days. Plain-language explanation, a written list, and confirmed transmission to the receiving clinicians convert the discharge reconciliation from a paperwork exercise into the patient-safety intervention the evidence supports. [10]
Prognosis & Disposition
The prognosis of an interaction depends entirely on whether it was anticipated and managed. A tacrolimus-azole interaction that is predicted, dose-adjusted, and monitored causes no harm; the same interaction unrecognised causes nephrotoxicity and graft complications. A warfarin-fluconazole interaction that triggers closer international normalised ratio monitoring stays safe; the same interaction ignored causes bleeding. Prognosis is therefore a function of the prescribing habit, not of the pharmacology. [1] [5]
Disposition decisions turn on the same habits. A child on a stable, reconciled regimen with planned monitoring for an accepted interaction can be managed as an outpatient or discharged safely. A child with an unresolved high-risk interaction, an unreliable medicines list, or a recent severe interaction-related toxicity may need inpatient stabilisation, closer monitoring, or specialist pharmacology input before discharge. The disposition follows the quality of the reconciliation, not the diagnosis alone. [7] [9]
The long-term prognosis of effective reconciliation and interaction management extends beyond the individual child. Children with complex chronic conditions accumulate medicines over years, and each avoided interaction and each accurate reconciliation builds a safer longitudinal record. Embedding reconciliation and interaction checking into every transition of care is the quality improvement that protects the child across a lifetime of prescriptions, not just a single admission. [6] [10]
Special Populations
The neonate requires age-adjusted interaction assessment as a core safety measure, not an optional refinement. Immature CYP3A4, CYP2D6, and renal function change both the baseline handling of every drug and the magnitude of any interaction. An inhibitor produces a proportionally greater accumulation in a neonate than in an older child because baseline clearance is already low. Neonatal pharmacology reference sources and specialist pharmacy input are mandatory, and adult values scaled by weight are inappropriate at every step. [2] [4]
The complex, technology-dependent child carries the highest interaction and reconciliation risk in paediatrics. Polypharmacy, multiple prescribers, and frequent transitions combine to create combinatorial exposure to interacting pairs and repeated opportunities for omission or duplication. Pharmacist-led reconciliation, a single shared medicines list, and a dedicated complex-care coordinator are the structures that reduce medication-related harm in this population. Every admission and discharge for these children should trigger a full reconciliation and interaction review. [6] [9]
Australia and Aotearoa New Zealand: the Australian Medicines Handbook Children's Dosing Companion (AMH CDC) and the Royal Children's Hospital Melbourne Clinical Practice Guidelines are the primary paediatric dosing and interaction references, supported by the Australian Commission on Safety and Quality in Health Care medication safety program, which sets the National Medication Management Plan standard for inpatient reconciliation. Local formulary and interaction-checker policies vary and must be checked against the current source. [7]
Global and low-resource settings: the WHO Medication Without Harm challenge frames medication safety, reconciliation, and interaction management as a global priority, particularly where pharmacy and electronic decision-support resources are limited. A structured, paper-based Best Possible Medication History and a simple interaction check using the available national formulary remain feasible and high-value in any setting. Adapting the process to local resources — rather than abandoning it — is the principle for low-resource practice. [7] [10]
Evidence, Guidelines & Regional Differences
The evidence base for clinically significant paediatric drug interactions has grown through ICU and surgical-cohort studies that quantify how often cytochrome P450-mediated interactions occur in children and which pairs are most consequential. The classic ontogeny work on CYP3A4 established the developmental basis for age-dependent interaction magnitude, and contemporary pharmacogenomic and physiologically-based pharmacokinetic modelling is extending that understanding. The pattern is consistent: interaction risk rises with polypharmacy, acuity, and the use of enzyme inhibitors or inducers, and it is greatest in the youngest and the most complex children. [1] [2] [3]
Medication reconciliation evidence is mature and consistent. Pharmacist-led reconciliation reduces medication errors at admission, transfer, and discharge, and structured interventions in specific paediatric populations — the emergency department, the haemato-oncology unit, and the neurology inpatient unit — have shown measurable reductions in reconciliation errors. The health-literacy-informed discharge communication randomised trial extended the evidence from accuracy of the list to safety of its transmission, showing that how the reconciled list is communicated to families changes outcomes. [8] [9] [10]
Prescribing-error epidemiology underpins both arguments. Studies across paediatric inpatient and critical-care settings document a substantial burden of prescribing errors, many arising from incomplete reconciliation and failure to anticipate interactions, with the highest rates in the most complex and acutely ill children. The evidence converges on a single message: structured reconciliation and proactive interaction checking are the interventions that reduce the error rate, and both must be embedded in routine practice rather than left to individual vigilance. [11] [12]
Board and assessment distinctions
RACP current PREP curriculum candidates in 2026 must demonstrate safe prescribing, interaction anticipation, and reconciliation within acute and general paediatric learning objectives, while first-year trainees from 2027 encounter these under quality and safety goals. RCPCH Progress+ embeds safe prescribing and patient safety as core outcomes. The ABP General Pediatrics Content Outline covers pharmacology and medication management alongside quality and safety as distinct domains. [7] [11]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Interpret a vignette and predict the interaction or identify the reconciliation error |
| RACP DCE long case | Reconcile a complex medicines list, anticipate interactions, and build a safe transition plan |
| MRCPCH clinical | Explain the reconciled list and interaction plan to a family in plain language |
| ABP | Apply pharmacology and patient-safety domains to predict and manage an interaction |
| RCPSC structured oral | Defend an interaction-management and reconciliation plan across age groups and transitions |
Exam Pearls
Viva: predict the interaction before it happens
A strong viva answer names the enzyme, the direction, the timing, and the management. "Tacrolimus is a CYP3A4 substrate with a narrow therapeutic window. Fluconazole is a potent CYP3A4 inhibitor, so the tacrolimus level will rise within hours to days, causing nephrotoxicity and neurotoxicity. I would anticipate this by using a non-azole antifungal such as nystatin where possible, reducing the tacrolimus dose preemptively if an azole is unavoidable, checking the level within a few days, and reviewing the child clinically. The principle is to predict the interaction before it causes harm." [1] [2]
Structured oral: build the Best Possible Medication History
Do not accept a single-source list. "I take the Best Possible Medication History from at least two sources — the family interview, the community pharmacy record, the general practitioner summary, and any transfer or discharge letter. For every medicine I record the name, dose, route, frequency, last dose taken, and adherence, and I ask specifically about over-the-counter, herbal, and as-needed products, because St John's wort and other inducers are easily missed. I compare this list against every admission order, flag omissions, duplications, wrong doses, and interactions, and resolve them with the prescriber before any drug is given." [7] [8]
References
- [1]Li, Ting; Hu, Bo; Ye, Lin Clinically Significant Cytochrome P450-Mediated Drug-Drug Interactions in Children Admitted to Intensive Care Units International journal of clinical practice, 2022.PMID 36081809
- [2]de Wildt, Saskia N; Kearns, Gregory L; Leeder, J Steven Cytochrome P450 3A: ontogeny and drug disposition Clinical pharmacokinetics, 1999.PMID 10628899
- [3]Emoto, Chiroaki; Johnson, Trevor N Cytochrome P450 enzymes in the pediatric population: Connecting knowledge on P450 expression with pediatric pharmacokinetics Advances in pharmacology (San Diego, Calif.), 2022.PMID 35953161
- [4]Lu, Hong; Rosenbaum, Sara Developmental pharmacokinetics in pediatric populations The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG, 2014.PMID 25762871
- [5]Faria, James; Solverson, Matthew; Faria, Matthew Potential Cytochrome P450 Drug-Drug Interactions among Pediatric Patients Undergoing Tonsillectomy Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery, 2019.PMID 30105930
- [6]Feudtner, Chris; Dai, Dongyang; Hexem, Kelly R Prevalence of polypharmacy exposure among hospitalized children in the United States Archives of pediatrics and adolescent medicine, 2012.PMID 21893637
- [7]Merandi, Jacqueline; Sapko, Michael; Catt, Carmen Medication Reconciliation Pediatrics in review, 2017.PMID 28044039
- [8]Sheth, Shreya; Bialostozky, Margarita; Hollenbach, Katherine Standardizing Medication Reconciliation in a Pediatric Emergency Department Pediatrics, 2024.PMID 38273780
- [9]Adducchio, Stefano; Grant, Evan D; Fonseca, Lais D Reducing Discharge Medication Reconciliation Errors at a Pediatric Neurology Inpatient Unit Neurology. Clinical practice, 2024.PMID 38524835
- [10]Carroll, Athena R; Johnson, Jeffrey A; Stassun, Jonathan C Health Literacy-Informed Communication to Reduce Discharge Medication Errors in Hospitalized Children: A Randomized Clinical Trial JAMA network open, 2024.PMID 38227315
- [11]Davis, Tom Paediatric prescribing errors Archives of disease in childhood, 2011.PMID 21109509
- [12]Glanzmann, Christiane; Frey, Bernhard; Meier, Christoph R Analysis of medication prescribing errors in critically ill children European journal of pediatrics, 2015.PMID 25899070